
Abstract
Background:
Patient safety during intra-hospital transport (IHT) of critically ill patients is a major global concern, as transfers expose patients to risks including physiological deterioration, equipment malfunction, and adverse events. Despite its importance, Iran lacks a standardized, culturally adapted tool to evaluate IHT safety from nurses’ perspectives. This study aimed to translate, culturally adapt, and psychometrically validate the Persian version of the Intra-hospital Transport Safety Scale (IHTSS) for use among Iranian intensive care unit (ICU) nurses.
Methods:
A methodological cross-sectional design was employed in three phases from April to June 2025. Phase 1 involved forward–backward translation and cultural adaptation of the IHTSS. Phase 2 assessed face and content validity through ICU nurses and expert panels using Content Validity Ratio (CVR) and Content Validity Index (CVI). Phase 3 comprised psychometric evaluation among 315 ICU nurses recruited from hospitals in western Iran. Exploratory and confirmatory factor analyses were conducted to examine construct validity. Reliability was assessed through Cronbach’s α, McDonald’s ω, and test-retest analysis.
Results:
The Persian IHTSS demonstrated strong content validity (CVR = 0.93; S-CVI = 0.91). Exploratory factor analysis identified a four-factor structure Organization, Teamwork & Transport-related Tasks, Tools and Technologies, and Environment, explaining 63.1% of the total variance. Confirmatory factor analysis supported model adequacy (CFI = 0.96, RMSEA = 0.067, SRMR = 0.048). Internal consistency was high (Cronbach’s α = 0.891; ω = 0.877), and test–retest reliability confirmed temporal stability (r = 0.881).
Conclusion:
The Persian version of the IHTSS is a valid, reliable, and culturally adapted instrument for assessing IHT safety in Iranian ICUs. Its application can help identify system-level strengths and weaknesses, guide targeted interventions, and enhance patient safety during critical care transfers.
Keywords
Introduction
Patient safety has emerged as a critical global concern within the healthcare sector.1,2 Among hospital units, intensive care unit (ICU) patients are particularly vulnerable to safety challenges and adverse events due to their compromised physiological status and the complexity of their care.3,4 While these patients necessitate continuous bedside monitoring and care, intra-hospital transfer (IHT) to access specialized diagnostic or therapeutic procedures unavailable within the ICU is often required. 5 This process, however, introduces inherent risks that can jeopardize patient safety. 6 The transition between care environments with differing resources presents a significant potential for adverse outcomes. Indeed, IHT has been associated with increased mortality and morbidity, contributing to up to 71% of reported adverse events during intra-hospital transport (IHT). 7 These events frequently include deterioration of physiological parameters, equipment malfunctions, and complications related to medical devices such as tubes and lines. 8 The etiology of these incidents can be attributed to reduced monitoring intensity compared to the ICU setting and limitations in providing advanced care during transit. 7 A study conducted in Iran by Alizadeh Sharafi et al. 9 identified critical care nurses’ recommendations for improving IHT quality. These recommendations were categorized into two main areas: (1) the patient’s clinical situation, which includes stabilizing the patient’s condition in terms of hemodynamic status and connections, as well as optimizing transport equipment; and (2) organizational structures, which involve planning for adequate human resources, effective IHT management, enhanced communication, prevention of physical injury, and improvements in organizational frameworks and physical space.
Established guidelines stipulate that an IHT team should consist of at least two healthcare providers, including a critical care nurse and a physician proficient in airway management. Additionally, in cases requiring mechanical ventilation, a respirator must be available. 9 Nurses constitute a pivotal component of the transfer team, playing a crucial role in safeguarding patient well-being throughout the IHT continuum. 10 Their expertise enables the identification and timely management of potentially life-threatening risks, thereby preserving patient safety. 9 Nurses are actively involved across various phases of IHT, from initial planning and equipment preparation to procedural execution and post-transfer evaluation. 11 Given their integral role, investigating the experiences of ICU nurses regarding IHT through a standardized assessment tool can provide valuable insights into the strengths and weaknesses of existing hospital protocols, facilitating targeted quality improvement initiatives.
A comprehensive review of available instruments for assessing IHT safety revealed several tools. Jarden and Quirke (2010) 12 developed an evidence-based tool for ICU nurses to enhance both the safety and documentation during IHT, integrating patient assessment with a procedural guideline. Furthermore, Brunsveld-Reinders et al. (2015) 13 designed a checklist to increase the safety of IHT, ensuring comprehensive coverage of critically ill patient transport from start to finish. While these instruments contribute to continuity of care and enhanced safety during IHT, they do not explicitly evaluate the overall level of IHT safety. To address this limitation, Bergman et al. (2020) 14 developed the Intra-hospital Transport Safety Scale (IHTSS) in ICUs, encompassing five dimensions: Organization, Tools and Technologies, Environment, Teamwork, and Transport-Related Tasks. This self-report scale comprehensively assesses ICU nurses’ perceptions of IHT safety for critically ill patients, offering valuable insights into multifaceted aspects of the process. Notably, Li et al. (2024) 15 psychometrically validated a Chinese version of the IHTSS among ICU nurses, indicating its potential for cross-cultural applicability.
In Sweden, where the original instrument was developed, hospitals have placed significant emphasis on improving the quality and safety of IHT, surpassing many other countries, including Iran, through continuous efforts to enhance this process. 5 It can be attributed to several factors, including adequate staffing during transfers, the availability of appropriate medical equipment and continuous monitoring, specialized transport teams with dedicated training, and a strong emphasis on quality and safety improvement initiatives. Conversely, physician presence is often lacking in Iranian hospital transfer teams, which typically comprise a nursing assistant, a nurse, and occasionally an anesthesia technician. 5 Deficiencies in monitoring, inadequate training, and insufficient awareness among nurses and transport teams contribute to the identified weaknesses in IHT practices within Iranian hospitals. Despite increasing attention in recent years, the concept of IHT remains in its nascent stages in Iran. Consequently, further research in this context is crucial to optimize the process and mitigate associated adverse events.
A study conducted in Iran suggested that the quality of IHT for critical patients is unsatisfactory. Furthermore, the study emphasizes the necessity of incorporating patient transfer standards and guidelines into the nursing curriculum and in-service training programs for practicing nurses to enhance safety and quality. 16 Generally, Iranian nurses often assume greater responsibility during IHT compared to their counterparts in many other countries, potentially leading to an increased psychological burden. Therefore, a standardized self-report assessment of IHT safety by Iranian ICU nurses can effectively identify strengths and weaknesses in current practices and protocols within Iranian hospitals, playing a pivotal role in enhancing the IHT process and ultimately improving patient safety. Furthermore, a standardized and comprehensive instrument specifically designed or validated to assess IHT safety within the unique cultural context, social norms, and healthcare system structure of Iran is currently lacking. The IHTSS presents a promising avenue to address this gap. 14 However, given that the IHTSS was developed and validated in Sweden, a country with distinct cultural, social, and healthcare system characteristics compared to Iran, its application necessitates a rigorous psychometric validation process tailored to the Iranian context. This will ensure that the specific needs of Iranian hospitals in this critical area are accurately and appropriately addressed. Consequently, to bridge this gap and recognize the significance of the issue, the present study was undertaken to adapt, translate, and psychometrically validate the IHTSS into the Persian language within Iran.
Methods
This methodological inquiry, employing a cross-sectional design, was implemented from April to June 2025 across three consecutive phases. The first phase entailed the forward–backward translation and cultural adaptation of the Intra-hospital Transport Safety Scale (IHTSS) into Persian. The second phase examined the face and content validity of the instrument through a consensus-oriented methodology. The third phase comprised a cross-sectional validation initiative, incorporating data collection to scrutinize the psychometric characteristics of the IHTSS among critical care nurses in Iran. The comprehensive research protocol was reported and substantiated in conformity with the Consensus-based Standards for the Selection of Health Measurement Instruments guidelines. 17
Phase 1: Cultural adaptation process
Before commencing the investigation, explicit authorization was procured from the original developer of the IHTSS. The scale was subjected to a systematic linguistic and cultural adaptation protocol, translating it from English to Persian. 18 Two independent bilingual translators, whose native language was Persian and who were fluent in English, performed the initial forward translation. One translator was a healthcare professional familiar with the study’s concepts (informed translator), while the other was a professional translator unfamiliar with these concepts (uninformed translator), ensuring both linguistic accuracy and clear lay understanding. Subsequently, an expert panel composed of the study investigators and two proficient translators—scrutinized and amalgamated these translations to yield a preliminary Persian variant. To validate accuracy and conceptual congruence, a bilingual expert executed a back-translation into English. The panel juxtaposed this back-translated iteration with the original to discern discrepancies and affirm semantic and conceptual equivalence. Divergences were meticulously deliberated, culminating in consensual revisions to augment clarity and cultural appropriateness. A pilot assessment ensued, engaging a targeted cohort of 15 ICU nurses with varying years of experience to evaluate item comprehensibility and contextual relevance using a structured questionnaire and cognitive interviews. Feedback from this pilot focused on the clarity of specific instructions and the relevance of certain safety checks in the local context. This process ensured that the Persian IHTSS authentically encapsulated the original constructs while aligning with the Iranian nursing paradigm.
Phase 2: Face and content validity
Face validity was assessed by 15 ICU nurses. The number of participants is consistent with the guideline proposed by Mikkonen et al. (2022), 19 recommending a sample of 10 to 20 individuals for such evaluations. The experts examined the tool for clarity and offered alternative wording for items that appeared ambiguous. Their feedback was subsequently reviewed by the research team, and consensus was achieved on the finalized version.
Content validity was appraised utilizing a mixed-methods paradigm. The expert panel comprised 14 specialists: 8 critical care nurses with over 10 years of clinical experience in ICUs, 3 anesthesiology physicians, 2 instrument psychometrics, and 1 medical linguist, furnished qualitative feedback pertaining to grammatical structure, lexical precision, item organization, instructional lucidity, and relevance to Iranian nursing practice. Quantitatively, content validity was quantified using the Content Validity Ratio (CVR) and Content Validity Index (CVI). Experts rated item essentiality on a three-point Likert scale (ranging from non-essential to essential) for CVR computation, the minimum acceptable CVR value against Lawshe’s criteria for 14 experts was 0.51. 20 For CVI, item relevance was gauged on a four-point Likert scale (from irrelevant to highly relevant), deriving item-level Content Validity Index (I-CVI) and scale-level average Content Validity Index (S-CVI/Ave). Acceptability thresholds were established as I-CVI exceeding 0.78 and S-CVI/Ave surpassing 0.90.21,22
Phase 3: Psychometric evaluation
Study design and participants
In accordance with a cross-sectional validation design, a sample of 315 nurses working in the ICUs of hospitals affiliated with the University of Medical Sciences in Kermanshah Province, Iran, was selected. Participant selection employed convenience sampling predicated on predefined inclusion criteria: possession of at least a bachelor’s degree, engagement in IHT of critically ill patients within the preceding year, and provision of informed consent. The exclusive criterion for exclusion was questionnaire incompletion exceeding 10%. 23 Sample size estimation adhered to established psychometric guidelines for exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). For EFA, 240 participants were designated in accordance with a maximum participant-to-item ratio of 1:10, 24 whereas CFA required 7 to 20 participants per item, 25 necessitating 315 participants. The EFA phase included 240 participants, which then increased to 315 participants for the CFA phase. The total sample was then divided into two independent subsamples to facilitate a robust construct validation process26,27: one for the EFA (n = 240) and the other for the CFA (n = 315).
Convergent and discriminant validity
Convergent and discriminant validity were measured using Fornell and Larker’s method, focusing on average variance extracted (AVE), maximum shared squared variance (MSV), and composite reliability (CR). It is advisable to ensure the CR values are above 0.7 and the AVE values of the constructs are above 0.5 to confirm convergent validity (CR > AVE). The Fornell and Larcker criterion mandates that the MSV should be lower than the AVE. To confirm discriminant validity, it is recommended that the values of the HTMT matrix should be below 0.9.28,29
Data collection procedures and context
Following institutional approvals, eligible nurses were recruited via convenience sampling at each facility. Study objectives were elucidated, informed consent obtained, and sealed questionnaires disseminated at nursing stations across all shifts (morning, afternoon, and night). To facilitate veracious self-reporting, participants completed the instruments autonomously in private locales, such as residences or designated respite areas. Bias mitigation was achieved by ensuring the absence of researcher or supervisory presence during completion. Of the 328 distributed questionnaires, 315 were fully completed and incorporated into the analyses, with 13 excluded owing to substantial incompleteness. The questionnaire encompassed three components: (1) informed consent from critical care nurses; (2) sociodemographic attributes (e.g., gender and age); and (3) the IHTSS items.
Instrument overview
Bergman et al. (2020), 14 developed the Intra-hospital Transport Safety Scale (IHTSS) in Sweden to evaluate the safety of intra-hospital transport among critically ill patients. The instrument includes 24 items distributed across five dimensions: organization (6 items), tools and technology (5 items), environment (5 items), teamwork (4 items), and transport-related tasks (4 items). Responses are rated on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree.” The overall score ranges from 24 to 120, with higher scores indicating a higher perceived level of transport safety. In line with the original validation, it is recommended to calculate and interpret both the total score and the individual subscale scores, as this provides a comprehensive view of the specific safety dimensions. “The original version demonstrated strong internal consistency, with a Cronbach’s α of 0.88, while the subscales also indicated acceptable reliability, with coefficients between 0.72 and 0.82.”
Statistical analyses
Psychometric scrutiny of the Persian IHTSS proceeded in two discrete stages. Initially, descriptive statistics—including means, standard deviations, frequencies, and percentages—delineated sociodemographic profiles and item distributions. Skewness and kurtosis values for all items of the Persian IHTSS ranged between −2 and +2, indicating an approximately normal distribution.
Subsequently, in alignment with contemporary psychometric methodologies, factorial validity was interrogated. Construct validity was elucidated via EFA and CFA. Data adequacy was corroborated by the Kaiser-Meyer-Olkin (KMO) index (threshold > 0.7) and Bartlett’s test of sphericity (p < 0.05).30,31
EFA was conducted employing maximum likelihood estimation coupled with oblique rotation (Promax) to delineate the underlying factor architecture. Promax rotation was selected for its efficacy in large samples, facilitating streamlined factor configurations while accommodating inter-factor correlations.32,33 Criteria encompassed total explained variance exceeding 40%, eigenvalues surpassing 1, and factor loadings greater than 0.5.34–36 Communalities were inspected, with values of 0.30 or higher deemed satisfactory for ascertaining the extent of item variance captured by extracted factors. 37
CFA utilized maximum likelihood estimation to corroborate the hypothesized model. Model fit was appraised using established indices: (a) χ²/df ratio below 3; (b) comparative fit index (CFI) and (c) Tucker-Lewis index (TLI) at or above 0.90;38,39 (d) root mean square error of approximation (RMSEA) at or below 0.08; and (e) standardized root mean square residual (SRMR) at or below 0.08.40,41 Item-factor associations were validated by loadings exceeding 0.30 and t-values surpassing 1.96. 42 Temporal stability was assessed through test-retest reliability, 52 participants were selected from the initial cohort, considering their continued availability and willingness to participate in study, re-administering the scale after a 10 to 14-day interval stating that it was chosen to minimize recall bias while assuming the stability of the nurses’ clinical knowledge and experience in patient transport over this short period. 43
It is also recommended that the sample size be at least 30 for the test–retest. 44 Internal consistency was evaluated via Cronbach’s α and McDonald’s ω, with coefficients exceeding 0.70 considered acceptable. 45 Statistical significance was set at p ⩽ 0.05. Analyses were performed using SPSS version 27 and LISREL version 8.
Results
Cultural adaptation process
The rigorous process of translation, back-translation, and cultural adaptation of the Persian version of the IHTSS demonstrated full conceptual equivalence with the original instrument. The forward–backward translation procedures revealed no major discrepancies between the source and translated versions. Furthermore, feedback from the pilot testing with ICU nurses confirmed that all items were clear, comprehensible, and contextually relevant to clinical practice in Iran
Face and content validity
During the pretest, minor linguistic modifications were applied to items 8, 16, and 20 to resolve ambiguities identified by participants. The changes were: Item 8 from “was reliable” to “demonstrated high reliability” for contextual precision; Item 16 from “maintain” to “preserve” to better encompass privacy protection; and Item 20 to “I feel safe during the sharing of transfer information” for grammatical clarity. All adjustments preserved the original meaning while enhancing item clarity and contextual appropriateness for the ICU nurse participants. Following expert appraisal and adjustments, all items were ratified as appropriate. Quantitative metrics yielded a CVR of 0.93, situated within the acceptable spectrum of 0.75 to 1. All I-CVI values surpassed 0.88, and the S-CVI attained 0.91, substantiating content validity across the 24 items.
Psychometric evaluation
The EFA subsample consisted of 240 nurses (mean age = 32.79 ± 4.82 years, range = 25–57), with 47.9% male, 57.5% married, and 81.67% possessing a bachelor’s degree. The CFA subsample included 315 nurses (mean age = 32.96 ± 4.79 years, range = 24–57), with 46% male, 57.46% married, and 83.17% holding a bachelor’s degree. Sociodemographic particulars are detailed in Table 1.
Demographic characteristics of participants in study.

The suitability of the data for factor analysis was confirmed, with the KMO measure of sampling adequacy being 0.88 and Bartlett’s test of sphericity reaching statistical significance (χ² = 3354.578, df = 276, p < 0.0001). EFA delineated a four-factor solution with eigenvalues exceeding 1, accounting for 63.12% of the total variance. Item loadings ranged from 0.556 to 0.903, all surpassing 0.50, thereby corroborating the factorial structure (Table 2). The scree plot further endorsed the four-factor model of the IHTSS (Figure 1).
Factor load and communalities of each item in IHTSS of 24 Items (n = 240).

Factor loadings ⩾ |0.50| are presented in bold to indicate a strong association with the intended factor.
IHTSS: Intra-hospital Transport Safety Scale.
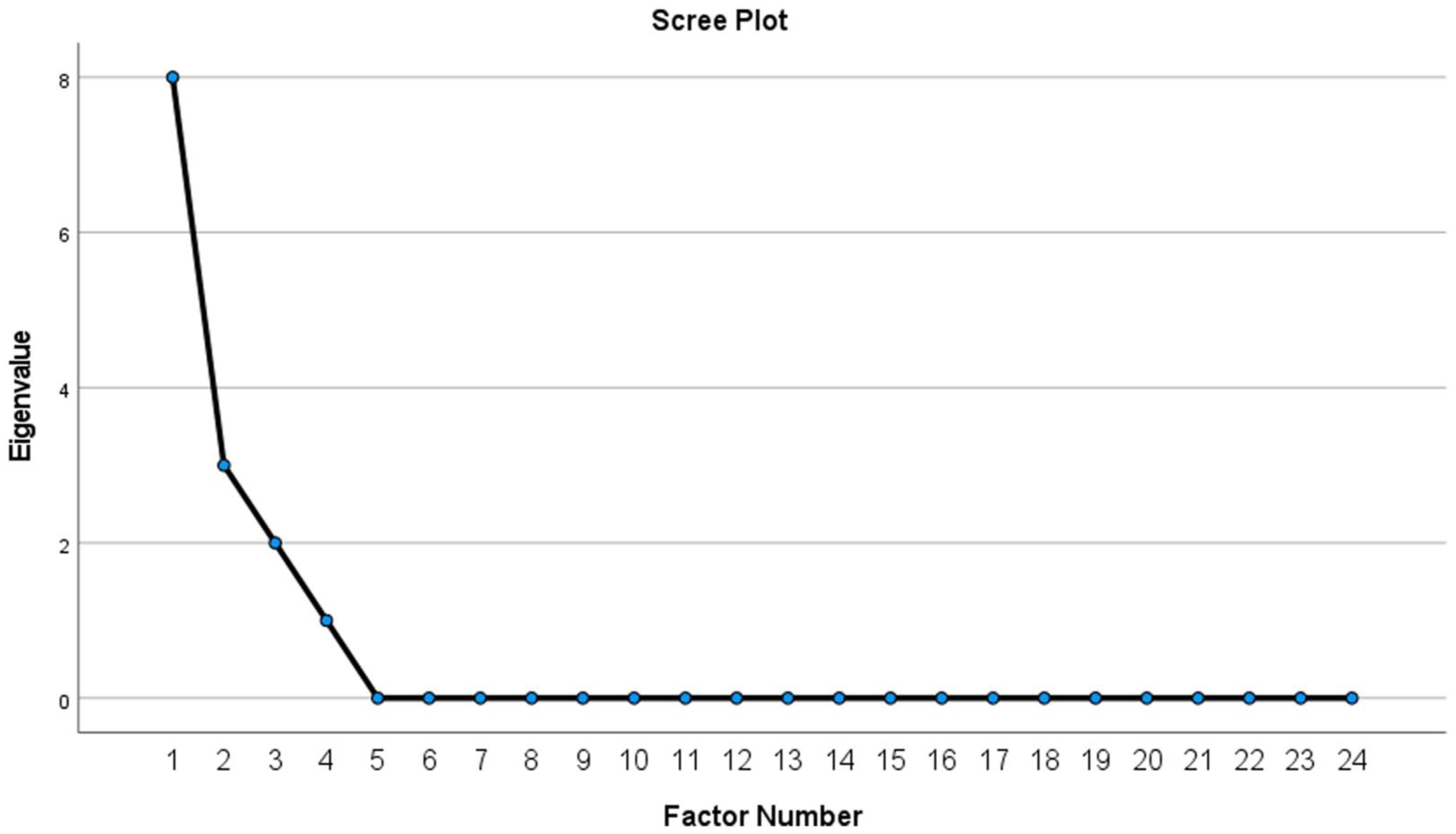
Scree plot of the extracted components of the Intra-hospital Transport Safety Scale.
According to Table 3, the Persian version merged all items from the original Teamwork and Transport-related Tasks into one dimension, Item 16, which was formerly part of the Environment dimension, has been relocated to the Tools and Technology dimension due to cultural factors affecting its interpretation. Following thorough discussions, the research team decided to rename the Teamwork and Transport-related Task dimensions to Teamwork & Transport-related task.
Item comparison after EFA.

Bold items indicate a shift from their originally hypothesized dimension to a different factor in the EFA.
EFA: exploratory factor analysis.
In the CFA model, all items exhibited factor loadings exceeding 0.30, ranging from 0.35 to 0.90, indicative of good associations between manifest variables and latent constructs (Figure 2). Corresponding t-values spanned 14.08 to 19.52, all attaining statistical significance (p < 0.001). Goodness-of-fit indices for the CFA model encompassed: χ² = 507.3, df = 246, p < 0.0001, χ²/df = 2.41, RMSEA = 0.067, NNFI/TLI = 0.95, CFI = 0.96, GFI = 0.96, and SRMR = 0.048, collectively denoting an acceptable model fit. Pearson correlation coefficients revealed positive and significant interrelations between subscales and the aggregate scale (Table 4).

Final measurement model of The Intra-hospital Transport Safety Scale from confirmatory factor analysis (N = 315).
Reliability, final scores, and correlations of IHTSS-P (N = 315).

The intra-hospital transport safety scale.
P < 0.05 **P < 0.01.
Convergent and discriminant validity
Convergent and discriminant validity were confirmed. CR and AVE values exceeded 0.7 and 0.5, respectively. AVE was higher than MSV and all HTMT values were below 0.9 showing divergent validity. CR was also confirmed, as CR values all exceeded 0.7 (Table 5).
Indices of the convergent and discriminant validity of the IHTSS-P (n = 315).
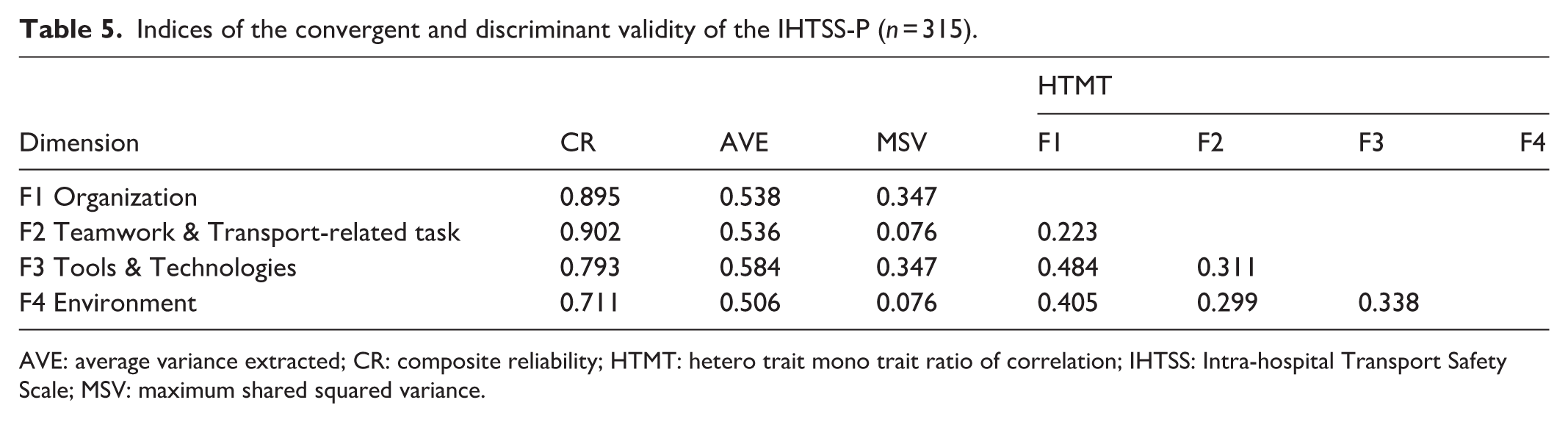
AVE: average variance extracted; CR: composite reliability; HTMT: hetero trait mono trait ratio of correlation; IHTSS: Intra-hospital Transport Safety Scale; MSV: maximum shared squared variance.
Reliability assessments
Internal consistency
The overall Cronbach’s α coefficient was 0.891, signifying commendable internal consistency. Subscale α values ranged from 0.744 to 0.904. McDonald’s ω for the total scale was 0.877, with subscale estimates from 0.774 to 0.904, further buttressing reliability (Table 4).
Test-retest reliability
To evaluate temporal stability, the instrument was re-administered to 52 nurses following a 2-week hiatus, yielding a reliability coefficient of 0.881(Pearson correlation coefficient). This outcome attests to the scale’s satisfactory consistency over time.
Discussion
In the present study, the IHTSS, originally developed by Bergman et al. (2020) 14 in Sweden, was translated into Persian, and its validation and psychometric evaluation were conducted on a sample of nurses working in ICUs. The final Persian version of this instrument comprised 4 factors and 24 items, adapted to the Iranian cultural context and confirmed accordingly. The content validity assessment of the instrument using the CVR and S-CVI yielded values of 0.93 and 0.91, respectively, indicating a high level of expert agreement and satisfactory content validity in the Persian version. To enhance the cross-cultural validity of the IHTSS, another study by Li et al. (2024) 15 in China reported I-CVI values ranging from 0.88 to 1.00 and an overall S-CVI of 0.91. These values also demonstrate strong content validity of the instrument in a different cultural context.
During the EFA phase of this research, four factors were identified: Organization, Teamwork & Transport-related Task, Tools and Technologies, and Environment. The findings revealed that the dimensional structure and item allocation in the Persian version of the IHTSS differed from the original version. 14 While the original version consisted of five factors, the present study extracted four factors, aligning with the structure of the Chinese version of the IHTSS. 15 One of the key differences between the Persian and Chinese versions compared to the original is the merging of the “Teamwork” and “Transport-related Task” dimensions, whereas in the original, these were defined separately. To justify the merging of “Teamwork” and “Transport-related Tasks” in the Persian IHTSS, it is important to acknowledge that IHT is inherently a team-based process, requiring coordinated and interdependent actions among nurses and transport personnel. Transport-related activities rely on effective team collaboration, as they cannot be performed in isolation. Research indicates that failures in team communication and coordination are major contributors to transport-related adverse events (Zhang et al., 2022; Manser, 2009).46,47 Thus, merging these factors is both statistically and theoretically justified, accurately reflecting that transport tasks are practical manifestations of teamwork and essential for ensuring patient safety in clinical practice. Some items exhibit minor cross-loadings on other factors, while their primary loadings remain strong. These cross-loadings are theoretically meaningful, reflecting the interconnected nature of IHT, where Organization, Teamwork & Transport-related Tasks, Tools, and Environment collectively contribute to patient safety. Overall, the strong primary loadings support the robustness and validity of the factor structure. Additionally, the placement of item 16, titled “We were able to maintain the patient’s privacy during the transport,” shifted in the Persian version from the “Environment” factor to the “Tools and Technologies” factor. This change likely reflects cultural differences and varying interpretations of the concept of “privacy”; in some cultures, patient privacy preservation is more closely associated with the use and application of nursing tools and equipment rather than physical environmental conditions. This relocation aligns with findings from the Chinese version of the instrument. 15 In the Iranian context, the concept of patient privacy extends beyond physical space to encompass the use of equipment and techniques that protect patient dignity and confidentiality. This interpretation aligns with culturally grounded nursing practices and ethical norms emphasizing modesty, respect, and patient dignity in Iranian healthcare settings. These differences clearly highlight the prominent role of cultural, linguistic, and demographic characteristics of the study population in interpreting and responding to the instrument’s items. Prior evidence has shown that the process of translating and culturally adapting psychometric instruments can significantly influence respondents’ perception of concepts. 48 Therefore, the current results emphasize the importance of meticulous attention to cultural and contextual differences during the translation, localization, and validation stages of psychometric instruments.
The four extracted factors in this study collectively accounted for 63.12% of the total variance in the data, indicating an acceptable and appropriate factor structure for the Persian version of the IHTSS. In the study by Bergman et al. (2020), 14 the variance explained by the five factors was reported as 59%. In contrast, Li et al. (2024) 15 in China reported that the four factors explained 75.97% of the variance. Comparing the percentages of explained variance across Iranian, Swedish, and Chinese contexts underscores the efficacy of the IHTSS in measuring key dimensions of IHT safety for critically ill patients in diverse cultural settings. The variance explained in the Persian version may have been influenced by differences in sample composition, such as variability in participants’ clinical experience and institutional resources. Additionally, contextual factors, including variations in transport protocols, staffing ratios, and equipment availability across Iranian hospitals, may account for some discrepancies with the Swedish and Chinese studies.
In this study, among the examined components of the instrument, the “Organization” factor accounted for the highest percentage of the total variance explained by the instrument, contributing 31.94% alone. These results align with the findings of Bergman et al. (2020), 14 where the organization factor also accounted for approximately 29% of the total variance. This finding suggests that organizational components, particularly in the pre- and post-transport phases, play a pivotal role in enhancing the safety of IHT processes. This factor includes six items and reflects structural and managerial dimensions effective in ensuring the safe execution of transports for critically ill patients. The items in this factor specifically emphasize the necessity of adequate staffing, appropriate time allocation, and effective coordination among pre- and post-transport care teams. Achieving these requirements is essential for maintaining care continuity, preventing treatment interruptions, and reducing functional disruptions in ICUs. Studies indicate that sufficient human resources and appropriate timing, both in the pre-transport preparation phase and the return and re-establishment phase in the ICU, are fundamental prerequisites for safety in the transport process.49,50 Strengthening organizational factors such as human resource management, proper scheduling, and improved coordination mechanisms can enhance the quality and safety of care during patient transports.
The second component of the instrument, “Teamwork & Transport-related Task,” explained 15.12% of the total variance in the present study, playing a significant role in ensuring the safety of IHT for critically ill patients. This factor comprises eight items addressing various aspects of team interaction, task division, team leadership, and coordinated performance of team members during transport. These findings demonstrate that transport safety depends not only on individual skills but also on coordinated and supportive team performance. The role of teamwork in improving clinical performance has been emphasized in numerous prior studies.8,51 Safe execution of tasks during transport requires a designated team leader, shared understanding of task sequences, clear division of responsibilities, and continuous feedback among team members. The presence of these items enhances team efficiency, reduces the likelihood of errors, and promotes patient safety.51,52 Effective task performance necessitates technical skills and knowledge related to transport stages. When team members share a common understanding of the workflow and support each other, performance improves substantially.8,9 Coordination in roles and responsibilities, along with effective team communication, are factors that can prevent human errors and enhance care quality during transport.
The third component of the present instrument, “Tools and Technologies,” consists of 6 items addressing the characteristics of equipment and tools used in the transport process, including reliability, alignment with needs, efficiency in patient monitoring, and preservation of patient privacy. Equipment used in transport can support patient safety only if it is reliable, efficient, and suited to transport requirements. Nurses feel greater safety and control over the transport process when the tools employed possess desirable technical quality. Equipment such as monitoring devices, alarm systems, infusion lines, and tubes must be designed and selected to align with specific transport conditions and environmental space limitations. These tools should enable precise and unobstructed monitoring of vital signs and critical patient systems by nurses.8,53,54 Preserving patient privacy during the transport process is of high importance and is often influenced by technical and operational constraints and requirements. Nevertheless, from the perspective of nursing professional ethics, it plays a key role in care quality and patient safety. Utilizing appropriate equipment effectively contributes to maintaining patient dignity, respect, and psychological comfort for the patient and family.16,55,56 Overall, the “Tools and Technologies” factor emphasizes that the quality and reliability of tools and technologies used in IHTs not only impact the safety and effectiveness of the care process but also affect patient comfort and privacy. Therefore, it is recommended that clinical managers and medical equipment officials pay special attention to reliability, ease of use, and alignment with ICU nurses’ operational needs when selecting and updating transport equipment.
The fourth component of the instrument, “Environment,” directly influences the safety and quality of IHTs for patients in ICUs. This factor includes four items addressing the physical characteristics of the transport location, such as hospital and ICU layout, destination room design, and unobstructed pathways. Appropriate design and layout of hospital spaces, including ICUs and destination rooms, play a vital role in facilitating safe transport processes. Unobstructed pathways and sufficient space for patient transfer are key factors in reducing environmental risks during transport.5,49 Accordingly, it is suggested that in hospital space planning and design, particularly for ICUs and transport pathways, special attention be given to eliminating physical barriers to ensure the transport process is conducted with minimal risk and maximum security for patients and staff.
In the present study, in addition to EFA, CFA was also performed, based on which the four-factor structure was examined and confirmed in the study sample. Each item loaded onto one presumed component. Furthermore, fit indices for the instrument were calculated, and the values indicated good model fit. Consistent with these findings, in the study by Li et al. (2024), 15 which examined the cultural validity of this instrument in China, the CFA results indicated satisfactory fit indices for the four-factor model (CFI = 0.943, IFI = 0.943, GFI = 0.845, CMIN/DF = 2.765). These results demonstrate that the relationships between items and dimensions are consistent. 57
In the present study, internal consistency was assessed using two statistical indices: Cronbach’s alpha and McDonald’s omega (ω). The obtained values for Cronbach’s alpha and ω were 0.891 and 0.877, respectively, which fall within an acceptable range and indicate adequate reliability of the Persian version of the IHTSS. The original version of the scale also reported acceptable reliability levels, with a Cronbach’s alpha of 0.88 for the entire instrument and subscale alphas ranging from 0.72 to 0.82. 14 Similarly, in the Chinese version, 15 Cronbach’s alpha coefficients for the four factors ranged from 0.89 to 0.95, with an overall α of 0.97. Additionally, other indices such as split-half reliability (0.90) and test-retest reliability (0.85) confirm the instrument’s high temporal stability. Overall, these results indicate that the IHTSS, in its Persian, Swedish, and Chinese versions, possesses a high level of reliability. Accordingly, the Persian version of this instrument can be utilized as a valid, reliable, and culturally adapted tool for assessing IHT safety for critically ill patients in the Iranian context.
Finally, it should be noted that the structure of the IHTSS for critically ill patients is multidimensional, comprising independent yet interrelated components. This structure aligns with human factors engineering models and the “Systems Engineering Initiative for Patient Safety” framework, which emphasize the complexity of work systems in care environments. 14 Similar to many developing countries, intensive care nursing in Iran is experiencing rapid growth and development, with enhancing safety for critically ill patients emerging as a key priority in the health system. In this regard, managing safety in IHT processes is a critical point in care, directly linked to patients’ clinical outcomes and family satisfaction levels. 55 The IHTSS can serve as a comprehensive, standardized, and psychometrically sound instrument, providing a valid framework for evaluating IHT safety.
Limitations and future research directions
This cross-sectional study employed convenience sampling to evaluate the psychometric properties of the IHTSS among nurses working in ICUs at a medical university in western Iran. Given the sampling nature, the generalizability of findings to other regions with differing cultural, structural, and organizational characteristics is limited. Additionally, the use of self-report questionnaires as data collection tools may introduce response biases and affect result accuracy.
Future studies are recommended to validate the Persian version of the IHTSS across broader and more diverse cultural and institutional settings. In particular, measurement invariance testing should be conducted across key demographic and professional subgroups (such as gender, educational level, and ICU type) to determine whether the scale functions equivalently across these groups. Moreover, known-groups validity testing is suggested by comparing nurses from ICUs with established, formalized IHT protocols to those from units without such protocols. To strengthen the generalizability of the findings, multi-site replication studies are also recommended, involving hospitals from different provinces and healthcare systems in Iran. Finally, future studies could explore the development of adapted tools or methodologies to capture patients’ perspectives, allowing a more comprehensive assessment of IHT safety from both the provider and patient viewpoints.
Implications for healthcare education and practice
The findings of this study indicate that the Persian version of the IHTSS for critically ill patients is a valid instrument adapted to the Iranian cultural context and can be employed to assess and enhance transport safety in ICUs. Utilizing this tool enables precise identification of areas for improvement and the design of targeted educational and managerial interventions. Focusing on organizational factors, including adequate staffing, proper scheduling, and effective team coordination, along with enhancing teamwork skills and proper execution of transport-related tasks, can significantly reduce human error risks. Furthermore, updating and ensuring equipment quality, as well as attention to appropriate environmental design, are key requirements for guaranteeing safe transport.
Conclusion
The present research aimed to localize, validate, and psychometrically evaluate theIHTSS in the Iranian cultural context among nurses working in ICUs. The psychometric analysis findings led to the identification of four key factors in assessing IHT safety: “Organization,” “Teamwork & Transport-related Task,” “Tools and Technologies,” and “Environment.” The obtained factor structure, considering cultural and linguistic differences, demonstrates adequate construct validity for the Persian version. Given the critical role of safety in transporting critically ill patients, employing the IHTSS can serve as an effective tool for monitoring the current status, identifying improvement areas, and designing educational and managerial interventions at the health system level. Moreover, using this scale can facilitate interventional studies and ultimately contribute to enhancing care quality and improving clinical outcomes for critically ill patients.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261416822 – Supplemental material for Psychometric properties of the Persian version of the intra-hospital transport safety scale in intensive care
Supplemental material, sj-docx-1-smo-10.1177_20503121261416822 for Psychometric properties of the Persian version of the intra-hospital transport safety scale in intensive care by Azam Sharifi, Amir Jalali, Keyvan Moradi, Leila Moradi, Jalal Karimi, Keivan Babaei and khalil Moradi in SAGE Open Medicine
Footnotes
Abbreviations
Content Validity Index (CVI); Content Validity Ratio (CVR); Kaiser Meyer Olkin (KMO); Exploratory Factor Analysis (EFA); Confirmatory Factor Analysis (CFA); Tucker-Lewis Index (TLI); Normed Fit Index (NFI); Goodness of Fit Index (GFI); Root Mean Square Error of Approximation (RMSEA); Principal Components (PC); Standardized Root Mean Square Residual (SRMR); Kermanshah University of Medical Sciences (KUMS).
Ethical considerations
Ethical endorsement was secured from the Ethics Committee of Kermanshah University of Medical Sciences (approval code: IR.KUMS.REC.1403.652., Date: 2025-02-26). Written permission for instrument utilization was obtained from its originator.
Consent to participate
All participants provided written informed consent, and the study adhered to the tenets of the Declaration of Helsinki. Research procedures conformed to pertinent ethical guidelines and regulatory frameworks.
Consent for publication
Not applicable.
Author contributions
Amir Jalali: conceptualization, methodology, investigation, validation, formal analysis, supervision, visualization, project administration, resources, writing—original draft, writing—review and editing. Khalil Moradi and Azam Sharifi: conceptualization, methodology, investigation, validation, formal analysis, supervision, visualization, project administration, resources, writing—original draft, writing—review and editing. Keivan Babaei, Keivan Moradi, Leila Moradi and Jalal Karimi: investigation, validation, formal analysis, visualization, project administration, data curation, software, resources, writing—original draft, writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the faculty members of the Research Committee of Kermanshah University of Medical Sciences. This research project has been registered with code 4030954 at Kermanshah University of Medical Sciences, Iran.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Clinical trial number
Not applicable.
Consent
All nurses received detailed information about the study and provided written informed consent before completing the questionnaires.
Patient consent
Not applicable
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.