
Abstract
Recent clinical practice guidelines recommend analgosedation in intensive care unit patients, where the patients' pain first is relieved, followed by sedatives only on indication. The aims of the present study was to examine sedation practice today, to evaluate the degree to which there is a difference in sedation practice between units, and to investigate the associations between nurses' demographic characteristics and their perception of sedation practice. A cross sectional survey was conducted to the nurses in three intensive care units in Norway. The results indicated that light sedation was implemented in the three intensive care unit studied. Continuous infusion of propofol and dexmedetomidine were used most frequently, and continuous infusion of midazolam was used occasionally. However, the sedation practices varied significantly between the units. Subjective scoring systems, physician's prescriptions, and prescription follow-up were reported to be most frequently used as guidelines and directives, and Richmond Agitation–Sedation Scale was reported to be the most frequently used sedation assessment tool.
Keywords
Introduction
Mechanically ventilated patients in intensive care units (ICUs) experience pain,1–3 anxiety, and discomfort.4,5 Traditionally, ICU patients haven been sedated to a deep levels of consciousness, 6 which made it difficult to assess intensive care patients cognitively. 7 However, there is now solid evidence that deep sedation is associated with longer ICU stays, more infections and higher mortality compared with light sedation.7–12 Therefore, clinical practice guidelines recommend analgosedation, where the primary goal is to relieve the patients’ pain, followed by sedatives only on indication. The aim is to have a more alert patient who is able to both mobilize and communicate during their ICU stay.12,13 However, healthcare professionals continue to disagree regarding whether this sedation strategy is a humane treatment for ICU patients.14,15 Some healthcare professionals even ask whether patients might suffer.16,17 Culture and context can affect the perception of what is the best treatment for an intubated and mechanically ventilated ICU patient. 18 Although several studies have suggested different methods to educate clinicians in this approach, 19 changing staff behaviour remains a challenge in clinical practice.19,20
In a recent study, Holm and Dreyer interviewed ICU patients 1–2 days after extubation. 21 Patients received light sedation during mechanical ventilation. The study showed that the tube in the mouth and the feeling of being drugged but still conscious bothered the patients. Prime and colleagues interviewed 16 former ICU patients, treated under an analgosedation protocol. 22 Most of these patients experienced pain, and half experienced discomfort during the treatment. Half of the patients preferred to be awake and to be able to communicate. In addition, in interviews with more lightly sedated patients in Denmark, it was learned that the patients were satisfied with being more in control and being able to cooperate with the nurses. 23
In 2007, Wøien and colleagues evaluated sedation practices in Norwegian ICUs. 24 Findings from this study contradict international recommendations from 2013 regarding sedation practice. 13 Respondents listed propofol (69%) as the most common sedatives used in their ICU, followed by midazolam (54%). Dexmedetomidine (i.e. a short-acting drug) was less used as a sedative. This finding is consistent with other surveys conducted in the same time period in Denmark, 25 Sweden 26 and in other European countries. 27 However, during the past 13 years, there has been a change regarding the choice of sedatives. In line with international guidelines, dexmedetomidine now appears to be used more frequently in countries such as Norway, 28 the United Kingdom 29 and elsewhere in northern Europe. 30
The implementation of nurse-led protocols and guidelines for sedation and the use of sedation assessment tools result in more alert patients;13,31 nevertheless, multi-centre studies have demonstrated a wide variation in the adherence to these protocols and guidelines. For example, nurse-led protocols and guidelines for the use of sedatives or analgesics were implemented in 29% of the ICUs in Canada, 32 in 36% of the ICUs in France 33 and in 64% of the ICUs in the USA. 34 Sedation assessment tools were used by 31% of the nurses and 44% of the physicians in Denmark, 25 52% of the anaesthesiologists in Germany 35 and 88% of the anaesthesiologists in the United Kingdom. 36
New research exploring sedation practice is needed to evaluate whether sedation practice has changed in recent years. In Norway, sedation practice has not been mapped since 2007 24 and 2008. 37 Therefore, the purpose of this study was to examine: 1) the extent to which light sedation is practised, and 2) the extent to which guidelines and assessment tools have been implemented in clinical practice in Norway. Moreover, we aimed to examine the association between the demographic variables of the nurses and their perception of practised sedation, and the degree to which there is a difference between units.
Methods
Design
The study had a cross-sectional design, using a questionnaire to explore sedation practice in three general ICUs at three different hospitals in Norway.
Setting
ICU A was located at a university hospital with 10 ICU beds, ICU B was located at a central hospital with eight ICU beds, and ICU C was located at a central hospital with five ICU beds. All three units treated both medical and surgical ICU patients. However, ICU B and ICU C did not treat neurosurgery or thoracic surgery patients. In all three ICUs, intensivists or specialized critical care physicians oversaw all patients. The nurse/patient ratio was 1:1, and most of the nurses had a master’s degree in critical care nursing. The survey was conducted in Norway, which is a country with well-developed public welfare systems, where there is interdisciplinary cooperation between nurses and critical care physicians.
To be able to evaluate the variation in sedation practice in each ICU, all nurses employed at these three units were asked to participate in the study and to answer a paper-based questionnaire. The study was conducted from October 2015 to February 2016.
Instrument development
The questionnaire in the present study was developed based on questionnaires used in two previous Norwegian studies24,37 on nurses’ and physicians’ practice in the assessment of the analgesic and sedative needs of mechanically ventilated ICU patients. Originally, these two questionnaires were translated and modified versions of a questionnaire conducted by Egerod and colleagues. 25 From the two Norwegian questionnaires,24,37 questions regarding practice of sedation, administration of medications, use of guidelines and directives and use of sedation assessment tools were used in the present questionnaire. Questions regarding pain, indication for sedation, and procedures for the sedation of different ICU patient groups were removed, according to the aims of our study.
To test for content validity, five nurses employed at an ICU pilot-tested a draft of the questionnaire. They answered questions about the wording of the questions, the response categories, the content (e.g. comprehensiveness of questions, potential content covered by items), time used to complete the questionnaire, and if they had qualifications needed to answer the questionnaire. The results from the pilot test led to minor changes in the wording of the questionnaire and its layout. The final version of the questionnaire consisted of the following items:
Practice of sedation and administration of sedative medications included questions regarding the use of different sedative medications (propofol, midazolam, dexmedetomidine) and use of different forms of administration (continuous infusion, bolus without fixed intervals, bolus with fixed intervals). These response categories were scored on a five-point Likert scale, and the response categories were: never, to a small degree, occasionally, often, and always. In addition, the nurses were asked to answer this statement: ‘In this unit, medication for pain is used as a basic, and medication for sedation is given just on indication’. Here, the response categories were: disagree, slightly disagree, unsure, slightly agree, and agree.
Use of guidelines and directives included questions regarding the use of written sedation protocols, use of different subjective scoring systems (e.g. Richmond Agitation–Sedation Scale) 38 and use of objective scoring systems (e.g. Bispectral Index). 39 The nurses were also asked whether target sedation level was ordered every day (physicians’ prescription), whether sedation level was routinely documented/evaluated and/or followed up (prescription follow up), and whether daily awakening (daily sedation discontinuation) was routine. Here, the response categories were: never, to a small degree, occasionally, often, and always.
Use of sedation assessment tools included questions regarding the use of the Motor Activity Assessment Scale (MAAS), 40 the Richmond Agitation–Sedation Scale (RASS), 38 the Glasgow Coma Scale (GCS), 41 and other sedation assessment tools. Here, the response categories were: never, to a small degree, occasionally, often, and always. In addition, the questionnaire comprised demographic data (i.e. gender, age, and working experience as nurse at the ICU).
Data collection
Paper questionnaires were distributed to 221 nurses employed at the three ICUs included in the study. The first author or a study nurse distributed the questionnaires during the unit’s education days. All nurses employed at the units were asked to fill in the questionnaire, except for the leaders and those who did not participate in the education days (i.e. due to illness). After the nurses had filled in the questionnaires, the forms were returned via a sealed box at each unit.
Analysis
Descriptive statistics, including numbers and percentages, were used to present the data. A chi-squared test was used to compare positive responses (i.e. reported answers = often/always, except for use of lighter sedation where reported answer = slightly agree/agree) to each survey item between the three ICUs, because the data were not normally distributed. The association between demographic variables of the nurses and the use of light sedation was assessed using multiple logistic regression analyses, to obtain odds ratios (ORs) and 95% confidence intervals (CIs). Statistical significance was set at p ≤ 0.05. A statistician controlled all analyses.
Age was dichotomized at the median value, with 0 representing 24–46 years and 1 representing 47–64 years. Dichotomization of age was performed to examine whether there was different perceptions of sedation practice in the oldest group compared to the youngest group. We hypothesized that the younger had more up to date theoretical evidens om sedation compared to the older nurses. Work experience and age were highly significantly correlated (Person’s r = 0.763, p = 0.000). In the preliminary single logistic regression analyses (results not shown), work experience had no significant correlation with the outcome variable; therefore, it was removed from the multiple logistic regression analyses. Data were analysed using the Statistical Package for the Social Sciences (SPSS) version 23.0 (SPSS, Inc., Chicago, IL, USA).
Ethical considerations
The study was conducted in line with the recommendations of the Declaration of Helsinki, and based on written, willing, informed consent, anonymity and confidentiality. Chief administrators at the three ICUs approved the study. As only anonymous data were collected, no application was sent to the Regional Committees for Medical and Health Research Ethics in Norway as no approval was required. However, Norwegian Social Science Data Services approved the study (project number 44726).
Results
Demographics.

SD = standard deviation; ICU: intensive care unit.
Practice of sedation
Reported answers regarding lighter sedation, administration of medications, assessment tools, guidelines and directives (n = 193).
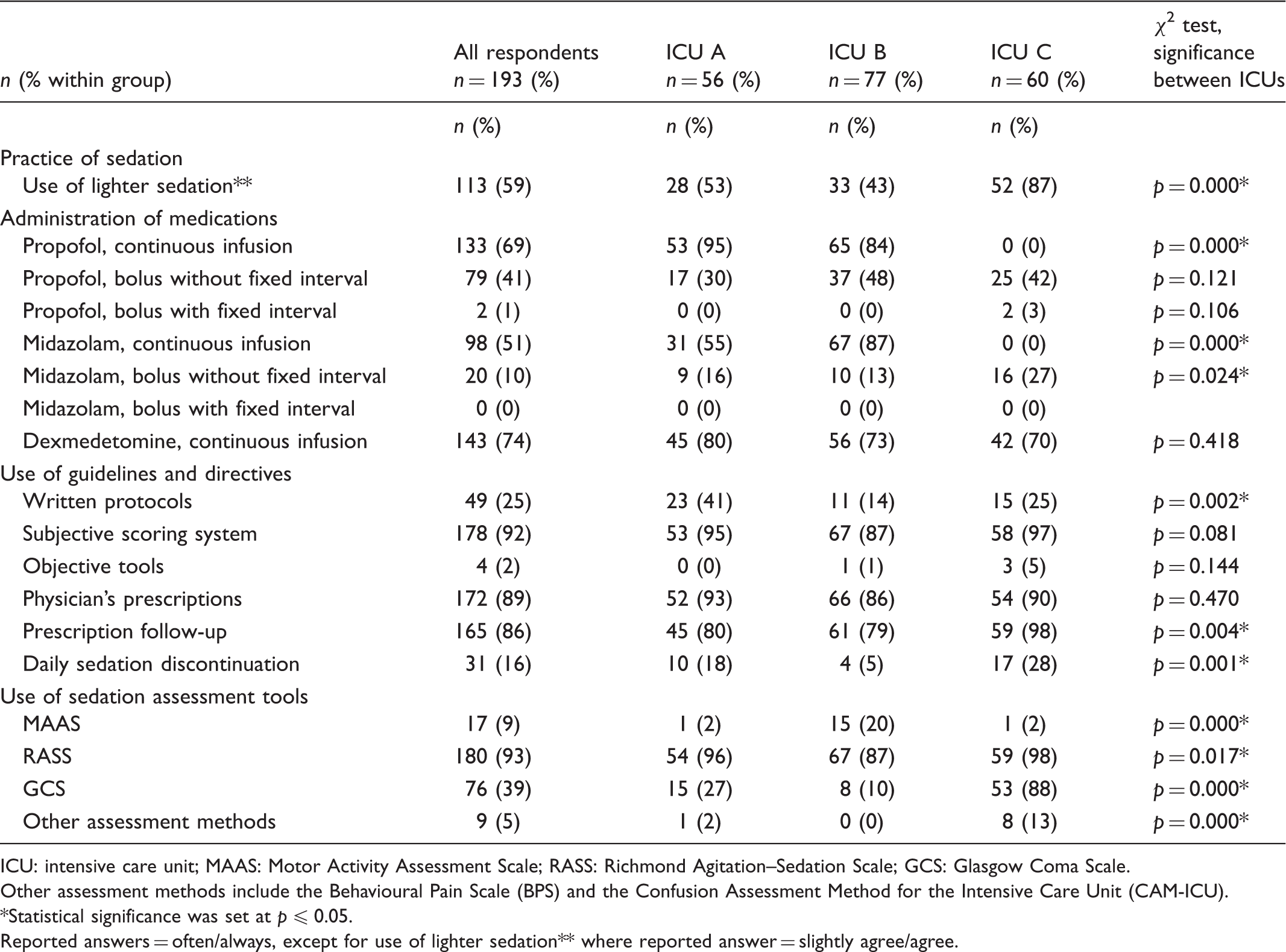
ICU: intensive care unit; MAAS: Motor Activity Assessment Scale; RASS: Richmond Agitation–Sedation Scale; GCS: Glasgow Coma Scale.
Other assessment methods include the Behavioural Pain Scale (BPS) and the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU).
Statistical significance was set at p ≤ 0.05.
Reported answers = often/always, except for use of lighter sedation** where reported answer = slightly agree/agree.
Administration of medications
Continuous infusion of midazolam (51%), propofol (69%) and dexmedetomidine (74%) was most often used. However, the use of midazolam (p = 0.021) and propofol (p < 0.001) varied significantly between the three units. In ICU A, 95% of the nurses reported that they often/always administered propofol as continuous infusion. In ICU C, 0% of the nurses reported that they administered propofol as continuous infusion. Of the nurses in ICU B, 87% reported that they often/always administered midazolam as a continuous infusion, while 0% of the nurses in ICU C reported that they often/always administered midazolam as continuous infusion (Table 2).
Use of guidelines and directives
The most frequently used guidelines and directives were reported to be subjective scoring systems (92%), physician’s prescriptions (89%), and prescription follow up (86%). However, regarding the use of prescription follow up, this varied between units from 79% in unit B to 98% in unit C (p = 0.004) (Table 2).
Use of sedation assessment tools
The Richmond Agitation–Sedation Scale (RASS) was reported to be the most frequently used sedation assessment tool (93%). However, the use of all four sedation assessment tools varied between the three ICUs (Table 2).
Associations between demographic variables and perception of practised sedation
Results of the logistic regression analysis for use of lighter sedation in own ICU (n = 193).
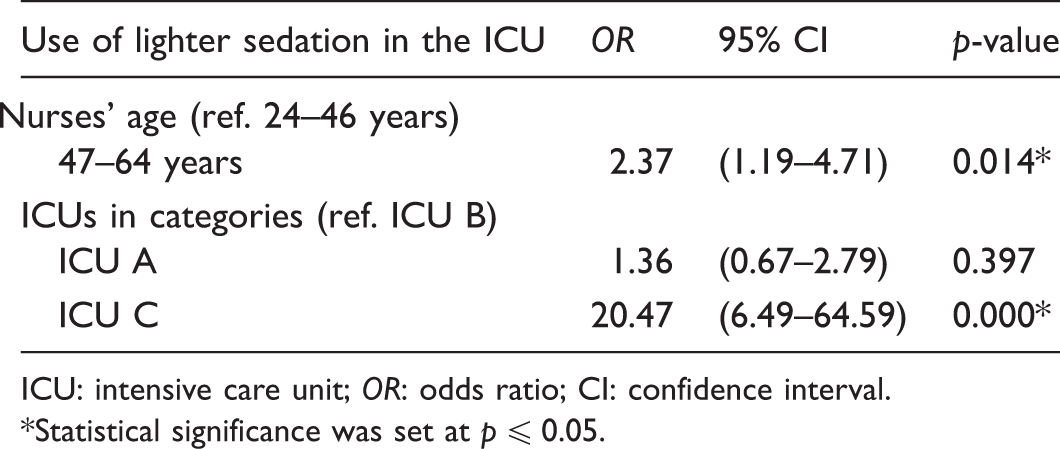
ICU: intensive care unit; OR: odds ratio; CI: confidence interval.
Statistical significance was set at p ≤ 0.05.
Discussion
This study provides information on current sedation strategies in three ICUs in Norway. Many nurses agreed that light sedation was practised in their unit. Based on nurses’ answers we found a significant variation between the ICUs regarding the practice of light sedation, defined as medication to relieve pain first and sedation just on indication. Continuous infusion of midazolam was used occasionally; propofol and dexmedetomidine were used more frequently. The nurses report that the use of both midazolam and propofol varied significantly between units. Subjective scoring systems, physician’s prescriptions and prescription follow up were reported to be most frequently used as guidelines and directives. The Richmond Agitation–Sedation Scale was reported to be the most frequently used assessment tool.
The response rate was high both at the university hospital and at the central hospitals. The nurses’ mean age and work experience were comparable at the three hospitals. Only critical care nurses responded to the questionnaire, as only critical care nurses work in these units. Thus, respondents appear to have a high level of experience-based knowledge as well as formal education-based knowledge. Moreover, the demographic distribution in the study is generalizable to the population of critical care nurses in Norway. 42
Findings from the present study indicate that light sedation, first pain relief and sedation on indication have been implemented to varying degrees in the three ICUs. This is supported by Sneyers and colleagues, who evaluated health professionals’ attitudes to light sedation, suggesting that practices for sedation vary between different regions and that the variation is related to health professionals’ attitudes to light sedation. 16 In addition, practices with sedation tend to differ depending on whether clinicians are familiar with the purpose of light sedation or not. It seems that a sedation practice that seeks to minimize the use of sedation will challenge clinicians, because patients experience discomfort in terms of pain1–3 as well as other types of discomfort.4,17 To implement a strategy of light sedation, Miller and colleagues found that health professionals’ knowledge of the purpose of keeping patients at a light sedation level is a key factor. 20
In the present study, dexmedetomidine was frequently administered at all three units – in line with the new guidelines. Previous studies have shown that propofol and midazolam were the sedative drugs most commonly used, while dexmedetomidine was less used.24,30 The finding in the present study is supported by Dahl and colleagues, 28 who found that the use of lighter sedation is more common. Both propofol and midazolam administration was reportedly frequently in use as a continuous infusion, but there was significant variation between units. The 2018 ‘Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU’ (PADIS) recommend using either propofol or dexmedetomidine rather than benzodiazepines for the sedation of critically ill mechanically ventilated patients. 12 A recently publicated literature review indicates that propofol and dexmedetomidine are similarly effective, thus they may both be used for sedation of mechanically ventilated patients in clinical practice. 43 The claim that dexmedetomidine reduces mortality and length of ICU stay is still controversial. Nevertheless, a recent study of dexmedetomidine shows it to be significantly related to lower mortality when compared with midazolam and propofol. 44 However, a recent study suggested that a gap still exists between clinical practices and current guidelines. Arroyo-Novoa and colleagues found in a study conducted in San Francisco that benzodiazepines were used for sedation in mechanically ventilated patients. 45
In the current study, nurses report that subjective scoring systems, physician’s prescriptions of sedation level and the prescribed sedation level follow up by the nurses are all frequently used directives in the three ICUs. An earlier study conducted in Norway suggested that written protocols and systematic assessments of pain and sedation were not routinely used in mechanically ventilated ICU patients. Moreover, only half of the ICUs in the study used subjective scoring systems to assess and titrate patients’ sedation level. 24 In the present study, all nurses, regardless of unit, reported that they frequently used subjective scoring systems. This finding may indicate that clinical practice in Norwegian ICUs nowadays is in accordance with international recommendations in this area.
Contrary to recommendations,12,13 findings from the present study showed that daily sedation stops and objective scoring systems were rarely used. Daily sedation stops refer to a period of time each day during which a patient’s sedative medication is discontinued and patients can wake up and achieve arousal and/or alertness. The present study indicates that daily sedation stops do not appear to be more frequently used in clinical practice nowadays compared to what was found in previous studies.24,37 Moreover, it is interesting that Mehta and colleagues 46 found that implementing a daily sedation stop practice in combination with a light sedation strategy did not reduce average ventilator time in ICU patients. Indeed, it was associated with increased need for sedation and pain relief. New guidelines published in 2018 recommend light levels of sedation. This light level of sedation can be achieved either through daily sedative interruption or by using nursing protocols. 12 Moreover, in a study from the United Kingdom, only 57% of the units reported having written sedation protocols. 29
In the present study, the Richmond Agitation–Sedation Scale (RASS) was the most commonly used sedation assessment tool, followed by the Glasgow Coma Scale, which is in accordance with international recommendations.12,13 In the study by Wøien and colleagues, half of the ICUs used the Motor Activity Assessment Scale (MAAS). 24 This finding is supported by a prospective study conducted in San Francisco, where only 52.5% of patients were within the recommended Richmond Agitation–Sedation Scale (RASS) scores. 45
Older nurses (47–64 years) report to a greater extent that light sedation was a strategy used in their own department compared to younger nurses (24–46 years). However, these results may also be related to work experience, as age and work experience are highly correlated in this study. Previous studies have shown that nurses with less work experience used mapping tools more systematically than nurses with more work experience. 37 One explanation of this finding may be the fact that nurses with less work experience are more dependent on guidelines, because of limited prior practice with conscious and ventilated patients. 25 Moreover, newly educated nurses with less work experience may also be more informed regarding new trends and strategies for treating ICU patients. Sneyers and colleagues found that the more experienced nurses did not use sedation scales to determine patients’ sedation levels because they had more confidence in their own assessment competence. 16 The absence of a common frame of reference and common designation contributes to a less precise level of desired and achieved sedation. Thus, the patient may be at risk of being more sedated than was intended.
Despite the fact that clinical practice to some degree appears to to have employed PADIS guidelines, there are still differences between clinical practice and clinical practice guidelines.12,13 For example, even if guidelines recommend the use of light sedation, a multi-centre prospective cohort study conducted in 45 Brazilian ICUs showed that 35% of ICU patients were nevertheless deeply sedated. 47 A comparable result was found in a German study, which reported that 27% of ICU patients still were deeply sedated. 48 Results from a recent study conducted in San Francisco show that 46% of mechanically ventilated patients were deeply sedated. 45 Clinicians have tried to implement a strategy for light sedation for almost 20 years. 12 However, they continue to struggle to implement this sedation strategy. The e-CASH approach (early Comfort using Analgesia, minimal Sedatives and maximal Humane care) attempts to meet these challenges. 49 This new, holistic approach may require a change in the culture of care. 49 To succeed in making such a change, it is important that all health professionals collaborate and work together as a team, keeping the focus on a good healthcare environment for each patient.17,49
Methodological considerations
The present study had some limitations. Because only three units were included in the study, the generalizability of the results may be limited. However, using three ICUs at three different hospitals may give a broad picture of sedation practice in one country. Moreover, the use of questionnaires as a single source of information has limitations, as the respondents interpret questions individually, and there may have been categories that were absent, thus preventing respondents from reporting their actual practice. Free-response items were lacking in the study, and this may have hindered the respondents in clarifying their answers. In addition, the questionnaire was only pilot tested, as no thorough reassessment testing has been performed on the form.
The response rate was 87%, which means that the findings in the study are highly representative of the group of nurses surveyed. In addition, the selected nurses were representative in terms of gender, age and work experience. 42 The innovative aspect in this study derives from the fact that the nurses worked at three hospitals with a large geographical distribution. Thus, this sample does not include nurses employed at the university hospitals in the capital city, as was the case for the samples included in comparable studies. 37 However, this survey was conducted within the context of a country with well-developed public welfare systems, where the nurse-to-patient ratio is 1:1. Nearly all the nurses in these ICUs have a master’s degree in critical care education, and there is interdisciplinary cooperation between nurses and anaesthetists.
Conclusion
Light sedation was implemented in the three ICUs studied, even though sedation practices varied significantly between the units. In the present study, continuous infusion of propofol and dexmedetomidine were used most frequently, and continuous infusion of midazolam was used occasionally. However, we found significant variations between units. Subjective scoring systems, physician’s prescriptions, and prescription follow up were reported to be most frequently used as guidelines and directives, and RASS was reported to be the most frequently used sedation assessment tool in all three units.
To succeed in the implementation of lighter sedation in mechanically ventilated ICU patients, comprehensive care should also be implemented in these patients to create a healing environment for the most critically ill patients. Otherwise, lighter sedation of this patient group may not be feasible.