
Abstract
Intensive care unit (ICU) nurses are expected to facilitate effective day-to-day communication with patients and family members at the bedside. To date, communication training for ICU health care professionals has targeted mainly intensivists-in-training, but there is limited data on communication experience and needs to be evaluated among ICU nurses. This qualitative study used focus group interviews to explore daily communication experiences with patients’ families and communication training needs and preferences among ICU nurses in South Korea. Five focus group interviews were conducted with 27 ICU nurses (4–6 nurses per group). The results of inductive qualitative content analysis highlighted four main categories: “Perceived difficulties during communication,” “burden from working conditions,” “endeavors to promote communication skills,” and “strategies for cultivating effective communication.” Regarding suggestions for future communication training, nurses preferred interactive learning with peer-support over traditional methods (e.g., lectures). Nurses also suggested that communication training for ICU nurses should include learning skills appropriate for difficult situations (e.g., angry family members). Findings from this study can serve as a framework for stakeholders in ICU care and healthcare education (e.g., hospital and nursing administrators, nurse educators) when designing communication training to support ICU nurses with their practical knowledge and communication skills.
Introduction
Effective family-clinician communication in the intensive care unit (ICU) is crucial to provide support, build trust, and promote outcomes and satisfaction for patients and families (Hamilton et al., 2020; Seaman et al., 2017). Unfortunately, many ICU patients cannot communicate due to the critical nature of illnesses and/or the effects of ICU treatments, such as mechanical ventilation and sedation (Karlsen et al., 2019). With these limitations, family members are expected to process complex updates about the patient’s illness and make decisions (Davidson et al., 2017). While physicians are usually responsible for delivering significant updates on medical care, ICU nurses are expected to help families understand patients’ daily conditions and to provide emotional support (Anderson et al., 2015; Newcomb et al., 2020; Pecanac & Schwarze, 2018).
Studies indicate that ICU nurses need better support to improve communication skills (Adams et al., 2017; O’Donnell et al., 2020). Schubart et al. (2015) reported that the major obstacles to efficient nurse-family communication were emotional arousal of families under stress, disjointed interactions between ICU teams and families, and limited resources and time. Studies also reported that role constraints in nurses made them less empowered to fill in the information gaps asked by families (Bloomer et al., 2017; Pecanac & King, 2019; Schubart et al., 2015). In an ethnographic study of ICU nurse-patient-family communication (Slatore et al., 2012), communication mainly was on updating patients’ biophysical information (e.g., vital signs), but rarely included the implications of the information. Nurses recognized the importance of their role as a communication partner and an intermediary between physicians and patients/families, yet nurses were also reluctant to be active in such roles (Slatore et al., 2012). Also, according to a multi-center survey with 199 ICU nurses in Korea, nurses rated their communication competence at a moderate level (Park & Oh, 2018).
To date, communication training for ICU clinicians has mainly targeted training physicians about leading formal family meetings (Scheunemann et al., 2011). Since most nurse-family communication occurs at patients’ bedsides (Au et al., 2019), training for ICU nurses may need a different focus. But, few studies to date have explored day-to-day challenges and needs from the viewpoints of bedside ICU nurses. To inform communication training for ICU nurses in Korean hospitals, conducting a qualitative study was crucial. Thus, this study aimed to (1) explore ICU nurses’ communication experiences with patients’ families and (2) identify nurses’ needs and preferences regarding communication training methods and content in South Korea.
This study is guided by the Facilitated Sense-making Model (FSM), a middle-range theory that presents a basis for family-centered critical care (Davidson, 2010). According to the FSM, ICU admission is a disruptive event for families who need to make sense of what has happened to the patient and the new roles expected of families (Davidson, 2010). Since nurses are the key facilitators of the sense-making process, the model suggests four intervention foci: caring relationships (e.g., building rapport between families and ICU clinicians), communication (e.g., effective delivery of updates), presence (e.g., inviting families to bedside activities), and decision-making (e.g., facilitating shared decision making) (Davidson, 2010). The FSM is relevant to our study because high-quality nurse-family communication is a key contributor to the success of each focus in the model.
Methods
Study Design and Setting
This qualitative study was conducted in a tertiary academic medical center in Seoul, South Korea. We conducted focus group interviews to generate rich discussion from participants with similar backgrounds but varying perceptions and reactions (Kreuger & Casey, 2014).
Study Sample and Recruitment
We enrolled 27 nurses who provided direct patient care from six adult ICUs. We excluded nurses working in ICU management. For recruitment, we posted flyers in the nurses’ lounge and visited each ICU to present the study and answer nurses’ questions.
Focus Group Interview and Data collection
We conducted five interviews (4−6 nurses/group) between November 2019 and January 2020. Each interview took place in a conference room for 50−60 minutes. We used a semi-structured interview guide with questions about ICU nurses’ communication with families and preferences regarding future training (e.g., “Tell us about your communication experience with patients’ family.” “Tell us what you wish to learn to improve communication with families.”). A facilitator (JJ or JC) opened each interview by presenting the purpose and asking participants to share their experiences and thoughts. At the end of the interview, the facilitator summarized the discussion and asked the participants to clarify the content. Interviews were audio-recorded, transcribed verbatim, reviewed for accuracy, and uploaded into the NVivo 11 (QSR International Pty Ltd., Victoria, Australia).
Ethics Statement
The institutional review board approved the protocol at Yonsei university (IRB number: Y-2019–0078). Written informed consent was obtained before the interview from each participant.
Data Analysis
Two investigators (JJ, JC) with extensive experience in qualitative methods analyzed data using inductive content analysis (Elo & Kyngäs, 2008). The episode of nurse-family communication was the unit of analysis. Each investigator repeatedly read the interviews and independently conducted open coding. In the weekly meetings, investigators reviewed and compared the codes and discussed discrepancies until a consensus was reached. Then, codes were grouped into categories. These categories were re-evaluated and grouped into higher-order categories. We paid attention to (1) the frequency of critical words, (2) the depth of the shared thoughts, (3) the extent to which individual experience was reflected upon, and (4) the observed group dynamics.
To assure trustworthiness, we used a guide from Elo and colleagues (2014). To secure credibility and dependability, a debriefing was conducted immediately after each interview. When new data was added, we compared/contrasted the categories found in each interview. For coherence (Morse et al., 2002), weekly meetings continued to verify categorization and abstraction consistency. For transferability, we used purposive sampling to ensure diversity in ICU experience (3 years or ≥3 years) and ICU types (medical or surgical). Two researchers scrutinized the reporting process to compare/contrast the nurses’ voices and categories presented.
Results
Sample Characteristics
Participants’ Characteristics by Focus Group.
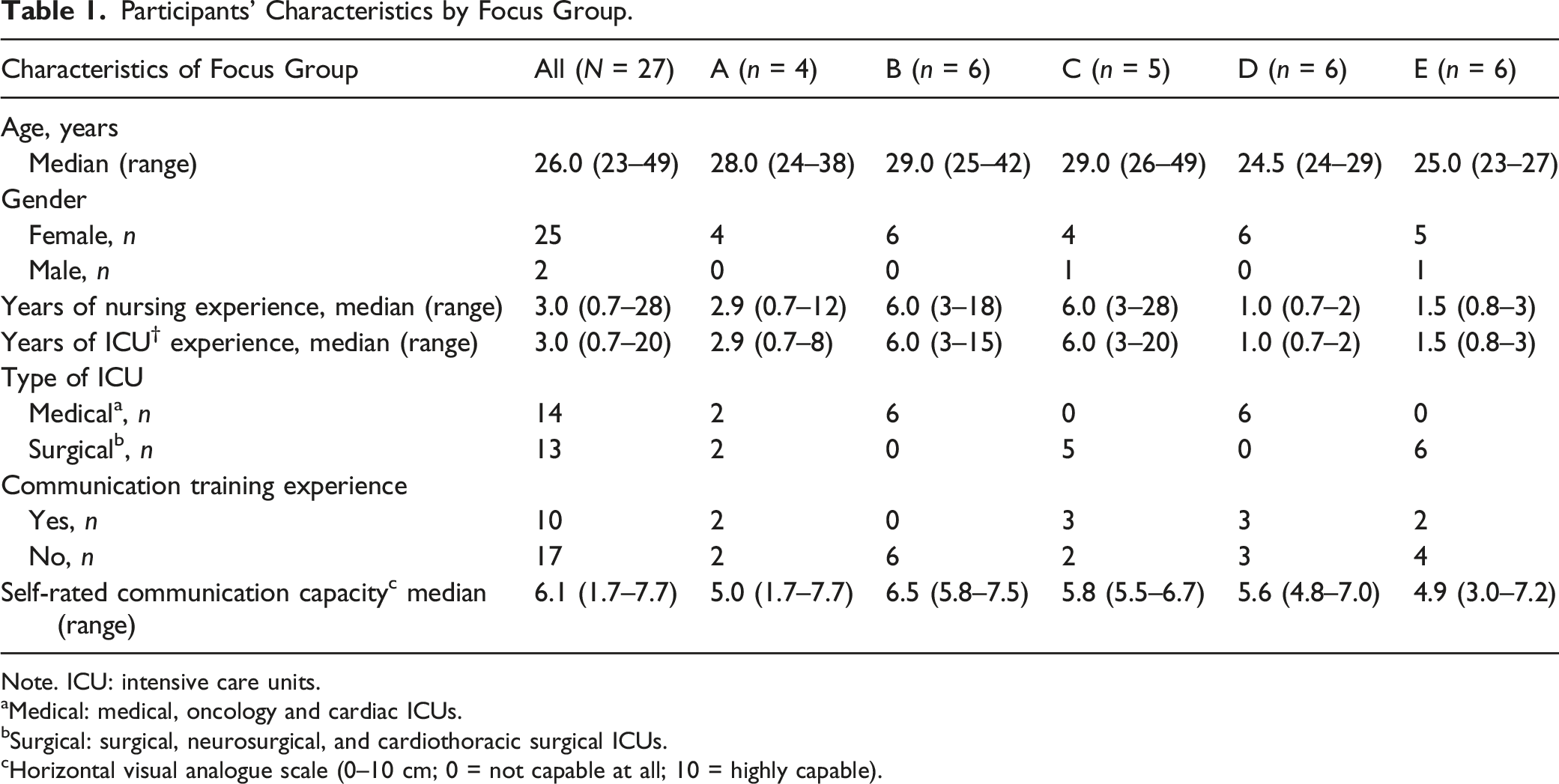
Note. ICU: intensive care units.
aMedical: medical, oncology and cardiac ICUs.
bSurgical: surgical, neurosurgical, and cardiothoracic surgical ICUs.
cHorizontal visual analogue scale (0–10 cm; 0 = not capable at all; 10 = highly capable).
Main Categories
Main Categories, Subcategories, and Sample Quotes About Challenges and Needs of Nurse-Family Communication as Perceived by Intensive Care Unit Nurses.
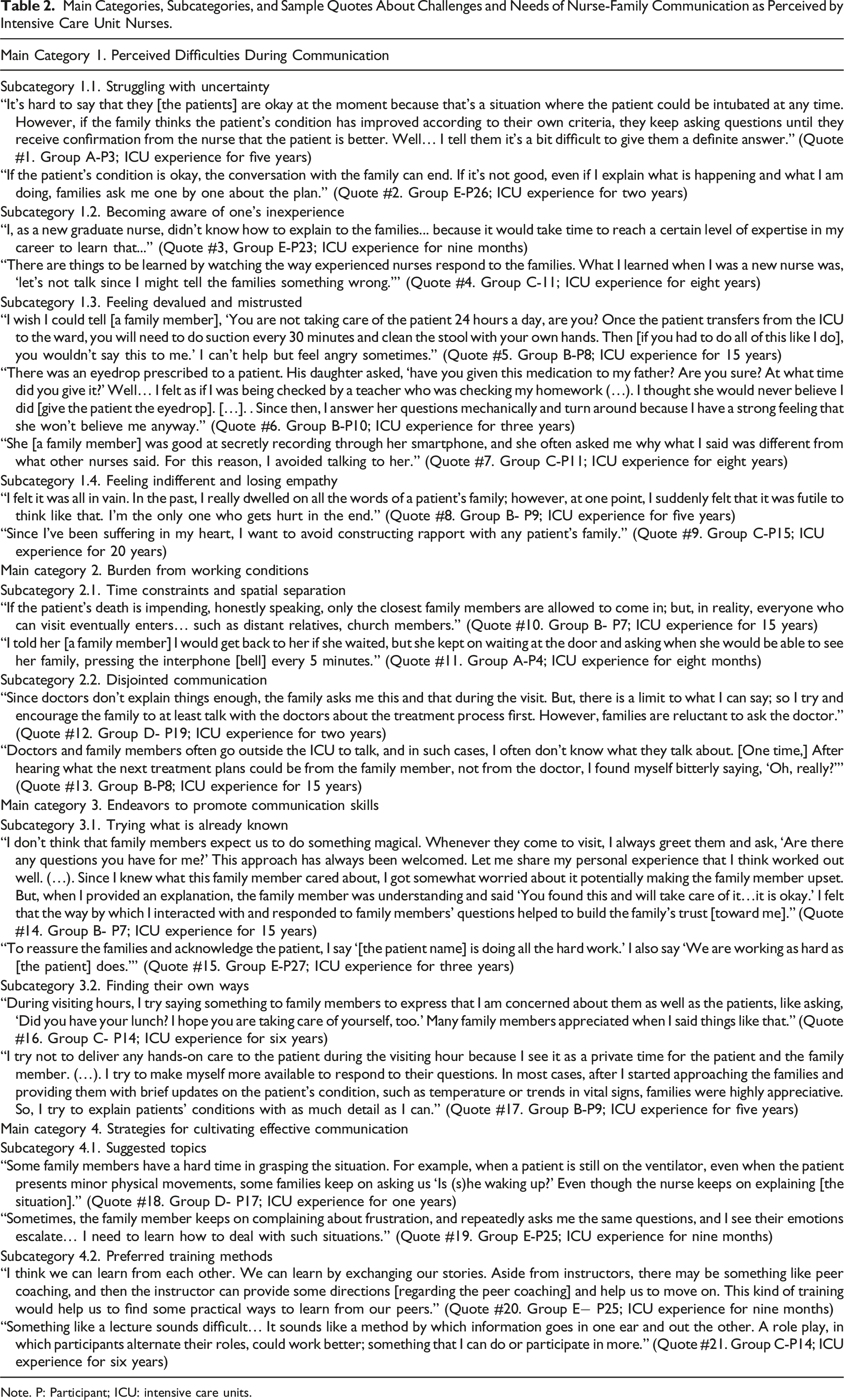
Note. P: Participant; ICU: intensive care units.
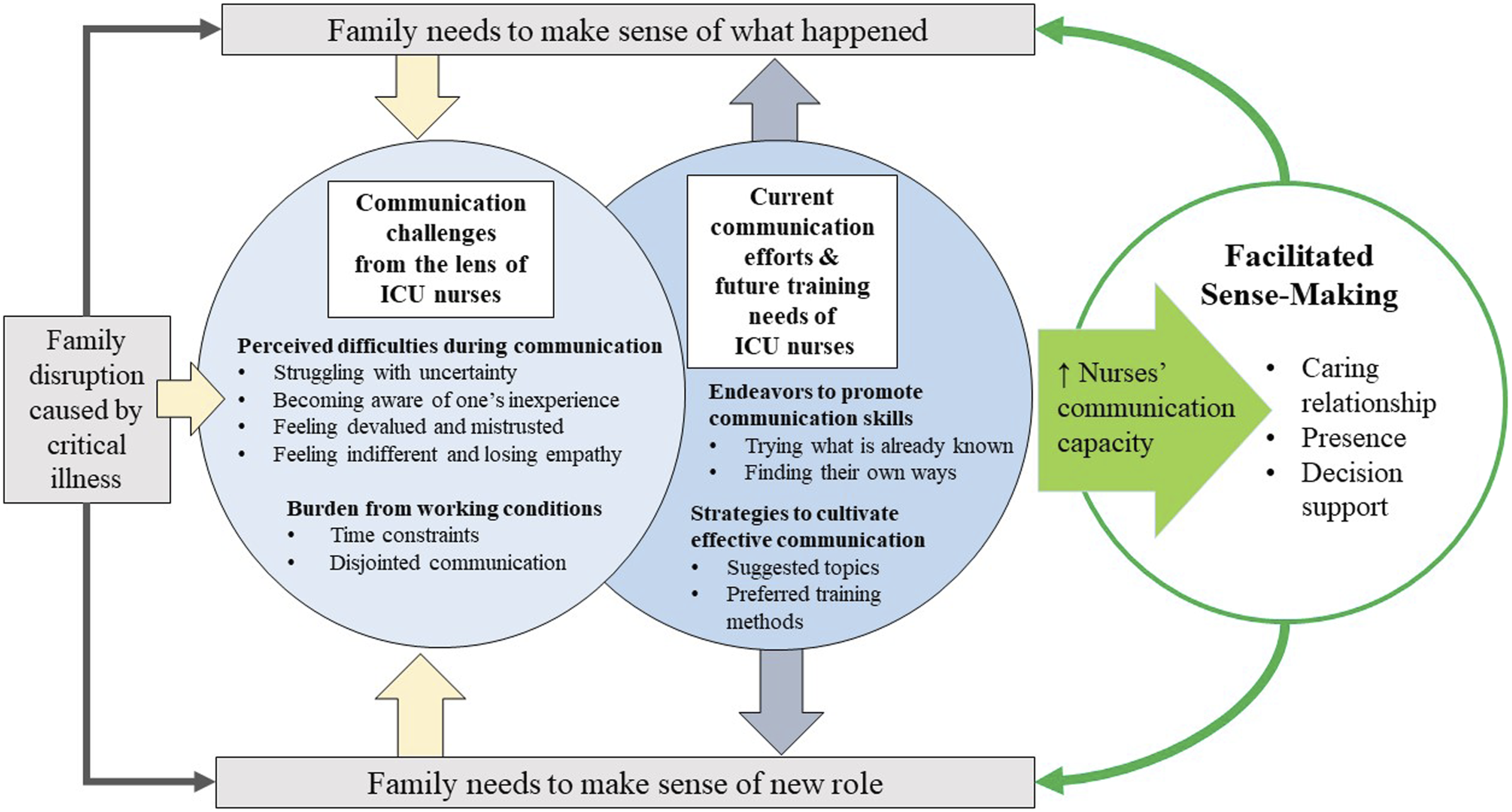
Intensive Care Unit Nurses’ Communication Experiences and Training Needs that Correspond to the Family Needs and the Focus of Facilitated Sense-Making Model.
Perceived Difficulties During Communication
This category illustrates nurses’ overall concern and emotions during nurse-family communication. These reactions led to self-doubt and avoidance behaviors.
Struggling With Uncertainty
Nurses were often uncertain about the level of detail to communicate to families. With uncertainty, nurses often had to keep their communication vague with little detail while making efforts to give hope to families (Table 2. Quotes #1 & #2).
Becoming Aware of One’s Inexperience
Nurses, especially new graduate nurses, stated a lack of confidence and experience to master communication with families. Ascribing such difficulties to a lack of clinical experience, some new graduate nurses said they either tried to avoid face-to-face contact with visiting families or relied on senior nurses (Table 2. Quotes #3 & #4).
Feeling Devalued and Mistrusted
Nurses stated, regardless of their efforts, families’ reactions were often harsh and filled with complaints on minor details that seemed irrelevant to patients’ overall safety and well-being. Nurses reported perceiving devaluation and mistrust often negatively affected the dynamics of the nurse-family interactions (Table 2, Quote#6). Nurses also shared disappointment when they noticed disrespect towards their work based upon unreasonable standards set by the families (Table 2, Quote #7).
Feeling Indifferent and Losing Empathy
Nurses said that experiencing disheartening situations repeatedly made them indifferent to family interactions. Nurses said it made them avoid direct nurse-family interactions unless necessary (Table 2, Quote #8 & #9).
Burden From Working Conditions
This category refers to structural factors unique to ICU settings and culture. These factors further complicated daily nurse-family communication.
Time Constraints
Nurses described that time constraints were often challenging during visiting hours. Since they were rushed to manage routine tasks, nurses often wanted to strictly enforce the visitation policy upon families; however, families resisted leaving patients’ bedsides. Despite the ICU policy limiting the number of visitors and visiting hours, nurses often felt pressured and reluctantly allowed additional visitors or extended visits (Table 2, Quote #11).
Disjointed Communication
Nurses said that physician-family communication was often not shared with nurses, causing communication breakdown. Sometimes nurses had to handle families’ dissatisfaction with the information from physicians (Table 2, Quote #12 & #13).
Endeavors to Promote Communication Skills
This category refers to how participants tried to apply communication skills at the bedside. Nurses used communication strategies that had worked in the past or some individualized support.
Trying What is Already Known
Nurses shared experiences that led to positive responses; for example, being silent around family members; verbalizing empowering words to family members; giving a light physical touch (e.g., lightly placing a hand on the family members’ shoulder while escorting them to the door). (Table 2, Quote #14 & #15).
Finding Their Own Ways
Nurses said that providing simple instrumental support helped calm families (e.g., physical space for grieving). When communicating about patients’ conditions, helpful strategies included giving daily updates (e.g., test results), inviting families to ask questions, or helping families learn basic hands-on care skills (Table 2, Quote #16 & #17).
Strategies for Cultivating Effective Communication
This category refers to suggestions for future communication training. Nurses acknowledged the need to learn more of the “how-to” to improve their communication.
Suggested Topics
Nurses highlighted skill gaps that were most problematic. For example, they wanted to learn simple phrases to support bereaved families. In addition, they suggested that communication skills to assist angry families would be valuable. (Table 2, Quote #18 & #19).
Preferred Training Methods
Nurses preferred using interactive formats (e.g., role play) and including peer support (e.g., sharing experiences and reflections) as training methods. Nurses agreed that lengthy readings or one-way lectures—regardless of mode of delivery—were less helpful except as Supplemental materials (Table 2, Quote #20 & #21).
Discussion
In this qualitative study, we explored nurses’ daily communication experiences with patients’ families among 27 ICU nurses in an urban tertiary academic medical center in South Korea. To the best of our knowledge, this study is one of the first that highlights gaps in communication skills expressed by Korean ICU nurses and preferences of communication training specific to bedside ICU nurses. Furthermore, we illustrated how our results support developing communication training for ICU nurses within the FSM (Figure 1). The categories that emerged in our data depict communication challenges from the lens of ICU nurses when they respond to the needs of family members who experience disruptions caused by patients’ critical illness. While dealing with these challenges, nurses were making efforts to help family members make sense of the situations and their new roles and were eager to learn more to cultivate effective communication. This finding justifies the importance of improving ICU nurses’ communication capacity to achieve the cores of the FSM and ultimately promote family-centered critical care.
Previous studies on ICU communication training primarily focused on training physicians to support structured family meetings and/or end-of-life decision-making (Mendez et al., 2020; Miller et al., 2016; Scheunemann et al., 2011). Because of the nature of nursing care, not every ICU nurse attends or facilitates family meetings; thus, these types of training may not be appropriate for nurses. Instead, ICU nurses are present at patients’ bedsides, and families are often influenced by daily communication with nurses (Au et al., 2019; Hamilton et al., 2020). Our findings provide viewpoints from bedside ICU nurses to guide interventions for nurses.
Cultural contexts unique in Korean ICUs contributed to our findings. Compared to Western countries, the length and flexibility of visiting hours are more restrictive, and families have limited control over the environment and access to information (Choi et al., 2021). Also, power differentials between professions and genders that are more prevalent in East Asia (Lee et al., 2021) may have contributed to the nurses’ uncertainty about sharing information with families. Assessment of cultural contexts may be necessary when interpreting communication self-efficacy rated by nurses in future studies.
In our results, the perceived difficulties during communication indicated that ICU nurses need better support to build communication self-efficacy. While individual differences existed, participants felt that their preparation and authority to communicate with family members was insufficient, which hindered their ability to fulfill families’ expectations. These results are consistent with a review by Adams et al. (2017) which called such a sequence “a vicious cycle.” Nurses first experienced emotional exhaustion due to constant feelings of devaluation and mistrust from families; subsequently, nurses noticed that these emotions negatively influenced their interactions with families; finally, these resulted in negative behaviors (e.g., avoidance). In our results, vicious cycles seem to negatively affect nurses’ overall emotional well-being as well.
Based on our findings, we recommend strategies to develop future communication training for ICU nurses that are practical and sustainable. First, given the family members’ experience of uncertainty and emotional distress, empathic communication skills must be the core of the training to help nurses effectively explore and respond to each situation. Learning to recognize emotion from verbal and non-verbal cues and expressing compassion will help build rapport and set a safe stage to communicate more complex topics (Moudatsou et al., 2020; Pehrson et al., 2016).
Secondly, our participants suggested using interactive learning (e.g., role play) rather than traditional approaches (e.g., lecture). Our participants liked the focus group format; they saw the group discussion as an opportunity to self-reflect, voice their experiences and concerns, and learn from each other. Thus, for future interventions, we recommend including small group activities and peer support, strategies used by oncologists (Bickell et al., 2020; Niglio de Figueiredo et al., 2018). Training a nurse champion may be a practical resource for nurses to enable unit-based communication training. The nurse champion can facilitate small group sessions that promote reflection of day-to-day communication experience and peer-learning. While evidence of the use of nurse champions in improving communication is limited (Miech et al., 2018), if successful, they have been effective in other unit-based implementation studies.
Thirdly, organization-level support and cultural changes are essential to sustain the benefits of communication training. Consistent with the report from a previous study (Schubart et al., 2015), time restriction was a structural factor that caused role constraints in nurses. Altering family visiting restrictions may be a way to resolve this concern. However, despite the prominence of open visitation internationally (Chapman et al., 2016), restricting in-person visits is often inevitable (e.g., global COVID-19 pandemic). Therefore, employing alternate strategies is imperative (Hart et al., 2020). For example, interventions using technology (e.g., short message services for updates) may help reassure families (Rodríguez-Huerta et al., 2019).
Lastly, institutions should treat the quality of nurse-family communication as a major element of family engagement in ICUs (Seaman et al., 2017). Developing unit-based information-sharing processes among ICU healthcare teams can help mitigate nurses’ reluctance to discuss patient information with families. Strategies to optimize the sharing of daily updates and goals between ICU healthcare teams and families may be a way to improve family-centered care (Justice et al., 2016; Seaman et al., 2017). Considering that most existing ICU communication training is “physician-centric,” future training needs a more interdisciplinary focus and increased nurse-family communication content (Slatore et al., 2012).
Limitations
Our study contains several limitations. First, we only interviewed bedside ICU nurses; thus, future studies should examine diverse viewpoints from other stakeholders (e.g., family members, ICU physicians). Second, although our participants had varied clinical experiences and came from multiple ICUs, they all worked at a single institution; therefore, interpretation should be made with caution due to limited representability. Last, our groups were homogenous (i.e., women in mid-20s to late 40s), thus hindering access to more nuanced insights.
Conclusions
Although communication is the foundation of patient- and family-centered critical care, the nurses in our sample admitted that time constraints and inefficient information sharing within the ICU healthcare team restricted their communication capacity. This study highlights the need for intervention development to assist ICU nurses in improving communication with families.
Footnotes
Author Contributions
Study design: JC. Data collection: JC, JJ. Data analysis: JC, JJ. Study supervision: JC. Manuscript writing: JC, JJ, YJS, JAT. Critical revisions for important intellectual content: JC, JJ, YJS, JAT.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (grant number 2019R1F1A1057941) and Mo-Im Kim Nursing Research Institute, Yonsei University College of Nursing.
Ethical Approval
This study protocol was approved by Yonsei University Health System Institutional Review Board (No. Y-2019–0078).