
Abstract
Background & Aim
The use of mechanical ventilation devices as a supportive respiratory system for hospitalized patients in intensive care units is often accompanied by the inability of alert patients to establish verbal communication. This study aims to determine the impact of patient communication software on facilitating communication for mechanically ventilated patients in the intensive care unit.
Methodology
This clinical trial was conducted with two groups, each comprising 60 alert, mechanically ventilated patients hospitalized in medical universities in Mashhad, from December 2022 to January 2023. Patients were randomly assigned to the intervention and control groups. In the intervention group, communication with the patient was established using specially designed software, while in the control group, conventional methods were used to identify patient needs. Data collection tools included a demographic questionnaire and the Ease of Communication Scale. SPSS software (version 20) was utilized for data analysis, employing chi-square, independent t-test, Mann–Whitney, Wilcoxon and paired t-tests. Cohen's d was also used to evaluate the magnitude of the effect size.
Results
The composition of the groups, including gender and marital status, was comparable, as was their baseline demographic and clinical characteristics (age, gender, education level, marital status, underlying diseases, airway type, hospital stay length, sedative medication, and mechanical ventilation duration), with no significant differences found (p > 0.05). Before the intervention, there was no difference in communication ease scores between the groups. Post-intervention, the intervention group showed significantly improved communication ease scores compared to the control group (P < 0.001) The Wilcoxon test results indicated a significant reduction in the average communication ease score after the intervention within both the intervention and control groups.
Conclusion
Software designed to assist communication for patients on mechanical ventilation with artificial airways could enhance their ability to communicate their needs more effectively, offering an alternative to methods such as lip-reading, writing, alphabet boards and communication boards.
Keywords
Introduction
Effective communication between healthcare providers and patients is essential for delivering high-quality care, especially in critical care settings. 1 However, patients who are mechanically ventilated often face significant challenges in verbal communication due to the presence of endotracheal or tracheostomy tubes, which prevent them from speaking. This inability to communicate can lead to increased levels of anxiety, frustration and a sense of isolation, as well as hinder the accurate assessment of patient needs and the delivery of appropriate care. 2 Addressing communication barriers for these patients is, therefore, a critical component of patient-centred care in intensive care units (ICUs).2–7 Consequently, these patients are compelled to resort to alternative communication methods such as lip reading and body gestures, writing, alphabet boards and communication boards.6,8 Therefore, the use of communication tools for mechanically ventilated patients in the ICU is essential for enhancing patient-centred care. Since these patients often cannot communicate verbally, various augmentative and alternative communication (AAC) interventions have been developed to facilitate interaction between patients and healthcare providers. The effectiveness of these tools is influenced by patient conditions, technology and nursing strategies. Low-tech options such as simple communication boards allow patients to point to symbols or words. However, studies have shown that these have limited message conveyance and lower satisfaction compared to high-tech options. 9
Extensive studies have been conducted to enhance communication methods with patients in the ICU, suggesting various communication tools and approaches, including speaking tracheostomy tubes, Family Meetings and Counselling, speech-generating devices, hearing devices and more.6,10,11 However, these methods have their limitations, such as high costs, restrictions on adding new capabilities, and not available for the patient. 11 High-tech solutions such as eye-tracking devices significantly improve communication effectiveness, enabling more messages and greater patient satisfaction 9 . Tablets with communication software also show promise, although their use is not yet systematic.12,13 Additionally, the use of AAC tools has been associated with reduced anxiety levels in mechanically ventilated patients and has a positive psychological impact. 14 Studies have shown that systematic training for nurses in the use of these tools leads to increased communication effectiveness and patient comfort.15,16–18 While the integration of technology in communication is promising, challenges remain, including patient fatigue and cognitive impairments that may hinder the use of tools. Balancing technology with personal interaction is crucial for effective communication in the ICU.
Therefore, various communication tools, ranging from simple picture boards to more advanced electronic devices, have been developed to assist patients who cannot speak. While some of these tools have been effective in facilitating basic communication, their application can be limited by factors such as patients’ physical or cognitive limitations, as well as the complexity and availability of devices.12,19 In recent years, advancements in digital health technologies have led to the development of applications specifically designed to enhance patient-provider communication. These applications offer features such as customizable interfaces, multilingual support and user-friendly designs that can meet the unique needs of mechanically ventilated patients. Despite these advancements, there is a lack of strong evidence from clinical trials to evaluate the efficacy of such software in real-world ICU settings. The present study aims to address this gap by investigating the impact of a patient communication software application on facilitating communication for mechanically ventilated patients in the ICU. This randomized controlled trial evaluates whether the use of this application can improve communication effectiveness, reduce patient anxiety and enhance the overall patient experience compared to standard care approaches. By providing empirical evidence on the effectiveness of digital communication tools in critical care settings, this study seeks to contribute to the development of more comprehensive and patient-centred approaches to caring for nonspeaking, mechanically ventilated patients.
Methods
Trial design
This study employed a randomized, two-group clinical trial design involving 60 patients. The study was conducted on conscious patients undergoing mechanical ventilation in the ICUs of Imam Reza, Qaem and Hashemi Nejad University Hospitals affiliated with Mashhad University of Medical Sciences. The study took place from December 2022 to January 2023 (Figure 1) and it followed the CONSORT checklist for reporting.

CONSORT flow chart of participants.
The setting for this study was Ghaem Hospital, which has a total of 60 active ICU beds, and Imam Reza Hospital, with 150 active ICU beds. Both hospitals are under the auspices of Mashhad University of Medical Sciences. The ICU unit specifically used for this study was the open-heart surgery ICU at Ghaem Hospital, which has 17 active beds. In this section, patients with underlying internal, neuromuscular diseases, and those needing ventilation are admitted. The typical nurse-to-bed ratio in these hospitals’ ICUs is usually 2 to 1 (at times, due to a shortage of staff, this ratio reaches 3 to 1). The Richmond Agitation-Sedation Scale (RASS) is also used for the sedation of patients in the ICU, where midazolam is the most common choice. For pain reduction in these patients, morphine, pethidine and methadone are commonly used.
Participants
Inclusion criteria encompassed having an artificial airway, proficiency in the Persian language, an acceptable level of consciousness (Glasgow Coma Scale score between 9 and 10, RASS = 0; ACVPU scale level A), age between 18 and 65 years, adequate visual and auditory capabilities, and basic literacy; the exclusion criteria included unwillingness to cooperate in any research stage and changes in the patient's level of consciousness to the extent that communication was no longer possible.
Intervention
Development of the communication application
In the initial phase, the researcher extracted effective communication themes for alert intubated patients undergoing mechanical ventilation by reviewing published research and consulting experienced nurses in the ICUs. Then, the content for software development was handed over to the software development and information technology teams. Following the creation of the initial software, it underwent expert validation by 10 IT specialists. The patient communication software was equipped with audio playback capabilities, display of schematic images and a typing feature, and it possesses visual appeal, flexibility, aesthetic appeal and quality. For example, each of the patients’ primary needs was visually presented on digital pages, with each image capable of being magnified and having audio added to it. Also, a schematic image of an overview of the body has been designed to show the location of pain. This software also has the ability to record and log the needs presented by the patients and can be installed on the researcher's phone? as a user of the software, which makes it possible to establish communication between the nurse researcher and the conscious patient who is unable to speak. The said software runs on the Android operating system and is in airplane mode to avoid harmful effects of waves on the electronic devices in the ward.
This software is an application provided to patients, allowing them to select options and view pictures to more easily communicate their problems to the nurse.
Patients do not need to use any additional devices to operate this software. They select items (such as hunger, thirst, etc.), and when a sound option is chosen, it is immediately played. Image, text, and voice features are included for user convenience (Figure 2).
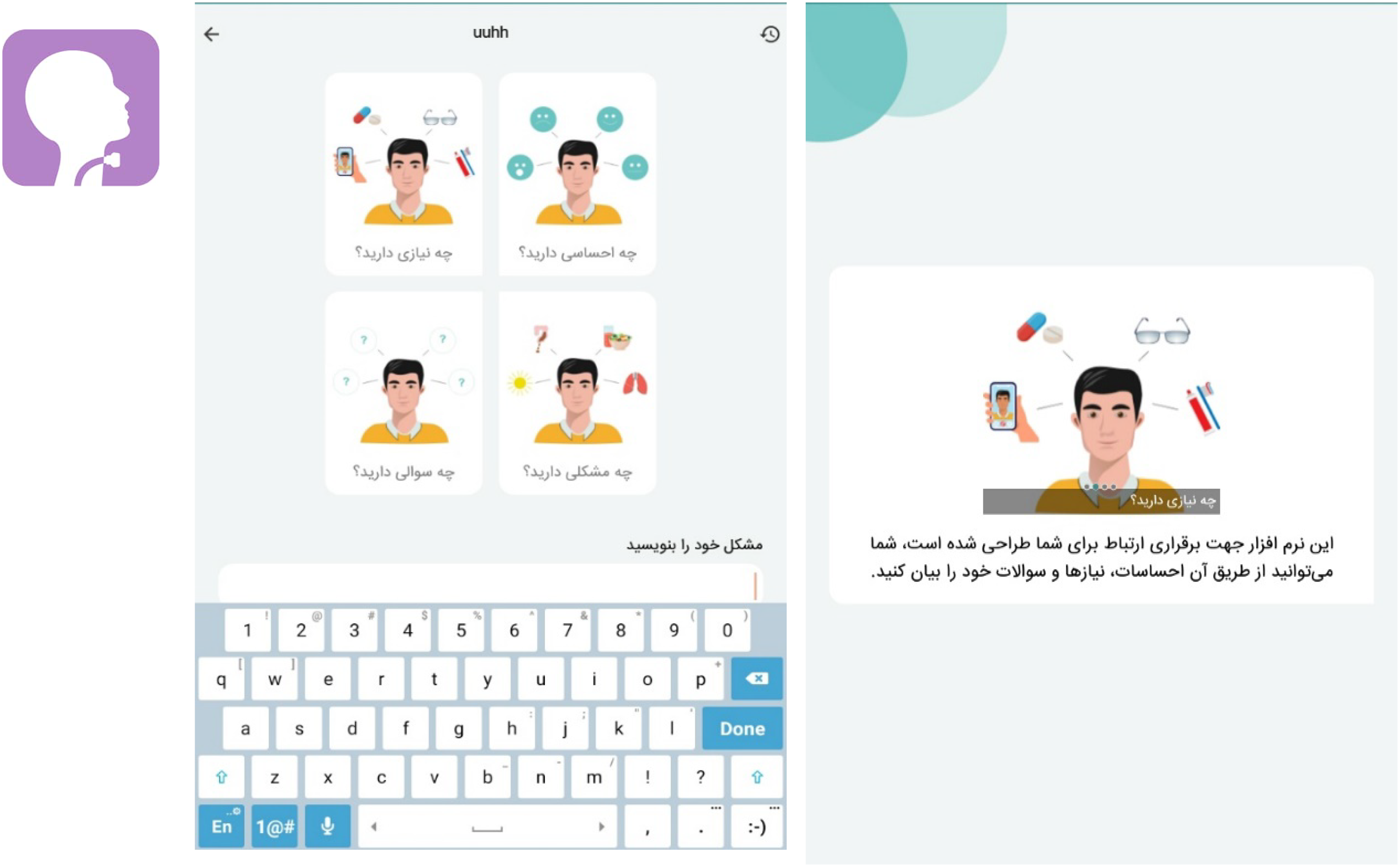
Application environment on mobile phone or tablet and screenshot.
Implementation steps
The intervention duration in this study was set at 12 h, taking into account the patient's stay in the ward and considering human biological rhythms that might give rise to various needs, such as thirst, warmth, cold, pain, etc. In the intervention group, communication was established using the developed software. In the control group, communication with patients was conducted through standard methods for identifying patient needs based on their condition. These methods included lip-reading, sign language, the use of pen and paper, and a whiteboard, allowing patients to express their feelings, needs and problems using the available communication tools. It is important to note that routine care procedures were identical in both groups over the 12-h period, and all patients in both control and intervention groups were cared for by the same nursing staff.
Outcome
Data collection tools included the sociodemographic questionnaire and the Communication Ease Questionnaire (ECS). The sociodemographic questionnaire gathered information on gender, age, education level, occupation, marital status, reason for hospitalization, underlying diseases, disease severity, receiving or not receiving sedation, type of artificial airway, length of stay in the ICU, length of hospital stay and duration of mechanical ventilation. The Communication Ease Questionnaire assessed the difficulty of communication in non-speaking patients using a 5-point Likert scale (0 = not difficult at all, 1 = slightly difficult, 2 = moderately difficult, 3 = very difficult, 4 = extremely difficult) for six questions. The communication ease score for patients unable to speak was obtained by summing the scores of six questions, with a score range of 0–24. Higher scores indicated greater communication difficulty. The Iranian version of this tool was validated for use in this study by Hosseini et al. in 2018. 20 In this study, the questionnaire was completed by 10 faculty members of the School of Nursing and Midwifery to confirm its applicability in the research community. The reliability of the questionnaire was assessed using Cronbach's alpha, which was found to be 0.94 based on evaluations by 10 participants. Before the intervention, the level of communication ease for both the intervention and control groups was assessed using the ECS questionnaire. At the end of the study, after 12 h, the ECS questionnaire was completed again for both groups through patient interviews (Supplemental material).
Sample size and randomization
The sample size was determined by 28 patients in each group based on the results of a pilot study on 10 participants in each group using the comparison of two means formula with 95% confidence interval and 80% test power. To ensure a more robust analysis in subgroup categories and considering a 10% attrition rate, 30 patients were enrolled in each group, resulting in a total of 60 patients for the study. After introducing the researcher to the patients, providing sufficient explanations regarding the research objective and methodology, and obtaining informed consent from the patients, the selected sample population was randomly allocated into control and intervention groups using a random sequence generated from the Randomizer.org website. Eligible individuals for participation in the study were included in the research environment after ensuring the confidentiality of their information and obtaining their informed consent.
A concealed allocation method was employed, where a sequence was written on small cards, and each card was placed inside a sealed packet. When a patient met the inclusion criteria, the sealed packet was opened, and the patient's group assignment was determined based on the code inside.
Statistical methods
After data encoding and entry into statistical software, descriptive statistics, including frequency distribution, mean and standard deviation, were used to describe the characteristics of the research sample. The normality of quantitative variables was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. For the assessment of homogeneity between the two groups and to examine the research objectives, the independent t-test was used for quantitative variables that followed a normal distribution and the Mann–Whitney test for quantitative variables that did not follow a normal distribution. For within-group comparisons, the paired t-test (normal distribution) or Wilcoxon signed-rank test (non-normal distribution) was employed. Cohen's d was also used to evaluate the magnitude of the effect size, calculated by standardized mean difference, with g > 0.2 to 0.5 = small effect size, g > 0.5 to 0.8 = medium effect size and g > 0.8 = large effect size. 21 A confidence level of 95% and a significance level of 0.05 were considered in all tests, and the analysis was conducted using SPSS version 21.
Results
The 70 patients were screened for eligibility in the study. After reaching the desired sample size, the sampling process was completed. Sixty alert mechanically ventilated patients were randomly assigned to two groups: intervention (n = 30) and control (n = 30) (Figure 1).
In the intervention group, 16 individuals (53.3%) were male, while in the control group, 15 individuals (50.0%) were male. The majority of patients in the intervention group, 23 individuals (76.6%), and in the control group, 22 individuals (73.3%), were married. The results of the Chi-squared, Mann–Whitney and Fisher's exact tests indicated that the two groups did not significantly differ in terms of variables such as age, gender, education level, marital status, underlying diseases, type of airway, length of hospital stay, receipt of sedative medication and duration of mechanical ventilation (p > 0.05), demonstrating their homogeneity (Table 1). Before the intervention, there was no statistically significant difference in the mean and standard deviation of communication ease scores between the intervention group (12.7 ± 3.5) and the control group (12.4 ± 3.3) (p > 0.05). However, after the intervention, the mean communication ease scores were statistically significant in the intervention group (7.7 ± 3.3) compared to the control group (11.0 ± 3.2) (p > 0.001), with the control group having lower scores (Table 2).
Demographic variables of the intervention and control groups.

**** Chi-square; *** Mann-Whitney; ** Fisher exact.
Mean and standard deviation of ease of communication in conscious patients under mechanical ventilation.

*Mann-Whitney; **Wilcoxon test.
In the intra-group comparison, the Wilcoxon test showed that the average score for ease of communication after the intervention had significantly decreased compared to before, both in the intervention group (P < 0.001) and in the control group (P < 0.001) (Table 2). All members of the intervention group successfully utilized the software. The intervention group used the application for an average of 30 min per day over the study period. The application's features that were most commonly utilized included sending text messages for expressing needs (e.g. pain, thirst, need for assistance), accessing predefined icons for common requests (e.g. turning, repositioning), and using audio recording for detailed communication when text was insufficient.
Discussion
This study investigated the impact of communication software on facilitating communication with alert, mechanically ventilated patients in the ICU. Our findings indicated that the use of communication software improved communication with these patients. Therefore, the researcher attempted to draw upon the results of other studies in this field. Results from Hosseini et al. (2018) in Iran demonstrated that a communication board is an effective method to facilitate communication and reduce stress in alert mechanically ventilated patients. 6 In our study, communication software also improved communication in alert, mechanically ventilated patients. Thus, innovative communication interventions can reduce communication difficulties and improve patient–nurse interactions, and their use has been recommended in multiple studies.6,22 Therefore, the results of Hosseini's study align with ours. The study by Trotta et al. (2019) showed that implementing communication assistance strategies between nurses and patients significantly improved communication. 22 Humans possess analytical and interpretive abilities, and difficulty in communication causes them distress. 3 To achieve dynamic and effective interaction in communication with ventilated patients, nurses need to constantly evaluate various aspects of communication. In our study, the communication software improved the perceived ease of communication between nurses and patients, according to the patients’ feedback. However, it is important to note that our study did not directly measure whether messages were accurately conveyed and received between nurses and patients. Therefore, Trotta's study results are in line with ours. The results of Sasmitha Das et al.'s (2015) study demonstrated that the use of a communication board improved communication ease in alert, mechanically ventilated patients. 23 Studies have shown that communication difficulties pose a significant challenge for nurses and patients in ICUs, emphasizing the need to choose and implement effective communication methods with these patients.8,22 In Sasmitha Das's study, a communication board reduced communication challenges. In our study, we utilized innovative communication methods to facilitate effective communication between patients and nurses. Therefore, the results of Sasmitha Das's study are consistent with ours. Rodriguez et al.'s (2017) study showed that using a specific communication tool improved communication in patients who suddenly lost their speech. 24 This communication tool included visual buttons with pre-recorded speech messages, a separate touch screen with finger or stylus input, and a separate keyboard for typing. The use of modern technologies, especially electronic tools and designed software, has been found to increase communication ease in patients who lack verbal communication abilities. 25
Electronic communication applications have the potential to improve patient care by enhancing communication between physicians and patients, increasing efficiency, expanding resources and saving time. 26 The use of communication technologies, such as electronic tablets and video communication, has been particularly relevant in acute-critical care settings, especially during the COVID-19 pandemic. 27 The study by E cox et al. (2024) showed the effectiveness of a mobile application-based primary palliative care intervention called ICUconnect for family members of critically ill patients in ICUs. This randomized clinical trial found that a mobile app-based primary palliative care intervention effectively reduces the unmet needs of family members of ICU patients. 28 In this study, Emilie Szymkowicz (2024) showed that the eye-tracking device (high-tech) may further improve the communication effectiveness of mechanically ventilated patients compared to the conventional communication board, both quantitatively and qualitatively. 9
Overall, electronic communication applications have the potential to empower patients, improve care coordination, and provide valuable information for healthcare providers in various healthcare settings. Accordingly, the communication software developed in our study, which offers features such as displaying zoomable schematic images, audio playback, precise body location selection based on anatomical images, as well as typing and recording patient-provided needs, can represent an innovation for facilitating communication with such patients. However, it is important to note that the software mainly facilitated basic communication needs of patients rather than the more complex process of therapeutic communication. Therapeutic communication involves deeper interactions, such as active listening and empathy, which require reciprocal engagement from both patient and healthcare provider. As our study did not analyze the specific content or complexity of the messages exchanged, it cannot conclusively state that communication extended beyond basic needs. The results of Wahidin et al.'s (2020) study indicated a significant relationship between therapeutic communication and postoperative patient improvement. 29 Nonetheless, comparing their findings with our results should be approached with caution, as their study context and the scope of communication differ.
Various case studies have shown that VidaTalk™ allows patients to communicate effectively despite the physical limitations imposed by medical interventions; however, some challenges persist, such as ensuring consistent usage by all staff members, adapting to individual patient preferences, and incorporating updates into the application based on user feedback.30,31
This study faced several limitations that may influence the interpretation of the results. One of the primary constraints was the variability in patient accuracy when responding to the questionnaire, which could stem from a range of factors, such as comprehension difficulties or misinterpretation of the questions. In addition, the psychological status of the patients at the time of the study could have a significant impact on how they responded to the questionnaire. For instance, patients experiencing anxiety or stress might interpret and answer questions differently compared to those in a more stable psychological state. These variations in psychological conditions could lead to inconsistencies in the data collected, thereby affecting the reliability and validity of the study findings. Moreover, such factors might also result in response bias, limiting our ability to draw definitive conclusions from the study outcomes. It is important for future research to take these limitations into account and consider methods for minimizing their impact.
Conclusion
The development of software designed to facilitate communication with conscious patients with artificial airways under mechanical ventilation has the potential to supplement existing methods, such as lip-reading, writing, alphabet boards and communication boards by providing an alternative mode of communication. Preliminary feedback suggests that such software may increase patients’ perceived ease of communication, allowing them to express their needs with less difficulty.
Supplemental Material
sj-doc-2-dhj-10.1177_20552076241299639 - Supplemental material for The impact of patient communication software app on facilitating communication with mechanically ventilated patients: A randomized clinical trial
Supplemental material, sj-doc-2-dhj-10.1177_20552076241299639 for The impact of patient communication software app on facilitating communication with mechanically ventilated patients: A randomized clinical trial by Zahra Poursadeghi, Kheizaran Miri, Fatemeh Hajiabadi, Seyyed Reza Mazloum, Javad Malekzadeh and Fereshteh Niazi in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241299639 - Supplemental material for The impact of patient communication software app on facilitating communication with mechanically ventilated patients: A randomized clinical trial
Supplemental material, sj-docx-3-dhj-10.1177_20552076241299639 for The impact of patient communication software app on facilitating communication with mechanically ventilated patients: A randomized clinical trial by Zahra Poursadeghi, Kheizaran Miri, Fatemeh Hajiabadi, Seyyed Reza Mazloum, Javad Malekzadeh and Fereshteh Niazi in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to all the nurses, doctors and patients who have cooperated in this study.
Availability of data and materials
The datasets generated in the current study are available from the corresponding author upon reasonable request.
Contributorship
All authors have read and approved the manuscript. Study design: ZP, FH, SRM; data collection and analysis: ZP, FH, JM, FN; manuscript preparation: KM, FH, SRM, ZP.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
The research was approved by the Research Ethics Committees of Mashhad University of Medical Sciences, Mashhad, Iran (no. IR.MUMS.REC.1401.074), and registered in the Iranian Registry of Clinical Trials with the code IRCT20220315054293N1. An official permission was obtained from hospital administrators to conduct the study. Informed consent was obtained from all subjects. Anonymity and confidentiality were assured through coding the data. Participants were assured that their participation was voluntary and they could withdraw from the study at any time without any penalty. All methods were performed in accordance with the relevant guidelines and regulations, which are aligned with the Declaration.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mashhad University of Medical Sciences.
Guarantor
FH
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.