
Abstract
Patient participation is is a highly valued goal within healthcare. The aim of this study was to assess the validity of a Finnish version of the Participation in Rehabilitation Questionnaire (FI-PPRQ) developed to measure patients’ perceptions of the importance and their experience of participation in care. The original PPRQ was translated from Swedish into Finnish, then subjected to psychometric pilot testing using data acquired in a cross-sectional survey with a sample of adult patients in eight primary healthcare units (n = 88). The importance and experience ratings were evaluated separately, by calculating distributions of item and scale scores, Cronbach’s alpha coefficients, and correlations between items and scales. In addition, experience ratings were subjected to exploratory factor and multi-trait scaling analyses. The results of this study support the validity and reliability of the instrument for use in clinical settings to provide information about patient participation. However, further studies are needed with more varied settings.
Keywords
Introduction
Patient participation is a highly valued concept in modern healthcare, and many Western countries, including Finland, have introduced healthcare strategies and legislation promoting it. Relevant Finnish laws include the Act on the Status and Rights of Patients 1 and the Health Care Act. 2 Participation is also based on ethical principles such as justice, dignity, integrity and autonomy, and a key justification for participation in healthcare is the right of individuals to influence matters that concern their own lives, and to receive services and care that correspond to their needs and values. 3
Patients generally seem to consider participation important and desirable,4–6 but their participation preferences and capabilities can differ considerably7–9 and they may also vary over time and from one situation to another.4,10,11 For example, some patients may not want to be involved in decision-making in a particular situation, but they may still value discussion about the options.7,12 Previously reported patients’ experiences indicate that perceived inability to participate may be due to feeling overwhelmed by illness,10,13,14 lack of knowledge4,10,14 and/or low self-confidence.10,14 Moreover, patients’ participation may reportedly be restricted by professionals behaving in ways that hinder it, for instance by demonstrating a lack of empathy10,14,15 or paternalistic attitude,5,14,16 and failing to take patients seriously or consider their views.9,15,17 Another frequently mentioned barrier to participation is lack of time.4,11,18
Thus, professionals can either promote or hinder patient participation through their actions.14,15,19 In previous studies patients have mentioned respect as a requirement for participation20–22 and emphasised the importance of access to adequate information and knowledge.4,10,20 It is important that patients feel confident in participating in their own care. This is enabled by respectful encounters that foster patients’ feelings that their willingness and capacity to participate in the particular setting and circumstances is seriously considered, and that they are being recognised as equals and individuals. 23
Participation has many advantages for patients, as it can improve satisfaction and motivation, 24 commitment to treatment,4,25 sense of security and control in care,4,5 patient–physician communication, 26 recall of treatment recommendations27,28 and management of chronic illness. 19 Moreover, increases in participation can improve patients’ perceptions of the quality of care received and contribute to reductions in medical errors and adverse events,29,30 thereby increasing safety.19,29,30 Thus, implementing patient participation is imperative for any healthcare system intending to provide patient-centred, high-quality and effective care.
However, although the importance and significance of participation have been internationally acknowledged, realising it in everyday practice is challenging,31,32 and patients’ reported experiences indicate that improvements in measures to promote it are required.16,33 Thus, there are needs for greater insight into optimal ways to implement participation in specific contexts, and more knowledge of patients’ experiences and preferences regarding participation. Further, although participation has been researched in recent decades, from both professionals’ and patients’ perspectives, there is a lack of relevant quantitative data, 34 and appropriate validated instruments for measuring patient participation in healthcare are needed.35–37 In particular, it is vital to understand healthcare clients’ subjective perceptions, i.e. the experience of participation in their own care, to enable provision of good quality care.38–40
The Participation in Rehabilitation Questionnaire (PPRQ) was developed in Sweden to measure patients’ perceptions of the importance and their experience of participation in care and rehabilitation. 41 It was originally based on interviews with patients with spinal cord injuries 42 and has shown satisfactory reliability in use with this patient group. 41 However, no published studies have assessed the instrument’s reliability for use with other groups. In this study its validity for assessing the participation of a sample of patients using diverse health services (inpatients undergoing rehabilitation, and outpatients who frequently attended appointment services) was tested. It is particularly important to explore ways to improve care for such patients, and primary healthcare in general, to meet challenges posed by an ageing population, growing numbers of people with chronic health conditions, and tight budgetary care constraints.43,44 Fundamental underlying premises are that primary healthcare should be universally accessible to individuals and families, by means that are acceptable to them, with their full participation, and at a cost that the community and country can afford. 43 In the study presented here, a Finnish version of the Participation in Rehabilitation Questionnaire, FI-PPRQ, was tested and validated.
Aim
The aim of this study was to assess the validity of the FI-PPRQ, an evaluative self-report instrument that has been developed to measure patients’ perceptions of the importance and experience of participation in care and rehabilitation.
Methods
Study design
The original PPRQ questionnaire was translated from Swedish into Finnish. The translated instrument (FI-PPRQ) was then subjected to psychometric tests with a quantitative cross-sectional design.
Instrument
The original PPRQ instrument includes 23 items covering five scales: respect and integrity (six items); planning and decision-making (four items); information and knowledge (four items), motivation and encouragement (five items); and involvement of family (four items). It is intended to provide indications of both the importance and experience of participation: respondents rate each item in terms of perceived importance and how frequently they experienced it during their own care. Respondents assess their care as a whole, regardless of its duration, and refer to the all of the personnel involved in their care during that period (inter alia, doctors, nurses, physiotherapists and psychologists). Each item is rated on a five-point Likert scale. Higher scores indicate stronger endorsement: the ratings for ‘importance’ are extremely important (5), very important (4), important (3), slightly important (2), and not at all important (1), while the ratings for ‘experience’ are always (5), often (4), sometimes (3), seldom (2), and never (1). 41
The original Swedish version of the PPRQ was translated into Finnish for this study using forward and backward translation. First the original questionnaire was translated into Finnish by a professional translator. Then the Finnish translation was translated back into Swedish by another professional translator unfamiliar with the wording of the original Swedish questionnaire. Then the translated and original questionnaires were compared by both translators together, to create a translation corresponding to the original content. They produced a draft Finnish version of the questionnaire, along with a report outlining possible differences in meaning and alternative solutions. The study group then met with a multidisciplinary group of primary healthcare professionals to discuss the wording, intelligibility and cultural relevance of this translated questionnaire. Next, a bilingual native of Finland who had worked as a physiotherapist in Sweden for decades produced a second translation of the original questionnaire. Final revisions of the Finnish version were then completed by the study group, i.e. the authors.
In this study, one item associated with the ‘respect and integrity’ scale in the original PPRQ (‘Personnel should leave the patient alone when he/she so desires’) was deleted because it was deemed inappropriate for clients of the appointment services. The modified FI-PPRQ questionnaire thus consists of 22 items associated with the five scales established in the original version. The Likert scales were not changed. Data on demographic characteristics (age, gender, marital status, education and number of healthcare appointment visits in the preceding year) were also collected.
Data collection procedure
The participants were recruited from six units of the appointment services and two rehabilitation wards of the hospital services of primary healthcare in one municipality in Finland between June and October 2016. Candidate participants included all clients who had been cared for in the rehabilitation wards and discharged at the time of data collection, as well as all ‘key clients’, i.e. frequent attenders of the appointment services, who were recruited while attending appointments. There is no generally accepted definition of frequent attendance 45 but in units involved in this study criteria for this category were multiple uses of the provided services (with no strict definition of the numbers or kinds of services used) and poor therapeutic equilibrium (which may be related to life-management difficulties or psycho-social difficulties) so they were usually patients with one or more chronic diseases. People younger than 18 years old or unable to respond to a questionnaire, due to language or cognitive barriers (according to professionals working with the relevant clients and familiar with this study), were excluded from the study.
Prior to data collection, the researcher briefed staff in each unit involved in the study to establish the arrangements. Written instructions were also provided. Staff members in the relevant units were instructed to consider the above criteria when inviting clients to participate. These personnel, mostly nurses, asked whether clients were willing to participate and, if so, forwarded questionnaires to them at the end of their care period. In total, 300 questionnaires were sent out, together with return envelopes and detailed written information including: the purpose and objectives of the study; assurance with regards to anonymity, confidentiality, and the voluntary nature of participation; and the researchers’ contact details. Participants were asked to return completed questionnaires by putting them in closed envelopes and placing the envelopes in sealed boxes located in the units. Completion of this procedure was considered to imply informed consent to participate in the study.
Data analysis
Statistical methods were used to evaluate the properties of the FI-PPRQ using the software package SPSS 23 for Windows. Each respondent’s and all respondents’ ratings of the importance and experience of participation were evaluated separately, at both item and scale levels. The sample was small and distributions of some of the data did not meet normality criteria for parametric tests (according to Kolmogorov–Smirnov tests and visual inspection of the data), so nonparametric tests were used. The level for statistical significance was set at p < 0.05. 46
A half-scale method was used to impute missing values; that is when a respondent had answered at least half the items associated with a scale, missing values for that scale were replaced with her or his mean score for the other items associated with the scale. 47 However, no value was entered if the respondent had answered less than half of the items on this scale. (For example, five items are associated with the respect and integrity scale, so the maximum allowed number of missing answers for a respondent is two.) This was done to ensure that all values of scales were average scores for valid item values and thus maintained validity. Imputed values were included when calculating inter-item and item-scale correlations, which are sensitive to missing values. Cronbach’s alpha coefficients were calculated before imputation.
Descriptive statistics were used to characterise the sample of patients in terms of participants’ demographic characteristics and measured or calculated variables (distributions of item and scale scores, frequencies and percentage distributions, means, standard deviations, medians, ranges, missing values, and frequencies of ceiling and floor responses). The ideal proportion of both floor and ceiling responses was determined to be between 1% and 15%. 48
To evaluate the reliability of the questionnaire, its internal consistency was assessed by determining Cronbach’s alpha coefficients and Spearman correlation coefficients between the instrument’s items and scales. 49 Alpha coefficients of 0.70 or higher were considered satisfactory.46,49 Cronbach’s alpha coefficients were also calculated following the deletion of items to identify items that should potentially be excluded. Correlation coefficients of 0.1–0.3, 0.3–0.5 and >0.5 were respectively regarded as indicating weak, moderate and strong correlation. 46
The construct validity (which indicates how well an instrument actually measures the constructs it is intended to measure, based on the construct’s relationships to other variables) and structure of the FI-PPRQ 50 were assessed by subjecting the experience ratings to exploratory factor analyses (EFA), using principal axis factoring with varimax rotation to obtain the simplest factor solution. Exploratory factor analyses is widely regarded as being largely or solely applicable to datasets describing or collected from large samples, but it can also provide acceptable solutions for data concerning or drawn from small samples.51,52 The instrument’s item convergent and discriminant validity were also tested by examining correlations of the items with their corresponding scales (corrected for overlap) and other scales. Item convergent validity was judged to have been confirmed if correlations between items and the corresponding scales exceeded 0.40. Item discriminant validity was judged to have been confirmed if correlations between items and the corresponding scales were significantly higher (by more than two standard errors) than correlations between the items and the other scales. 49
Ethical considerations
This study was conducted following the ethical standards outlined in the Declaration of Helsinki 53 and responsible research practice guidelines. 54 Permission to use the Finnish version of the PPRQ was obtained from the developer of the original instrument. Prior to data collection, the study was approved by the hospital’s Institutional Review Board (2760/2016). Ethical assumptions of confidentiality and voluntary participation were respected. Completion and return of the anonymous questionnaire was considered to imply informed consent for participation in the study. Due to the anonymity of responses no ethical approval was required.
Results
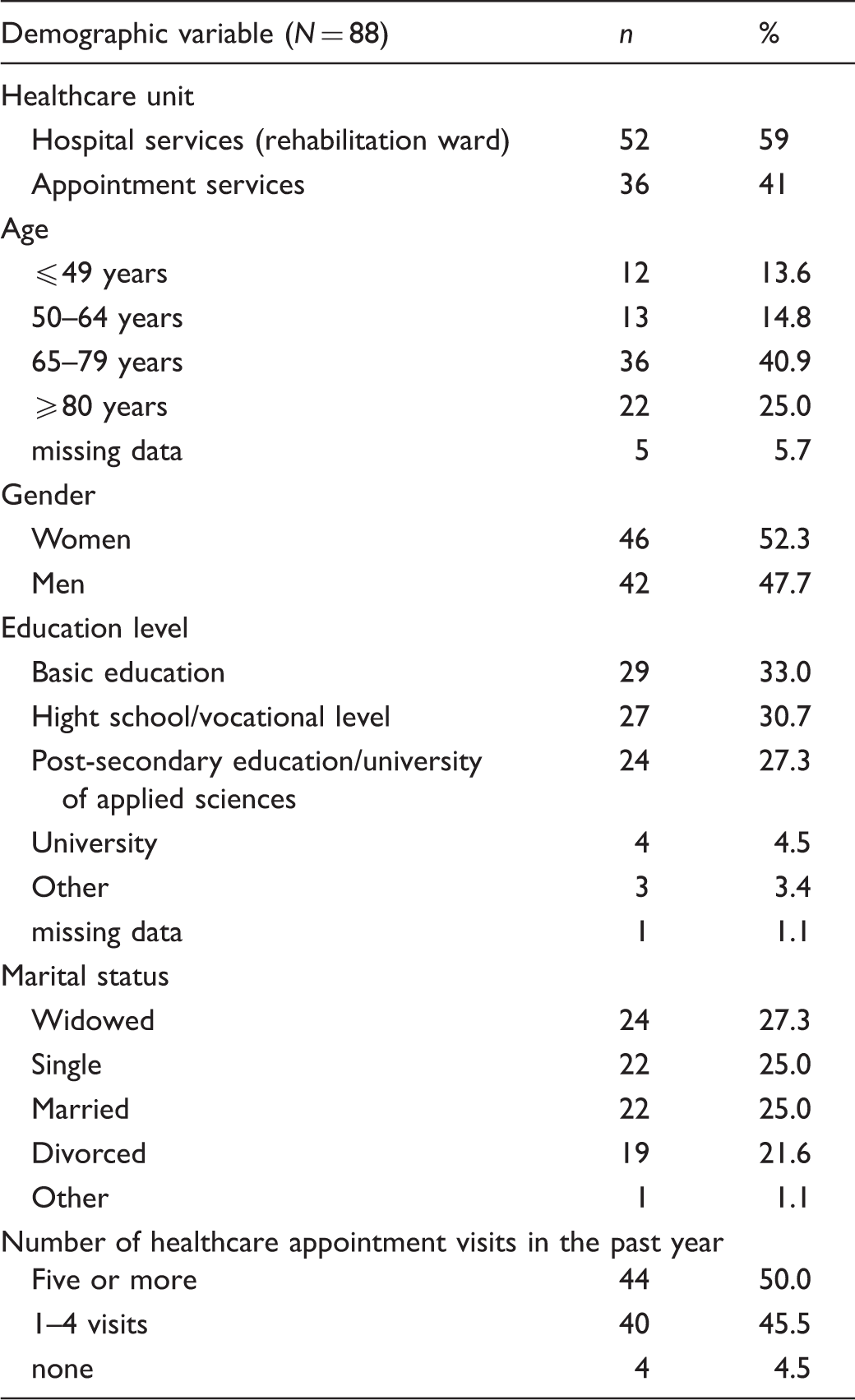
Sample characteristics
Basic demographic characteristics of participants (n, %).
FI-PPRQ scores
Summary of results of FI-PPRQ scales (Mean, SD, Median, % at ceiling and floor, Cronbach’s alpha coefficients and inter-item correlations of scales).
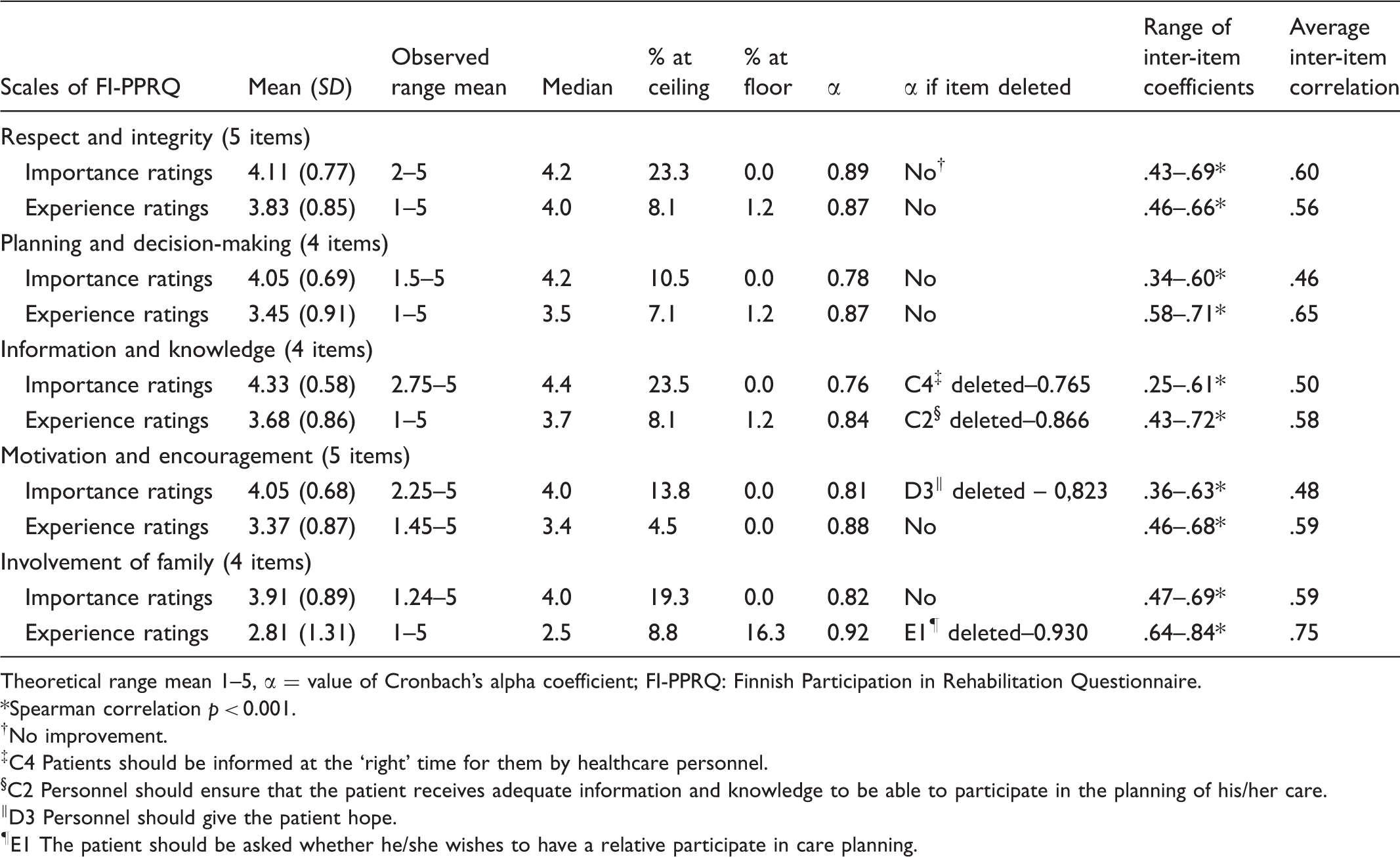
Theoretical range mean 1–5, α = value of Cronbach’s alpha coefficient; FI-PPRQ: Finnish Participation in Rehabilitation Questionnaire.
*Spearman correlation p < 0.001.
†No improvement.
‡C4 Patients should be informed at the ‘right’ time for them by healthcare personnel.
§C2 Personnel should ensure that the patient receives adequate information and knowledge to be able to participate in the planning of his/her care.
‖D3 Personnel should give the patient hope.
¶E1 The patient should be asked whether he/she wishes to have a relative participate in care planning.
Reliability of the FI-PPRQ
Correlation coefficients between the scales for importance and experience ratings.
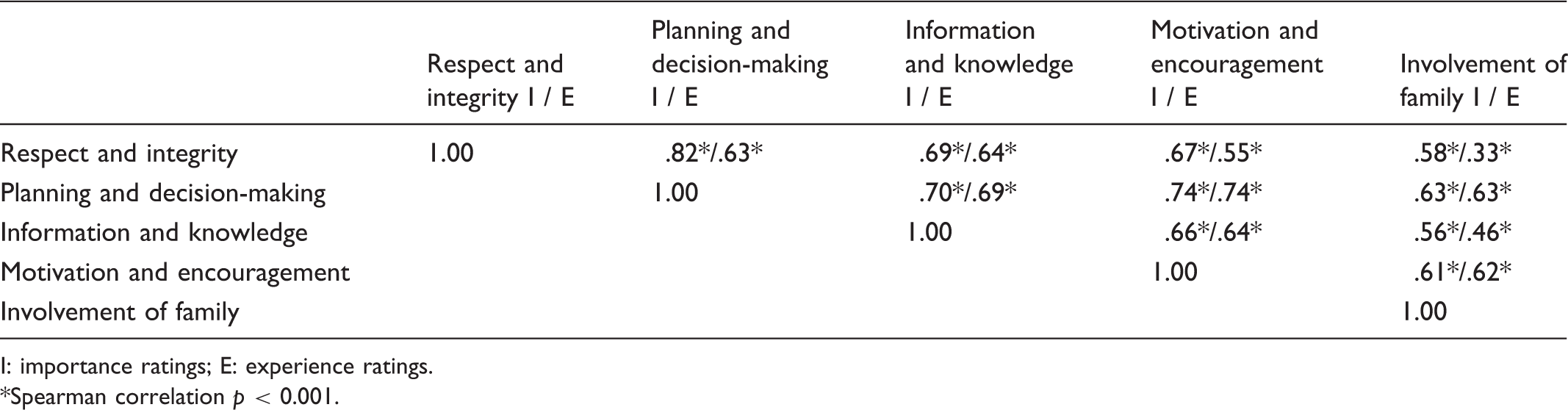
I: importance ratings; E: experience ratings.
Spearman correlation p < 0.001.
Construct validity of the FI-PPRQ
Item convergent and discriminant validity
Statistics of item convergent and discriminant validity.
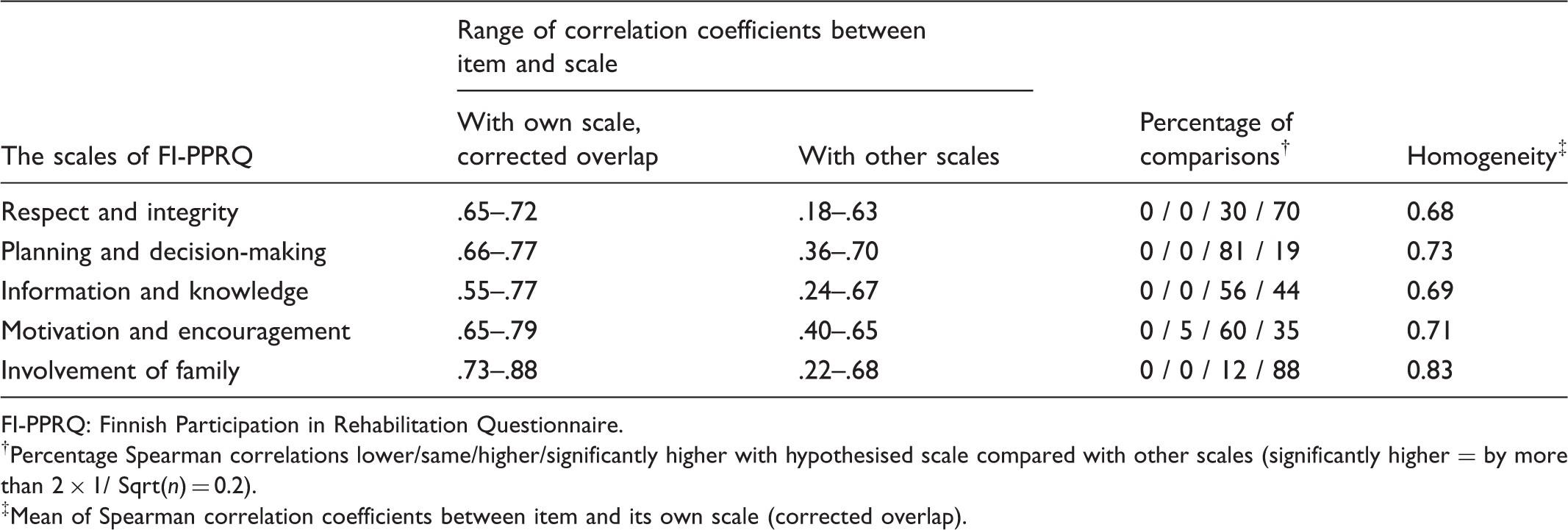
FI-PPRQ: Finnish Participation in Rehabilitation Questionnaire.
†Percentage Spearman correlations lower/same/higher/significantly higher with hypothesised scale compared with other scales (significantly higher = by more than 2 × 1/ Sqrt(n) = 0.2).
‡Mean of Spearman correlation coefficients between item and its own scale (corrected overlap).
Factor structure
As mentioned above, to examine the FI-PPRQ’s construction and construct validity, the experience ratings were subjected to EFA using principal axis factoring with varimax rotation to obtain the simplest factor solution. The distributions of variables met the normality requirements (Kolmogorov–Smirnov statistic, 0.2; p > 0.05), although the small sample size should be considered when interpreting the results. Moreover, results of Kaiser–Meyer–Olk’s measure of sampling adequacy and Bartlett’s sphericity tests (0.847 and 0.000, respectively) showed that the correlation matrix had acceptable covariance and factorability.
Structure of questionnaire and factor loadings according to analyses for experience ratings.

†Principal axis factoring with varimax rotation.
Discussion
This article describes the creation and evaluation of a Finnish version of the PPRQ, FI-PPRQ, a self-report instrument designed to measure patients’ perceptions of the importance and their experience of participation in care. Earlier studies have described the development of the original Swedish instrument and tests of its psychometric properties with patients who had been treated for spinal cord injuries41,42 and their family members. 55 In contrast, in this study the instrument was applied to gauge perceptions of patients (inpatients and outpatients) who frequently used healthcare services (in various permutations) in Finnish primary healthcare settings. The legitimate use of previously validated instruments provides stronger foundations for reliability than use of instruments that have never been previously tested. 46 Nevertheless, it was important to conduct a rigorous pilot study before using the instrument more widely because it was both translated from another language and used for the first time in this context. 56
Approaches for developing and evaluating psychometric patient-reported outcome instruments are generally rooted in Classical Test Theory (CTT), Item Response Theory (IRT) or Rasch Measurement Theory (RMT). The methodology applied in this study is based on CTT, because it is long-established, widely used, and primarily based on evidence from correlations and descriptive statistics 57 and is so consistent with the testing of the original PPRQ instrument. 41 The assessment of equivalency is also a commonly used method but in this study concurrent validity was not tested, because there was no criterion variable or parallel instrument available.
Comparison of three studies using PPRQ instrument (mean, SD, α).
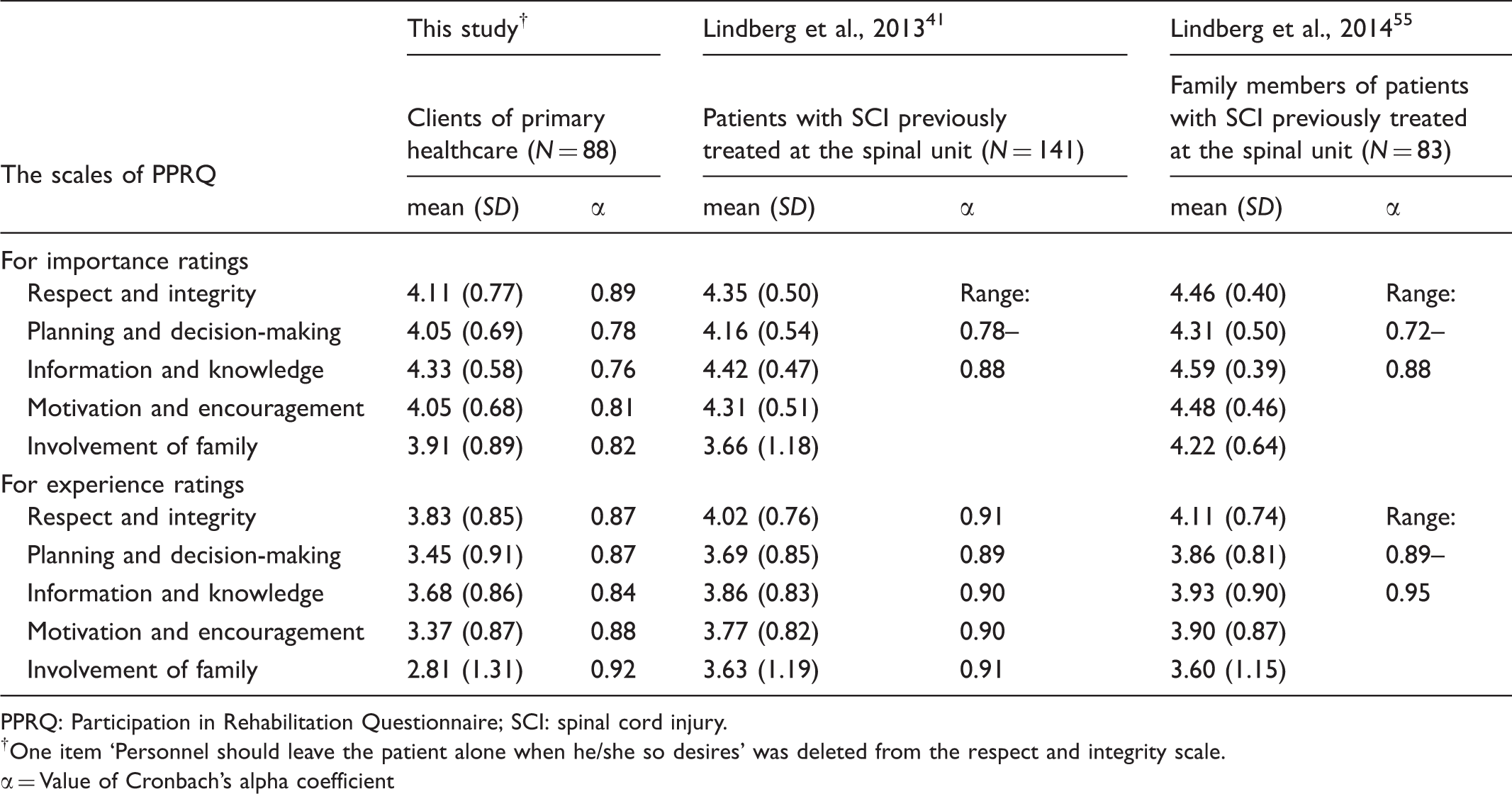
PPRQ: Participation in Rehabilitation Questionnaire; SCI: spinal cord injury.
†One item ‘Personnel should leave the patient alone when he/she so desires’ was deleted from the respect and integrity scale.
= Value of Cronbach’s alpha coefficient
The results obtained in this study show that the FI-PPRQ has adequate reliability and validity. Cronbach’s alpha coefficients were all well above 0.70 for all FI-PPRQ scales and both dimensions (importance and experience) of the instrument as a whole, indicating good internal consistency for group-level comparisons.46,50 Intercorrelations of items within scales ranged from 0.25 to 0.84, while average inter-item correlations ranged from 0.46 to 0.75, and were highest for the family involvement scale. Some inter-item correlations for this scale also exceeded 0.80, indicating that some associated items are very narrowly focused, possibly overlapping. 58 Correlations of the items with corresponding scales, corrected for overlap, varied from 0.55 to 0.88, well above the threshold of 0.40 for acceptable convergent validity. These results also support the internal consistency of the scales. 49
The instrument’s construct validity was also examined using EFA (principal axis factoring with varimax rotation). This yielded a five-factor solution that corresponded very well with the five domains of participation identified in the development and tests of the original PPRQ instrument,41,42 except that four items loaded most strongly on factors that did not match corresponding dimensions in the cited study. In the dataset acquired in this study, the item ‘Personnel should ensure that the patient receives adequate information and knowledge to be able to participate in the planning of his/her care’, associated with the information and knowledge factor according to the cited study, loaded strongly on the planning and decision-making factor. One item reportedly associated with the planning and decision-making factor, ‘Personnel should know if the patient has any special obstacles/problems that limit good care and rehabilitation’, strongly loaded on the motivation and encouragement factor. In addition, two items reportedly associated with the respect and integrity factor loaded strongly on both the planning and decision-making factor (‘Personnel should treat each patient as a unique individual’) and information and knowledge factor (‘Personnel should respect the patients’ private/personal matters’).
Despite these discrepancies, the structure obtained in the studies with the original PPRQ was applied in further analyses and interpretation. When assessing the results of the EFA generated in the present study the small sample size should be considered. 52 However, the discrepancies are theoretically understandable, considering the essence of participation. Respect is manifested in ways that individual patients are treated and their personal matters are handled by staff members, but it is particularly important to address these issues in planning, information processing and care-related decision-making. According to previous studies, the starting points for participation are recognition of individuals’ autonomy23,34 and respecting them.15,20,23 Sufficient information and knowledge are further general requirements for participation, particularly for ensuring that individuals can meaningfully participate in the planning and implementation of their care. 23 Information and feedback must be based on individuals’ personal needs and preferences,15,20 and patients have emphasised the importance of receiving adequate information, developing knowledge and being listened to – i.e. a two-way communication process for sharing information.4,10,20 Clients’ experiences of factors that currently hinder good care must also be taken into account, both in the planning of care and in offering motivation and encouragement. According to patients, it is important to be acknowledged as competent and regarded as an individual, taking into account one’s personal life situation. 15 Thus, patients’ experience-based knowledge and lived experience should be valued by healthcare professionals.23,34
The PPRQ provides information about various core aspects of participation. These include patients’ expectations and actual experiences of being treated with respect by professionals, involved in care-planning and decision-making, motivated and encouraged, receiving adequate and timely information about care, and family members having opportunities to participate. 42 The instrument can be used to measure clients’ perceptions of both the importance and experience of participation in care and rehabilitation. Importance ratings allow clients to depict their personal preferences. The results of this study show that participation is considered to be very important, confirming results of several previous studies.4–6 Experience ratings reflect clients’ perceptions of the degree to which the requirements for participation are actually provided in healthcare contexts. The attitudes and behaviour of personnel can strongly affect patient participation and it is important to ensure that organisational practices and culture enable clients’ participation. 19 Health professionals have considerable scope to support patients by showing empathy, encouraging them, and sharing knowledge and power, thus enabling them to participate, take responsibility and assume an active role in their own care to the fullest extent possible given their capabilities. 23 Both this and previous studies indicate that the PPRQ contribute to continuous quality improvement efforts in the health and care sectors by providing valid measures of patient participation.
Several methodological considerations should be taken into account when interpreting the results of this study. The sample size was small, but probably sufficiently large for a pilot study of an instrument that had been previously validated in other settings. One factor that restricted the sample size was the limited number of patients who met the inclusion criteria in the units involved during the data collection period, even though this was quite long. Further, it was not possible to calculate the overall response rate for the total sample or to analyse the comparability of non-respondents and the final sample due to the anonymity of responses. However, the study participants did seem to reflect the wider target population in terms of their age, gender and education profile. To ensure that respondents’ assessments accurately reflected their perceptions of patient participation during care, they filled out the questionnaire immediately after their care periods, thus minimising recall bias.
Conclusion
The presented results show that the FI-PPRQ had acceptable reliability and validity for assessing the respondents’ perceptions of the importance and their experience of participation, indicating that it is a useful instrument for assessing participation in primary healthcare contexts from clients’ perspectives. However, the generality of its validity and reliability requires further evaluation in more studies with larger samples and more varied settings. It would also be worthwhile to use RMT or
Author contributions
LP, A-MP and PK designed the study, A-MP supervised and LP coordinated the translation process, LP collected and analysed data and PK provided feedback on statistical analyses. LP wrote the manuscript as first author, A-MP and PK critically revised the manuscript and supervised the study. MK provided critical revisions of content. All authors approved the final manuscript.
Footnotes
Acknowledgments
The authors would like to thank Dr Ari Voutilainen, University of Eastern Finland, for applying his expertise in statistical research methods in a review of this study and Dr Jeanette Melin, University of Gothenburg, for her critical comments regarding the manuscript. We also thank all the health professionals, translators and clients who participated in this study for their collaboration and invaluable contributions.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.