
Abstract
Objectives
The current research aimed to develop a questionnaire for the evaluation of the staff viewpoints in mobile phone use in the delivery of their services and then to assess the primary health center staff attitudes toward this area.
Methods
This was a two-stage cross-sectional study. In the initial stage, a questionnaire was constructed that tested their reliability and validity through Cronbach’s alpha coefficient, multitrait/multi-item correlation matrix and multivariate method of factor analysis. In the second phase, we computed the raw score of each construct which was calculated by taking the mean of the responses of all the items in a particular construct. The normality of the scores for each construct was tested via Kolmogorov-Smirnov and various parametric/non-parametric statistical tests were applied to compare the responses of the subjects. After statistical tests, the final questionnaire was confirmed, including 28 items.
Results
The final questionnaires’ five main axes consisted of health services efficiency, education, notices, consultation, as well as follow-up. Personnel perspective assessment indicates that there is no difference of view among individuals coming from various demographic features, including gender, age, work experience, as well as education level, to mobile phone use in their services.
Conclusion
The attitude of public health center staff to mobile phone use in providing health services was positive in general, which would be an influential context for the effective application of mobile phones in public health; such a context would result in users' intentions to use and accept m-Health.
Introduction
Information technology (IT) has become one of the vital mechanisms today for the growth of the healthcare industry. Healthcare experts need to have access to information about their patients anytime and anywhere. Mobile phones are one of the instruments that may effectively assist such access to information about patients. 1 The use of such tools in health results in a new field, mobile health (mHealth); this refers to medical and public health deeds supported by mobile tools, including mobile phones, patient monitoring instruments, personal digital assistants, as well as other wireless devices. 2 The most significant aim of mHealth is identified to be the improvement of health services quality and healthcare access. 1 , 3 , 4 The use of mobile phones in health may result in reducing health services expenses, as well as altering population behaviors to preventive ones, which may improve the results of health systems in the long run. 4 Certain types of preventive behavior that may be managed in some way by mobile phones are smoke cessation, weight loss, alcohol consumption management, and sexually transmitted infections. 3 Information and resource sharing via mHealth may result in delivering information on health matters, making data available to providers in remote geographical zones, increasing patient self-education, as well as improving diagnosis practice. 5
In developing countries, mobile phone use is a cost-effective method to satisfy the particular needs of the health system and an appropriate device for disease control interventions. 6 In the face of traditional methods in behavioral change interventions, mobile technology has appeared to enhance clinical and behavioral effects with today's advances. The potentiality of mHealth in preventing disease and self-managing chronic disease has been demonstrated. Mobile phones, in recent decades, have been adapted as an operative device for behavioral change in chronic disease prevention, as well as a personal site for patient communication, engagement, health data tracking, information up to dating, and reminders of health behavior. 7 In research, kidney transplant recipients have a positive attitude to mobile phone use in their care practice in general; they believe that such tools offer appropriate conditions for self-efficacy and assist providers in better medical care management. 8
As the most primary healthcare (PHC) goal is offering the highest levels of health and well-being through centering on needs and preferences of people, efforts have been made to improve access to preventive services, treatment, early diagnosis, as well as focusing on people by decreasing hospital admissions and re-admission to decrease total health expenses and enhance care efficiency. 9 Non-communicable ailments in low and middle-income countries, in particular, trigger much damage and risk to the well-being and health of the international community. PHC has the potential to prevent such ailments. 10 Mobile phones have potential, including a high level and easy acceptance of optimal application, and may be a proper tool for PHC purposes. 7
Public health with distinct sections has great potential to be linked by mobile phones similar to other IT services. Certain examples of IT services in this scope are information dissemination, data analysis, as well as disease surveillance. 11 Decision-making in public health requires timely accurate data, 12 and mobile phones may meet this need with the potential to ease communication. A systematic review of the mHealth application in disease surveillance offered proof about the use of various mobile applications (apps) in collecting health observation data in sub-Saharan Africa. 13 Public health staff can notify and send preventive messages through mobile phones to the patients to get health services and peer support. 2 According to Medhanyie et al.'s research, it was feasible to use electronic forms on a smartphone in primary health to collect data on maternal health on a small scale. 14
In the last two decades, the Iranian government has focused on primary care services and has become the most significant provider of healthcare in the country with certain services, including vaccination and prenatal services for free. 15 Villages or a set of them encompass Health Homes (health delivery service centers in Iranian villages) being the first point of contact with the health system based on the structure of the primary healthcare network in Iran. Health sites and centers in the cities are the first contact point, all of which work under the supervision of the University of Medical Sciences in each province. 16 Various services are offered by the health centers that include vaccinations, care of the pregnant and elderly, as well as management of chronic and non-chronic diseases like diabetes, hypertension, and cancer. In Iran, the human resources and organizational structure of health centers may be employed as a chance for lifestyle adaptation interventions. 17
Leong et al. 18 exploited the performance, attitudes, and beliefs of phone hygiene amongst healthcare workers of Singapore tertiary acute care hospital. They also examined how the effect of phone hygiene stations started to enhance phone hygiene. In their survey, it was recorded that 11.5% healthcare workers cleaned their phone regularly while 9.4% had never cleaned it, but that was altered to 16.9% and 3.8% respectively after the setting up of phone hygiene stations. Feroz et al. 19 explored the potential of the use of the mobile phone in low- and medium-income countries to improve the performance of community health workers. Evidence confirmed that services offered by the community health workers had a major role in the decline of child and maternal mortality and morbidity rates and the burden of non- communicable and communicable diseases. Islam et al. 20 estimated the cost-effectiveness of a mobile-phone text-messaging program for patients with type 2 diabetes mellitus. The intervention costs for the mobile-phone text-messaging program were summed as $2842. Hence, it was a valuable addition to the diabetic patients’ treatment and predicted to provide a good saving in low-resource settings. Mobile health (mHealth) has a great influence on healthcare in different ways. 21 Smartphones can be utilized in delivering media-rich medical advice and providing clinical decision support. Smartphones can serve as an influential support tool for community health workers in developing countries. Recently, there have been many novel health mobile technologies including smartwatches and activity sensors.
In Iran, on the other hand, more than 80% of individuals who use mobile phones send short message services (SMS) once a day at least. Service popularity makes the phone a health messenger. Numerous investigations have supported mobile performance, as well as its effect on lifestyle and health education, in chronic diseases like diabetes in particular. Evidence has indicated that mobile technology, the SMS particularly, might be applied as a training instrument to improve the outcomes in patients with type 2 diabetes. 22 Mobile technology may be a preventive instrument in patients with cardiovascular disease (CVD); two communication forms with patients are SMS and mobile apps based on Park et al. 7 As the most frequent visitors to Isfahan health centers are women, a corrective package is planned to shift the behavioral health of women with hypertension referred to the centers according to Hasandokht et al. 17 Given the potential of mobile phones in primary care, this research aims to review the perspective of Zahedan health center staff on mobile phone use in providing their services; to make it a positive technology adoption, it is essential to distinguish and improve the users’ perspective at first. Zahedan is a city and capital of Sistan and Baluchestan Province, southeast of Iran. At the 2016 census, its population was 587,730. The authors did not find an appropriate instrument to assess the viewpoint of public health staff; thus, as the first stage, a unique questionnaire was designed, and then the views were evaluated.
Materials and methods
Study design
The current research was conducted as a descriptive cross-sectional study to evaluate the perspective of public health center staff in Iran on mobile phone use in service delivery, which was done in two stages: the initial draft of the questionnaire with 31 items was designed using a literature review in the first stage. In the second stage, reliability and validity of the questionnaire were tested based on a cross-sectional analysis and gathering information from health staff, and then their perspectives were analyzed. Thirty Zahedan public health centers were included in this study, from which 203 health staff were involved as the study population. We have used single-stage cluster sampling. In this case, we have considered the cities of different provinces of Iran as different clusters. From these clusters, Zahedan was selected randomly using simple random sampling methods. All the public health centers within Zahedan are included in the study.
Study tool and data collection
A questionnaire designed by researchers was used to assess the viewpoint of personnel. The initial questionnaire was designed after a literature review and extraction of main concepts. The final questionnaire included two central sections: demographic information and the 28 questions in five sections, which evaluated staff perspectives on mobile phone effects on health service quality and efficacy, education, notices, consultation, as well as follow-up. The replies were ranged in a five Likert-point scale from completely agree to completely disagree with a score of 1–5 (completely agree=5, agree=4, no idea=3, disagree=2, completely disagree=1) (see Appendix 1).
After study planning and questionnaire preparation, as well as their approval by the student’s research center of Zahedan University of Medical Sciences, the researchers went to these public health centers and provided the personnel with the questionnaires. A cover letter with certain information on mHealth was included with questionnaires; responders were assured about the confidentiality of their information . The researchers returned and collected the questionnaires on the day after each distribution. A total of 203 questionnaires were collected from 30 centers. Data collection was done over a month.
Statistical methods
Phase 1 questionnaire analysis
Before implementing the tool, its reliability and validity were tested through various statistical processes. Cronbach’s alpha coefficient tested the internal consistency reliability. The multitrait/multi-item correlation matrix was used to test the convergent and discriminant validity, and the multivariate method of factor analysis was applied to test the construct validity. The designed questionnaire to investigate delivery services of mobile phone in healthcare included five concepts which were health service effectiveness, education, notices, consultation, as well as follow-up. All other constructs apart from the construct consultancy satisfied the internal consistency reliability. The tool consisted of 31 items divided into five constructs of health service effectiveness (eight items), education (five items), notices (five items), consultation (two items), and follow-up (eight items). Once the validity had been tested, the instrument was restructured; the new questionnaire had 28 items as shown in Table 1.
Description of construct, number of items and item number.

Phase 2 of analysis
Once the reliability and validity of the questionnaire were tested, the proper statistical test was applied to compare the perception of mobile phone delivery services in healthcare concerning various demographic characteristics. The first phase to achieve this goal was to compute the raw score of each construct which was calculated by taking the mean of the responses of all the items in a particular construct. The normality of the scores for each construct was tested via a Kolmogorov-Smirnov (K-S) before applying the statistical test to the raw scores. Various parametric/non-parametric statistical tests were applied to compare the responses of the subjects.
Ethical considerations
The study plan was approved in the student research center by the Research and Technology Department of Zahedan University of Medical Sciences. After receiving written permission, the researchers referred to the centers. The personnel were provided with all descriptions about the research, such as the method and benefit, they took part in the research with informed consent. They were assured about the confidentiality of their information and that their opinion was to be used just for research goals.
Results
In the final analysis, a total of 203 respondents were involved. There was a female majority in the sample with around 78%. Most respondents were in the age group of 30–40 (54%) years followed by the age group of less than 30 years (28%). The education level of most respondents was associate degree (49%) followed by bachelor degree (29%). Table 2 presents a thorough profile of the subjects in the research.
Demographic profile of the study subjects.

Phase 1 results
For all the multidimensional scales of the questionnaire, Cronbach’s alpha coefficient of internal consistency was computed and Table 3 shows the findings.
Internal consistency reliability of the questionnaire.
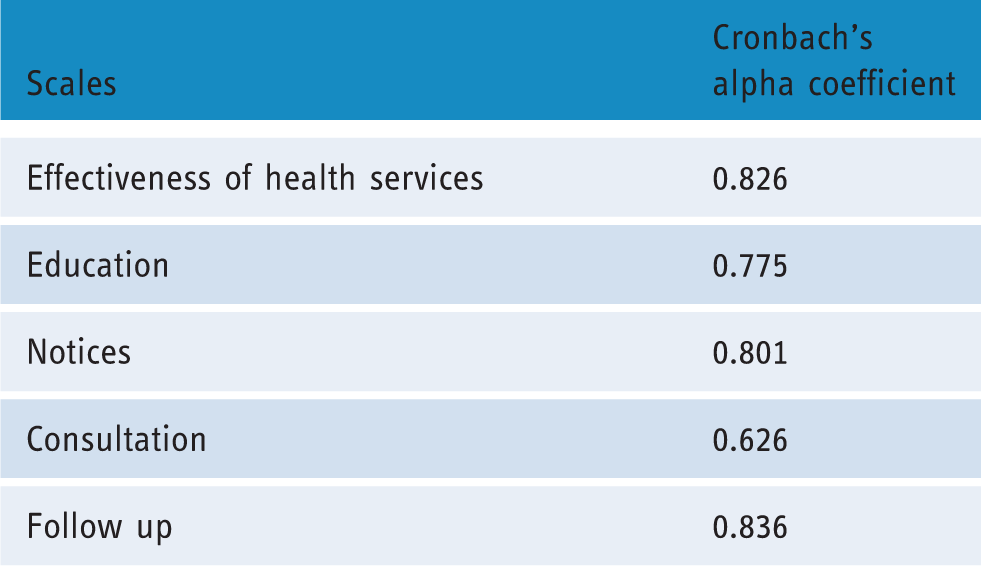
As can be seen in Table 3, most scales of the tool demonstrate a high value of alpha coefficient (α≥0.70). However, the alpha coefficient for the scale consultation is lower, i.e. α=0.626. All the scales apart from consultation, therefore, meet the reliability of internal-consistency. The multitrait/multi-item correlation matrix is used to test the convergent and discriminate validity of the scales. Table 4 demonstrates the multitrait/multi-item correlation matrix.
Multitrait/multi-item correlation matrix of the questionnaire.
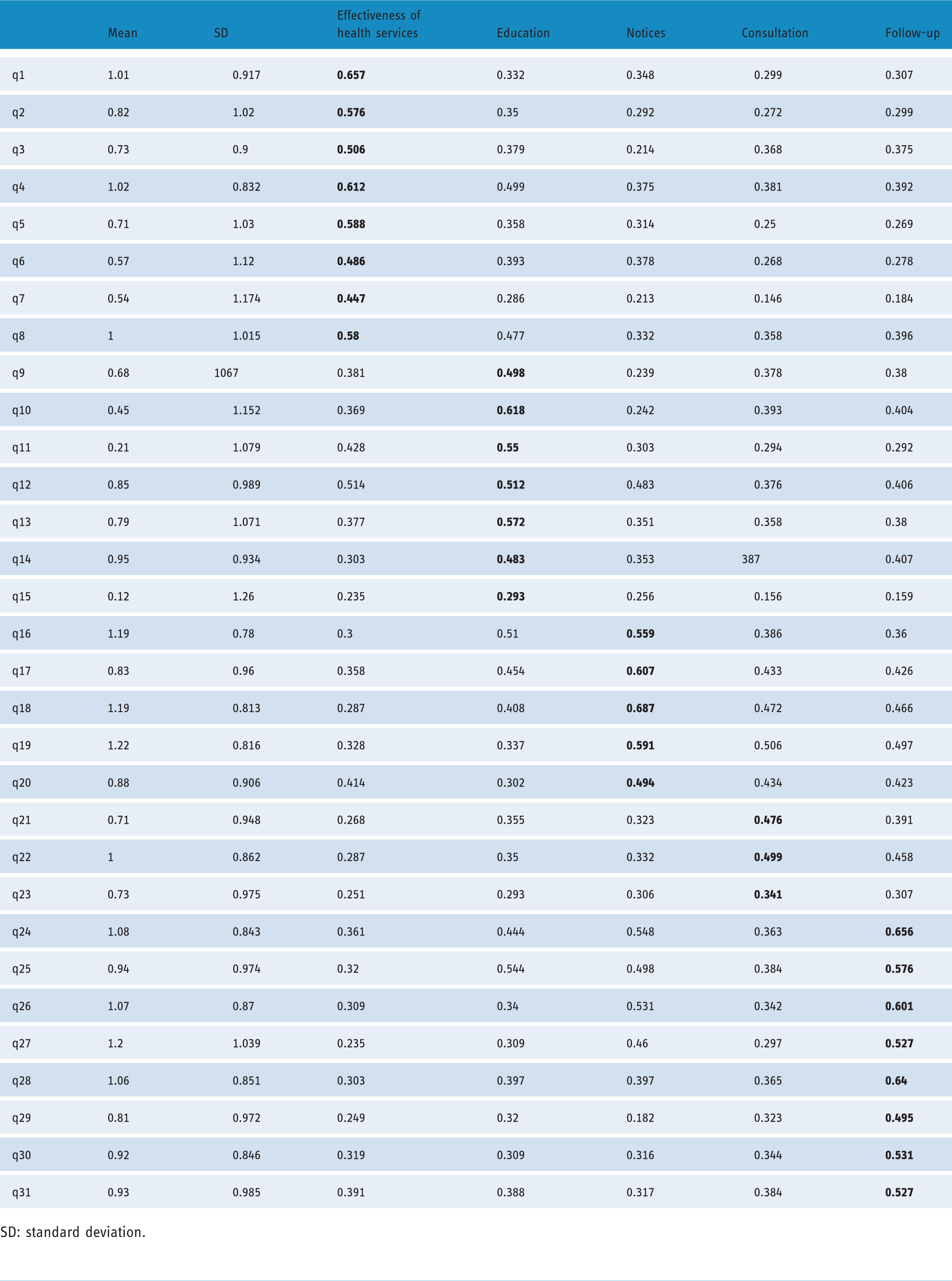
SD: standard deviation.
As can be seen in Table 4, all items in the health service effectiveness scale have registered a correlation higher than 0.4 with its scale. All the items, thus, meet convergent validity. Moreover, all items of the scale have a lower correlation with other scales rather than its scale. All the items, therefore, meet discernment validity. All items of the education scale meet convergent validity. Questions 10 and 12 (q10 and q12) have also recorded a high correlation with the scale of notices and follow-up. These two items can be excluded from the analysis. For the scale of notices, all questions meet convergent validity with a correlation higher than 0.4 with its scales. Questions 19 and 20 fail to meet discriminate validity; its correlation with the scales of consultation and notices are quite high. Q23 of the consultation scale fails to satisfy both convergent and discriminant validity with low correlation with its scale (0.341) and high correlation with other scales. This question, thus, may be omitted from the questionnaire. For the follow-up scale, all questions meet convergent validity with a correlation higher than 0.4 with its scale. Q24, q25, and q26 fail to satisfy discriminant validity as they register a high correlation with the scales of notices and education, respectively.
Factor analysis
Factor analysis is performed to recognize the nature of factors building fundamental measures in the questionnaire. Before factor analysis, Kaiser-Meyer-Olkin (KMO) measures of sampling adequacy and Bartlett's Test of Sphericity were applied to investigate the data appropriateness for the analysis.
The factor analysis extract factors and the factor loading matrix is given in Table 5.
Rotated component factor loading matrix.

The first factor with Eigen value of 9.169 loads q16, q17, q18, q19, and q20 that forms the construct “notices” with factor loading range of 0.742–0.462. Q20 has high factor loading of 0.526 with the fourth factor. Therefore, q20 is highly correlated with the first and the fourth factor, and it may be excluded from the questionnaire. The similar findings may be observed in the matrix of multitrait/multi-item correlation. Higher factor loading may be observed in the second factor for q24, q25, q26, q27, q28, q29, q30, and q31 that construct the follow-up. Also, q24, q25, and q26 hold higher factor loadings with the first one. Thus, these items are correlated with the fourth and the first factor, and they may be omitted from the second factor. Accordingly, the second factor is constituted with q27, q28, q29, q30, and q31 that can be labelled as a follow-up. The factor loading of the latter factor ranges from 0.482–0.694; approximately the total variation of 7% is clarified by that. The third factor describes approximately 7% of the total variation in the data. Q1, q2, q3, q4, and q5 have shown higher factor loading for the third factor. Therefore, “health services effectiveness” is constituted by q1, q2, q3, q4, and q5. A significantly higher factor loading is observed in the fourth factor for q6, q11, q15, as well as q23. The total variance is described by this factor as 5.701. Q9, q10, q12, q13, and q14 have higher factor loadings for the fifth factor that forms “Education”. Q11 and q15 being regarded to be items of “Education” loaded poorly with it. These two items fail to meet the convergent and discriminant validity, as observed through the multitrait/multi-item correlation matrix in Table 5. Approximately 5% of the total variation in the data is explained by the fifth factor. Q21 and q22 hold significantly higher factor loading with the sixth factor that clarifies around 4% of the total variance q23 to have its place in “consultation” together with q21 and q22 show very low factor loading. The similar results may be observed in the matrix of multitrait/multi-item correlation, where q23 also correlates poorly with its scale. The seventh factor holds significantly higher factor loading for q7 and q8 that appears to build a new scale.
After testing the reliability and validity of the questionnaire, the modified version was finalized. The modified version of the questionnaire was used to study the perception of mobile phone delivery services in healthcare for different demographic characteristics and these were compared by using an appropriate statistical test. The first step to achieve this objective was to calculate the raw score of each of the constructs which is nothing but the means of responses of all the items of a particular construct. Before applying a statistical test to the raw scores the normality of the scores for each construct was tested by using the K-S test.
The results of the K-S test are presented in Table 6.
Kolmogorov–Smirnov test on the raw scores.

As may be seen in Table 6, the raw scores of all the factors/constructs do not follow a normal distribution. Non-parametric statistical test were, therefore, employed to investigate the raw scores concerning various demographic characteristics.
Phase 2 results
In order to compare the raw scores of various dimensions concerning the individuals, the non-parametric method of Mann–Whitney U-test was applied; Table 7 shows the results of the test. As can be observed in Table 7, the perception of males and females as regards the healthcare service effectiveness are statistically insignificant (p-value <0.05). The opinion on the subject of mobile technology use in healthcare service effectiveness regarding gender is relatively the same. Comparable outcomes may be seen in the case of the other constructs, namely education, notices, consultation, as well as follow-up. Therefore, it may be established that the views of males and females as regards mobile technology use in healthcare services are more or less the same.
Comparison of raw score with respect to gender.

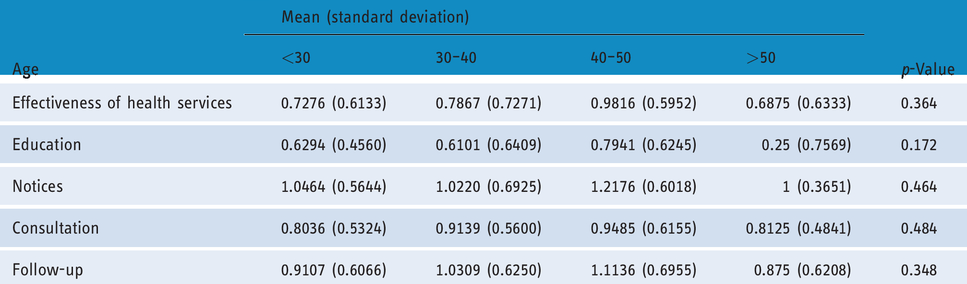
The research subjects were distributed into four groups concerning their ages; below 30, 30–40, 40–50, as well as above 50 years. The Kruskal-Wallis test was applied to investigate the differences of views on the subject of mobile technology use as regards age. The mean and standard deviation of the raw scores of all constructs were computed, as given in Table 8. Similarly to Table 7, for all the five constructs demonstrating the mobile technology application in healthcare services, the people's viewpoints are relatively the same as regards age. The p-value computed by the Kruskal-Wallis test reveals that the people viewpoints concerning the five constructs are more than 0.05.
Comparison of raw scores with respect to age.
Further, some efforts were made to investigate the perception of individuals as regards the mobile technology application in healthcare services concerning education level. The means and standard deviations of raw scores of all the constructs on the education level were computed, as shown in Table 9. To investigate the differences in the raw scores regarding the education level of all five constructs, the Kruskal-Wallis test was applied. The Kruskal-Wallis test results show that the opinions of individuals with different education level were statistically insignificant for all constructs regarding health service effectiveness, education, notices, consultation, as well as follow-up.
Comparison of raw score according to education level.

The perception of the individuals as regards the mobile technology application in healthcare services was further investigated concerning work experience. The means and standard deviations of the raw scores in all the five constructs were computed concerning the different levels of work experience. The Kruskal-Wallis test results reveal that for all constructs, calculating the effectiveness of mobile technology use in healthcare services, the views of people with various work experience levels were statistically insignificant as shown in Table 10.
Comparison of raw score with respect to work experiences.

Discussion
Certain mobile phone-based interventions, such as educating, informing, consulting, reminding, as well as monitoring, may enhance patient adherence. 23 In the current research, a tool was developed to investigate the efficiency of mobile technology in primary healthcare services, which was divided into five constructs as health service effectiveness, education, notices, consultation, as well as follow-up. These, indeed, may be regarded as five factors affecting public health personnel's opinion on mobile use.
Health service effectiveness
Some main goals of mHealth are health service quality improvement, clinical error decrease, as well as resource integration; 1 such goals may also improve patient lifestyle. 5 Patients with heart failure in the Seto et al. study were more likely to apply mobile-based monitoring; they named certain advantages, including immediate feedback from providers on their health situation. Also, they believed that this monitoring system may be below-cost and a useful method of managing the condition of heart failure patients. 24 Remote monitoring through mobile technology, indeed, appears to be an effective approach to ease patient-provider communication. 25
In the present study, most participants also agreed with mobile phone capability to improve patient lifestyle. The decrease in travel cost to receive health services, as well as in total cost of the services using mobile phones, was another agreed matter by most responders. Several studies have reported the cost-effectiveness and cost-saving effect of mHealth in managing disease.25–27 The majority of responders in the present research also believed in the mHealth capability to make equal access of individuals to health services.
Notices
The communicative capability of mobile systems makes it a suitable platform for informing goals. The findings of the current research show that personnel have a positive attitude toward the informant role of mobile phone. Communication and informant improvement resulted from using such devices, has a remarkable role in disease monitoring and education. Health providers may appear in visit sessions or present some self-monitoring advice to patients by mobile reminders. 28
Follow-up
Most participants of the Proudfoot et al. study were likely to apply mobile phones for mental health monitoring and self-management if such services were free. 29 Among the prevalent mHealth services is SMS, which may be employed for patient follow-up, health behavior, as well as data collection. 2 , 5 Lester et al. concluded that the patients who received SMS were more expected to report their adherence to Antiretroviral Treatment Adherence (ART) than the group with standard care. 26 The results of the current study reveal a positive attitude of personnel to mobile phone use in follow- up services. The use of text messages and reminders increases appointment attendance up to 7% according to Chen. 30 SMS benefits providers and patients by increasing clinic attendance. 3 Zolfaghari et al. report better improvement in Glycated hemoglobin (HbAtc) in patients to receive SMS and is followed by telephone. 31 Follow-up and communication services are the most prevailing activities offered by public health centers. Pregnant women, newborn, children, as well as elderly, are certain groups receiving services like a medication reminder or a visit attendance through mobile phones.
Education
SMS appears to be an appropriate communication tool among health providers and patients to improve their knowledge. 32 Online courses provided by mobile phones offer independent education opportunities for providers and patients. 5 The participants, in Al-Fahad’s research, were interested in using mobile phones to access their information; they also recognized it as an independent education instrument anytime and anywhere. 33 In the present research, the participants also had a positive attitude toward mobile phone use in education services. Educational track, which may be sent as a Bluetooth file to mobile phones, was the choice the majority of the participants agreed to. The educational family program on the same devices was another item that most responders were agreed with. Most health apps were installed on mobile phones to be applied for monitoring, informing, as well as educational goals. 34 Goodarzi et al. reports that sending educational SMS leads to a significant increase in the knowledge of the experimental group as compared to the control. 35 Similarly, Fatehi et al. conclude that there is an improvement in the knowledge of patients receiving educational SMS. 32
Consultation
mHealth can offer remote consulting services without any in-person visits. In research on patients with spina bifida, the application of a skincare app led to increased patient adherence to regime therapy, remote monitoring, as well as better communication between patients and the treatment team. 36 The majority of the participants in the current research agreed to provide medical and pharmacy counselling services through mobile phones with no appointments in-person.
The non-parametric statistical test was applied to investigate the views of individuals with various demographic characteristics, including gender, age, education, and work experience. The opinions of male and female respondents concerning mobile technology effectiveness in healthcare services were found to be just about the same. Further, the results indicated that there is no difference in opinion among people from various age groups. Such differences also were not observed among the subjects with different education levels. Also, the findings revealed that the differences in work experience do not lead to any variation in opinion concerning the application of mobile technology in healthcare services. Due to the popularity and high penetration rate of mobile phone use, it may be introduced for a wide range of usage disregarding age, gender, education, as well as work experience.
Conclusion
The current research follows two central objectives, first designing a questionnaire to assess public health personnel approaches to mobile phone application in their services and second evaluating their perspective to this technology. A questionnaire was suggested with 28 questions in five parts of health services effectiveness, education, notices, consultation, as well as follow-up. Staff perspective assessment reveals that there was no difference in opinion of people from various demographic characteristic, including gender, age, work experience, as well as education level toward mobile phone use in their services. Public health center staff attitudes toward the use of the mobile phone to deliver health services were generally positive, which would be an influential context for the successful application of mobile phones in public health; this context, in turn, would encourage users to apply and accept mHealth. Zamani et al. state that the attitude to the use of the mobile phone is an important alternative affecting m-learning acceptance by medicine students of Isfahan University of Medical Sciences. 37 Hence, the implementation of certain short and long-term programs in mobile phone apps and its abilities, including SMS or Multimedia Messaging Service (MMS) in public health centers, would be beneficial and may make appropriate context to reach higher quality in health services and improvement in patients’ lifestyle.
Based on the results of the present study, the following can be suggested: the designed questionnaire can be used in other areas of healthcare to evaluate the views of personnel regarding the use of mobile phones in providing services. Also, the positive view of the respondents of the present study shows the utility of mobile phones in various areas of public health, so managers can use this tool in various areas of service in public healthcare centers such as communicating with patients, providing reminders for medications and appointments, educating them and changing lifestyle. They can also evaluate their services and thus improve them by receiving patients' comments via mobile phone. Remote counselling services will be very useful without face-to-face visits, especially for the elderly and pregnant mothers who are unable to be present at all attendance visits. It will also be much easier to track the condition of patients by mobile phone. The results of the present study can help to increase the awareness of public health managers about the potential of mobile phones in providing services so that they can make more effective decisions about using these tools in health centers.
Footnotes
Acknowledgement
The authors would like to acknowledge all of the public health center staff for their assistance with data collection on this project.
Conflict of interest
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethical approval
The present study was approved by the Ethics Committee of Zahedan University of Medical Sciences (code: IR.ZAUMS.REC.1392.6379).
Contributorship
LE developed the study protocol, conducted data collection and drafted the manuscript. SH and MP contributed to data analysis and edited the manuscript. RB assisted with data collection and GA contributed in the final manuscript edition. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Student Scientific Research Center in Zahedan University of Medical Sciences for financially supporting this study with contract number 6379.
Guarantor
LE.
Peer review
Ammar K Almasri, Al-Balqa' Applied University, and Sivia Gaftandzhieva, University of Plovdiv, reviewed this article.
Appendix 1: The designed questionnaire to assess public health staff viewpoints about mobile phone use in the delivery of their services.

| Completely disagree | Disagree | No idea | Agree | Completely agree | ||
|---|---|---|---|---|---|---|
| Effectiveness of health service | ||||||
| 1 | The use of mobile technology improves the quality of public health services. | |||||
| 2 | Using mobile technology reduces the cost of providing public health services. | |||||
| 3 | Mobile technology improves self-management in public-healthcare professionals. | |||||
| 4 | The use of mobile technology expands the range of health services. | |||||
| 5 | The use of mobile technology creates equal access to facilities and services for the general public. | |||||
| 6 | Mobile technology improves interpersonal interactions between the provider and the recipient. | |||||
| 7 | Using mobile technology reduces the number of visits to health centers. | |||||
| 8 | Using mobile technology, travel costs for services are reduced. | |||||
| Education | ||||||
| 9 | Mobile technology makes public health education unrestricted. | |||||
| 10 | Mobile-based tutorials provide lifelong learning for people. | |||||
| 11 | Family planning training can be provided through mobile technology. | |||||
| 12 | Educational programs (including personal hygiene, oral care, and family planning) can be provided in the form of Bluetooth movies on client's mobile devices. | |||||
| 13 | Using mobile-friendly technologies is easy for everyone. | |||||
| Notices | ||||||
| 14 | Using mobile technology, notification is faster. | |||||
| 15 | Mobile notification helps improve disease prevention. | |||||
| 16 | Warnings on the prevalence of contagious diseases can be provided through mobile technology. | |||||
| 17 | Reminders for immunization and vaccination can be provided through mobile technology. | |||||
| 18 | By promoting mobile communication, health plans are promoted by individuals. | |||||
| Consultation | ||||||
| 19 | Therapeutic and pharmaceutical counselling can be done through mobile technology for individuals. | |||||
| 20 | Introduction of specialist physicians to patients can be done by mobile technology without a face-to-face visit for an appointment. | |||||
| Follow-up | ||||||
| 21 | Mobile notification facilitates follow-up services. | |||||
| 22 | Nutritional care for pregnant women and infants can be provided through mobile technology. | |||||
| 23 | The pursuit of pregnant women can be enhanced through mobile technology. | |||||
| 24 | The timing of attending can be provided through mobile phones. | |||||
| 25 | Reminders for medication use in patient groups can be provided via mobile phones. | |||||
| 26 | Mobile technology provides the opportunity to serve and attend the medical staff on the patient's bedside at any moment. | |||||
| 27 | Mobile technology facilitates the promotion of people's awareness in rural and harsh rural areas. | |||||
| 28 | Mobile notification reduces patients' need for unnecessary visits. | |||||