
Abstract
Background
Adequate digital competence is crucial for clinical nurses to effectively adapt to the evolving digital technologies in their practice. Currently, there is a lack of a brief assessment tool in China that comprehensively measures the digital competence of nurses in clinical practice across the dimensions of knowledge, skills, and attitudes. Therefore, this study aims to translate the Digital Competence Questionnaire (DCQ) into Chinese and evaluate its psychometric properties.
Methods
Following Brislin's translation model, the DCQ was translated and back-translated, and cultural adaptation and revisions of the Chinese version were conducted through expert consultations and a pilot survey. A cross-sectional study was carried out from July to October 2024 to conduct a methodological investigation on the translation and validation of the DCQ.
Results
The Chinese version of the DCQ includes two dimensions—attitude and knowledge & skills—with a total of 12 items. The overall Cronbach's α value for the questionnaire is 0.970, while Cronbach's α for the individual dimensions ranges from 0.921 to 0.945. The split-half reliability of the entire scale is 0.912, and the test–retest reliability is 0.846. Confirmatory factor analysis supported the hypothesized first-order two-factor model, with all fit indices demonstrating satisfactory values and remaining within acceptable levels.
Conclusion
The Chinese version of the DCQ has been successfully introduced in China, demonstrating strong psychometric properties. It can be used in healthcare settings as a tool to assess the digital competence of nurses, providing a basis for developing subsequent digital technology training programs and targeted interventions.
Introduction
Digital competence refers to an individual's overall ability to use digital technology effectively in a variety of tasks and contexts, and it covers not only an understanding of the use of technology, but also practical skills and attitudes and behaviors when interacting with technology.1,2 In 2006, digital competencies were recognized as one of the core competencies for lifelong learning among the final “eight core competencies” issued by the European Union Parliament and the Council of the European Union. 3 With the development of digital technology, clinical nurses spend most of their working hours providing direct care to patients in addition to acquiring skills in the use of electronic health record systems, the ability to manage and protect patient data, and proficiency in the operation of telemedicine equipment and software to ensure the provision of efficient and safe nursing care,4–6 and the resulting associated technological pressures have become a common problem in the clinical work environment. 7 Studies have shown that persistent technological stress can lead to burnout, decreased job satisfaction, and even increase nurses’ intention to leave their jobs, 8 therefore, having sufficient digital competence is critical for clinical nurses to be competent in their work with currently evolving digital technologies. 7
Currently, digital competence is evaluated through self-reported questionnaires, and some existing tools for assessing digital competence among clinical nurses primarily focus on individual knowledge and skills.9,10 For instance, a recent scoping review on nursing informatics competency assessment revealed that 10 out of 14 questionnaires solely concentrated on knowledge and skills topics. 11 Nevertheless, positive attitudes and favorable experiences with technology are crucial aspects in guaranteeing the successful adoption and utilization of digital technologies. 12 Additionally, in a review report on the digital competence of healthcare professionals, Konttila et al. further emphasized that beyond knowledge and skills, attitudes toward technology in the workplace should also be included in the understanding of digital competence. 13
As most current questionnaires include a large number of items, the time required to complete them indirectly hinders their usability. A research team 14 designed the TIGER-based Nursing Informatics Competencies (TANIC) tool, based on the Technology Informatics Guiding Education Reform (TIGER) standards, 15 to assess the nursing informatics competencies of newly hired and experienced nurses across three dimensions—basic computer skills, clinical information management abilities, and informatics knowledge—with a total of 85 items. However, in practical application, this process is time-consuming and labor-intensive. In clinical practice, nurses often face significant time constraints and heavy workloads, 16 making the development of a more efficient and concise assessment tool increasingly urgent. Moreover, most nursing information competency assessment tools developed internationally are based on evaluation frameworks such as the US Staggers Standards, the TIGER standards, the Canadian Nursing Information standards, and the Australian Nursing Information Competency Evaluation standards.17–20 These tools primarily emphasize communication technology and individual computer competency in their self-assessment sections.21,22 However, due to varying levels of digital maturity in healthcare systems across different regions, the relevance of these competencies is not uniformly perceived by all nurses in clinical practice.23,24
In China, the adoption of digital technologies among nurses is hindered by several unique challenges. One major issue is the disparity in digital maturity across different regions, particularly between urban and rural healthcare settings. While hospitals in metropolitan areas are equipped with advanced digital infrastructures, rural healthcare facilities often lack the necessary resources and support for digital integration. Additionally, nurses experience significant variations in digital skill levels and access to technological training, which further exacerbates the difficulties in utilizing digital tools effectively in clinical practice. For the development of digital competency assessment tools for nurses, China started late, and although the country has been gradually exploring the development of relevant assessment tools in recent years, they are mostly framed by relevant international guidelines and lack a certain theoretical foundation.10,25 Moreover, these tools have not fully accounted for the cultural differences, educational system, and technological acceptance specific to China's healthcare context. In recent years, with the rapid advancement of digital technologies, nursing practice has been increasingly exposed to a greater integration of digital tools and technologies, which has raised the demand for nurses to possess higher levels of digital competence to ensure the enhancement of care quality and efficiency. 26 Therefore, there is a pressing need for an effective and reliable tool specifically designed to measure the digital competence of clinical nurses within China's nursing environment. The Digital Competence Questionnaire (DCQ), recently developed by Golz et al., 27 is a concise tool designed to assess nurses’ digital competence in clinical practice. This questionnaire is structured around DeVellis's developmental guidelines and evaluates three key dimensions: knowledge, skills, and attitudes. Therefore, the aim of this study was to introduce the scale in China and to measure its psychometric properties through translation and cultural adaptation, in order to provide a reliable measurement tool for assessing the competence of clinical nurses in the use of digital technology.
Methods
Overview of the DCQ
The DCQ was developed by Swiss scholar Golz et al. 27 in 2023, starting with an initial item pool of 26 items derived from the original Delphi study. Following further psychometric validation, a concise 12-item questionnaire was formulated. 28 And with the original author's permission, we obtained this simplified version in advance. The scale encompasses two dimensions: knowledge & skills (6 items) and attitudes (6 items). Each item on the scale is rated using a 5-point Likert scale, ranging from “strongly disagree” (1) to “strongly agree” (5). The total score ranges from 12 to 60, with higher scores indicating a greater level of self-perceived digital competence. Clinical nurses can complete the questionnaire in less than 5 minutes. The Cronbach's α coefficients for the “knowledge & skills” and “attitude” dimensions of the scale were 0.81 (95% confidence interval [CI]: 0.79–0.82) and 0.91 (95% CI: 0.90–0.93), respectively, indicating good reliability and validity. Karvouniari et al. 29 conducted a cultural adaptation and reliability assessment of the instrument among Greek healthcare professionals, and the tool was validated among healthcare workers, showing a Cronbach's α of 0.826, indicating its suitability for measuring the digital competence levels of clinical nurses.
Study design
This cross-sectional study comprises two stages. In the first stage, the translation and cultural adaptation of the tool were accomplished. In the second stage, the psychometric evaluation of the instrument was performed. To ensure the quality and consistency of the study, this research adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The STROBE checklist was followed throughout the study design, data collection, and analysis process, which ultimately enhanced the reproducibility and reliability of the findings.
Stage I: translation and culture adaptation
Professor Golz was contacted via email, and permission to use the scale was obtained. The translation into Chinese, including translation, back translation, transcultural adaptation, and a pilot study, was conducted in strict accordance with Brislin's translation model. 30
Stage II: psychometric testing
Participants and setting
This study employed a cross-sectional survey to evaluate the Chinese version of the DCQ. Conducted from July to October 2024, participants were selected using convenience sampling from secondary and tertiary hospitals in Shandong and Guizhou provinces. The participants in this study were selected to ensure demographic diversity. Nurses were recruited from both urban and rural healthcare settings, as well as from different types of wards (e.g. general medicine, intensive care, and emergency departments). This approach helps to capture the variability in digital competence across different nursing roles and environments. As the study employed convenience sampling, potential biases associated with this method, such as overrepresentation of certain groups, were considered. To mitigate these biases, we made efforts to recruit from various healthcare institutions and used stratified sampling to ensure balanced representation across urban and rural settings. Inclusion criteria were: (1) possessing a registered nursing license; (2) actively involved in direct patient care; and (3) informed consent and voluntary participation in the survey. Exclusion criteria included: (1) nursing interns and rotating nurses (interns are nursing graduates working in hospitals for 9 months without independent practice rights; rotating nurses are those training from other hospitals); (2) nurse assistants and administrative nursing staff not involved in frontline work. Based on international guidelines for questionnaire design and principles of psychometric measurement, 32 an appropriate sample size is typically 10–20 times the number of survey items. Considering a 20% attrition rate, this study, which included 12 items, required a sample size of 144–264. Furthermore, exploratory factor analysis (EFA) suggested a minimum sample size of over 100, while confirmatory factor analysis (CFA) required more than 200. Ultimately, 559 clinical nurses were included in this study.
For the psychometric testing of the questionnaire, thresholds for reliability (e.g. Cronbach's α) and validity (e.g. content and construct validity) were set based on established guidelines in the literature. 33 The sample was split for EFA and CFA to ensure the robustness of the findings. The EFA was used to identify the underlying structure of the digital competence dimensions, while the CFA tested the fit of the hypothesized model. This approach strengthens the findings by validating the factor structure and ensuring that the instrument is both reliable and valid for assessing digital competence in clinical nursing. This study has been approved by the Hospital Ethics Committee (SWYX: No. 2023-470).
Data collection
We distributed an electronic questionnaire using the Wenjuanxing platform (http://www.wjx.cn), after obtaining approval from the relevant hospital management authorities. Detailed instructions for completing the survey were provided. The collected data included general demographic information and responses to the Chinese version of the DCQ scale, as shown in Supplementary Tables 1 and 2. The general demographic questionnaire was developed based on a literature review and expert opinions, covering variables such as age, gender, education, professional title, years of work experience, and type and level of the hospital. To ensure data quality, submission standards were set on the Wenjuanxing platform, allowing each IP address to complete the survey only once and requiring full completion before submission. After data collection, two researchers manually reviewed the responses and excluded invalid questionnaires. In total, 28 invalid questionnaires were excluded due to obvious response patterns, insufficient completion time, incomplete answers, or significant logical inconsistencies. Further details can be found in Supplementary Data. This procedure was completed manually to ensure a thorough review of each response, allowing for the identification of potential errors that statistical software might not detect, such as inconsistent or illogical answers.
Item analysis of the questionnaire
The suitability and reliability of scale items were assessed using the decision value method and the correlation coefficient method, and these methods also served as effective tools for selecting or revising items. 34 (1) Decision value method: The total scores of the Chinese version of the DCQ were ranked from lowest to highest. The bottom 27% formed the low-score group, and the top 27% formed the high-score group. Independent sample t-tests were conducted for each item between the two groups. Items were considered for deletion if the differences were not statistically significant (P > 0.05) or if the critical ratio (CR) was less than 3.0. 35 (2) Correlation coefficient method: Each item's score was analyzed for its correlation with the total scale score and the total dimension scores. Items with a correlation coefficient r ≥ 0.4 (P < 0.05) were retained. 36
Validity analysis
Six experts specializing in cultural adaptation were selected to evaluate the content relevance of each item. A 4-point Likert scale was used, with scores ranging from 1 (not relevant) to 4 (highly relevant), to assess the content of each item. The item-level content validity index (I-CVI) and the average scale-level content validity index (S-CVI/Ave) were calculated. If I-CVI is ≥0.78 and S-CVI/Ave is ≥0.90, it indicates that the scale has good content validity. 37
This study used principal component analysis with varimax rotation to conduct EFA to evaluate the structural validity of the Chinese version of the DCQ. The EFA followed three guiding principles: (1) factor loadings for each item should be ≥0.4; (2) the cumulative variance explained by all common factors should be ≥40%; and (3) each extracted common factor should include at least three measurement items. 38 Items that did not meet these statistical requirements were excluded. Before extracting the common factors, the Kaiser–Meyer–Olkin (KMO) test and Bartlett's test of sphericity were conducted. A KMO value greater than 0.8 and a significant Bartlett's test indicated suitability for factor analysis. 39 From the total sample, we randomly selected 200 cases for EFA to explore the underlying factor structure of the scale. The remaining 339 responses were used for CFA using the maximum-likelihood estimation method. This was done to test whether the factor model derived from EFA could be supported across different samples. In this model, common factors were treated as latent variables, and the relevant items were treated as observed variables. Structural validity of the scale was further assessed based on various fit indices, and the optimal ranges for fit indices are: χ2/DF (Degrees of Freedom) < 3, RMSEA (Root Mean Square Error of Approximation) < 0.08, and values for CFI (Comparative Fit Index), NFI (Normed Fit Index), GFI (Goodness of Fit Index), and TLI (Tucker-Lewis Index) greater than 0.90 indicate good model fit. 40
Reliability analysis
We conducted internal consistency and test–retest reliability analyses for the Chinese version of the DCQ. For reliability analysis, we calculated Cronbach's α coefficients for the overall questionnaire and for each dimension, along with split-half reliability, to evaluate internal consistency. 41 To assess test–retest reliability, 30 participants completed the translated questionnaire again after 2 weeks, and correlation coefficients were calculated to evaluate stability over time. We set a minimum threshold of 0.7 for Cronbach's α, split-half reliability, and test–retest reliability coefficients.42,43
Data analysis
Data analysis was undertaken using IBM SPSS Statistics version 29.0 (IBM Inc., Armonk, NY, United States) and AMOS 24.0 (IBM Corp., Armonk, NY, United States). If the quantitative data follows a normal distribution, it is expressed as the mean ± standard deviation. For data that does not follow a normal distribution, the median and interquartile range are used for descriptive statistics. Categorical data is summarized using frequency and percentage. Statistical significance was defined as a P value of less than 0.05.
Results
Cultural adaptation and translation of the DCQ
The translation and cultural adaptation of the DCQ followed Brislin's model to ensure reliability and validity. However, specific cultural adjustments were made to better align the questionnaire with Chinese healthcare practices and sociocultural contexts. For example, the item “Digital technology fits well with the way I like to work” was translated as “Digital technology aligns well with my preferred way of working,” reflecting the local cultural understanding of work practices and attitudes toward technology, which may differ from Western contexts. Feedback from a panel of Chinese clinical nurses and healthcare professionals played an essential role in refining the tool. For instance, “office space” was replaced with “workplace” to better match the typical working environment of nurses. Additionally, some phrases related to patient outcomes and digital tools were adjusted to ensure they were relevant and accurately understood in the context of Chinese nursing. For instance, terms such as “electronic health records” and “telemedicine” were used to align with common terminology in Chinese healthcare settings. The final version of the questionnaire was revised based on expert feedback to improve clarity, cultural appropriateness, and relevance, ensuring that all items were easily understood by Chinese nurses and reflected their experiences with digital tools in practice.
The general demographic characteristics
Among the 559 clinical nurses included in this study, 439 (78.5%) were female, reflecting the predominant gender composition of the nursing workforce in China. Of the 559 nurses, 367 (65.6%) were married, while 192 (34.4%) were single or divorced. In terms of years of experience in their current department, 241 nurses (43.1%) had worked for 0–5 years, 127 nurses (22.7%) for 6–10 years, and 191 nurses (34.2%) for more than 10 years. Additionally, 239 participants (42.7%) reported having received training in digital technologies, highlighting the growing integration of digital tools in nursing education and practice. This finding underscores the necessity of a validated tool to assess digital competence, as variations in training and exposure could significantly impact nurses’ ability to adopt and utilize digital technologies effectively. Further details can be found in Table 1.
Demographic characteristics of participants (N = 559).

Item analysis of the questionnaire
The decision value method results indicated that the CR values for all items ranged from 15.928 to 25.529 (P < 0.001), all exceeding the threshold of 3.000, suggesting good discriminatory power. Consequently, all 12 items were retained. Similarly, the correlation coefficient method showed that the correlation between each item score and the total score of the Chinese version of the DCQ ranged from 0.774 to 0.900 (P < 0.001 for all), indicating high homogeneity among the items and the overall scale, resulting in no items being removed.
Evaluation of psychometric properties of the questionnaire
Content validity
A total of six experts participated in the evaluation, resulting in item-level I-CVI values ranging from 0.830 to 1.000 and a scale-level S-CVI/Ave of 0.986. Both values exceeded the reference thresholds, indicating good content validity. This suggests that the items in our study were well-designed and consistent with the measurement objectives.
Construct validity
The factor structure of the Chinese version of the DCQ aligns with the theoretical framework that defines digital competence as a multidimensional construct encompassing knowledge, skills, and attitudes. The CFA supported a two-factor structure consisting of attitude and knowledge & skills, which is consistent with the original DCQ framework. The attitude dimension reflects nurses’ perceptions, confidence, and willingness to engage with digital technologies, while the knowledge & skills dimension assesses their proficiency in using digital tools in clinical settings. The consistency of this factor structure across different cultural and healthcare contexts suggests that the DCQ is a robust instrument for evaluating nurses’ digital competence. Additionally, the KMO value was 0.935, and Bartlett's test of sphericity was significant (χ2 = 2725.632, P < 0.001), indicating that the scale was suitable for EFA. Principal component analysis initially extracted one common factor with an eigenvalue greater than 1, accounting for 73.520% of the total variance. However, based on previous research, 44 a two-factor model was applied using varimax rotation, which increased the cumulative variance contribution to 80.647%, with all item factor loadings exceeding 0.4. Factor loadings were satisfactory. The attitude factor (items 1–6) and knowledge & skills factor (items 7–12) were consistent with the theoretical framework, as expected. Scree plot is shown in Figure 1, and factor loadings are detailed in Table 2.
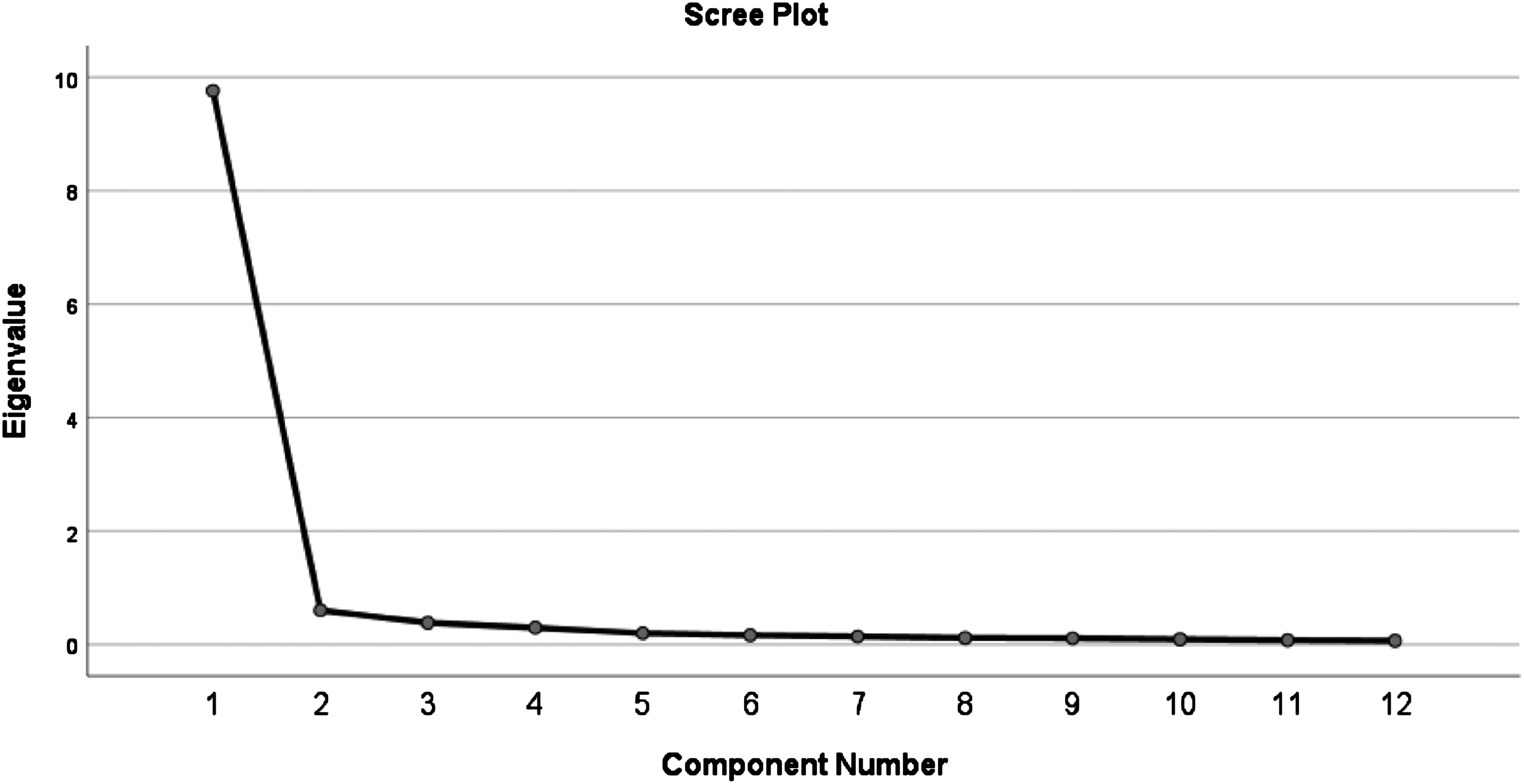
Scree plot of exploratory factor analysis for Chinese version of the DCQ.
Factor loadings of exploratory factor analysis for the Chinese version of the Digital Competence Scale (n = 200).
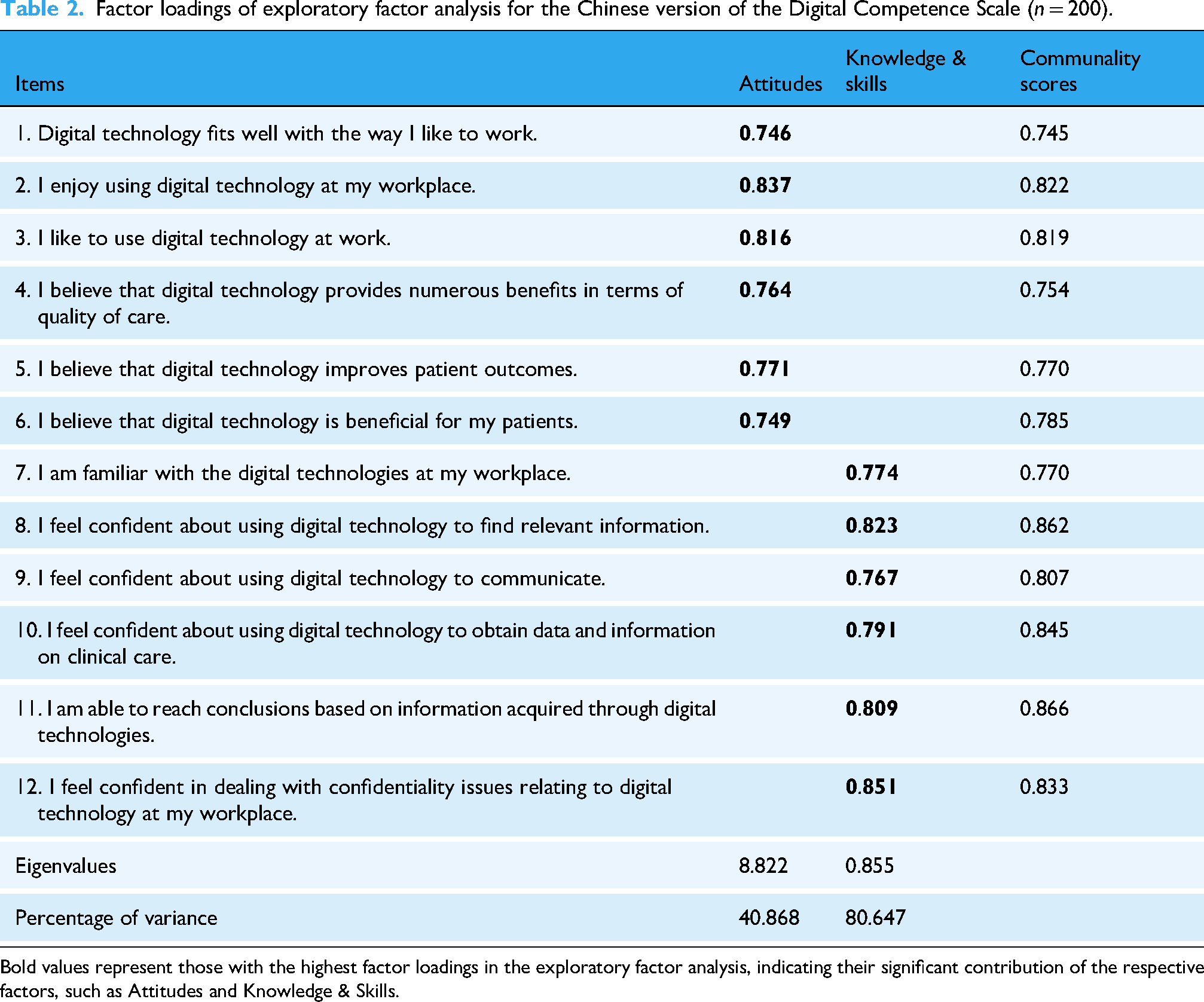
Bold values represent those with the highest factor loadings in the exploratory factor analysis, indicating their significant contribution of the respective factors, such as Attitudes and Knowledge & Skills.
CFA was conducted on data from 359 questionnaires using AMOS software. The model fit was assessed based on the two-factor structure of the scale (Figure 2). The initial CFA model yielded a χ2/DF value greater than 3, indicating the need for modifications to achieve an acceptable model fit. Upon reviewing the modification indices (MIs), a high correlation was observed between items 5 (“I believe that digital technology improves patient outcomes”) and 6 (“I believe that digital technology is beneficial for my patients”). Given the conceptual overlap between these two items, a covariance path was added between their error terms, significantly improving the model fit indices. This modification was theoretically justified, as both items assess perceptions of the impact of digital technology on patient care, which may inherently share variance. After this adjustment, all fit indices met the recommended thresholds, ensuring the structural validity of the questionnaire. Future studies could further refine these items to minimize redundancy while preserving the comprehensive nature of the instrument. Specific fit indices are provided in Table 3.

Standardized two-factor structural model of the DCQ (n = 359).
Goodness of fit indices.

Internal consistency, split-half reliability, and test–retest reliability
The reliability of the Chinese version of the DCQ was evaluated through internal consistency, split-half reliability, and test–retest reliability. The overall Cronbach's α coefficient for the Chinese DCQ was 0.970, while the two dimensions, attitude and knowledge & skills, had Cronbach's α values of 0.945 and 0.921, respectively. The overall split-half reliability was 0.912, with the dimensions having split-half reliability values of 0.907 and 0.953. The overall test–retest reliability was 0.846, with reliability values of 0.818 for attitude and 0.755 for knowledge & skills. Further details are provided in Table 4.
Reliability analysis for the Chinese version of the DCQ.

DCQ: Digital Competence Questionnaire.
Discussion
The digitization of healthcare has reshaped nurses’ roles, impacting nursing practice, quality of care, care ethics, and even environmental sustainability. It has also opened numerous opportunities for integrating digital technologies into nursing.45,46 The importance of digital competence for clinical nurses is undeniable, especially in the modern healthcare setting, where it has become essential for delivering high-quality care. 10 Enhancing nurses’ digital skills not only supports their professional growth but also serves as a foundation for improving the efficiency and quality of the entire healthcare system. Similar to the study by Karvouniari et al. 29 in Greece, which focused on translating and validating a digital competence tool for healthcare professionals, the research by Golz et al. 47 also highlights the growing importance of digital competence in healthcare. Both studies underscore the necessity of culturally and contextually adapting digital competence assessment tools, such as the DCQ, to fit diverse healthcare environments, including those in China and Switzerland.
The digital maturity of the healthcare system in China plays a pivotal role in shaping the utility of the DCQ. As China advances in digital healthcare, the disparities between urban and rural areas in terms of access to digital technologies remain a significant challenge. Urban hospitals are often equipped with advanced digital infrastructure, such as electronic health records and telemedicine systems, which facilitate the integration of technology into daily healthcare practices. In contrast, rural healthcare settings frequently face limitations in both technology access and digital training for healthcare workers. Given these disparities, the DCQ serves as a critical tool for evaluating the digital competence of nurses across different regions, helping identify areas that require improvement. By assessing digital competence, the DCQ not only contributes to understanding the current digital landscape but also guides efforts to address digital gaps, particularly in underserved areas. This aligns with China's healthcare reform goals of improving care quality and efficiency through digital transformation, emphasizing the importance of equipping nurses with the necessary digital skills to utilize emerging technologies effectively. In this study, we completed the translation of the DCQ into Chinese following standard scale translation procedures. This is the first time the DCQ has been translated into Chinese, and its psychometric properties were verified through factor analysis. Reliability and validity analyses indicate that the 12-item DCQ is a reliable and valid tool.
The Chinese version of the DCQ exhibits strong validity
Validity refers to the extent to which a scale accurately reflects the concept being measured, often assessed using content and construct validity.37,48 In this study, six experts, all with extensive experience in medical informatics, clinical nursing, or nursing research, evaluated the scale items. The results showed that the I-CVI ranged from 0.830 to 1.000, and the S-CVI/Ave was 0.986, suggesting that the scale effectively reflects the intended content. Construct validity was evaluated using EFA. Principal component analysis with varimax rotation was conducted, extracting two factors with eigenvalues greater than 1, named “attitude” (items 1–6) and “knowledge & skills” (items 7–12). The original CFA model demonstrated suboptimal fit, as indicated by a χ2/DF value greater than 3. This suggested the need for further adjustments to enhance model adequacy. Upon reviewing the MIs, it was observed that items 5 and 6 had notably high MI values. Conceptually, these two items appeared to share overlapping content, both focusing on the perceived benefits of digital technology for patients. Given this conceptual overlap, it was reasonable to introduce a covariance between their error terms. After implementing this modification, the model demonstrated significantly improved fit, with all indices reaching acceptable levels. This adjustment likely accounts for shared variance related to the positive perceptions of digital technology, which was not initially captured in the factor structure. This finding underscores the importance of considering the conceptual relationship between items when evaluating model fit. Future iterations of the DCQ should consider refining these items to further reduce redundancy and enhance discriminant validity.
The Chinese version of the DCQ shows high reliability
Reliability describes the consistency, stability, and dependability of test results, typically expressed through internal consistency. A higher reliability coefficient indicates greater consistency, stability, and reliability of the test outcomes. 43 Generally, a Cronbach's α coefficient above 0.70 is considered indicative of good internal consistency reliability, while a test–retest reliability greater than 0.7 indicates good temporal stability. 42 The Cronbach's α for the Chinese version of the DCQ was 0.970, and the coefficients for the individual dimensions ranged from 0.921 to 0.945, all above 0.7, indicating strong internal reliability of the Chinese DCQ, which effectively reflects Chinese nurses’ ability to use digital technologies in clinical settings. Despite demonstrating good internal consistency, additional assessments such as split-half reliability and test–retest reliability were also conducted. The overall split-half reliability was 0.912, with dimension-specific coefficients of 0.907 and 0.953, suggesting high internal consistency. Test–retest reliability evaluates whether repeated measurements using the tool produce consistent results over time. 49 In this study, the overall test–retest reliability was 0.846, with values of 0.818 and 0.755 for the individual dimensions, indicating good temporal stability of the scale.
The Chinese version of the DCQ demonstrates significant clinical applicability
With the continuous introduction of information technology, nurses are facing increasing technical pressures.47,50 New systems and devices require ongoing learning and adaptation, which can be particularly challenging for older nurses who may struggle to keep up with the rapid pace of technological advancements. For example, complex electronic health record systems may require significant time for learning and adaptation, adding to the workload and increasing stress, which can lead to burnout and decreased job satisfaction.26,51 The development of information technology has brought unprecedented opportunities and convenience to clinical nursing, making care delivery more precise, efficient, and sustainable. However, it also presents numerous challenges for clinical nurses, including the need for continuous skills updates, privacy concerns, and increased psychological stress. Therefore, it is highly meaningful to explore the factors that affect the digital competence of clinical nurses and to develop targeted strategies for enhancing their digital skills. This makes the development or introduction of a specific measurement tool for assessing the digital competence of clinical nurses particularly valuable. In this study, we followed a strict scale introduction process, 52 including forward translation, back-translation, review by the original author, cultural adaptation, and a pilot survey to create the Chinese version of the DCQ. The findings of this study demonstrate the potential of the DCQ to be integrated into various facets of nurse education, training, and performance evaluations. By assessing nurses’ digital competence, healthcare organizations can identify specific areas where further training and development are needed. For example, integrating the DCQ into nursing education curricula could ensure that future nurses are equipped with the necessary skills to thrive in a digital healthcare environment. Furthermore, the tool can be used for performance evaluations, helping to track nurses’ digital skills and knowledge over time. This is especially important in underserved or rural areas, where access to digital training and resources may be limited. In such settings, the DCQ could be instrumental in identifying gaps in digital competence and directing interventions aimed at enhancing nurses’ ability to use digital technologies effectively.
Future research should focus on further validating the DCQ in diverse samples across different regions of China, especially in rural areas where healthcare workers may have limited access to digital resources. Additionally, testing the DCQ among other healthcare professionals, such as physicians and allied health workers, could help extend its applicability and refine its use in various healthcare contexts. By expanding the scope of the tool, researchers can gain a more comprehensive understanding of digital competence across healthcare professions and facilitate the integration of digital technologies into all levels of care.
Limitations
While the limitations of this study are acknowledged, further discussion is warranted regarding the exclusion of interns, rotating nurses, and administrative staff from the sample. The decision to exclude these groups could limit the generalizability of the findings, as it may not fully represent the diverse experiences and digital competence of all nursing staff. Specifically, interns and rotating nurses may have different levels of exposure to digital tools, and administrative staff could offer valuable insights into the broader healthcare environment and its integration with digital technology. Future studies could consider including these groups to enhance the breadth and applicability of the results. Additionally, as with most self-reported data, this study may be subject to biases such as social desirability bias, where participants may have reported higher levels of digital competence to align with perceived expectations. To mitigate such biases in future studies, strategies such as ensuring anonymity, providing clear instructions, and including objective measures (e.g. observational assessments) could be implemented. These measures would help reduce the impact of social desirability bias and improve the accuracy and reliability of the data collected.
Conclusions
This study strictly followed the scale adaptation process and evaluation standards to translate and validate the reliability and validity of the DCQ scale. The Chinese version of the DCQ consists of two dimensions, with a total of 12 items, maintaining consistency with the original structure and demonstrating high reliability and validity. The succinct items and streamlined assessment enhance practicality. The Chinese version of the DCQ can effectively assess the digital competence of clinical nurses in China and serve as a basis for related digital training programs in clinical settings. The validated tool developed in this study plays a crucial role in addressing the challenges of digital transformation in nursing practice. By offering a comprehensive assessment of nurses’ digital competence, it enables healthcare organizations to identify gaps in digital skills and implement targeted interventions to enhance overall digital competence. This tool can serve as a reliable instrument for guiding the integration of new digital technologies in healthcare settings, helping nurses adapt to rapidly evolving digital environments. In addition, the tool has several practical applications that can contribute to the ongoing improvement of digital competence in nursing. It can be used to evaluate the effectiveness of digital training programs, tracking changes in nurses’ digital skills before and after training. This will allow healthcare providers to assess the success of training initiatives and refine them for better outcomes. Furthermore, the tool can be used to monitor progress in digital competence over time, offering valuable insights into how nurses’ digital competencies evolve in response to advancements in technology and changes in healthcare practice. These applications will ultimately support the continuous enhancement of digital skills among nurses, ensuring they are well-prepared to manage the increasing demands of digital transformation in the healthcare sector.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251332987 - Supplemental material for Translation and psychometric evaluation of the Chinese version of the Digital Competence Questionnaire for clinical nurses
Supplemental material, sj-docx-1-dhj-10.1177_20552076251332987 for Translation and psychometric evaluation of the Chinese version of the Digital Competence Questionnaire for clinical nurses by Zhengang Wei, Hongli Liu, Jicheng Zhang, Yan Chen, Lixia Chang, Huiyu Cheng, Xue Bai, Xiaohua Wang and Su Li in DIGITAL HEALTH
Supplemental Material
sj-xlsx-2-dhj-10.1177_20552076251332987 - Supplemental material for Translation and psychometric evaluation of the Chinese version of the Digital Competence Questionnaire for clinical nurses
Supplemental material, sj-xlsx-2-dhj-10.1177_20552076251332987 for Translation and psychometric evaluation of the Chinese version of the Digital Competence Questionnaire for clinical nurses by Zhengang Wei, Hongli Liu, Jicheng Zhang, Yan Chen, Lixia Chang, Huiyu Cheng, Xue Bai, Xiaohua Wang and Su Li in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Christoph Golz for providing the original version of the questionnaire. His support was invaluable in the adaptation process. Additionally, we would like to thank all participants involved in this study for their contributions.
Guarantor
Xue Bai.
Ethics considerations and consent to participate
All procedures performed in studies involving human participants were approved by the Ethics Committee of the Shandong First Medical University Affiliated Provincial Hospital. The experimental protocol was approved by the Ethics Committee (SWYX: No. 2023-470) and conducted in accordance with the principles of the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards.
Informed consent
Written informed consent was obtained from all participants included in the study.
Author contributions/CRediT
ZW designed the study, collected and analyzed data, interpreted results, and drafted the manuscript. XB and XW revised the manuscript. HL analyzed data and contributed to the manuscript. JZ, YC, LC, HC, and SL assisted in data collection. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China, the Science and Technology Fund Project of Guizhou Provincial Health Commission, Shandong Provincial Medical and Health Science and Technology Project the China International Medical Foundation (grant number 61861047, gzwkj2024-575, 202319010307, 2-2018-35-2004).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.