
Abstract
The objective of this study was 1) to assess the length of stay in hospital after birth among multiparous and primiparous women, 2) to investigate relational continuity of midwifery care, 3) to investigate the validity and reliability of the home visit questionnaire, and 4) to investigate the possible positive influences of a home visit by a midwife two to six days after birth. A total of 85 postnatal women participated in the intervention group, which received home visits from a midwife, while 98 women participated in the control group, which did not receive home visits from a midwife. Of the multiparous women, 16.9% left hospital within 24 hours after birth, whereas only 4.0% of the primiparous women left hospital at this stage. No significant differences between the intervention group and the control group were evident with regard to the length of the postnatal stay. However, considering the primiparous women in the total sample, the intervention group tended to leave hospital earlier than the control group. The women who received a home visit from a midwife reported higher scores on the experience of predictability and continuity in the postnatal care than the control group. The primiparous women experienced the home visit to have a significant influence on their ability to handle the care of their newborn baby, on their mental health, and their feeling of being recognized and supported. A home visit by a midwife early after discharge from hospital seems to have a positive health-promoting influence on primiparous women's confidence and ability to handle the care of their newborn babies, and on perceived support, predictability and continuity of midwifery care.
Introduction
In Norway, the duration of postnatal stay in hospital for women with uncomplicated births has been substantially reduced. 1 Early discharge from hospital for the woman and her newborn baby is often 6–24 hours after birth and normal discharge is approximately 48 hours after birth. This reduction of the postnatal stay in hospital is judged to increase stress during the first days at home, affecting breastfeeding and the woman's ability to cope with daily activities involving the newborn baby.2,3 As mothers have a strong desire to cope with motherhood, they tend to put aside their own basic needs, such as eating, sleeping and pain relief. Consequently, the lack of a follow up shortly after birth may affect the family's health adversely. 2 Many parents are caught in their feelings of incompetence because they do not know how to satisfy the baby's needs. When discharged early from hospital it is essential to get support from health professionals in order to build parental confidence. 3 Professional care following birth represents an important support mechanism and a significant contribution to the long-term health and wellbeing of the mother and her baby. Accordingly, midwifery care in the postnatal period represents an essential component of health promotion and a key concern of the public health services.4,5 It is emphasized that health promotion in the postnatal period includes professional support to enhance the family's ability to cope in their new life situation.6,7 According to the World Health Organization, health promotion is the process of enabling people to increase control over, and to improve their health. 8
In Norway, antenatal care is part of the primary health service, while the specialist health service is responsible for intrapartum and early postnatal care. As a result, the care is fragmented and the women encounter several different midwives and other professionals instead of continuous and trusting relationships. The Norwegian Directorate of Health
9
has emphasized that continuity and integrated services are important for achieving the best possible outcome for the women. Several studies have shown that women who experience relational continuity of care are more likely to be satisfied with their care than women who are offered other types of care.10–12 Relational continuity is defined as ‘an ongoing therapeutic relationship between a patient and one or more providers’.13(p.1220) Haggerty et al. define continuity as the degree to which a series of discrete healthcare events are experienced as coherent and connected and consistent with the patient's medical needs and personal context. Continuity of care is distinguished from other attributes of care by two core elements: care over time and the focus on individual patients.13(p.1221)
The present study examines the length of postnatal stay in hospital and possible health-promoting influences within the framework of a clinical collaboration project between a university hospital and a public health clinic in Mid-Norway. The objective of the project was to offer women at a public health clinic a home visit by a midwife, representing relational continuity, two to six days after childbirth. A secondary aim of the project was to reduce the length of the postnatal stay in hospital by offering midwifery care at home. This project was based on a model of relational continuity of care, where the midwife responsible for the care of the woman during pregnancy at the public health clinic also offered a home visit to the family in the postnatal period. The midwife made an appointment for the home visit the day after the woman left the hospital. At the home visit, the midwife offered individual care such as guidance in breastfeeding and baby care. The home visit also included physiological examination of the baby and the mother. The midwife offered to have a dialogue about the birth and the woman's birth experience. The home visit by the midwife did not replace the ordinary home visit by the public health nurse 7–14 days after birth.
Objectives
The objectives of this pilot study were 1) to assess the length of stay in hospital after birth among multiparous and primiparous women, 2) to investigate relational continuity of midwifery care, 3) to investigate the validity and reliability of the home visit questionnaire, and 4) to investigate the possible positive influences of a home visit by a midwife during the first days at home after birth. We expected that primiparous women would need more support from professional caregivers and therefore wish to stay longer in hospital than multiparous women. Furthermore, we presumed that when offered a home visit by a midwife, primiparous women would feel more comfortable in leaving hospital early and be better able to cope with the care of their newborn baby. Thus, knowing that they would receive a home visit by a midwife might lead to a shorter stay in hospital for primiparous women. The hypotheses tested were: H1: Multiparous women leave hospital earlier after birth than primiparous women. H2: When offered a home visit by a midwife shortly after birth, primiparous women will leave hospital during the first 48 hours after birth. H3: The postnatal women in the intervention group experience more predictability and continuity of care during the postnatal period than women in the control group. H4: A home visit by a midwife shortly after birth positively influences coping with the care of the newborn baby, feelings of support, perception of relational continuity of care and benefit mental health among primiparous women.
Methods
The participants in the intervention group were 85 out of 93 women at a public health clinic who had received a home visit by a midwife during the early postnatal period. Participants in the control group were women belonging to a similar public health clinic in the same area of the Norwegian city who had not received a postnatal home visit by a midwife. The inclusion criteria were the same for both groups: a woman who had a healthy newborn baby at term and command of the Norwegian language. The participants in the intervention group were requested to participate by the midwife during the home visit two to six days after birth, whereas participants (98 out of 100) in the control group were asked to participate by the public health nurse during the ordinary home visit 7–14 days after birth. The women were given written and verbal information about the aim of the study as well as the terms of confidentiality. They subsequently signed a written consent form. The Regional Research Ethics Committee approved the study (Ref.nb. 2014/56).
Data collection
Quantitative data were collected from the intervention and the control group from December 2013 to December 2014. Six weeks after the birth, the women in both groups answered a questionnaire at the public health clinic. In total, 183 out of 193 women (intervention group n = 85, control group n = 98) with different backgrounds completed the questionnaire, giving a response rate of 95%.
Measures
Relational continuity of care was assessed by means of the Relational Continuity Scale (RCS). This scale comprising ten items was developed based on theory and previous research in 2013. The RCS was validated among postnatal women revealing good psychometrical properties in this population. 20 Among sample items were ‘To what extent did you experience care as predictable?’ ‘To what extent did you experience continuity of care during pregnancy, birth and the postnatal period?’ and ‘Overall, to what extent were you satisfied with the care during pregnancy, birth and the postnatal period?’
The influence of the home visit by the midwife was assessed with help of the Home Visit Questionnaire (HVQ) developed by the authors for this study. The questionnaire was based on theory and evidence2,3,5,7,15,16 and contained eight items, with scores on a Likert scale from not at all (1) to very much (5). An example item was: ‘To what extent did the home visit influence your experience of coping with the care of your newborn baby?’ The women's experiences of acknowledgement and support during the home visit by the midwife was assessed by means of a one-item index framed AS1: ‘To what extent did you feel acknowledged and supported during the home visit?’ Demographic variables such as the length of the postnatal stay in hospital, age, education and parity were included in the questionnaire. Since the control group did not receive the home visit by a midwife, the home visit questionnaire was administered only to the intervention group.
This study evaluated the possible influences of the care model termed ‘relational continuity of care’.13(p.1220) That is, we merely considered postnatal women's experiences of the home visit by the midwife, and did not assess the experiences of the ordinary visit by the public health nurse, which was not within the scope of this study. Therefore, the present data do not provide a possibility for comparing the influence of the visit by the public health nurse contra the home visit by the midwife.
Statistical analysis
The data were analysed using descriptive statistics, correlational analysis and independent t-tests for equality of means, using SPSS Version 22.0 (IBM, SPSS Inc, Chicago, IL, USA). P-values < 0.05 were considered statistically significant. 21 The variable sense of coherence (SOC) was included in the questionnaire, but the SOC data are not part of the study presented in this article. Power calculation was based on SOC values from a recently published study examining ‘fear of birth’ during pregnancy among healthy pregnant women. 22 The significance level of 0.05 was used (two-sided test), strength (1-beta) 0.80, and changes in SOC of 5 (delta), revealing a minimum of 71 participants in each group. Hence, the sizes for the intervention and control groups (n = 85 and 98) in this study conveniently exceeded the advisable threshold. Confirmatory factor analysis (CFA) was used to examine the measurement model of the HVQ. The overall model fit can be assessed statistically by the chi-square (χ2); a small χ2 and a non-significant p-value corresponds to good fit, 23 the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR) with values below 0.05 indicating good fit, whereas values smaller than 0.08 are interpreted as acceptable.24,25 In addition to the overall model fit, measures based on model comparison were used: the comparative fit index (CFI) and the non-normed fit index (NNFI) with an acceptable/good fit at 0.95/0.97 and above, and the normed fit index (NFI) with an acceptable/good fit at 0.90/0.95.24,25 The frequency distribution was examined showing that both skewness and kurtosis were significant. Thus, the robust maximum likelihood (RML) estimation procedure was applied, using an asymptotic covariance matrix, stating the Satorra–Bentler scaled chi-square (χ2). 26 Running CFA, missing data were handled by means of the listwise procedure.
Results
Demographics
Demographic variables for the total sample and the intervention and control group. Independent t-test for comparing means between the intervention and the control group.
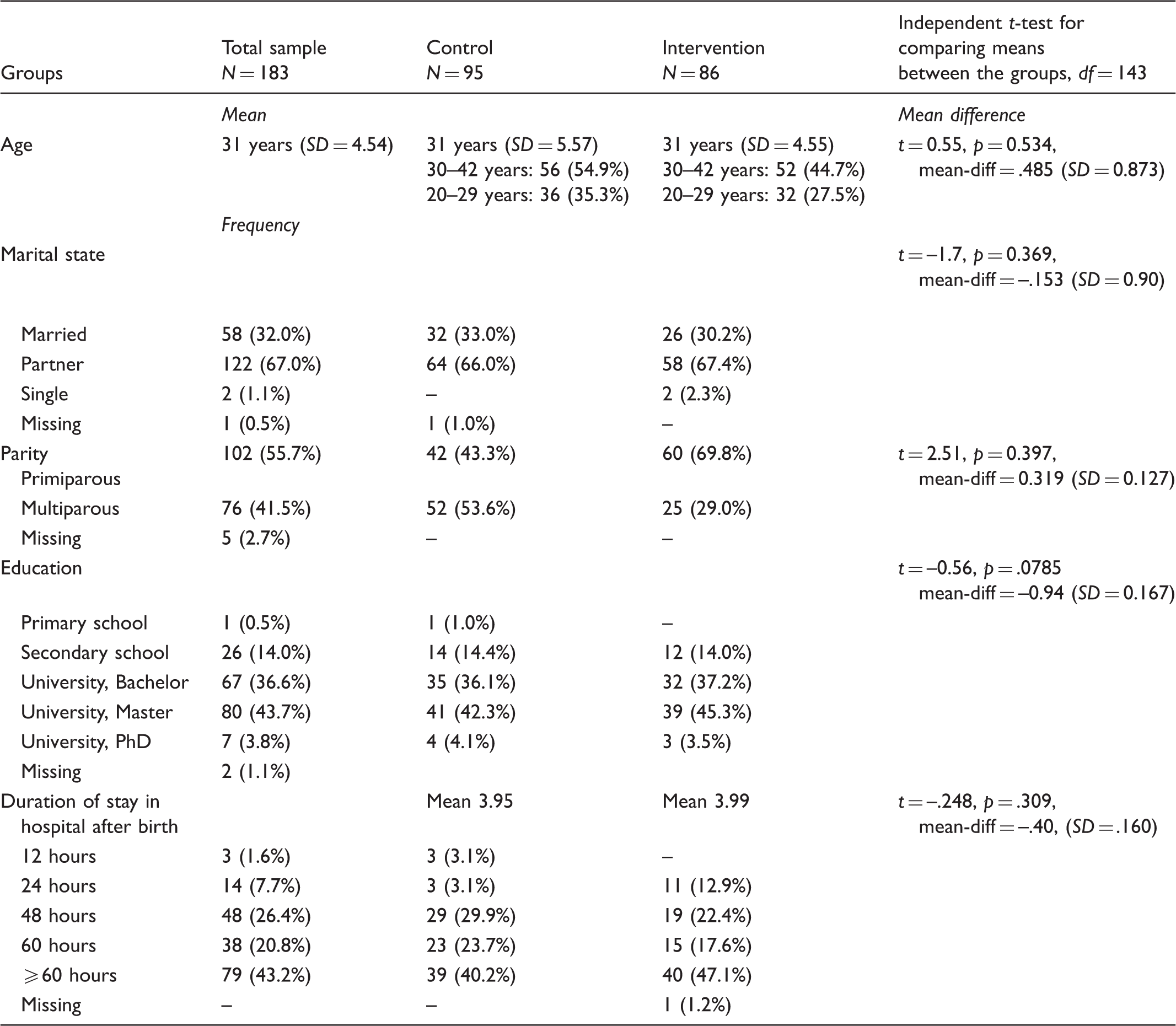
Note: SD = standard deviation; df = degrees of freedom.
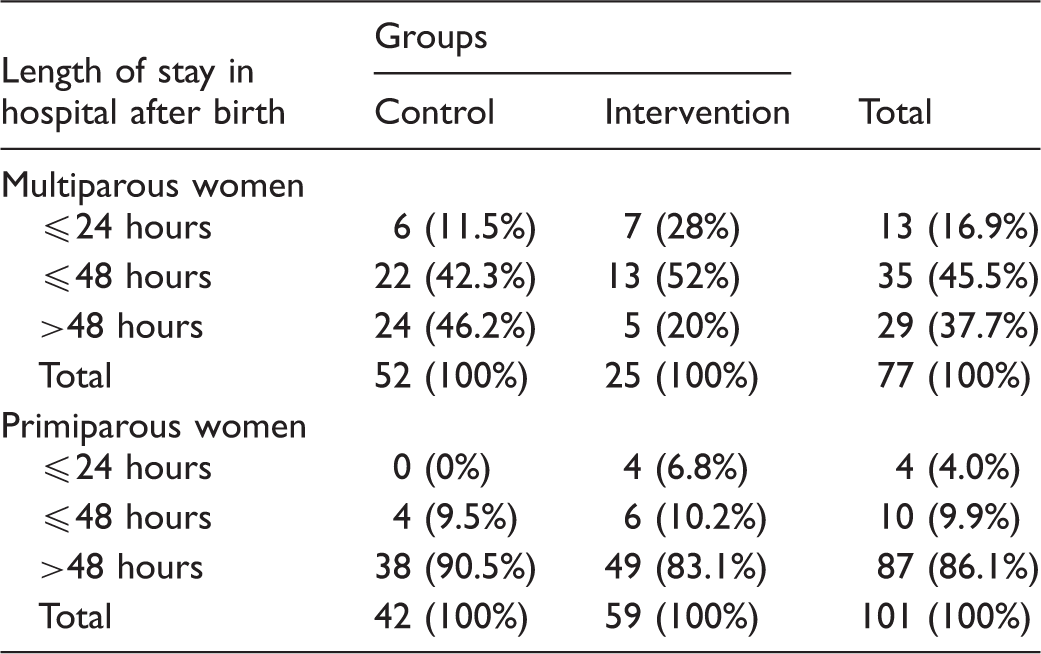
Length of stay in hospital after birth
Descriptive statistics, crosstabulation. Length of stay in hospital after birth reported by the control group and the intervention group, sorted by parity (primiparous and multiparous).
Primiparous women in the intervention and control groups – differences
Primiparous women's length of postnatal stay in hospital by the intervention and the control group.

Note: *significant at the 0.05 level. SD = standard deviation, sd.e. = Standard Error Mean, df = degrees of freedom, st.diff.error = Standard Error Difference.
Relational continuity of care
Relational Continuity Scale (RCS); means, standard deviation and independent t-test for equality of means between the control group and the intervention group.
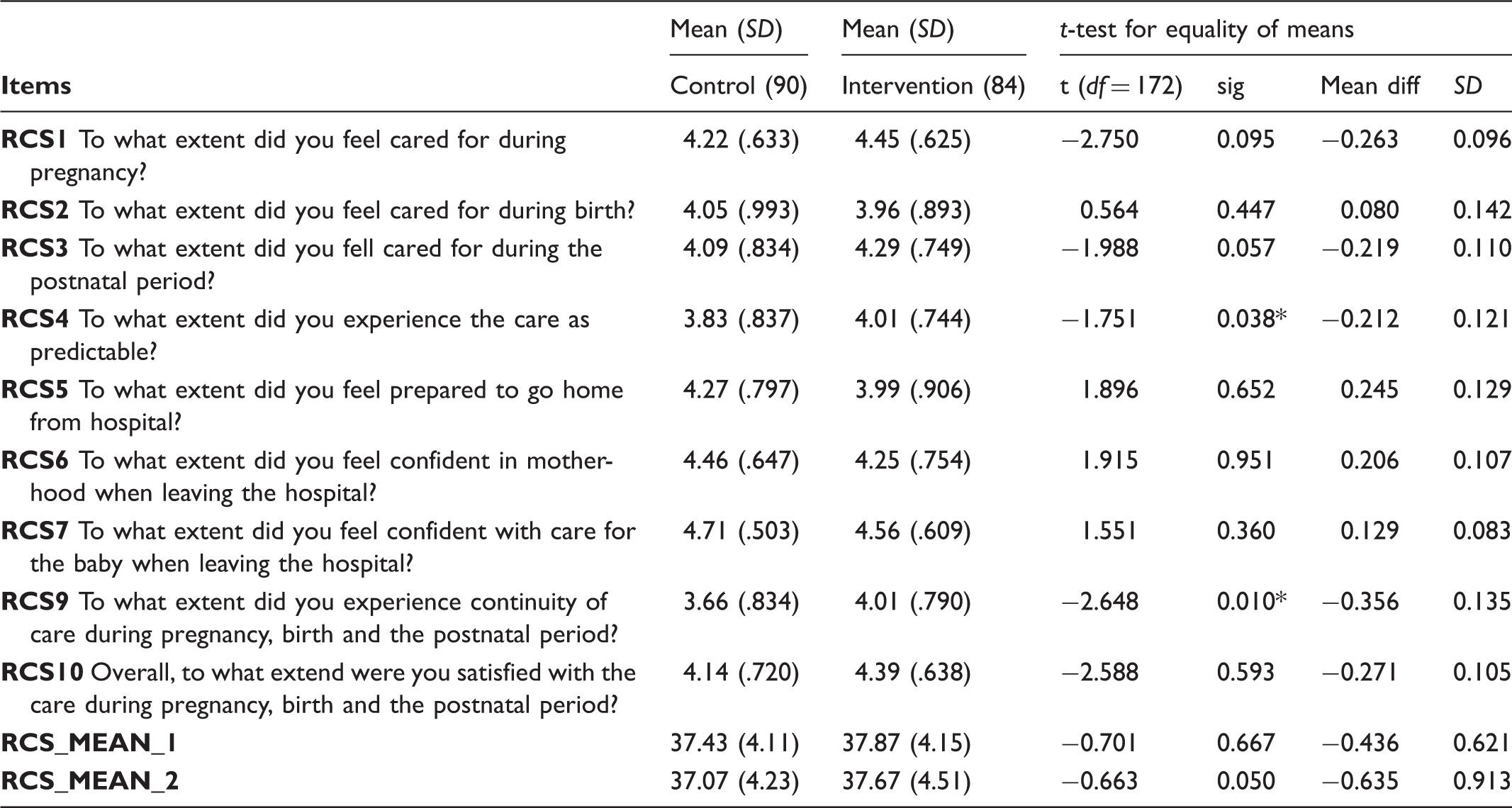
Note: *significant at the 0.05 level. Listwise N: Control group N = 90, Intervention group N = 84. Item RCS8 revealed non-significant correlations with the other scale items, probably due to a bad wording. Therefore, this item was excluded from the analysis. RCS_MEAN_1 = mean score for RCS scale in the whole sample. RCS_MEAN_2 = mean score for RCS scale among primiparous women.
The Home Visit Questionnaire (HVQ) – validity and reliability
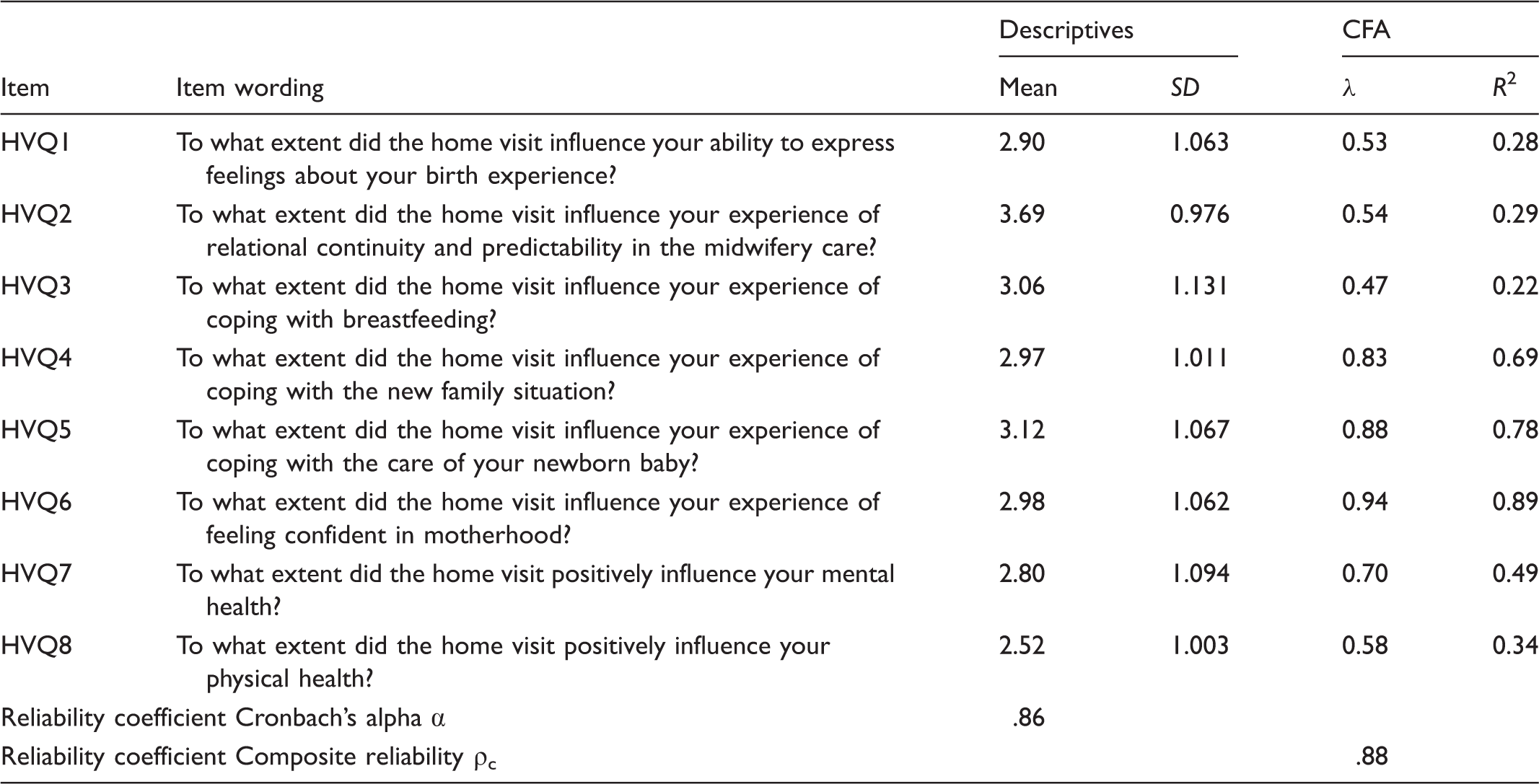
The measurement model of the HVQ including eight items was evaluated by means of confirmative factor analysis. Factor loadings (λ) between 0.94–0.47 with only one λ < 0.5 for item HVQ3, and squared multiple correlations (R2) between 0.22–0.89 were exposed, as well as acceptable fit indices: χ2 = 38.98, p = 0.0067, χ2/df = 1.95, RMSEA = 0.11, 90% confidence interval RMSEA = 0.054–0.15, NFFI = 0.95, CFI = 0.97, SRMR = 0.069. Good values for the reliability coefficients Cronbach's alpha (α = .86) and composite reliability (ρc = .88) were shown. Thus, the validity and reliability of the HVQ in this study seemed acceptable. Figure 1 portrays the HVQ measurement model. Table 5 shows estimates for the HVQ measurement model as well as the theoretical model tested.
Measurement model for the Home Visit Questionnaire (HVQ). Home Visit Questionnaire (HVQ): items, means, standard deviation (SD), confirmative factor analysis (CFA) including factor loadings (λ), squared multiple correlations (R2), fit indices for the measurement model,
a
and reliability coefficients (α, ρc). fit indices for the measurement model: χ2 = 38.98, p = 0.0067, χ2/df = 1.95, RMSEA = 0.11, 90% confidence interval RMSEA = 0.054–0.15, NFFI = 0.95, CFI = 0.97, SRMR = 0.069. Listwise N = 178.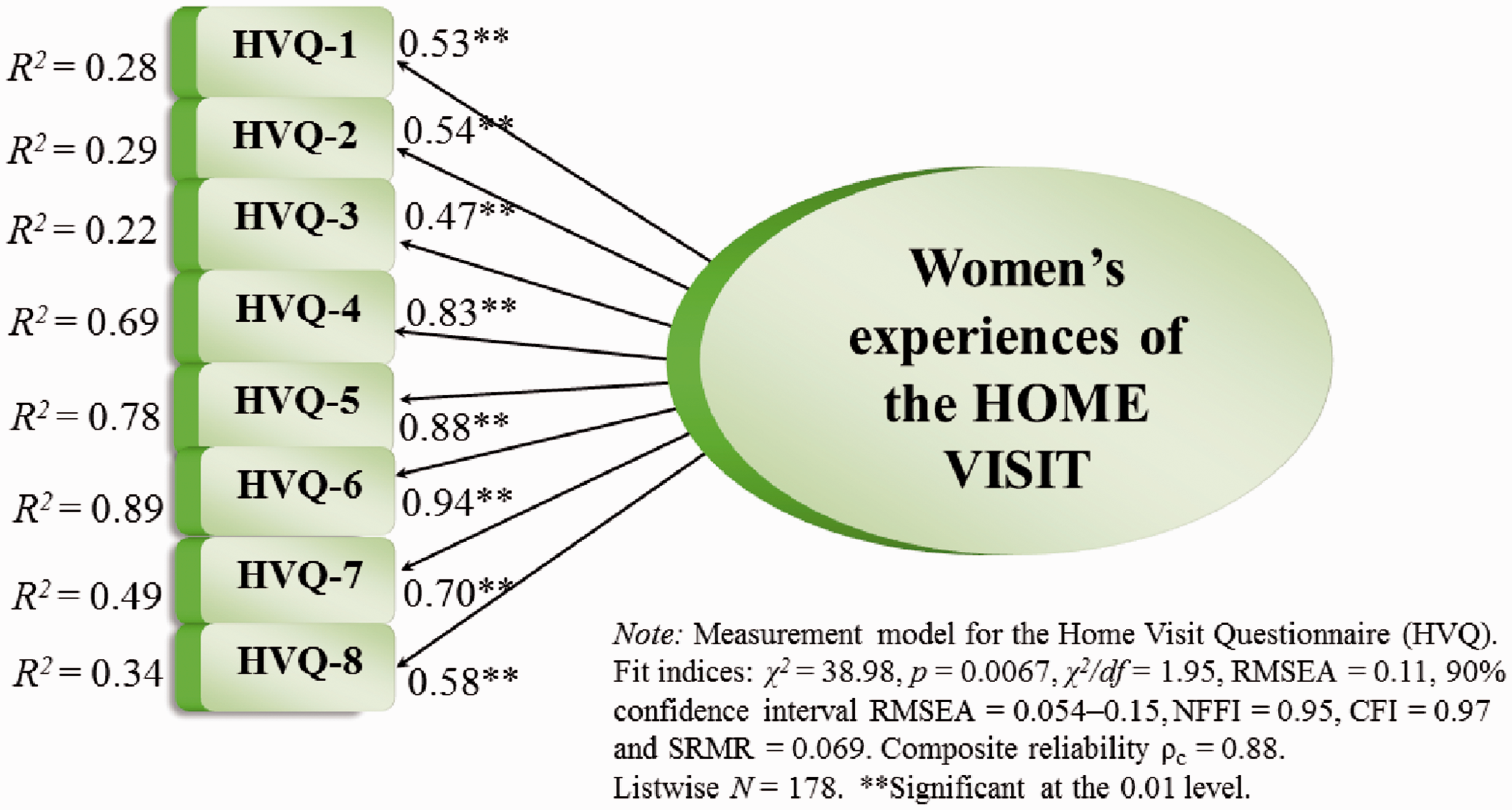
The intervention group: Positive influences of the home visit
Intervention group: perceived influence of the home visit (HVQ) and experience of support (SA1) among the primiparous women compared to the multiparous women.
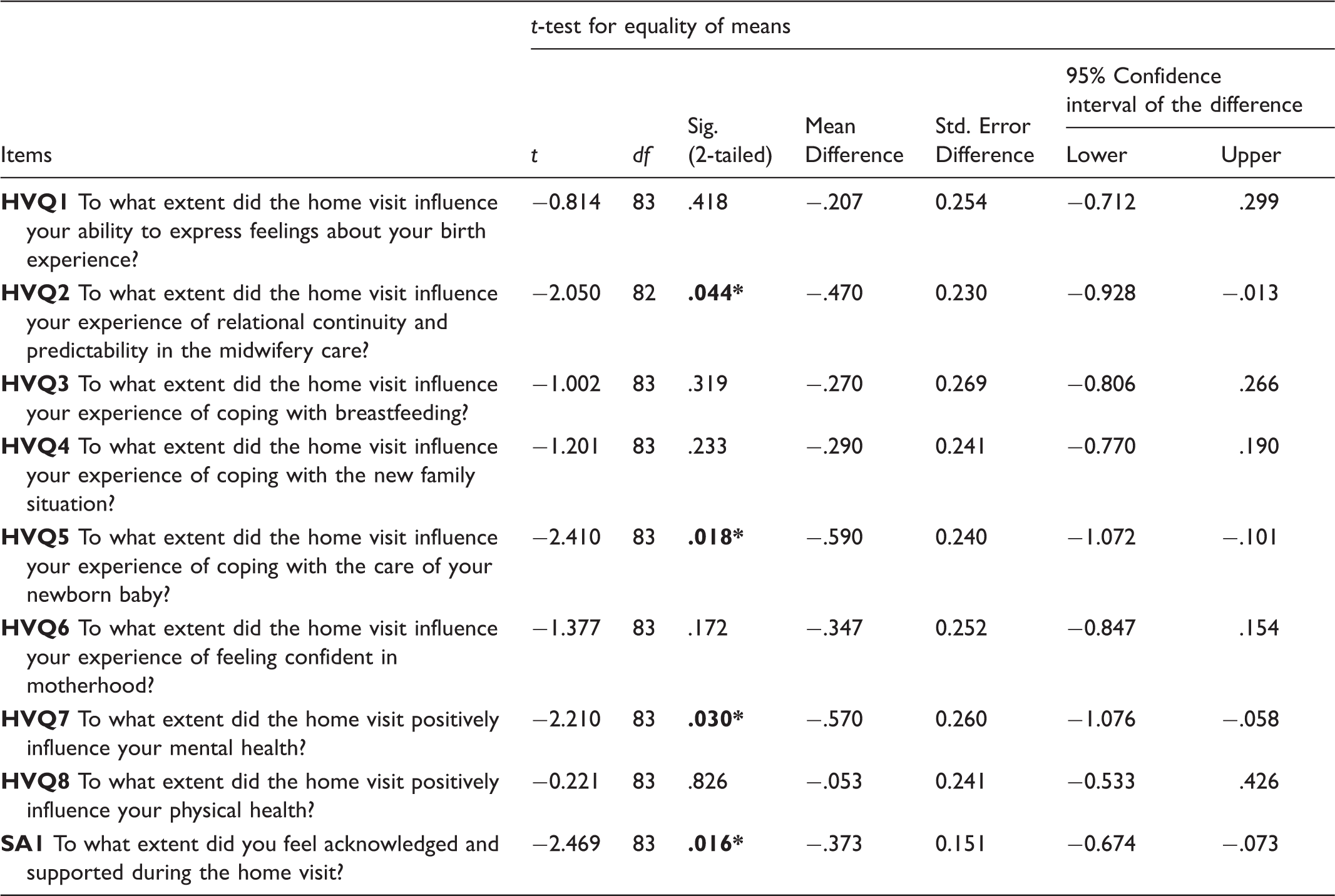
Note: Intervention group: primiparous women (listwise N = 59) and multiparous women (listwise N = 25). SA1 represents the one-item assessment of support. *significant at the 0.05 level.
Discussion
This study assessed the length of stay in hospital after birth among multiparous and primiparous women, as well as the possible health-promoting influences of a postnatal home visit by a midwife shortly after birth. Four hypotheses were tested (H1–H4), all of which were supported by the empirical data in this study. The present findings showed that the multiparous women left hospital earlier than the primiparous women (H1). As the multiparous women have one child or more at home, their motivation for an early discharge from hospital might be high. Moreover, among the multi-parous women the transition to becoming a mother is part of their previous experience. First-time mothers often experience insecurity and anxiety in understanding and handling the baby the first days after birth. They often need professional support for breastfeeding and baby care. 2
The second hypothesis (H2) explored the differences between the multiparous and the primiparous women who had all received a home visit shortly after birth. The study shows that in cases where the primiparous women were offered a home visit, they left hospital within 48 hours after giving birth. The fact that the women in the intervention group were aware that they would receive a home visit from a midwife shortly after arriving back home might explain this finding. Possibly, this assurance made the primiparous women feel more confident about leaving hospital early. Even though many women experience the first period after birth as overwhelming, they tend to consider early discharge from the maternity ward as safe when they know they can expect a home visit by the midwife within a few days. 27 The women want to be able to influence the timing of their discharge from hospital, regardless of whether this is early or after a few extra days. 28 In line with the National guidelines for postnatal care, 14 the time spent in hospital should be adjusted according to the individual needs of the woman and the newborn baby. An early discharge should be conditioned by properly organized services at the home place and available support from the woman's partner and social network. McLachlan et al. 29 highlight a need for greater flexibility in facilitating early postnatal discharge, as a fixed length of stay may undermine the requirements of individualized care. In a similar vein, Fenwick and colleagues 19 stress that attempts to reduce the length of the postnatal stay without providing community support is inappropriate, outdated and unsustainable. They emphasize that implementation of new models of care that value relational interaction between the woman and the midwife as well as the right approach is important.
The primiparous women in the intervention group experienced that the home visit significantly influenced their mental health, and their feeling of being supported (H4). This is notable, given that support is found to help prevent postpartum depression. 30 The mothers want midwives to provide more care and support, 31 though it is a challenge for the midwives in the specialist healthcare services to satisfy both the physical and emotional needs due to the short period of postnatal care in hospitals and the limited resources of the midwife profession. 32 Studies show that women perceive the quality of the midwifery care during the early postpartum period to be better at home than in hospital. This is due to the hospital environment where the midwives are busy and difficult to contact. As a result, the midwives do not give priority to the emotional aspects of care and the women often perceive the advice they receive as inconsistent.16,19 The women in a study by Dahlberg and co-workers 28 claimed that the midwife tended to focus on the emotional aspect of becoming parents during the home visit. According to them, the midwives did not exclusively devote themselves to the needs of the baby, but also seemed interested in the wellbeing of the woman and her partner. Women may need professional support to take care of themselves in the first week of the postnatal period.2,18 Barimani and colleagues 31 found that mothers want more attention paid to their own needs and that physical and emotional support is strongly appreciated. Razurel et al. 33 emphasize that emotional and social support is more essential than practical knowledge in the early postnatal period. Whether the women encounter challenges or experience the postnatal period as completely normal seems to have an insignificant effect on the need for support and recognition from the midwife. When the midwife is able to support the women in their decisions and understanding of the situation, it seems to promote a feeling of safety, confidence and coping.
The primiparous women in the intervention group also experienced the home visit by the midwife to significantly influence their ability to care for the newborn baby (H4). This finding indicates a health-promoting influence of the home visit on primiparous women, as coping with early parenting enhances empowerment. 11 Individualized available support focused on developing and recognizing the parent's experiences of taking care of their baby increases their sense of parental confidence.3,7,34,35 The physical presence and availability of professional support help to alleviate concerns about the safety and wellbeing of the newborn baby, especially for first-time mothers. 36 Guidance in relation to breastfeeding is important, in particular when the breastfeeding is in an early stage. This guidance along with advice about how to fulfill the baby's needs may contribute to a sense of coping. 2 Furthermore, unfulfilled needs tend to increase the use of medical services. 37 When the women feel safe about the conditions affecting the baby, they might become more aware about themselves and their own basic needs, like eating, sleeping and treating sore breasts. 2
In the present study, the women who received a home visit by a midwife reported higher scores on predictability and continuity in the midwifery care (H3) than the control group (Table 4). The primiparous women in the intervention group experienced the home visit to have a strong influence on the perceived relational continuity of their maternity care (H4). This is supported by Dahlberg and colleagues 28 and Aaserud and co-workers 35 who found that women who were visited by a midwife they had met before experienced the visit as more significant, especially with regard to the emotional aspect and the processing of the birth experience. Continuity in the relationship increases the woman's confidence in the midwife's expertise, advice and guidance. At the same time, the midwife helps her to believe in her own resources. 11 Studies reveal that relational continuity of midwifery care often helps the woman and her partner to gain attention and be respected. This type of care is based on a health-promoting approach and is associated with a positive birth experience.11,38 In our study, we found that the primiparous women in the intervention group who received relational continuity in the midwifery care, experienced that the home visit significantly influenced their feeling of being acknowledged and supported as well as influenced their ability to care for the newborn baby (Table 6).
In Norway, maternity care is fragmented, marked by a number of staff members interacting with vulnerable women. 39 Conflicting opinions, information and practices may result in negative perceptions about the care.40,41 Relational continuity of care can improve both the effectiveness of healthcare and its efficiency, with fewer staff handovers and more consistency in the care provided. It may further reduce the demand for additional services and the number of hospital admissions, while increasing patient satisfaction.42,43 Relational continuity of care responds to the women's need to have a relationship with one person or team, and receive consistent information.40,41 This model of care is seen as a vital condition for offering high-quality healthcare.11,19,31,38,44,45 The National guidelines for postnatal care 14 recommend a home visit by a midwife within the first couple of days after discharge from the hospital. Both the midwife and the public health nurse have a health-promoting approach, but still the focus is different. Midwives have expertise in women's health, pregnancy, childbirth and the postpartum period. 46 At the home visit, she is focused on the woman and her baby's health and wellbeing. The midwife may also contribute to boost the confidence of the woman in her new situation, helping her to develop skills as a mother. On the other hand, the expertise of public health nurses is focused on children, adolescents and families, 47 with an emphasis on the baby's health and development. Public health nurses may contribute to positive bonding and good family relationships. Stronger interdisciplinary collaboration and familiarity with different areas of competence will lead to a more efficient use of resources and skills and ensure that follow-up programs during the early postnatal period to a greater extent respond to the unique needs of each woman, baby and family. 48 The childbearing period is open to salutogenic interventions with an emphasis on health-promoting strategies, such as mobilization of the resources required to prepare for the changes following birth. Midwifery should have a stronger focus on the fact that individual needs and the coping experience of the woman are important when empowering a new family.11,16,27,49
Limitations
The small sample size of the intervention group (N = 85) and the control group (N = 98) represent a limitation of this study. The same applies to the high number of primiparous women in the intervention group (n = 59) compared to those in the control group (n = 42) (Table 3). An equal distribution of primiparous women in the two groups could have exposed significant differences between the groups. With regard to sample size, the power calculation revealed a desired sample size of N = 71 for the two groups. Subsequently, the sample size in this study should be sufficient. However, a larger sample would significantly increase the statistical accuracy of the tests. Moreover, the HVQ developed for this study has not been used and validated previously. Regarding the RCS, item 8 was excluded due to some misspecification. Item RCS8 includes to what extent the participants felt prepared to be a parent. However, item RCS6 includes confidence in motherhood, which is a wording very close to item RCS8.
Conclusions
No significant differences between the intervention group and control group regarding the length of the postnatal stay in hospital were discovered. Still, there was a significant difference between the primiparous and the multiparous women in the total sample, insofar as the primiparous women in the intervention group left hospital earlier than the primiparous women in the control group. The women who received a home visit by a midwife reported higher scores on predictability and continuity in the midwifery care than the control group. Furthermore, the primiparous women experienced a significant influence of the home visit on their ability to cope with the care for the newborn baby, as well as on their mental health and feeling of being acknowledged and supported. They also reported a perceived relational continuity of midwifery care. Accordingly, a postnatal home visit could have a health-promoting influence on both mental health and the ability to cope, resulting in a shorter postnatal stay in hospital to the benefit of the woman, the newborn baby and society. A model of midwifery relational continuity of care, including a postnatal home visit shortly after birth, should be further developed and studied with the help of larger samples.
Footnotes
Acknowledgements
The authors would like to thank the women who participated in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.