
Abstract
The aim of this study was to provide a description and evaluation of birth outcomes for women who started care at Føderiket Midwifery Unit (FMU), a freestanding midwifery unit in Oslo. FMU opened in 2007 as a five-year project. It was closed in 2011 for economic reasons, and the planned evaluations were never performed. Data from 495 women who started care at FMU were prospectively collected. Socio-demographic characteristics, transfers to hospital, maternal and neonatal outcomes were described. The findings showed that 115 (23%) of the women were primiparous and 380 (77%) multiparous. A total of 408 women (82%) had no complications and no need for additional medical treatment during labour and birth. There were 73 (15%) transfers before birth, and 14 (3%) after birth. Nine women (2%) were delivered by caesarean section and 19 (4%) by vacuum extraction. Thirty women (6%) had postpartum haemorrhage >500 ml and five (1%) received blood transfusions. Five babies (1%) were transferred to the Neonatal Intensive Care Unit, all were discharged to their homes within a week. There were no cases of deaths, or serious morbidity. Our conclusions are that the results after four years management were comparable to other freestanding midwifery-led units in Western countries.
Introduction
In Western countries, the majority of women give birth in obstetric units in hospitals. In many countries, low-risk women can choose alternative birth settings, like midwifery units and home births. Midwifery units are locations offering maternity care to women with straightforward pregnancies and low risk for intra-partum complications. Midwives have the professional responsibility for care, and women are transferred to hospital in case of complications or need for medical pain relief. There are two categories of midwifery unit: alongside midwifery units, which are situated inside a hospital and within the same buildings as an obstetric unit; and freestanding midwifery units with a geographical distance to the nearest obstetric unit.
A Cochrane review comparing alongside midwifery units with obstetric units found no difference in neonatal outcomes and a lower rate of medical interventions. 1 However, the results cannot be generalized to freestanding midwifery units, and there is concern about the safety of births in settings away from an obstetric unit, especially in case of transfers during labour and after the birth.
A recent guideline and systematic review from Great Britain compared outcomes from midwifery-led units and home births with obstetric units, and concluded that low-risk women should be advised to give birth outside an obstetric unit. There were higher rates of spontaneous vaginal deliveries and no difference in neonatal outcomes when low-risk women planned to give birth in a midwifery-led unit or at home. 2
A big cohort study from England compared outcomes in 11,282 low-risk women selected to give birth at freestanding midwifery units with 19,706 low-risk women who gave birth in obstetric units. 3 They found no difference in neonatal outcomes, and reduced risk of interventions like caesarean and assisted vaginal deliveries, oxytocin augmentation, episiotomy, epidural analgesia, blood transfusions and obstetric anal sphincter injuries. Transfer rates to hospital were 35.3% in primiparous and 9.4% in multiparous women.
Recent studies from Denmark, Australia and New Zealand4–6 have also reported lower rates of medical interventions and complications in low-risk women planning to give birth in freestanding midwifery units compared to obstetric units. Two of the studies5,6 found that there were fewer transfers of babies to a Neonatal Intensive Care Unit if the birth was planned in a freestanding midwifery unit.
A Norwegian study evaluated all births at freestanding midwifery units during the period 1995–1997. 7 In total, 1275 women started care in the midwifery units, 58 (4.5%) were transferred to hospital during labour and before the birth of the baby and 57 (4.5%) were transferred after the delivery for maternal or neonatal indications. Of the women selected to give birth at the midwifery units, 10 had caesarean deliveries (0.8 %) and eight women had assisted vaginal deliveries (0.6%). There were two cases of neonatal deaths and no cases of maternal deaths. The authors concluded that it was safe to give birth at the freestanding midwifery units given that strict selection criteria were followed.
The Norwegian parliament decided in 2001 that maternity care should be decentralized and differentiated, that women should be able to choose between different levels of care, and that care should be individualized. 8
On 21 May 2007, Føderiket Midwifery Unit (FMU), a freestanding midwifery unit, was opened in the centre of Oslo. The unit was organized as a part of Oslo University Hospital, Rikshospitalet, and was situated six kilometres away from the obstetric unit. It was initiated as a five-year project and was to be evaluated at the end of the project period. After four years, on 27 June 2011, FMU was closed for economic and strategic reasons, and the planned evaluation was never performed.
Norway has a population of five million, and there are approximately 60,000 births annually. There are 46 birthing institutions, 39 in hospitals and seven freestanding midwifery units. The caesarean section rate is 17.0%, and 10.0% of all deliveries are by vacuum extraction or forceps. 9 The seven freestanding midwifery-led units are in rural areas, situated between 70 and 230 kilometres away from the nearest hospital, mostly in the northern and interior parts of Norway. During the period 2007–2011, there were 4068 deliveries in freestanding units; that is 1.3% of all births. 9 One-third of all births were in hospitals with more than 3000 deliveries annually, 30% in hospitals with 1500–2999 deliveries, 25% in hospitals with 500–1499 deliveries and 10% in hospitals with fewer than 500 deliveries annually. 9 There are also five alongside midwifery-led units, all in large hospitals in the southern and western parts of the country. The number of births in alongside units is not separately registered, but in 2011 the five alongside units had 3378 deliveries, which is 5.6% of all deliveries (personal communications after telephone calls to the units).
The aim of the present study was to provide a description and an evaluation of birth outcomes for women who started labour at FMU. The results will be useful as they evaluate different models of maternity care in Scandinavia.
Methods
Study design
This was a prospective cohort study using data from all women who had planned to give birth at FMU, and were low-risk at the onset of labour. FMU existed from May 2007 to June 2011.
Background information to the present study
Pregnant women applied to give birth at FMU. To be accepted for birth, the women had to fulfil the selection criteria which were: non-smokers, body mass index (BMI) < 30, no chronic medical diseases before pregnancy, no complications in pregnancy, a single foetus in a vertex presentation, with spontaneous onset of labour at term (defined as from 21 days before to 10–11 days after term date), not more than five previous deliveries, and women with a previous caesarean delivery had to have had a subsequent uncomplicated vaginal delivery to be accepted. In cases of previous assisted vaginal deliveries, and if there were any doubts whether the inclusion criteria were fulfilled, individual assessments were done by a consultant obstetrician. FMU was primarily meant for multiparous women, but primiparous women were also accepted.
The women were offered acupuncture, immersion in water and other forms of drugless pain relief. In cases of slow progress of labour, amniotomy could be performed. If any signs of complications occurred, needs for assessment by a consultant, for continuous foetal surveillance, oxytocin augmentation or operative delivery, the woman was transferred to the obstetric ward at Oslo University Hospital, Rikshospitalet. Transportation time was 7–10 minutes by ambulance or private car. FMU was equipped with a portable vacuum extractor, drugs and other equipment to manage situations such as asphyxia in the baby, maternal postpartum haemorrhage and other emergencies. All midwives participated in regular training in emergency delivery procedures. There were regular audits regarding transfers and other events as part of an ongoing learning and safety process.
FMU was staffed by eight midwives (6.5 full-time equivalents) who provided antenatal care, birth preparation classes, intra-partum care and postnatal care. Each woman was offered eight antenatal check-ups. There was an ongoing selection process during pregnancy, and it was considered important to prepare the women for pregnancy, giving birth and breastfeeding. During labour, one midwife was continuously present with the woman and during delivery another midwife should be present in the unit to assist if needed. The women were supposed to stay in the unit for 6–24 hours after the birth. On the third or fourth day after the birth, the child was offered a paediatric check-up and neonatal screening for hearing and phenylketonuria.
Data collection
Data were prospectively collected from the antenatal journal and the hospital’s electronic patient files by one of the authors (ASH). FMU opened on 21 May 2007 and closed on 27 June 2011, and all women were registered in the study. The following variables were collected:
Maternal: Age, marital status, level of education, parity, BMI, birthing position (upright position or not), waterbirth, caesarean section, assisted vaginal delivery (vacuum or forceps), oxytocin augmentation, epidural analgesia, perineal tears, postpartum haemorrhage and transfers to hospital during labour or within 72 hours after the birth for maternal indications. Neonatal: Apgar scores at five minutes, whether the baby was resuscitated, transfers or admittance to hospital within 72 hours after birth for neonatal indications, perinatal deaths (stillborn or infant death during the first 7 days of life) and neonatal death (death of a live-born infant during the first 28 days of life). It was also noted if the transfers were urgent, defined as if the mother or infant needed medical assistance as soon as possible.
Data analyses
Data were entered and analysed using SPSS, version 17.0. Descriptive analyses, like frequency tables, proportions and averages, were performed.
The study was evaluated and approved by the Oslo University Hospital’s Data Protection Official for Research (case no. 093978). The study was assessed as part of a quality control exercise, and approval from the Regional Committee for Medical Ethics was not necessary.
Findings
In total, 808 women applied to give birth at FMU and 495 started labour at the unit. After the first antenatal visit, it became clear that 102 women did not meet the inclusion criteria. Of the remaining 706 women, 211 were selected to hospital care because of miscarriage, twin pregnancy, premature delivery, foetal growth retardation, pregnancy-induced hypertensive disorders, post-mature delivery, other complications or because the woman changed her mind (Figure 1).
Overview of all women who booked a place at Føderiket Midwifery Unit.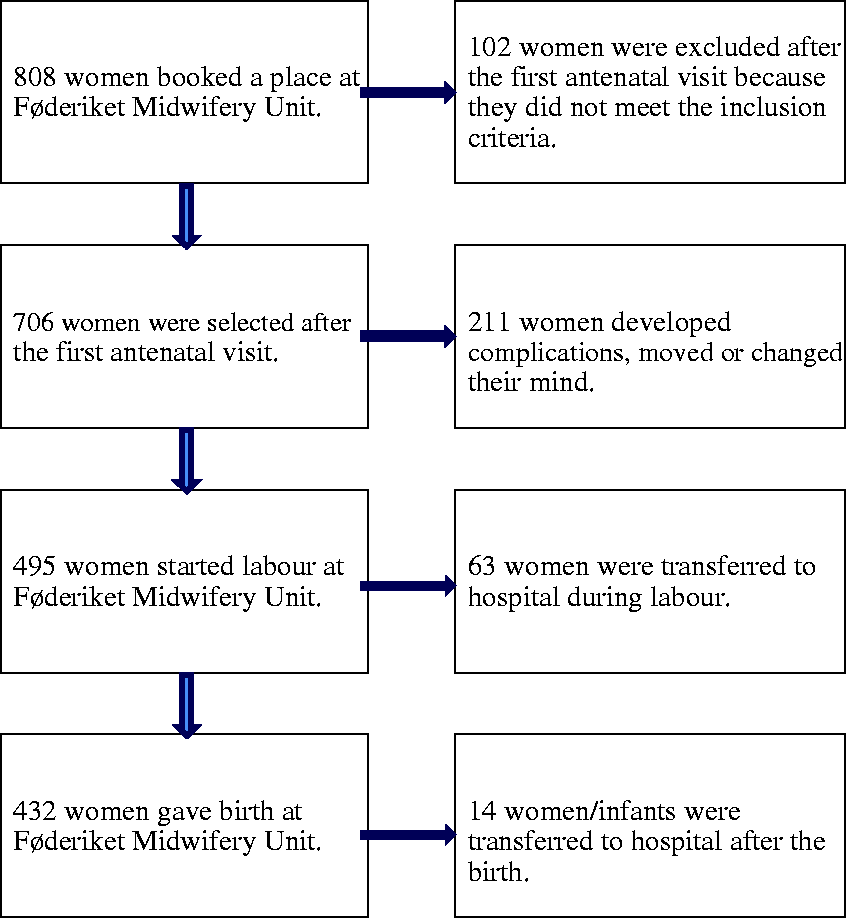
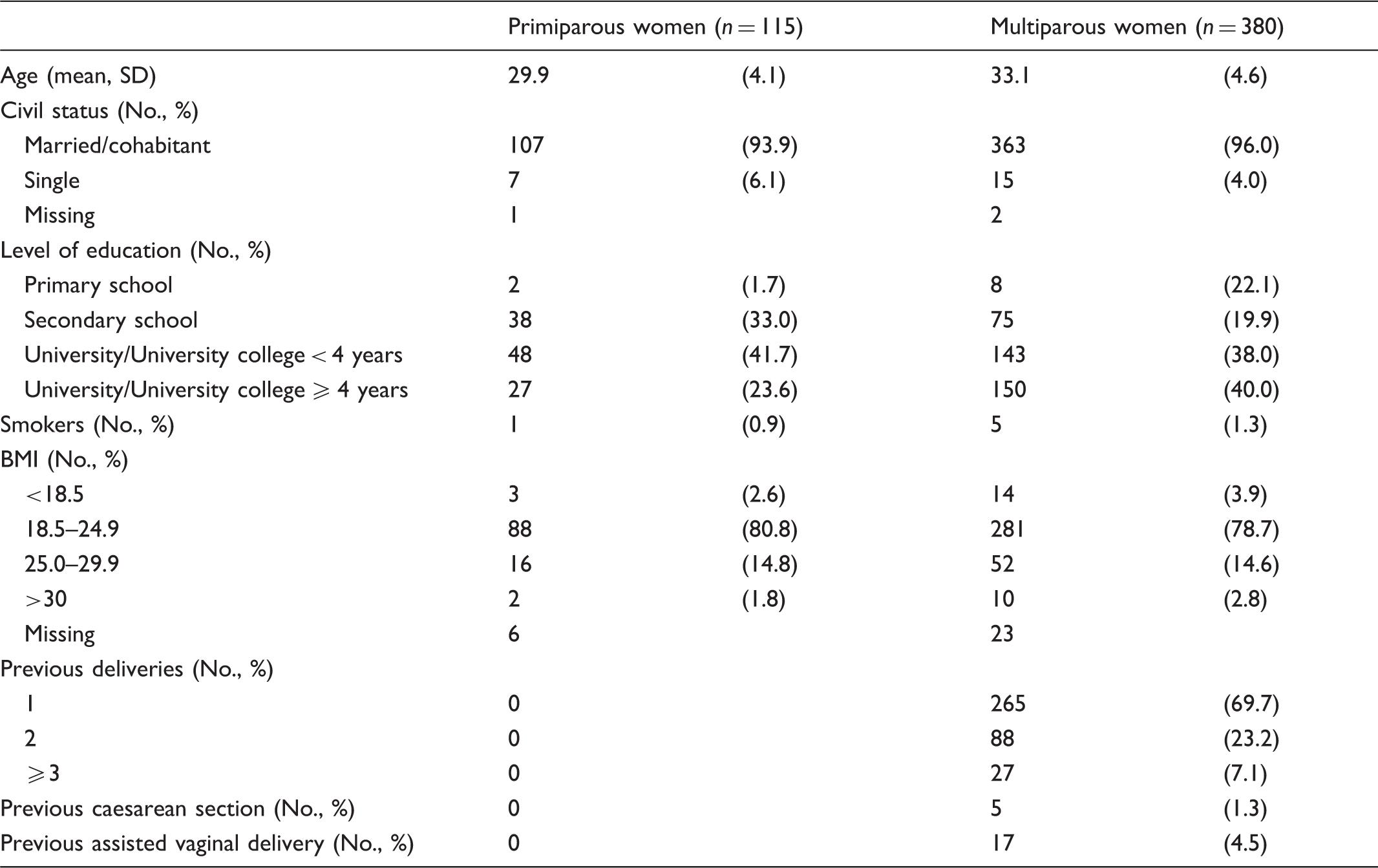
Socio-demographic characteristics of 495 women who started labour at Føderiket Midwifery Unit.
Maternal and neonatal outcomes in 495 women who started labour at Føderiket Midwifery Unit (FMU).
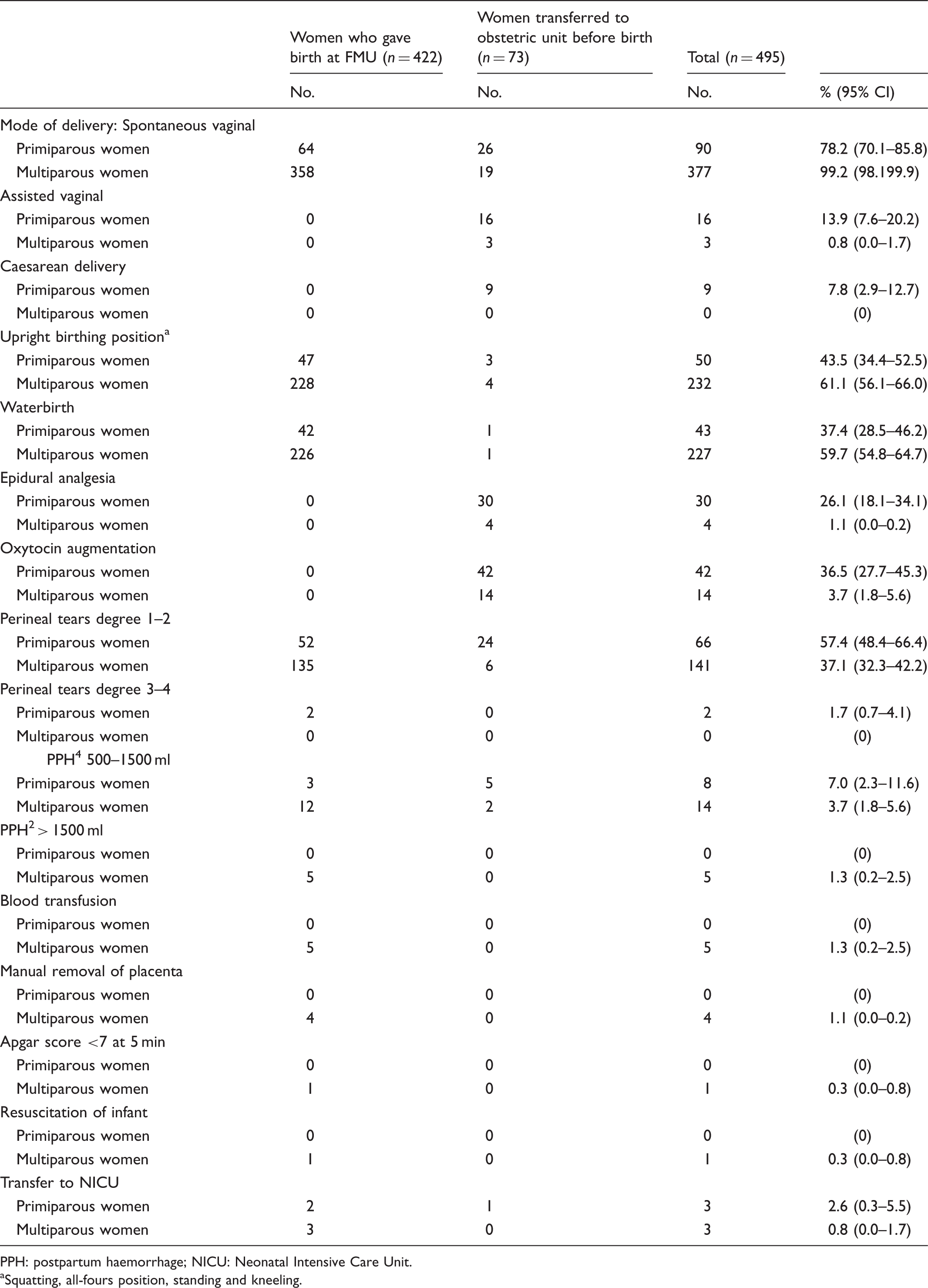
PPH: postpartum haemorrhage; NICU: Neonatal Intensive Care Unit.
Squatting, all-fours position, standing and kneeling.
Reasons for transfers during labour and after birth, and if it was an urgent transfer.
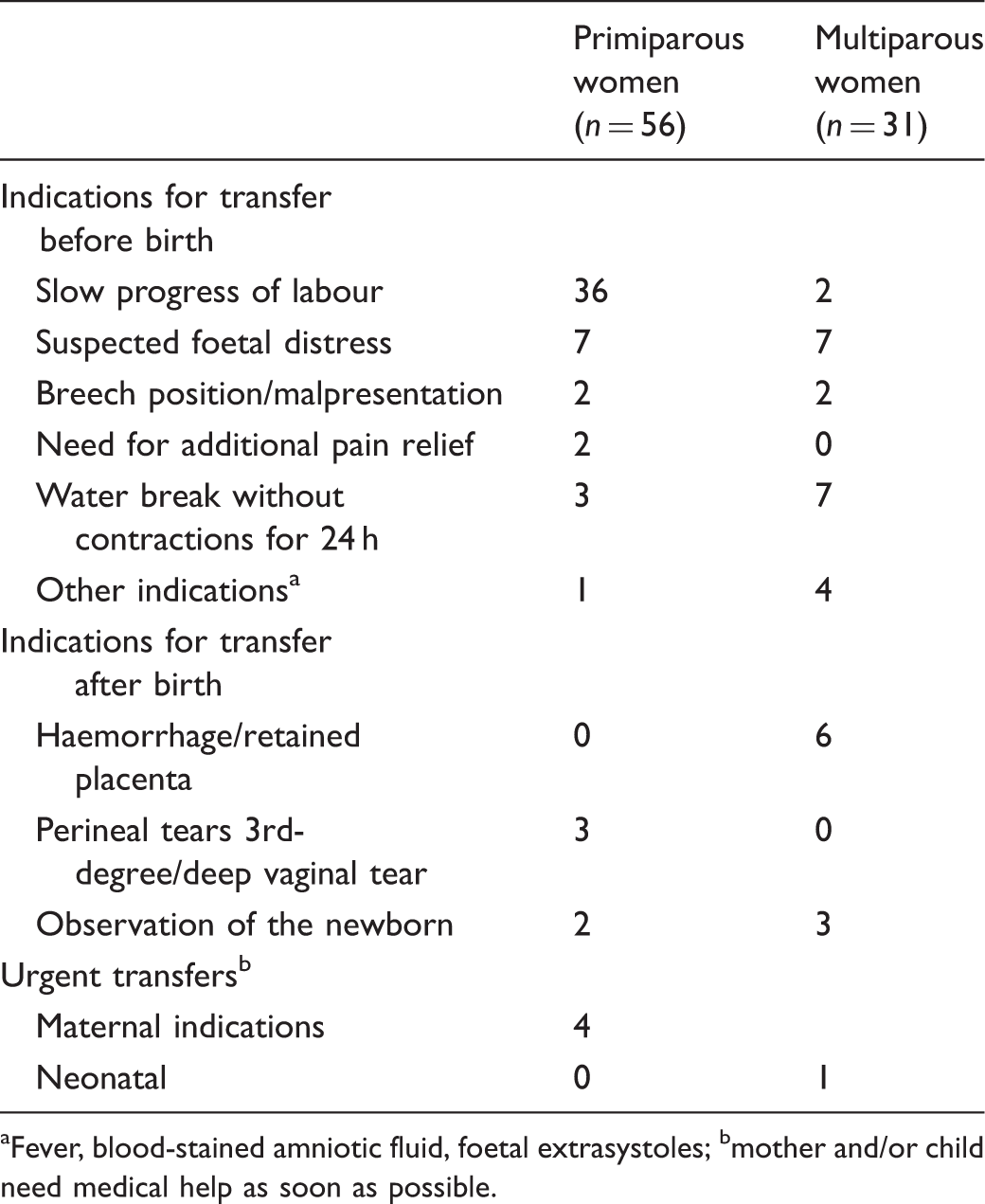
Fever, blood-stained amniotic fluid, foetal extrasystoles; bmother and/or child need medical help as soon as possible.
Ten of the transfers were classified as urgent transfers, indicating that the mother or the infant needed immediate medical assistance. The indications for urgent transfer were: undetected breech presentation in late labour (two cases), suspected foetal distress (three cases), retained placenta (three cases), postpartum haemorrhage (one case) and low Apgar score (one case). The time from when the transfer decision was made until the transfer was completed was registered in seven of the ten cases: five were transferred within 20 minutes, one within 30 minutes and one within 50 minutes. The two women with babies in breech presentation were delivered by caesarean section and no complications were reported. The three cases of suspected foetal distress ended with uncomplicated vaginal deliveries. Of the four women with either retained placenta or postpartum haemorrhage, all four had blood transfusions (two to six units), three had manual removal of the placenta and one had a revision of the uterine cavity. One infant had an Apgar score of 5 at 5 minutes, was admitted to the Neonatal Intensive Care Unit and stayed there for one week. The infant was treated with antibiotics for a suspected infection.
Discussion
Of 495 women who started labour at FMU, 408 (82%) gave birth without complications, medical treatment or need for transfer to an obstetric unit. There were more transfers to hospital and medical interventions in primiparous than in multiparous women: 21.7% of the primiparous and 0.8% of the multiparous women had operative deliveries.
In the present study, 48.7% of all primiparous and 8.2% of all multiparous women were transferred to hospital during labour or after birth. A Norwegian study, 7 evaluating outcomes from all women who started labour at all freestanding midwifery-led units during 1995–1997, found that 2.2% ended with an operative delivery and 9.0% were transferred to hospital during labour or after birth. Analyses were not stratified for parity, which makes comparison difficult. The time span between the studies is more than 10 years, and it is possible that selection criteria and practice have changed.
The Birthplace in England prospective cohort reported outcomes in women who started care in 53 freestanding midwifery units. The transfer rate was 36.3% in primiparous and 9.4% in multiparous women. 3 A Danish study reported that 36.7% of all primiparous and 7.2% of all multiparous women experienced an intra-partum transfer from freestanding midwifery unit to obstetric unit. 4
In our study, 7.8% of the primiparous women had a caesarean delivery and 13.9% an assisted vaginal delivery. The rates in multiparous women were 0% and 0.8% respectively. The Birthplace in England study reported similar rates, 6.7% and 10.7% in primiparous and 0.7% and 1.1% in multiparous women respectively. 3 We were not able to find other recent studies who reported analyses of operative deliveries in freestanding midwifery units stratified for parity.
Robson group 1 is often used as a proxy for low-risk primiparous women and Robson group 3 for multiparous low-risk women. 10 According to the Medical Birth Registry of Norway, women classified as Robson group 1 in 2007–2011 had a caesarean section rate of 8.2% and assisted vaginal delivery rate of 18.3%. The rates in Robson group 3 women were 2.8 and 1.8% respectively. 9 Rates of medical intervention in labour were lower in our study than in all low-risk women registered in the Medical Birth Registry during the same period. Our study design does not allow us to draw conclusions about whether FMU facilitated a reduction in medical interventions during childbirth. However, there is a growing body of evidence which suggests that care for low-risk women in freestanding midwifery units reduces medical interventions without compromising neonatal outcomes.2–6
Our study has strengths and limitations. The study was prospective, and all available women were included and followed up. The main limitation of the study is the observational and descriptive design, and we cannot draw conclusions about the effect of giving birth in a freestanding midwifery unit. Furthermore, outcomes like Apgar scores and postpartum haemorrhage may be influenced by measurement subjectivity.
Conclusions
FMU was established to effectuate and evaluate differentiated birth care in the capital city in Norway, which was the wish of the Norwegian authorities. The results after four years were comparable with results from freestanding midwifery units in other Western countries.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.