
Abstract
The World Health Organization recommends that all countries with a well-developed midwifery service offer a midwifery-based practice formed on relational continuity of care. Pregnant women in Norway have stated that they experience the service throughout the childbearing process as fragmented. The present study aimed to gain knowledge about how midwives working in the primary healthcare service experience relational continuity of midwifery care and what challenges they encounter. In-depth interviews were conducted with 10 midwives working in different public health clinics in Norway. The qualitative data were carefully analysed using systematic text condensation. The COREQ checklist was applied. The participants indicated the importance of providing individualised midwifery care by meeting the women early in pregnancy and establishing a mutual relationship built on trust and safety. This helped ease the midwife’s work. The midwives expressed a desire for continuity in the follow-up of the women, but this was not always possible due to a lack of capacity. This study shows that relational continuity of midwifery care is important to midwives working in the primary healthcare service. The midwives wanted a midwifery-led practice that would allow them to lead their profession and use their full expertise. To achieve relational continuity in the primary healthcare service, the informants declared the importance of management seeing the midwives’ potential.
Introduction
In Norway, antenatal care for healthy pregnant women is part of the primary healthcare services, whilst the special health services have the main responsibility for intrapartum and postnatal care. Antenatal care is a voluntary offer, where the pregnant woman chooses whether she wants follow-up care from a midwife, general practitioner (GP), or a combination of both during the antenatal period. In recent guidelines, midwives in the primary healthcare service have been given additional tasks such as home visits in the early postnatal period along with contraception guidance.1–3 Midwives and public health nurses work together, and they are expected to collaborate in providing postnatal care. In the early postnatal period, the midwives ensure continuity of care and a smooth transition to the public health nurse’s further follow-up. In an international context, midwifery care in Norway is of high quality. However, maternity care could be improved to provide systematic and comprehensive care to women and their families. 4
The World Health Organization (WHO) recommends that all countries with a well-developed midwifery service offer a midwifery-based practice formed on relational continuity of care.
5
A midwife-led practice in the primary healthcare service in Norway means that the same midwife independently plans, organises, and offers a follow-up to healthy women throughout pregnancy and conducts home visits during the early postnatal period. This ensures that care is individually tailored to the woman and her family.
6
Relational continuity is defined by Haggerty and colleagues as ‘an on-going therapeutic relationship between a patient and one or more providers’.
7
These authors define continuity as … the degree to which a series of discrete healthcare events is experienced as coherent and connected and consistent with the patient’s medical needs and personal context. Continuity of care is distinguished from other attributes of care by two core elements: care over time and the focus on individual patients.
Continuity of midwifery care gives midwives and women a mutual opportunity to develop meaningful relationships 8 and can contribute to a sense of coherence and predictability. 7 Research shows that women want relational continuity of care during the childbearing process,9–12 and it may give a more positive experience of the care given.13,14 Women who receive midwifery-led care are more likely to be supported at birth by a midwife they know, 6 to experience a normal vaginal birth6,15 and to be more content with their care 6 than women who receive other models of care. They are also less likely to experience interventions, such as regional analgesia, amniotomy, and episiotomy. 6 This model of care contributes to an increased number of homebirths and higher breastfeeding rates 15 and women report that midwives keep them informed, that they are involved in decision-making, that their concerns are taken seriously and that they are more satisfied with the support provided by midwives. 12 When multiple healthcare providers are involved, different practices, advice, and opinions may result in a negative experience.9,10 Women may be critical towards the organisation of care since there are several care providers to relate to who do not necessarily collaborate. 16 Relational continuity of midwifery care is based on a health-promoting approach, is associated with a positive birth experience,17,18 and is considered a condition for high-quality maternity care.19–22
Relational continuity in a midwifery-led practice is a cost-effective 23 and safe model that should be offered to all pregnant women. 15 Midwives are recognised as responsible, professional practitioners and are dedicated to the independent follow-up of women in the childbearing process. Midwives play a central role in health promotion and preventive work at public health clinics.24,25 Pregnant women in Norway have stated that they experience the service throughout the childbearing process as fragmented, segmented, and centralised. 4 Research shows that relational continuity of midwifery care is a positive features of midwives’ working lives 26 and there is evidence that this model of care improves midwives’ job satisfaction.27–30 Norwegian midwives experience their role as autonomous and find that the support from their management affects their practice. 31 Knowledge about midwives’ experiences of caring for women through pregnancy and the early postnatal period is lacking. This knowledge gap motivated the researchers to conduct the current study.
The present study aimed to gain knowledge about how midwives working in the primary healthcare service experience relational continuity of midwifery care and what challenges they encounter.
Method and design
The researchers followed a qualitative approach and in-depth interviews were conducted. Interviews are useful for ascertaining participants’ experiences by discovering diversity and nuances. In this way, relational continuity was explored as experienced by midwives. 32
Setting and participants
A total of 10 midwives from different public health clinics and counties in Norway were recruited and included in the study. Public health clinics offering home visits after birth were chosen randomly and they had a geographical distribution from Southern to Central Norway. To be included, midwives had to have worked at a public health clinic for at least two years and offer home visits after birth. The number of years of experience in a public health clinic ranged from 2.5 to 22 years. All midwives offered home visits, but to varying degrees. At some of the public health clinics, home visits were offered only to first-time mothers and families at risk, while other clinics offered home visits to all women after childbirth.
Data collection
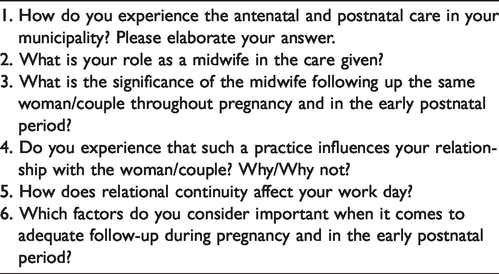
The midwives were interviewed individually at their workplace or the university, depending on the informants’ wishes. Each interview lasted approximately 30–65 minutes. During eight of the interviews, two researchers were present. The remaining two interviews were shared between the researchers due to geographical challenges and capacity. An interview guide (Table 1) containing six questions was developed based on published methodology. 32 A pilot interview was conducted, and the questions were tested and revised. Follow-up questions were asked to clarify opinions and statements. 32 Data collection continued until new data failed to add new information to the study. All midwives were encouraged to express themselves freely and after 10 interviews, data saturation was reached. The participants provided detailed statements of their experiences with relational continuity of midwifery care and what challenges they encounter.
Interview guide.
Data analysis
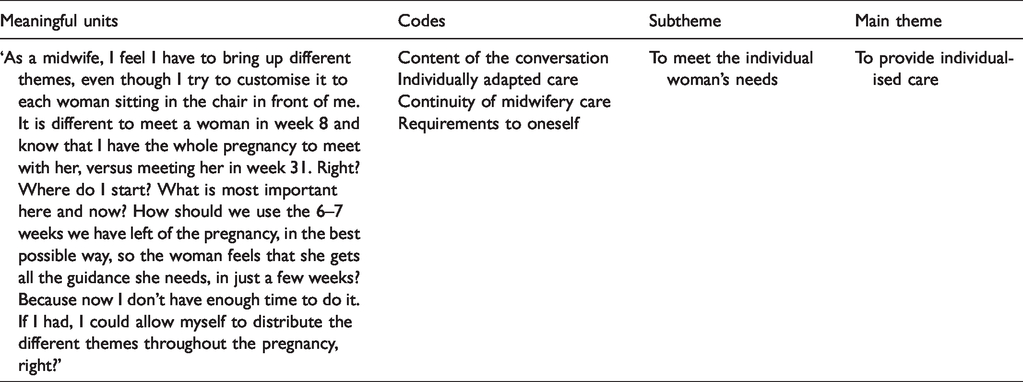
The interviews were tape-recorded and transcribed word for word. The qualitative data were carefully analysed using systematic text condensation (STC), which is a descriptive and explorative analysis method. 32 Developed by Malterud, 33 STC is a modified version of Giorgi’s 34 phenomenological analysis. The main purpose of the phenomenological approach is to gain knowledge from individuals’ experiences and feelings and to produce in-depth descriptions of the phenomenon. The researchers are searching for the essential topics that appear from the empirical data, with the researcher’s presumptive knowledge put aside. The systematic text condensation consists of four steps. 32 In the first step, the interviews were read to get an overall impression, and then preliminary themes reflecting the participants’ experiences were found. In step two, meaningful text units that represented different aspects of the midwives’ experiences were identified and coded by systematically reviewing the transcribed data material line by line. In step three of the analysis, the sorted data established from the second step were condensed, abstracted, and summarised. In the final step, the reflections, thoughts, and experiences that were shared by the midwives were redefined into re-contextualised versions, providing the basis for new descriptions and concepts. 32 To ensure validity, the analysed data were assessed in relation to the initial transcriptions. All three authors contributed substantially to the analysis of data. An example of the analysis process is shown in Table 2.
Example of the analysis process.
Ethical considerations
Prior to data collection, the midwives were contacted by their supervisors, who were informed about the study. Those who wanted to participate contacted the project manager by email or telephone to ensure volunteerism. The participants were given written and verbal information about the study, the terms of confidentiality, and their right of withdrawal at any time. A written consent form was obtained before the interview was conducted. The Norwegian Centre for Research data approved the study (reference number 55768). Quotations from the participants are used to illustrate the findings. They also contribute to the credibility and transparency of the research. To protect anonymity, fictitious names are used. The consolidated criteria for reporting qualitative research (COREQ), were followed. 35
Results
Two main themes were extracted from the data: ‘To provide individualised care’ and ‘The importance of management seeing the midwives’ potential’. Under the main theme ‘To provide individualised care’, two subthemes were identified: ‘To meet the individual woman’s needs’ and ‘Being professionally responsible’. Under the main theme ‘The importance of management seeing the midwives’ potential’, the subthemes ‘The possibility of creating safe and holistic midwifery care’ and ‘Having the opportunity to create high-quality midwifery practice’ were identified. In the following sections, the results will be presented and substantiated with quotations from the informants. Fictitious names have been used for the informants to ensure anonymity.
To provide individualised care
According to the participants, providing individualised care included meeting the individual woman’s needs and being professionally responsible.
To meet the individual woman’s needs
The informants identified the importance of meeting a woman in early pregnancy to establish a relationship. Due to this early contact, the midwife had the opportunity to meet the woman several times during pregnancy. This allowed the midwives to plan and provide individually adapted care, with the possibility of uncovering risk factors, as well as initiating preventive and health-promoting actions. It is different to meet a woman in week 8 and know that I have the whole pregnancy to meet with her, versus meeting her in week 31. Right? Where do I start? What is most important here and now? (Hanna)
Creating mutual trust and confidence in the relationship was seen as necessary by several informants to create openness in the conversation between the woman and the midwife. When the midwife showed a genuine interest in getting to know the woman, it helped to develop meaningful conversations in the consultations. This was seen as a gradual process where the midwife meets the woman on several occasions. I have experienced that women need to come back several times to check if I am trustworthy, if I am a person they want to share their secrets with. (Julie) I share some thoughts with them, and several women come back later and ask: ‘Can we continue with what you talked about in the first consultation…?’ (Mia)
Several informants stated that following up the same woman over time contributed to the midwife being able to address on-going issues and be ‘spot on’ right away. The midwife needed to have the opportunity to provide individualised care. This was seen as an important factor in providing optimal care. The informants believed that fragmented care, where women encounter several unknown caregivers, should be avoided. When following a woman from early pregnancy and support her in both the ups and downs, it is important that I come to her. We can report to each other, but that is never quite the same. (Maya) We are good at documenting, so in a way we know what the women have been through and what we have talked about with them. But there are a lot of interpersonal things that are not written down. (Ida)
Several informants said that they used different assessment tools, such as the TWEAK-score and the Edinburgh Postnatal Depression Scale (EPDS). These tools were seen by some as useful for assessing the women’s needs if they were used after a relationship was well established. Others questioned the need for these tools, as the establishment of a mutual relationship and follow-up over time were seen as the most important factors for identifying and meeting individual needs. We are using TWEAK-scores, the EPDS and all sorts of systems to reveal everything possible, but I often find that one must have much more trust and much more of a relationship before you get the serious things. (Amanda)
Several of the informants indicated that it was important to end the relationship with the woman by offering a postnatal home visit. Home visits enabled the midwives to receive feedback from the women and the midwife could make sure that the women had received adequate follow-up. The home visit was seen as a transitional phase, where the midwife transferred responsibility to the public health nurse. To gain this mutual benefit, the midwife who had followed the woman during pregnancy needed to perform these visits herself. If another midwife had been ill and I had the capacity, I actually wouldn’t perform a home visit on her behalf. It feels wrong … (Ida)
Being professionally responsible
The midwives emphasised their professional responsibility, as many sensitive questions are asked, which in turn obliges them to further investigate delicate topics. They also stated that they have a responsibility to ensure relational continuity, as this was considered necessary to observe developments in women over time. When there is no opportunity to get to know the woman, it is difficult to follow up on relevant issues. You have to meet the woman several times to be able to see the differences or to confirm the feeling you had when she went out the door last time. (Hanna) I don’t like it when the women are here in week 16 and then I do not see them again until week 32. What has happened in the meantime? I feel that it is my responsibility. Because as soon as the women come here, I feel that I somehow own them a little … they are mine and I have the professional responsibility for them. (Sophie)
Establishing a relationship over time helped ease the work and led to increased confidence in the role of the midwife. This applied to both single consultations, prenatal courses, and postnatal home visits. When the midwives offered relational continuity of care, it was easier for them to track and help the women, and the midwives experienced better job performance. When it’s a good relationship, it’s the best solution. Both concerning the upcoming family and the midwife, because there is something about being able to create safety and trust and open ourselves. (Nora)
Several informants had a desire and willingness to put in extra effort to ensure that they could attend their women. Relational continuity contributed to the midwives providing ‘a little extra’. To ensure the women’s needs were addressed, several of the informants set up extra consultations, worked overtime, and/or were available by telephone 24 hours per day. One informant went to home visits on her days off to ensure relational continuity. I fight with tooth and nail to care for my girls. I fight for this. ‘Don’t come here and take my girls! I will meet them myself, even if I have to do it at six in the afternoon!’ (Hanna).
They also stated that the desire to maintain their professional responsibility through relational continuity could quickly lead to the midwife’s role becoming too large. The midwife’s professional responsibility was described as two-sided – the midwife should be both caring and attentive but also professional. It was emphasised that the midwife must know her area of responsibility and know who can assist her when necessary so that she can concentrate on the midwifery-related tasks. It’s a key factor to know your municipality well, those who can help you in your job. Then you can get rid of what’s not your responsibility. (Hanna)
The importance of management seeing the midwives’ potential
The midwives highlighted the importance of creating safe and holistic midwifery care and high-quality midwifery practice.
The possibility of creating safe and holistic midwifery care
The informants described the health service as fragmented, both within the primary healthcare service and between the primary and specialist health service. They wanted relational continuity in the follow-up to promote normal pregnancies and to discover any complications. However, this was often impossible due to the organisation of maternity care and lack of midwife capacity. Fragmented care, where women were followed up by both a midwife and a general practitioner, often led to uncertainty about who had the ultimate responsibility. No one is entirely responsible for her, and I think that it is very unsatisfactory. To end up seeing that one loses track of things, things are not followed up. I’m supposed to stand up for the fact that my name is on the paper. (Hanna)
Several informants wanted to meet the women at each consultation to secure the responsibility for her follow-up. Attending all consultations gave the midwives an overview of the pregnancy and increased their job satisfaction. Some stated that they wanted to attend women during pregnancy, childbirth, and postnatally but experienced this as unrealistic because of the two-part nature of the current midwifery service. Sometimes we are fortunate, where we are following our own woman and can also support her at the hospital due to quick labour. Then we get the full package. (Amanda)
Several informants promoted the importance of midwives being specialists in women’s health. They expressed a vision of developing the practice into a holistic midwifery service. Tasks such as sexual education, contraception guidance, six-week postpartum check-up, and cervical cell sampling were highlighted as central to the midwife’s functional area. To achieve such a practice, the informants stressed the importance of both midwives and other professionals and leaders seeing the potential midwives have in developing a more comprehensive midwifery practice. We can do a lot of good things and lift the practice so that midwives get much more relational continuity in the follow-up, where they can follow up from birth to grave. (Amanda)
Having the opportunity to create high-quality midwifery practice
To create a holistic midwifery practice, almost all informants described the importance of leading their profession. Several were critical of the fact that the head of the midwifery service was not a midwife and they were led by others who did not have sufficient midwifery knowledge. They experienced being part of an ingrained establishment and felt that there is a contradiction between the expertise that midwives gain through education and the little amount of leadership that is allowed to them in practice. We control our profession completely autonomously. It feels very strange to be led by other professional groups. No one in this clinic knows what we are doing. They don’t know our profession. (Charlotte)
In some municipalities, midwives expressed frustration because the midwifery service is moving away from the principle of relational continuity of midwifery care. Having ownership of ‘their own women’ was seen as undesirable among the management, as it requires significant midwife resources. To positively develop the midwifery service, the informants discussed a need to highlight the significance of relational continuity to management, the municipality, and the government. The management believes that … it doesn’t matter who is following the women because she gets the same care from all … (Amanda)
To achieve relational continuity in the primary healthcare service, the informants declared the importance of management seeing the midwives’ potential. The management must ensure that midwives have the resources to deliver a service that is following current midwifery guidelines. In some municipalities, the midwives had strengthened the midwifery practice through increased employment rates. For example, the midwives wrote reports when there was not enough capacity to perform the service in accordance with Norwegian guidelines. By having sufficient resources, relational continuity was facilitated, thereby strengthening the quality of the care. I cannot work as a midwife at a public health clinic if I have a knife to my throat and no time to get to know the women. (Ida)
The informants stated that relational continuity of care was advantageous. Following a woman for a longer period and establishing a close relationship made them proud of their work. This helped to increase the midwives’ personal engagement, resulting in better job performance. Suddenly the conversation changes and you get a connection. You notice when that happens, and I think both notice it, that suddenly you touch something important to that person. (Julie) Meeting the parents who are proudly showing me the baby, it is so life-affirming and it gives me so much energy. (Amanda)
Discussion
One main finding in the present study was that the midwives thought it essential to meet women early in the pregnancy to provide individualised care. In this way, they could meet the women several times and establish a relationship with them. Results from several studies show that relational continuity of care contributes to mutual security and trust10,17,36,37 and increases the probability of a normal birth, a positive birth experience, and satisfaction with the care received.15,37,38 To establish a good relationship, one must promote open communication and provide individualised care. 10 By being available and having enough time and good communication skills, midwives can establish a relationship built on trust. 39 Boyle et al. 40 point out that a lack of continuity of care and enough time to build relationships may lead to the impression of the midwifery service being there purely for medical control purposes rather than meeting the woman’s emotional and psycho-social needs. When a midwife has enough time to follow up each woman, this facilitates individualised, high-quality care, which is in line with the original values of midwifery. 41
According to Norwegian laws and guidelines, women can choose where they receive care during the childbearing process.24,42 The midwives in this study did not always have the opportunity to attend women throughout pregnancy due to a lack of capacity. The first consultation was often performed by a general practitioner, and the midwives did not meet the women early on. When midwives are not able to perform their tasks, pregnant women may not be offered the care to which they are entitled. 43
Another finding was the positive effects of the home visits. Home visits represented an opportunity for feedback and learning for the midwife. The significance of home visits is supported by a Norwegian study which shows that home visits may contribute to the development of the midwife identity and are seen as a meaningful learning experience. 44 A home visit shortly after birth is increasingly important due to shorter hospital stays after birth. 11 The home visit is regarded as a good opportunity to end the relationship between the midwife and the new parents.11,44
The participants highlighted that relational continuity of midwifery care contributed to greater personal engagement among the midwives and led to increased job satisfaction. With relational continuity in midwifery care, midwives can work more independently and have increased control over their day-to-day activities. Jepsen et al. 41 highlight that continuity of care after birth may give midwives a sense of quality in the care they provide and that doing their utmost for the women and receiving gratitude for their work may give them a sense of meaningfulness. Additionally, relational continuity may increase the professional well-being of midwives and reduce the risk of burnout. 45 Relational continuity can also allow midwives to learn and gain confidence. 36 Job satisfaction can provide financial gain, as it helps midwives stay in the same workplace for longer. 46
The midwives did their utmost to ensure continuity in the follow-up of pregnant women. It could be that the midwives felt obligated to help and were genuinely interested in the women. 43 Being inaccessible may be seen as failing the women’s need for continuity of care. 41 Studies show that having the opportunity to make direct contact with a known midwife during pregnancy40,41 and to contact a known midwife between check-ups 40 is hugely important to women. However, a challenge with relational continuity of care is that midwives can easily become overworked and too attached because they work closely with women and form strong bonds with them. 36 Relational continuity in midwifery care may affect a midwife’s privacy, but the benefits of relational continuity are greater than the disadvantages. 41
The participants highlighted the challenges of management not seeing the midwives’ potential. The midwives expressed a desire to lead their profession within the primary healthcare service. They stated that other professionals who did not have sufficient knowledge of the midwifery practice were in leadership roles and declared that only midwives should lead the midwifery service. According to The Directorate of Health and Social Affairs, 24 good management is a prerequisite for achieving quality. The International Confederation of Midwives promotes the importance of midwives managing the midwifery practice themselves and states that the midwifery service should be strengthened globally through increased access to midwife-led practices. 25 A midwifery-led practice based on continuity of care means that midwives themselves are in leadership roles and independently follow up on healthy women during the childbearing process. 6 One of the subgoals for a coherent service in Norway is to create a responsive structure that includes a holistic midwifery service. This means that the accountability structure must be appropriately adapted in primary healthcare services. 4 Research shows that Norwegian midwives experience their role as autonomous and that the support from their management affects their practice. 31 Having ownership of their profession and being part of a larger community is highly valued by midwives. 41 Collaboration with other professional groups in primary healthcare services is essential to provide optimal care.47,48 Through a midwife-led practice, midwives can use their full competence, but to do that, it is important that the management sees this importance and facilitates such practice. 43
The present study found that midwives want to further develop the practice into a holistic midwifery service with a focus on women’s health through a lifetime perspective. A holistic midwifery service can allow midwives to utilise the breadth of their expertise and contribute to resource utilisation. Organising the midwifery service in such a way could contribute to continuity in antenatal and postnatal care and an increased feeling of safety for the women and their families. 4 Re-organising the midwifery service to facilitate continuity of care could better utilise the full competencies of midwives. 49 To achieve this, midwives must be able to offer the full spectrum of midwifery care and have an influence on the organisation of their practice. 39 Management and other professions must have a better understanding of what midwives do and the power that lies in the midwifery profession. Together, this can help increase the quality of midwifery care.39,50
Methodological considerations
When considering the transferability 51 of the findings it is important to consider that this study focused on the experiences of a small group of midwives about relational continuity in the midwifery practice. However, data saturation was achieved, and the midwives offered extensive descriptions, which provided a deeper insight into and understanding of how they experienced relational continuity in their midwifery practice and what challenges they encountered. For data analysis, systematic text condensation 32 was considered appropriate. The authors performed the four-step analysis procedure jointly, which enhanced the credibility of the study. To establish dependability, two authors conducted all the interviews and during eight of the interviews, both authors were present. They used the same interview guide. The four-step analysis process has been presented in Table 2, which increases the confirmability of the study. To allow transparency of the reporting of the results, quotations have been presented with fictitious names for the participants, showing which midwife gave which quotation. 51
Conclusions
This study shows that relational continuity of midwifery care is of great importance to midwives working in the primary healthcare service. The informants identified the importance of meeting a woman in early pregnancy to establish a relationship. Due to this early contact, the midwife had the opportunity to meet the woman several times during pregnancy to plan and provide individually adapted care. The participants highlighted that relational continuity of care contributed to greater personal engagement and the midwives did their utmost to ensure continuity in the follow-up of pregnant women. To achieve relational continuity in the primary healthcare service, the informants declared the significance of management seeing the midwives’ potential. The midwives emphasised the importance of safe and holistic midwifery care, a high-quality midwifery practice, and a practice that allows them to lead their profession and utilise their full competency. To implement a comprehensive midwifery service with a focus on relational continuity, it is necessary to perform further research regarding the organisation of antenatal, intrapartum, and postnatal care in Norway.
Footnotes
Acknowledgements
We wish to thank the midwives who shared their time and experiences with us.
Author contributions
The article is the authors’ original work. All authors have seen and approved the final version of the manuscript being submitted.
Ingvild Aune: Project administration, supervision, conceptualisation, data analysis, methodology, writing/revising the article.
Trude Tysland: Data collection, conceptualisation, data analysis, methodology, writing/revising the article.
Sigrid Amalie Vollheim: Data collection, conceptualisation, data analysis, methodology, writing/revising the article.
Conflict of interest
The authors declare that there is no conflict of interest
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.