
Abstract
This study investigated first-line managers’ experience of and responses to a concise leadership intervention to facilitate the implementation of oral care clinical practice guidelines (CPGs) in nursing homes. Leadership is known to be an important element in knowledge implementation but little is known as to what supports managers to facilitate the process. By means of a process evaluation with mixed methods, the context and a three-month leadership program was explored, including activities during and in relation to the program, and the effects in terms of oral care CPG implementation plans. While the managers appreciated the intervention and considered improved oral care to be a priority, their implementation plans mainly focused the dissemination of an oral care checklist. The findings suggest that extended implementation interventions engaging both managers and clinical staff are needed, and that a concise intervention does not facilitate first-line managers to adopt behaviors known to facilitate knowledge implementation.
Introduction
Leadership has been identified as a significant factor in the implementation of evidence-based clinical practice guidelines (CPGs) in healthcare and care of older people. 1 First-line managers are accountable for the quality of care in their organizations and, while there is a call for a faster and more consistent uptake of evidence-based CPGs, there is also a need for better understanding of the manager’s role and their potential function as facilitators of this process. 2 Rather, first-line managers need support in implementing CPGs. 3 The Ottawa Model of Implementation Leadership, O-MILe, suggests a structure for generating, effectuating and evaluating an implementation plan; in addition, the model includes a taxonomy of leadership behaviors, defined as relations-, change-, and task-oriented behaviors. All behaviors are found to contribute to effective leadership and facilitating the implementation of CPGs.3,4
Background
One way to support high quality care is the implementation of clinical practice guidelines. 5 Clinical practice guidelines (CPGs) are based on systematic reviews of the evidence, and are compiled at national, regional or local level.6,7 In order to reinforce safe practices and increase the quality of healthcare, an increased understanding of what facilitates knowledge implementation is needed. 8 Numerous studies have shown that nursing managers need to facilitate knowledge implementation.9–12 However, nursing home managers in Sweden have been found to display limited engagement in the implementation of CPGs. 13 This could be a result of lack of support; a complete picture as to what factors support managers’ adoption of means to facilitate the implementation of CPGs is pending. Nevertheless, an adoption by first-line managers of relations-, change-, and task-oriented behaviors is found to facilitate knowledge implementation. 14
There is an alleged complexity in addressing managers’ engagement and behaviors; supposedly, studying a potential change, or lack thereof, in individuals and organizations requires that the clinical evidence applied, the context in which the evidence is to be implemented, and the implementation strategy to facilitate change are considered.15–17 Thus, prior to a full study, a brief leadership program with a limited number of first-line managers in nursing homes in Sweden was trialed in 2014, with oral care CPGs as the case of evidence; improved oral healthcare is one of the single most important areas for enhancing the health and wellbeing of residents of nursing homes. 18 The adoption of the national evidence-based oral care CPGs varies notably, particularly with regard to the recommendations for frail older people. 19 This article represents first-line managers’ experience of and responses to the concise leadership intervention designed to facilitate their implementation of CPGs.
Method
Design
We conducted a process evaluation which considered the leadership intervention, the implementation of the intervention, and the mechanisms of the intervention activities, all in relation to the context and outcomes. 20 Outcomes of the intervention are represented by the intermediate effects, that is, the nursing home managers’ implementation plans, particularly the adoption of leadership behaviors designed to facilitate the implementation of the oral care CPGs.
Setting
A purposeful sample of four nursing homes in a standard municipality of circa 57,000 inhabitants was chosen: two units in a larger nursing home in a large town, and three nursing homes in smaller towns. Five first-line managers of these units and homes participated in the leadership intervention program. The units were typical for Swedish nursing homes, having 24–42 rooms (mean 34 rooms) for residents, and 20–30 nursing staff, that is, licensed practical nurses/healthcare assistants (mean 26), per unit/home. Each unit had an allocated registered nurse (RN), but with a separate first-line manager. All residents had extensive nursing needs, and met the criteria of ‘frail older people’. 21
Procedure
Baseline data were collected from August to September 2014, and the intervention ran from late September to early December 2014. The follow-up data collection was executed three months post intervention, in March
The intervention and its causal assumptions
Content of the evidence-based clinical practice guidelines on oral care applied in the study.

Source: Socialstyrelsen [The National Board of Health and Welfare]. Nationella riktlinjer för vuxentandvård 2011 – stöd för styrning och ledning [National guidelines for adult dental care 2011 – support for control and management]. Stockholm: Socialstyrelsen, 2011.
Overview of the leadership intervention delivered, and associated assumptions.
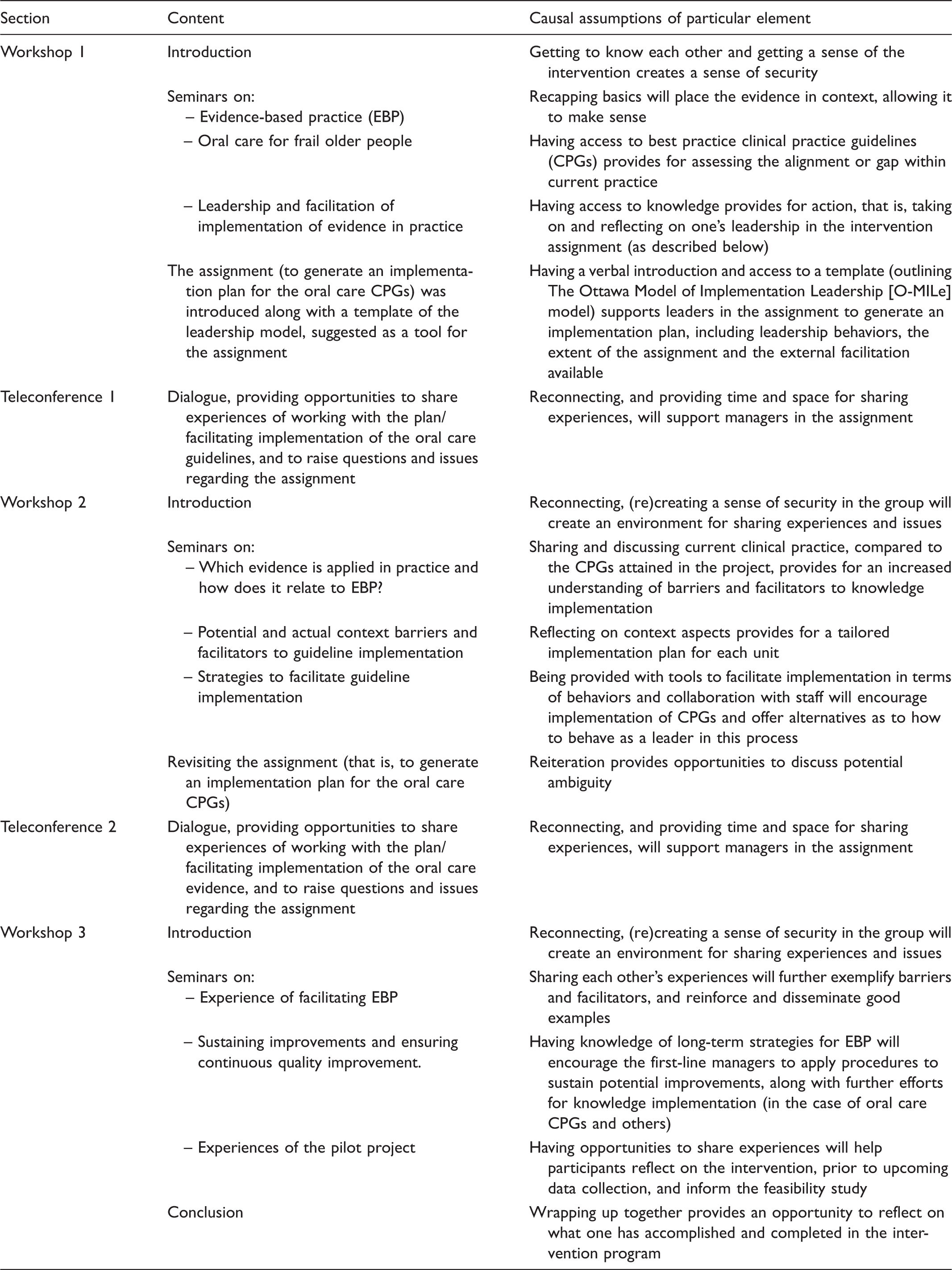
As a basis for the leadership intervention and its implementation, we assumed that:
The generating, effectuating and evaluating of an implementation plan for CPGs is promoted by external facilitators delivering the intervention having: a) competence in evidence-based practice, b) knowledge of up-to-date evidence on the clinical issue, in this case, oral care, and c) contemporary knowledge of leadership and its connection to knowledge implementation in theory and practice.
23
The pedagogical techniques applied, including workshops and opportunities for mutual reflection, support the participants in understanding knowledge implementation, guiding them to capture context, implement knowledge in practice, and utilize tools and strategies to facilitate knowledge implementation.
24
Group sessions provide opportunities to share experiences and concerns, and thus increase opportunities for learning.
25
Data collection and analysis
To convey all aspects of the process evaluation, there was a parallel collection and analysis of qualitative and quantitative data. 26
Qualitative data were collected by means of:
Interviews with the five first-line managers participating in the intervention, and the RN and a member of the nursing staff in each unit. The interviews adopted a narrative style, and followed agreed semi-structured guides on: the experience of implementation of CPGs; barriers and facilitators to change; key events; social, political and financial aspects of care; service delivery; and delivery of oral care. All interviews were audio-recorded and transcribed verbatim. Recordings of the intervention program, including video-recordings of the face-to-face workshops as well as tape-recordings and notes from the teleconferences.
The qualitative data were analyzed using qualitative content analysis. 27 All interview transcripts were initially read to obtain a naïve understanding, and thereafter inductively coded by two members of the research team not engaged in the delivery of the intervention, forming subcategories. These provided a matrix to a subsequent deductive analysis of interviews and the recordings of the intervention program.
The quantitative data consisted of two surveys, distributed to the nursing staff in each site at baseline:
A survey on context, using the Alberta Context Tool (ACT),
28
including the concepts of: leadership; culture; evaluation; social capital; formal interactions; informal interactions; structural/electronic resources; and organizational slack. The tool has been previously translated to Swedish and found to be valid in a nursing home setting.
29
A Swedish survey on leadership behaviors, the FARAX360,
30
measuring first-line managers’ relations-, change-, and task-oriented behaviors.
The survey data were analyzed by means of descriptive statistics, using SPSS version 20.
To conclude, the emerging findings were considered in relation to the process evaluation framework, 20 informing the components’ ‘context’, ‘implementation’, ‘mechanisms of impact’, and ‘outcomes’ – the latter including a qualitative appraisal of the implementation plans developed by the managers.
Ethical considerations
Ethical approval was granted by the Regional Ethical Review Board in Uppsala, Sweden (no. 2014/273).
Results
The findings are presented in accordance with the process evaluation framework: Context, Implementation, Mechanism, and Outcomes, in this case, Intermediate effects. Further, the relations between the components, including the context, implementation and mechanisms supposedly generating facilitators and barriers, respectively, and the intermediate effects are illustrated in Figure 1.
Schematic illustration of the process evaluation and outcomes of the study.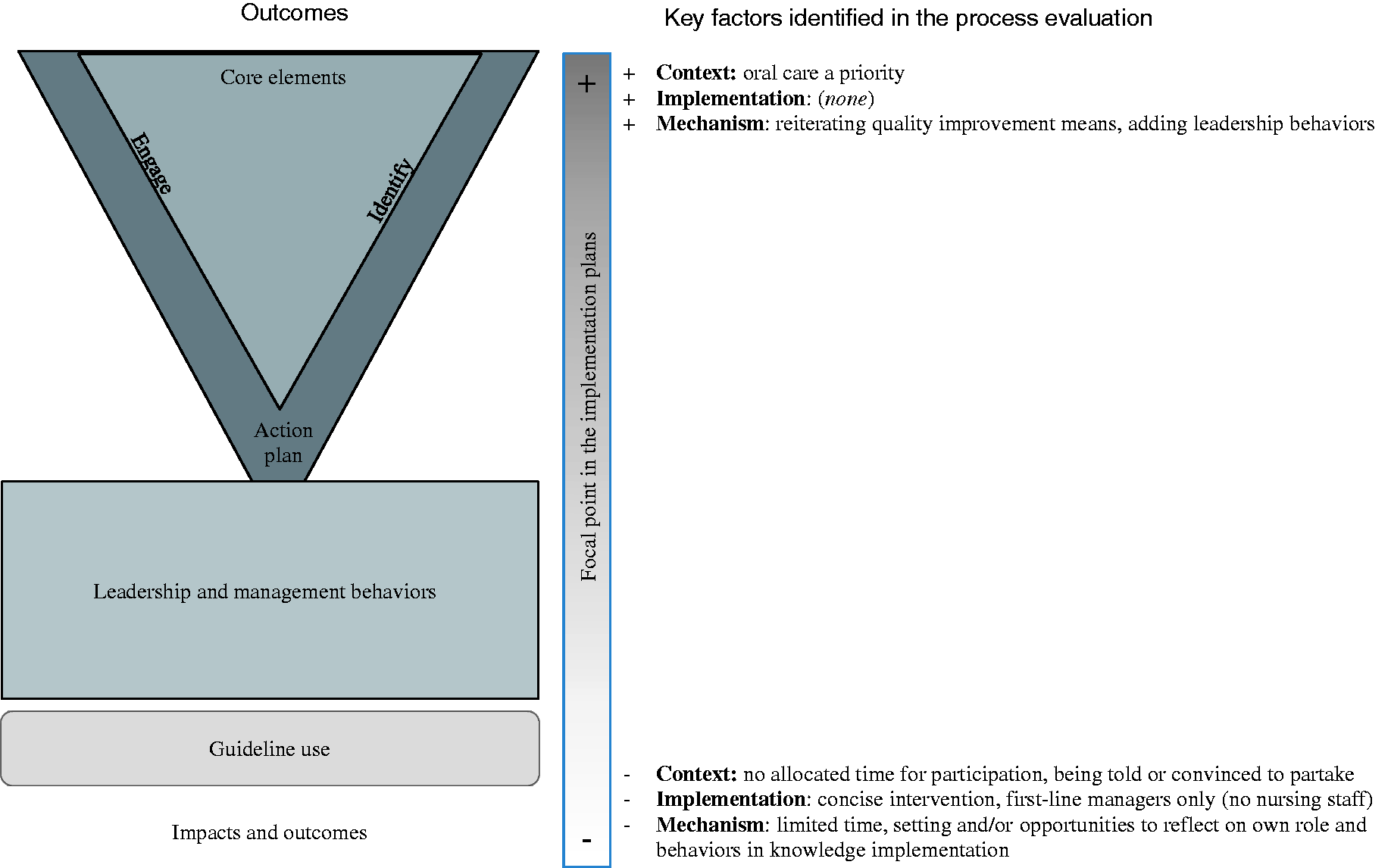
Context
Oral care
Before the intervention, none of the sites had oral care guidelines. An agreement between the municipality and the regional dental care provider ensured dental support: a dental hygienist paid annual visits to all nursing homes, performing assessments of the oral status of each resident, with a member of the nursing staff being instructed on the individual’s oral care. The dental hygienist had presented a general tutorial on oral care in all of the nursing homes. Further, for each resident, the dental hygienist prescribed an oral care plan, which was placed in the resident’s bathroom. For residents requiring assistance, oral care was provided by the nursing staff.
While the RNs had primary responsibility for the care of the older people, they had limited involvement in the planning and/or performance of oral care. However, the nursing staff were required to report any oral issues to the RN, who could take action in terms of a nursing intervention or making a referral to the dental hygienist or the dentist. I would assume some [staff] find it [oral care] horrid. And then, not everybody thinks it is important. (Nursing staff, prior to the intervention) In such case [if a resident has an oral care issue], we contact the nurse, and she gets in touch with the dental hygienist, and they will come [to the nursing home]. (Nursing staff, prior to the intervention)
Feedback, resources and leadership
Assessments of oral care were included in the standard reports to the national nursing quality registry, and were reported for all residents. However, the local data were neither used for analysis nor improvement of oral care.
The managers had extensive experience as first-line leaders in the care of older people. They depicted that the workload in care of older people continuously increases; they were frequently requested by their superiors to execute change in their nursing homes (such as implementing new administrative or clinical routines). Yet, they experienced limited opportunities to discuss the relevance of a new routine, why it was proposed, the rationale for change, the time frame for an implementation, and/or how to proceed. Further, the new routines were seldom accompanied by suggestions as to what routines should be replaced. The first-line managers primarily used the regular workplace meetings to inform the nursing staff about new routines; if needed, they would repeat the instructions until they considered all staff to have recognized the information. Implementing new routines … it is very difficult. OK, we bring things up but … it’s tricky enough to manage everything as it is … (RN, prior to the intervention) And then there are always some laggards – those who do not want to [change things]. And to constantly nudge them too, about the advantages … Provide some extra support for them, and some who are negative to change. (Manager, prior to the intervention) Means and standard deviations for the study’s participants on the Alberta Context Tool (ACT) and FARAX instruments. Responses not including a unit identification. These sub-dimensions were scored on a five-point Likert agreement scale. These sub-dimensions are means of summed count variables. These sub-dimensions were scored on a six-point Likert agreement scale.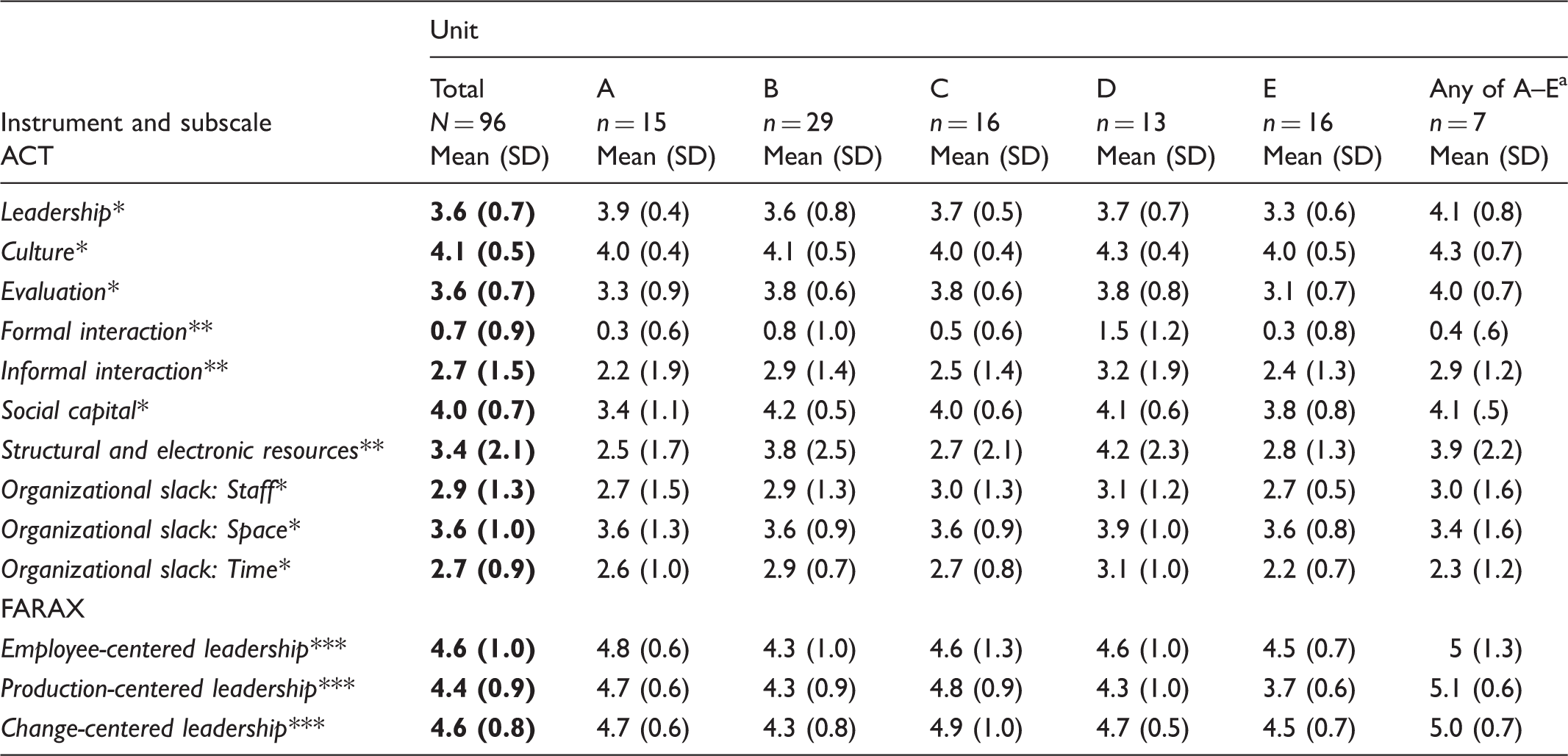
Implementation
As proposed, the intervention was delivered to the first-line managers in two face-to-face seminars (workshops 1 and 3) and one video-conference (workshop 2), plus two teleconferences. Further opportunities to contact the external facilitators via email or telephone, in between workshops and teleconferences, were offered but not utilized.
While all of the managers had the opportunity to set time aside for the workshops, they themselves had to reorganize their daily work to participate. Most participated in the entire program, but two managers did not attend the third and final workshop due to annual leave. Further, in one of the teleconferences, one first-line manager was excluded due to technical problems. This was resolved by conducting a subsequent one-to-one follow-up between one of the external facilitators and the manager, during which the manager shared notably more issues relating to the implementation of knowledge in general and the assignment of oral care CPG implementation in particular than in the group sessions.
Mechanisms
In the planning phase, the upper-level manager of the municipality was asked to suggest urban and rural nursing homes for this study. Upon initial contact with the first-line managers, we found that they had already either been convinced or instructed to participate in the intervention. Yet, at the first workshop, all first-line managers indicated that they were unprepared, and wondered what was expected of them. I heard that it was about oral care, and that’s somewhat embarrassing … maybe we don’t really include that [oral care] in the everyday nursing care … but we need tools to secure that it is done. (Manager, prior to the intervention) I can tell for sure that the documentation is improving, one is reminded [by the checklist]. (Manager, post intervention) It [the model] is not new really, but it’s good to be reminded, to take the time and sit down and complete the structure [the implementation plan]. That’s what’s lacking, the structure … you keep informing [staff] without really thinking it through … (Manager, post intervention) This could have worked much better had it not been oral care, but an issue we have to deal with … ’Cause it’s frustrating that as a manager, someone else tells [you] what’s important or not … (Manager, post intervention)
Outcomes
The first-line managers appreciated the intervention for its focus on leadership and leadership behaviors. However, neither the implementation plans nor the interviews indicated that the managers had adopted this element of the intervention, that is, to reflect on and focus on one’s own behaviors with regard to facilitating the implementation of CPGs. While the leadership behaviors suggested to engage staff and facilitate change in the organization were considered interesting and appealing by the managers, they found it difficult to reflect on their own behaviors; such reflection would require considerable amounts of time and support, beyond that provided within the brief intervention program. A couple of months was too short … too compressed. The meetings were long enough but to work on the implementation, using the theories … should have been over a longer period of time, taking in the knowledge and adapting it for oneself. (Manager, post intervention) But then, it depends … which kind of relation one has and how well we collaborate. Are we on speaking terms here? How to work on this together? And sometimes it’s awkward … and sometimes super easy … (Manager, post intervention) They have placed checklists in each room so that one checks each morning and evening that it is done [the oral care]. That serves as a reminder, for everyone, so I think it’s become more thorough [the oral care]. (Manager, post intervention)
Discussion
With a pending need to better understand which strategies facilitate the implementation of evidence in practice, the findings of this study contribute to the knowledge of what does (or rather, does not) support managers, and the factors that can influence knowledge implementation initiatives.
In the care of older people, healthcare in general, and in other knowledge-intense organizations, there is a growing awareness that leadership is fundamental in promoting systematic improvements, including knowledge implementation. In numerous cases, healthcare and nursing home managers call for concise support on implementing knowledge in clinical practice; the lack of time is suggested to be an impediment to promoting evidence-based practice. 22 Further, a lack of resources creates a strong urge to alleviate the perceived scarcity; 31 this renders a focus on tasks that seem urgent, while long-term objectives, such as knowledge implementation, are neglected by a manager under stress. Our concise program procured limited progress, but the managers focused on a particular task, using a straightforward dissemination approach for a checklist, rather than the implementation of the CPGs. This aligns with previous findings of nursing home managers being minimally engaged in knowledge implementation. 13 While this calls for sincere efforts to support managers in nursing homes, a concise intervention such as the one tested in this study may be of little worth. Rather, extended programs with facilitation tailored to context might be more effective in guideline implementation. 2
Alas, despite our intervention, oral care for frail older people remains an issue in the nursing homes where this study was performed, and presumably beyond. 19 Although the checklist may have improved oral care practices, our intervention did not reflect that the managers’ behaviors increased the nursing staff’s focus on oral care. In the care of older people, oral care is considered an everyday yet complex issue of low priority. 32 With the noted lack of engagement, future studies aimed at knowledge implementation should include professional representatives along with first-line managers.23,33
Previous experience suggests that engagement, as an organization and/or as individuals, affects the process and thus the outcomes of implementation projects. 34 The intervention participants were all aware of a need to improve the conditions to support evidence-based practice of oral care in their nursing homes and set out to enact change. However, none of the managers had volunteered to partake in the leadership intervention. While this may explain the fact that the implementation plans mainly focused on the quality improvement aspects, with limited reflections on leadership behaviors, it may also be an effect of the concise intervention, where supervision of the managers’ role and function in facilitating knowledge implementation was not feasible.
Our intervention was primarily a group intervention – thus differing from the individual mentoring described in similar Canadian studies applying the O-MILe. 35 Challenging one’s own conduct necessitates a suitable environment, 36 which was not the case with this group of participants; rather, the establishment of a creative team was limited. Future leadership interventions should extend participation to nursing team members and dental care support to foster teams, 37 and/or provide one-to-one interactions between external facilitators and first-line managers to promote further adoption of appropriate leadership behaviors. Further, this study reinforces the need to recognize the complexity of knowledge implementation, where leadership may represent a contextual factor, as well as a feature of facilitation.2,16
Methodological reflections
Although we strived to include a variety of nursing homes, this article reports the findings of a study representing only five managers and their units. Keeping this limitation in mind when appraising the study, the findings can serve as valuable input into future knowledge implementation initiatives. Further, the data collection and analysis procedures illuminate most aspects of the feasibility of the leadership intervention through process evaluation. However, future studies should consider including data on external and/or parallel processes, such as extended leadership influences, to further capture the mechanisms and illuminate the outcomes of implementation interventions.
Conclusion
While a purposeful strategy for supporting managers to facilitate knowledge implementation is still wanting, concise programs that focus on first-line leaders should be carefully considered. Long-term strategies supporting managers in phrasing and conducting implementation plans, including their own activities and behaviors, are more likely needed. Further, when promoting the implementation of evidence-based CPGs, key professionals need to be involved in the process, to benefit residents’ quality of care. Thus, implementation of nursing CPGs in nursing homes should engage nurses.
Footnotes
Authors’ contributions
LO, ME, LW, ACE, and BJ planned the project, and LO and LW obtained funding. ME and LO collected and analyzed the qualitative data, in collaboration with ACE and BJ. LD analyzed the quantitative data. ACE drafted the manuscript and revised it in collaboration with all co-authors, who have read and approved the final manuscript for submission.
Acknowledgements
We wish to thank Professor Estabrooks, and her research team at University of Alberta, Canada, for permission to use the Alberta Context Tool and the FARAX group, Sweden, for permitting us to use FARAX360 in this study. Further, Associate Professor W Gifford, University of Ottawa, Canada, has kindly shared the Ottawa Model of Implementation Leadership, O-MILe, and approved of its application in ![]() , to illustrate our findings.
, to illustrate our findings.
Funding
The research leading to these results received funding from VINNOVA, the County Council of Dalarna and the Region of Dalarna.
Conflict of interest
The authors declare that there is no conflict of interest.