
Abstract
We aimed to evaluate effects of the intervention on self-rated health, experiences of security/safety and symptoms. A non-blinded controlled trial was performed with participants randomised to either the intervention group or a control group, with follow-ups at 3, 6 and 12 months. The intervention involved collaboration between a nurse with geriatric competence at the emergency department, the hospital wards and a multi-professional team for care and rehabilitation of older adults, with a case manager from the municipality as the hub. Older people who sought care at the emergency department at Sahlgrenska University Hospital/Mölndal and who were discharged to their own homes in the Mölndal municipality were asked to participate. Inclusion criteria were age 80 years and older, or 65 to 79 years with at least one chronic disease and dependency in at least one activity of daily living. Analyses were conducted on the basis of the intention-to-treat principle. Outcome measures were self-rated health, experiences of security/safety and symptoms. These were analysed using Svensson’s method. Of 161 participants, 76 were allocated to the control group and 85 to the intervention group. Positive effects of the intervention were observed for frail older adult’s symptoms and self-rated health.
Keywords
Background
The proportion of older people is expected to increase in Sweden 1 and worldwide in the coming decades. 2 People aged 65 years and older account for 40% of all visits to the emergency department. 1 Fragmentation of care for older people is recognised as an international problem, and the need to develop a coordinated and integrated system of care has been raised. 3 Frail older adults already represent a large proportion of those in need of care and support from the healthcare system. 4 The system will face many additional challenges in the future, owing to the complexity of needs of frail older adults. As people age, their reserve capacity decreases and risks of morbidity, ill health and frailty increase.5,6 A Swedish review has emphasised the benefits of an integrated and structured healthcare system involving multi-professional teams with direct patient responsibility for frail older adults. 1 Another review of interventions to prevent disability among frail community-living older adults has pointed out the success of interventions that included a multi-disciplinary, multi-factorial approach, and has recommended that such a comprehensive approach be directed by individual patients’ needs. 7 In this study, we considered frailty as a multi-dimensional geriatric syndrome attributable to the multi-system deterioration of reserve capacity in older age. 5 High levels of frailty are associated with low levels of both life satisfaction 8 and physical and mental health-related quality of life. 9
Self-rated health (SRH) is a well-used, reliable measurement within the broader concept of general health. 10 Self-rated health refers to overall health status and captures multiple subjective aspects of health that decline with age, 11 although studies also exist that indicate improvement of subjective health with increased age.10,12 Self-rated health is a significant predictor of morbidity, mortality and disability among elders.11,13 Low SRH has been linked to disability and low physical functioning in an ageing population.14,15 As people age, their reserve capacity decreases and the risks of morbidity, ill health and frailty increase.5,6 At the same time, some studies indicate improvement of subjective health with increased age.10,12 This phenomenon, which has been described as the paradox of subjective health in ageing,10,11 was emphasised by a recent study showing that approximately two-thirds of the oldest-old adults (80+ years) reported their health as at least ‘good’. 12 The experience of good health despite frailty is possible if older people are able to experience harmony and balance in everyday life. 16 Frail older adults’ experiences of good health are associated with feeling self-assured and capable in everyday life, which is commonly based on their ability to manage their unpredictable bodies (co-occurrence of many symptoms and ailments that can lead to rapid deterioration), maintain a positive outlook, remain in familiar surroundings, handle everyday tasks, and have a sense of belonging and connection to the whole (social network). 17 Therefore, interventions for frail older adults could benefit from a person-centred approach and planning that improves the coordination of care. 18 The need for developing and evaluating interventions for frail older adults has been emphasised previously. 19 Person-centred care is defined here as ‘care that is respectful and responsive to individual patient preferences, needs, and values, and ensures that patient values guide all clinical decisions’.20(p.49) Person-centred care in practice is initiated by capturing the patient’s narratives and experiences of his/her suffering in an everyday context. The next step is invoking a partnership between patient and caregivers through shared discussion and planning of care and treatment. The last step is documenting the patient’s preferences, beliefs, values and decision-making. 21
Previous studies have suggested that experiences of security/safety and having fewer symptoms are important contributors to elders’ subjective health; 17 therefore, it is important to take these into account when evaluating an integrated intervention for frail elders. The theoretical framework of such an intervention emphasises teamwork and the importance of early coordination of healthcare interventions. Further, from a holistic perspective, sensitivity to frail elders’ real and everyday needs, desires and challenges is key for planning within the healthcare system. The overall hypothesis of the intervention ‘Continuum of care for frail elderly people, from the emergency ward to living at home’ (hereafter, CC) was that this intervention programme for frail elders could reduce the number of visits to the emergency ward, increase satisfaction with health and social care and maintain functional abilities. 22 Further, the hypothesis of the current study was that such a comprehensive continuum of care intervention can have the positive effect of maintaining frail elders’ self-rated health, feelings of security/safety, and experiences of symptoms. Previous studies on the effects of the CC intervention have shown improvement in frail elders’ activities of daily living (ADL), 23 satisfaction with quality of care 24 and self-determination. 25 The CC intervention has also shown positive results for implementation fidelity26,27 and attention to involved actors’ commitment to the intervention. 28 The aim of this study was to evaluate effects of the CC intervention on self-rated health, experiences of security/safety and symptoms.
Methods
Study design
This article presents the intervention and the outcome measurements in accordance with the 2010 CONSORT statement. 29 The study is a part of the CC intervention project, a randomised, non-blinded controlled trial with two study arms – one intervention group and one control group – with data collection at baseline and follow-ups at 3, 6 and 12 months. 22 The intervention was targeted to all frail elders living in a municipality in the west of Sweden. It was a multi-professional collaboration among the municipality, primary care and Sahlgrenska University Hospital. The study was conducted during the period October 2008 to November 2011. Ethical approval was obtained (ref. no: 413-08) from the regional Ethical Review Board in Gothenburg, and the study is registered at ClinicalTrials.gov: NCT01260493.
Participants and setting
The intention was that the study group should be a representative sample of frail elders at high risk of further care consumption. The sample includes elders who sought care at the emergency department at Sahlgrenska University Hospital/Mölndal and who were discharged to their own homes in the municipality of Mölndal, Sweden. The inclusion criteria were: aged 80 years and older, or aged 65 to 79 years with at least one chronic disease and dependent in at least one activity of daily living. People who had severe acute illness (with immediate need for medical treatment), were in need of palliative care (as documented in the medical record), suffered from dementia or cognitive impairment (according to medical records or judgment of registered nurses with geriatric training at the emergency department) were excluded. Two registered nurses with geriatric competence in the emergency department invited the older adults to participate. Those who accepted signed a written consent and were randomised to either the intervention or control group through use of a system of sealed opaque envelopes. 22
Procedure
Registered nurses with geriatric training and long experience of working in a geriatric hospital ward recruited the participants during the daytime on weekdays. Elders attending the emergency department at other hours were recruited either through a visit to the wards or by letter if they were discharged before the recruitment period – 17 participants were recruited via letter. The participants were informed about the study both verbally and in writing. The information included a description of the study procedure and what was expected of participants. It was stressed, in both the verbal and the written information, that participation was voluntary. There were opportunities to ask questions if anything was unclear.
Intervention group
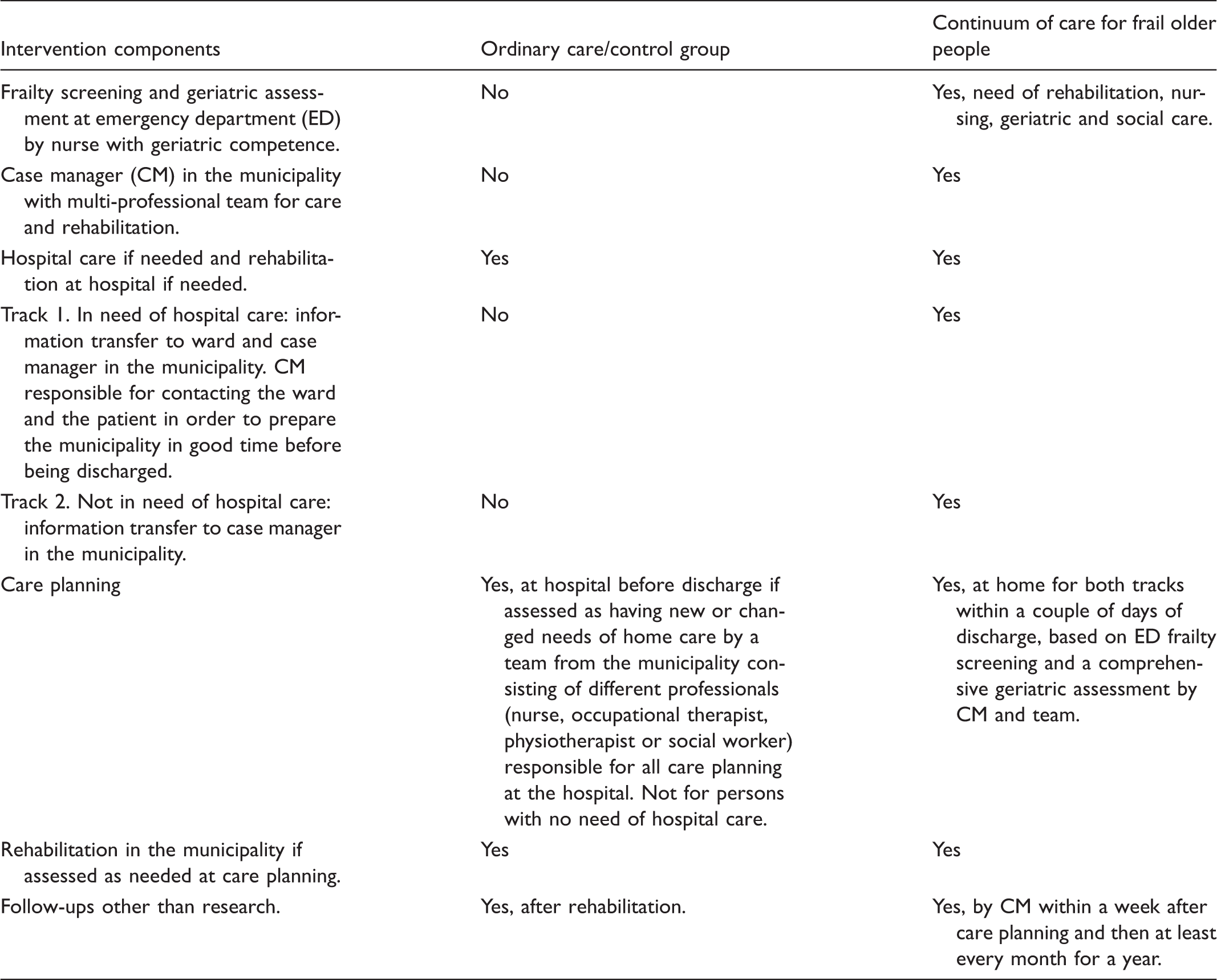
Components of ordinary care and continuum of care.
Control group
The control group received ordinary care, which did not include access to the multi-professional team and case manager. The elders in the control group, who were admitted to one of the geriatric hospital wards, had care planning (if needed) at hospital without follow-ups at their homes. The multi-professional team at the municipality did not get information from the hospital in the event that the elders in the control group revisited the emergency department, and no additional care planning was carried out in such cases. No care planning was held. No additional support or information was offered to the relatives of the elders in the control group. For details, see Table 1.22,23,27
Data collection
Data were collected through assessments and face-to-face interviews using a structured questionnaire which were conducted in the elders’ homes. Most baseline interviews were carried out within a week after discharge, but in three cases data collection was postponed by one to two weeks, and in one case the baseline interview was done as part of the three-month follow-up, in all instances to reduce the burden on the elders. The baseline data for the intervention group were collected by the multi-professional team as part of their comprehensive geriatric assessment. The baseline data for the control group and all follow-ups for both groups were collected by research assistants, who were either registered occupational therapists or registered nurses. Follow-up data were collected at 3, 6 and 12 months following discharge. All interviewers were trained thoroughly to interview, assess and observe according to the guidelines for the different outcome measurements. To ensure as much standardisation of the assessments as possible, study protocol meetings were held regularly throughout the study. The interviews encompassed a comprehensive geriatric assessment including a range of questions, tests and measurements for factors including activity, functional ability, life satisfaction, satisfaction with health and social care, dependence, self-estimated health, health-related quality of life, symptoms, and medications. 22
Outcome measures
Self-rated health
Self-rated health (SRH) was derived from one statement on the Short-Form Health Survey (SF-36): ‘In general, you would say your health is …’ followed by responses on a five-point Likert-type scale: excellent, very good, good, fair or poor. 30
Symptoms
Symptoms during the previous three months were assessed by one part of the Göteborg quality of life instrument, with yes or no responses. 31 A summary score of 1–30 symptoms was computed for each participant and scores were transformed into a six-grade scale with an interval of five symptoms in each grade.
Experiences of security/safety
A single question asked whether the participant had a sense of security/safety, with five possible responses: always, often, sometimes, rarely or never.
Sample size
A power calculation was made based on the Berg Balance Scale, which is a measure of frailty and one of the primary outcome variables. The scale has a range of 0 to 56, with an assumed mean for the intervention group of 32 and for the control group of 28 (15% difference), and a standard deviation of eight in both groups. To be able to detect a difference between the intervention and control groups with a two-sided test and a significance level of alpha = 0.05 and 80% power, 65 persons were needed in each group. The primary outcomes of the main study (CC intervention) were healthcare consumption, satisfaction with health and social care, and functional ability.22,23
Statistical analysis
The analyses were conducted on the basis of the intention-to-treat principle (ITT); i.e. missing data were addressed through imputation of the missing values by an estimated expected value. 32 Different methods for imputation were used depending on the reason for the missing value.32,33 The basic assumption was that older adults would deteriorate over time as a natural course of the ageing process. Therefore, the approach to data imputation in this study was to replace the missing value with a value based on the median change of deterioration (MCD) between two measuring points (baseline and the three-month follow-up or between two follow-ups) for all who participated at both measuring points, as suggested in previous studies.23,34 The MCD was added to the last actual individual value recorded, and imputed, substituting for missing data at the 3, 6 and 12-month follow-ups. For participants who completed the study but did not have observed values at each measurement occasion, we imputed the elders’ values on the same outcomes measured at a different point in time. 32 Missing values at baseline were replaced with the values of the respective outcome for that participant at the next follow-up, and missing values between two measurement occasions were imputed as a value between the observed values (mean). 32 The worst case was imputed at each follow-up for missing data due to death. To ensure that the MCD analysis was in line with complete cases, a sensitivity analysis was made showing alignment trends. 33
The baseline characteristics of study participants in each group were compared using a chi-square test. 35 The effect of the intervention on self-rated health, experiences of security/safety and symptoms were analysed using Svensson’s method, a nonparametric statistical approach developed for evaluation of change in ordered categorical data. 36 The software for Svensson’s method version 1.1.2 was used during the calculating phase. The method makes it possible to measure systematic patterns of change for the group separately from the individual variation unexplained by the systematic group change. A systematic change in position on a given scale is measured by the relative position (RP), which is the difference between the probabilities of systematic improvement and deterioration. Possible values of RP range from −1 to 1, where higher values indicate greater change, and a value of 0 means lack of systematic change.36,37 Higher RPs indicate greater levels of change. An RP above 0 for self-rated health, for example, means that self-rated health has improved, and a value below 0 means that self-rated health has declined, from baseline to follow-up.36,38 Relative Rank Variance (RV) is a measure of the individual variations (i.e. variations not due to systematic group change) between the measurement occasions. Relative Rank Variance ranges from 0 to 1, with higher values representing greater individual heterogeneity; RV > 0.1 is considered evidence of heterogeneity. The 95% confidence intervals were calculated for the RV and RP. In this study, we consider two types of change: first, the differences between the intervention and control group; and second, the changes within each group from baseline to follow-up. Statistically significant differences between the intervention and control group are defined as group confidence intervals that do not overlap. Statistically significant change between baseline and follow-ups within each group are defined as confidence intervals that do not include zero.36,39
Results
Baseline characteristics of intervention and control group
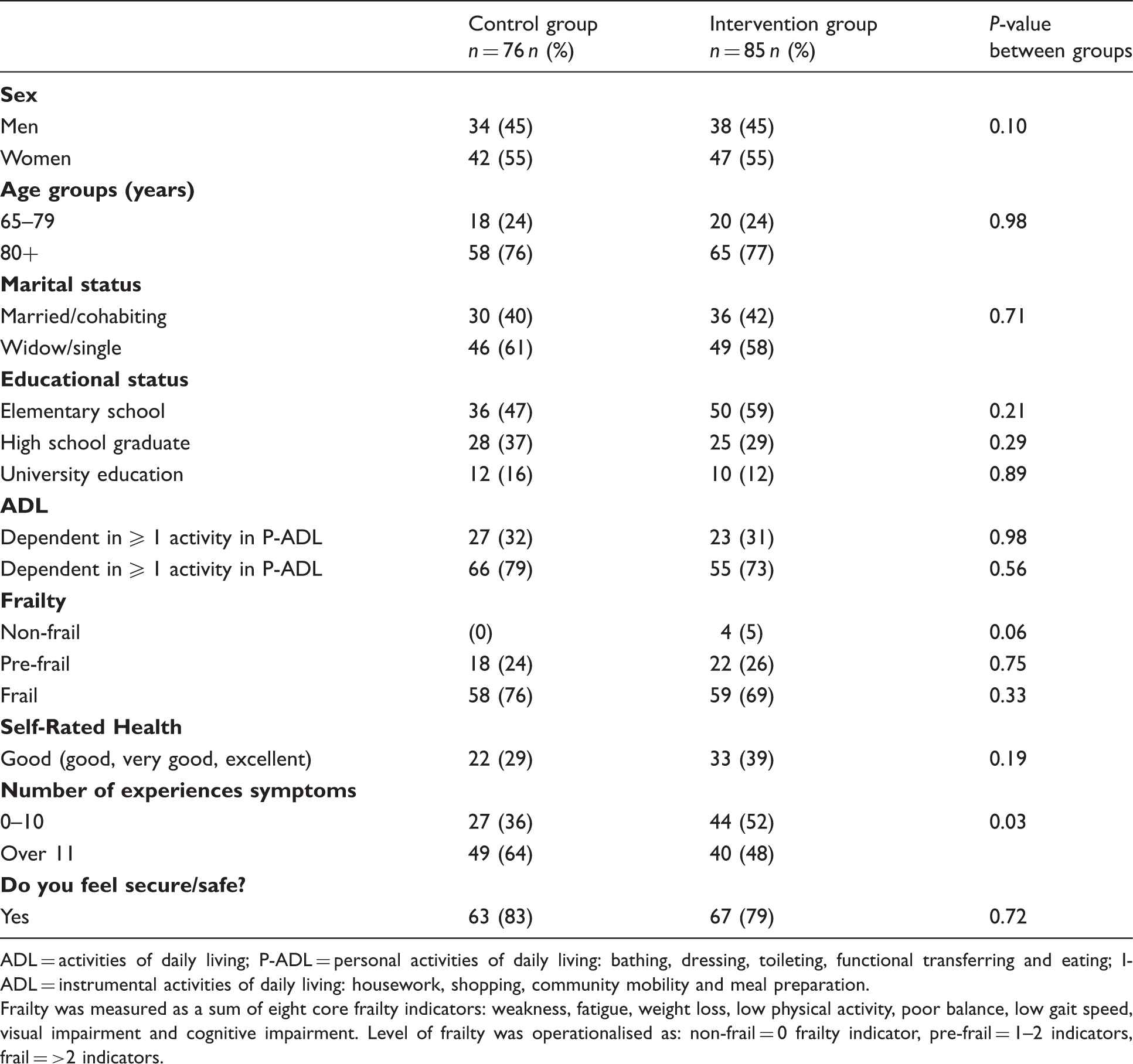
In total, 181 of 343 elders who sought care at the emergency ward were selected randomly for invitation to the study. Of these, 161 consented to participate (intervention = 85, control = 76). At 12 months, 17 and 18 people in the control and the intervention group, respectively, had been lost to follow-up (see Figure 1). Of the original 161 participants, 76% were at least 80 years old. The mean age of the sample was 82 years, with a range of 65–96 years. Just over half (55%) of participants were women. There were no significant differences between the intervention and control groups at baseline regarding sex, age, marital status, education status, ADL, frailty, self-rated health or experiences of security/safety. The most common symptoms in both groups were general fatigue, leg pain, dizziness, hearing loss and sleep disorders. There was a statistically significant difference in the number of symptoms (p = 0.033). See Table 2 for an overview of participants’ baseline characteristics.
Flow chart depicting the number of participants in the baseline and three-, six- and twelve-month follow-ups. Baseline characteristics of study participants, proportions and p-value for differences between groups. ADL = activities of daily living; P-ADL = personal activities of daily living: bathing, dressing, toileting, functional transferring and eating; I-ADL = instrumental activities of daily living: housework, shopping, community mobility and meal preparation. Frailty was measured as a sum of eight core frailty indicators: weakness, fatigue, weight loss, low physical activity, poor balance, low gait speed, visual impairment and cognitive impairment. Level of frailty was operationalised as: non-frail = 0 frailty indicator, pre-frail = 1–2 indicators, frail = >2 indicators.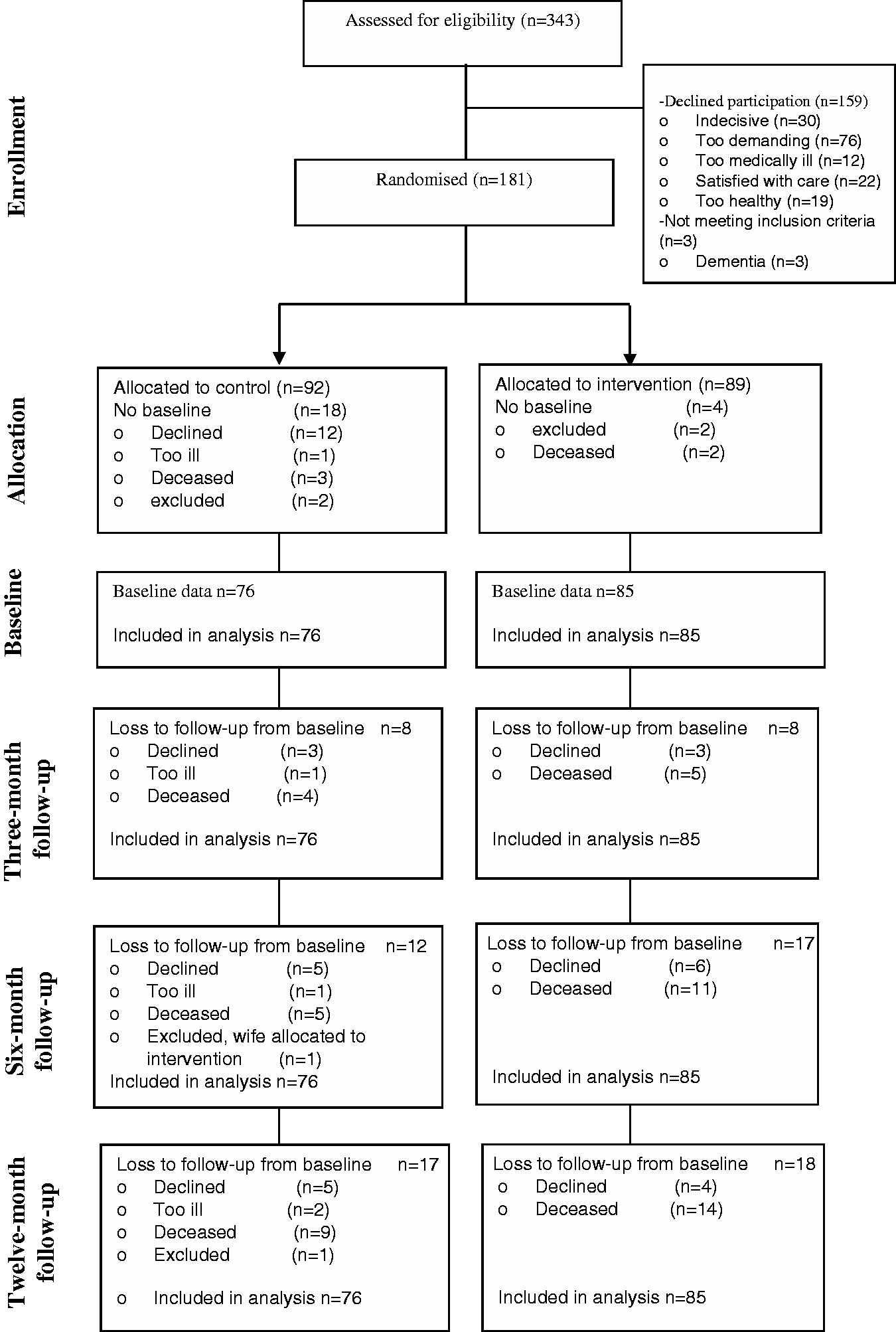
Differences in outcomes between intervention and control group
Self-rated health
There were group differences in elders’ self-rated health and in their ratings of the benefit of the intervention, but these were not statistically significant. The positive RP values at all follow-ups in the intervention group showed improvement, while RP in the control group at the three-month follow-up was negative, and at the six and 12-month follow-ups was positive but too close to zero to be significant.
Symptoms
The confidence intervals of RP for the groups did not overlap each other at the six-month follow-up, which indicates a statistically significant inter-group difference for systematic change in frail elders’ symptoms at the six-month follow-up. Relative Rank Variance values at all follow-ups were above 0.1 and also greater in the intervention group than in the control group, but the overall difference was not significant.
Experiences of security/safety
Inter-group differences for changes in the experience of security/safety were non-significant. However, in the intervention group the RP values were positive at all follow-ups, which indicates systematic improvement in experiences of security/safety, while the RPs of the control group were negative at three and six months. Relative position values of the two groups at the 12-month follow-up were the same.
Changes from baseline to follow-ups within each group
Self-rated health
A statistically significant improvement in self-rated health was observed within the intervention group. Relative Rank Variance values of the intervention group at all follow-ups were above 0.1, which indicates individual improvement in self-rated health in this group. Relative Rank Variance values only exceeded 0.1 at 12 months in the controls.
Symptoms
Variables measured from baseline to follow-ups.
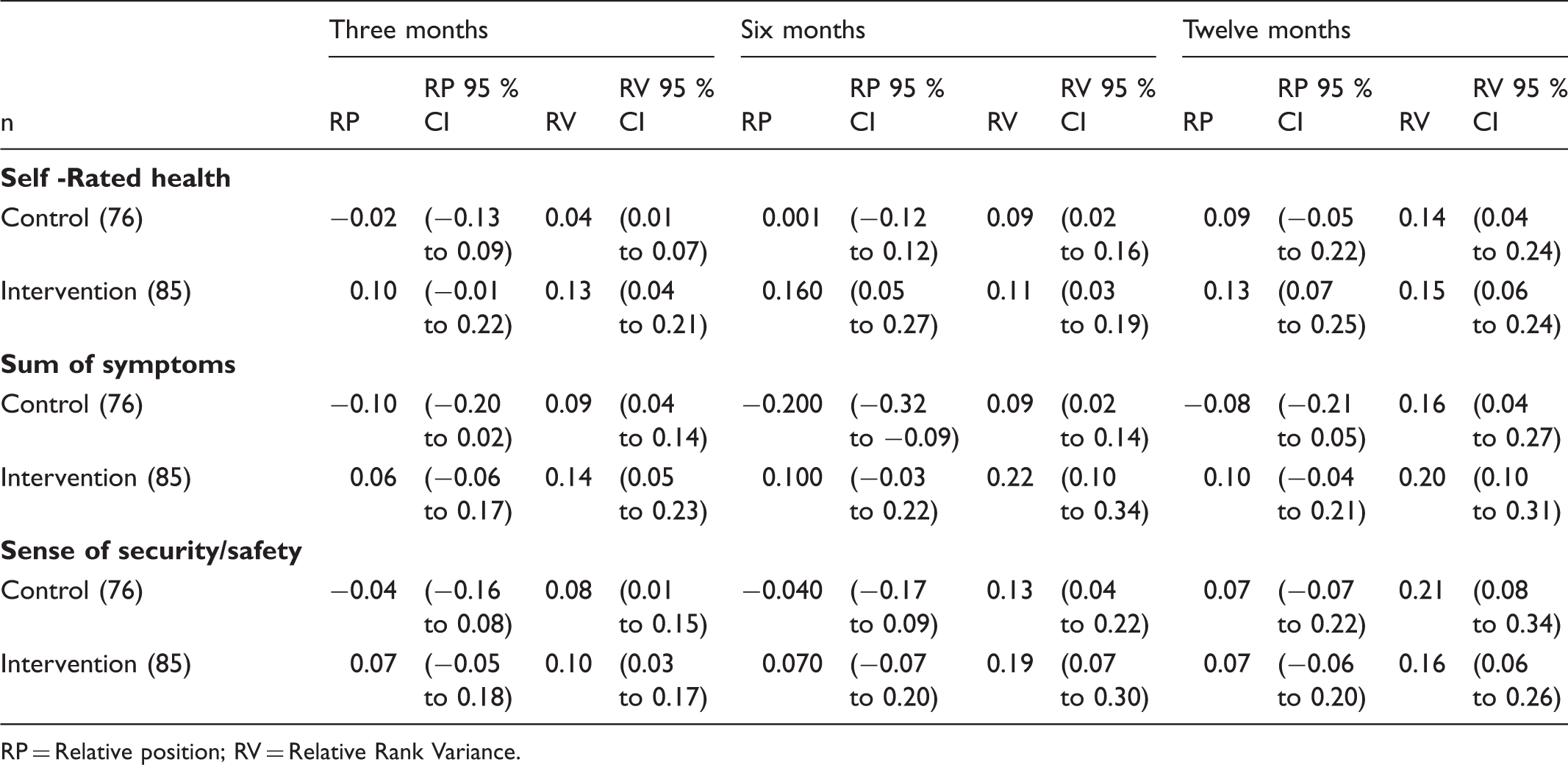
RP = Relative position; RV = Relative Rank Variance.
Experience of security/safety
The RV values of both groups at all follow-ups were above 0.1, with the single exception of the control group at the three-month follow-up. This suggests that the experience of security/safety improved within both groups.
Discussion
The purpose of this study was to evaluate effects of the CC intervention on self-rated health, experiences of security/safety and symptoms. The main finding was improvement in symptoms and self-rated health in the intervention group at the six-month follow-up. In addition, symptom improvement was observed in the intervention at all follow-ups, while deterioration of symptoms at all follow-ups was found for the control group. Further, elders in the intervention group improved in self-rated health, with positive effects reaching statistical significance at the 6 and 12-month follow-ups. The results also showed improvement in the control group’s experiences of security/safety, but this improvement was not statistically significant, nor was the inter-group difference significant. Regarding frail elders’ experiences of security/safety, no statistically significant inter-group differences were found. Instead, the results indicated that there was more individual variation than systematic change at the 6 and 12-month follow-ups in both groups.
The essential components of the intervention that may have had positive effects were, among others: conducting care planning meetings in the elder’s own home and the use of a comprehensive geriatric assessment, which enabled the elders’ participation and empowerment and also allowed caregivers to perceive the frail elders’ reality, resources and needs at a deeper level. Furthermore, the elders’ feeling of comfort at being in their homes facilitated a more equal balance of power between them and their caregivers. Access to a case manager (contact with one person over a long time) and the programme’s coordination of efforts, its continuous follow-ups, advising/problem-solving and visiting and telephone contacts are among other essential components of this intervention. The elders in the intervention group perceived that their knowledge about the care/service contact person had increased; this in turn may have enhanced the elders’ sense of security/safety.
This study showed statistically significant positive effects of the intervention on frail elders’ symptoms and self-rated health. Associations among self-rated health and subjective wellbeing and functional status have been proposed. 40 The results of the current study agree with previous studies that have shown effects of complex interventions for elders in improving relevant associated aspects of health and physical function, decreasing the risk of hospital admissions and falls 41 and increasing quality of life. 42 We found more individual variation in improvement of symptoms in the intervention group than in the control group. However, it is important to take into account that at baseline there was already a significant difference between the groups; i.e. the elders in the control group had more than 11 symptoms compared with elders in the intervention. Therefore, the results for symptoms must be interpreted with caution. However, using Svensson’s method showed the character of the changes in the respective groups at the individual and group levels. In the case of symptoms, the results showed improvement over time within the intervention group.
The intervention used a person-centred approach with shared decision-making and partnership throughout the care chain. The multi-professional team was responsible for individualised care planning, which was carried out with the involvement of the participants and their relatives. The process of this intervention facilitated construction of the elders’ narratives of their needs, problems, and resources in their life context. The planning of further care and rehabilitation was approached in a relationship of equals, in which the older adults and their relatives were involved and helped decide the care plan. The intervention, which started with a comprehensive geriatric assessment, involved the elders and their relatives in the planning of the healthcare and was delivered in the elders’ own homes, thereby providing the opportunity to initiate this relationship of equals. This approach was in line with the routines for ensuring implementation of person-centred care in daily clinical practice suggested by Ekman et al. 21 The results from our evaluation of this intervention emphasised the positive effects on many important factors in frail elders. These positive effects can be explained by the intervention’s integrated care design,3,7 its person-centred focus 43 and its complex, multi-level content. 44 Furthermore, our results emphasise that the experience of good health and balance in everyday life despite frailty is possible as we have shown previously, 16 for example, through implementation of a continuum of care with a person-centred approach. Frail elders experienced good health when they had a sense of assurance and capability in their everyday lives as we have also shown previously. This intervention is in line with a person-centred approach because it highlights the utilisation of the individual’s narratives, skills and knowledge side by side with the professionals’ skills and knowledge.
Another care planning programme with coordination of care services by a case manager has been shown to improve older adults’ subjective wellbeing, 45 which is consistent with our finding of a statistically significant improvement in frail elders’ self-rated health. A systematic review and meta-analysis has pointed out the importance of implementing complex interventions that aim to meet individuals’ needs and preferences, which can help elders experience safety and independence in their everyday lives. 41 The results from the current study are consistent with two newly published reviews, which show statistically significant positive effects of early coordination and interdisciplinary team rehabilitation for elders,46,47 the latter having documented effects of improved physical function and better performance of activities of daily living for elders after surgery for hip fracture. 46 Early coordinated discharge following an interdisciplinary rehabilitation in the homes of elders with moderate disability after stroke enhanced their activities of daily living and decreased mortality. 47 The current study reports statistically significant group effects favouring the CC intervention at the six-month follow-up; however, the effects are for the secondary outcomes of symptoms and self-rated health. Therefore, further studies are recommended to test the generated hypothesis about the positive effects of the intervention by a more specific person-centred approach on these outcomes as primary outcomes.
Complex interventions for older adults are more efficient in pre-frail individuals, i.e. those who are just beginning to develop frailty. 41 Consequently, two key issues that should be taken into account are that the participants in this study were frail elders and that deterioration in their health was expected. Therefore, the intervention can be considered successful if these frail elders maintain their pre-intervention experiences of health, security/safety and symptoms. The second issue is that the ordinary care services for elders in Sweden are among the best in the world.1,48 Therefore, even a slight improvement due to the intervention is remarkable and should be considered clinically significant.
In summary, this study tested the hypothesis that the integrated CC intervention would have the positive effect of maintaining frail elders’ self-rated health, feelings of security/safety and experience of symptoms. We found some support for this hypothesis; however, further studies are required for a complete understanding of the relationship between the CC intervention’s specific components and these critical outcomes.
Methodological considerations
The design of this study has several strengths. First it was a randomised controlled trial (RCT), which is the optimal study design to minimise bias and provide the most accurate evaluation of a complex intervention’s effects and benefits.49,50 Second, the fidelity of implementation of the CC intervention was investigated alongside the RCT study. 27 The target group was frail elders. The need for updating and developing knowledge of interventions, and of conducing RCT studies to evaluate the effects of continuum of care interventions, 51 in an integrated health and care system for frail elders with complex needs has been argued previously. 52 An additional strength of this study was that the instruments used were valid and adjusted for elders.
A limitation in the design of the intervention project was that the intervention began at the emergency department, and the baseline measurement was made after hospital discharge. It is arguable that collection of the baseline data should have been completed at the emergency department; however, there are ethical concerns related to exhausting older subjects with extensive questionnaires at the emergency department. 22 Nevertheless, our choice may have made it more difficult to detect actual differences between the groups; i.e. some effect of the intervention may already have occurred at baseline. Therefore, even the small observed differences should be considered important. Further, power calculations were based on the intervention’s primary outcome, so it could be argued that the secondary outcomes were less sensitive to detection of inter-group differences. Another possibility is that the study was underpowered for detecting significant differences. However, it is important to emphasise that the outcome measures of this study were secondary outcomes for the intervention; therefore, it is difficult to draw conclusions about the effects of the intervention. Additional studies are suggested to confirm the positive effects of the intervention on these outcomes.
The interviewers were not blinded to group assignment during the follow-ups. The participants revealed the allocated group assignment at follow-ups, and we assumed there would be less attrition if the older people could meet with the same interviewer at most of the follow-ups. The interviewers were doctoral students and research assistants who had university degrees and were well trained in assessing frail elders. In addition, study protocol meetings were held throughout the study period to ensure standardisation of the assessments, and this strengthened the validity of this study. 22
The dropouts were not random; they tended to be those who had experienced deterioration in health status or reduced functional ability, were too tired to continue, or who had died. The dropout rate was fairly low, considering the age and health status of the participants: 22% each in the control group and intervention group. 23 There were no significant differences in baseline characteristics between respondents who completed all follow-ups and those who dropped out with respect to sex, age or marital status, but as suggested previously, those who dropped out had poorer health status and a greater disease burden. 24 Therefore, the choice to impute MCD for missing data in those who declined to continue and to impute the worst value for those who had died seemed appropriate.32,53 The imputation method was based on the assumption that older adults (80+ years) are expected to deteriorate over time, an assumption that is consistent with other studies 53 and which was verified by poorer health status in the dropouts. In addition, the sensitivity analysis showed aligned trends when comparing with complete cases.
Practice implications and conclusion
This is a sub-study of a unique intervention and RCT study for frail elders. Elders who received the CC intervention were better able to improve or maintain their level of symptoms than were those who received ordinary care. The intervention, with its integrated continuity and collaboration within the healthcare system and between different caregivers, its focus on elders’ resources and needs in their own context, its provision of access to a case manager and its focus on multi-professional cooperation and exchange of information, continuous follow-ups and contact for problem solution over the long term can positively influence frail elders’ experience of health in their everyday lives. More research and intervention with integrated multi-professional healthcare is required, particularly with a person-centred approach that enables frail elders to experience good health and feelings of assurance and capability in everyday life by involving them and their relatives in the planning of healthcare. Intervention-based research on integrated multi-professional healthcare with a person-centred approach is a desirable step in the implementation of optimised care of frail elders.
Footnotes
Funding
The authors disclosed receipt of following financial support for the research and/or authorship of this article: Vårdalinstitutet, The Swedish Institute for Health Sciences.
Conflict of interest
The authors declare that there is no conflict of interest.