
Abstract
To respond to the needs of home healthcare (HHC) patients, HHC professionals must use strategies to navigate the influence of the institutional context, that is, laws and regulations, the administration, and the organization of HHC services. However, no synthesis of those strategies exists. This review aimed to synthesize the strategies used by HHC professionals working with older adults to navigate the institutional context. An integrative review was undertaken in 5 databases, from 2011 to January 2023. The quality of documents was assessed based on an adapted version of the Critical Review Form—Qualitative Studies (Version 2.0) in which a score was calculated out of 25, and data was analyzed through coding, data display and comparison. Thirteen documents were included. The quality of studies ranged from 13 to 21.75. Strategies are often used to overcome limited resources (e.g., time, funding). Six types of strategies were identified: Deviating (bypassing rules or processes), taking on more and more (taking additional work), offering one’s personal time (working without remuneration), reallocating resources (splitting HHC services between patients), limiting HHC visits (restricting interventions or actions) and relying on others (transferring responsibilities). The use of strategies could alleviate the discomfort felt by HHC professionals due to limited resources. However, as some strategies lead to a reduced scope of practice and to a loss of expertise, this could impede the quality of the care, resulting in non-responded needs for HHC patients.
Keywords
Introduction
Home health care (HHC) enables older adults to age in place, which is the preferred option for most of them.1 -3 To that end, HHC relies, among other things, on the work provided by health and social service professionals. These professionals are highly skilled workers who, through their tasks and duties, provide interventions based on extensive knowledge of health. 4 They typically consist of nurses, social workers, occupational therapists and physiotherapists.5,6 To intervene with HHC patients, HHC professionals rely on their professional practice, that is, a combination of knowledge and actions which are patient-centered and authentic, as well as a process to transform a situation from one specific state to another. 7 The practice is context-dependent, meaning the context in which HHC professionals work influences their practices.7 -11
The institutional context, which includes laws and regulations, the administration, and the organization of HHC systems 12 is a key factor that shapes professional practice. There are numerous instances of the institutional context having an influence on the practice of HHC professionals. For example, studies suggest that changes in laws (laws and regulations) can influence the interventions provided by HHC professionals, 13 as well as increase the number of HHC visits done. 13 Additionally, standardized referral forms (administration) can reduce the scope of practice, 14 as well as its patient centeredness. 15 To overcome the negative influence of the institutional context, HHC professionals seem to use strategies, that is, a plan to achieve a specific goal when the conditions are uncertain. 16 For example, when work is standardized with a list of tasks or predefined time for each task (administration), HHC professionals can “juggle” minutes between 2 HHC visits for patients 17 or negotiate with their supervisors for more time to complete their tasks. 18 When time is limited (administration), HHC professionals may opt to refrain from formalizing all their activities during a HHC visit. 19 Finally, when the HHC workforce is being reorganized (organization), HHC professionals may rearrange their schedules to ensure high quality of their practice. 20
Despite the numerous reviews that have been conducted regarding HHC, including those focused on interventions,21 -24 cost reduction and improved outcomes, 25 work experiences, 26 HHC models, 21 and health promotion practices, 24 there has yet to be a comprehensive synthesis of the strategies used by HHC professionals working with older adults to navigate the institutional context.
Summarizing the strategies used by HHC professionals working with older adults to navigate the institutional context could allow HHC managers to understand the effect of the context on the professionals’ actions. Thus, managers could anticipate potential consequences of changes in the institutional context on professional practices. Additionally, professionals report that HHC does not have sufficient resources (e.g., money, time) to respond to older adults’ needs in many eastern countries, including but not limited to Iceland, Norway, the United States of America, Canada, Sweden and Finland.17,27 -33 Thus, providing an overview of these strategies could support professional training by raising awareness about the consequences of using them.
Consequently, this review aims to synthesize the strategies HHC professionals use to navigate the institutional context when providing HHC to older adults.
Methods
An integrative review was conducted. 34 Integrative reviews summarize the scientific literature to provide a comprehensive understanding of a particular phenomenon or healthcare problem. 35 Whittemore and Knafl’s 34 five steps were used: Problem identification, literature search, data evaluation, data analysis and presentation.
Problem Identification
In this review, the “problem” was identified as the strategies HHC professionals working with older adults put into place to navigate the institutional context. As such, the main concepts were professional practice, HHC, older adults and institutional context.
Literature Search
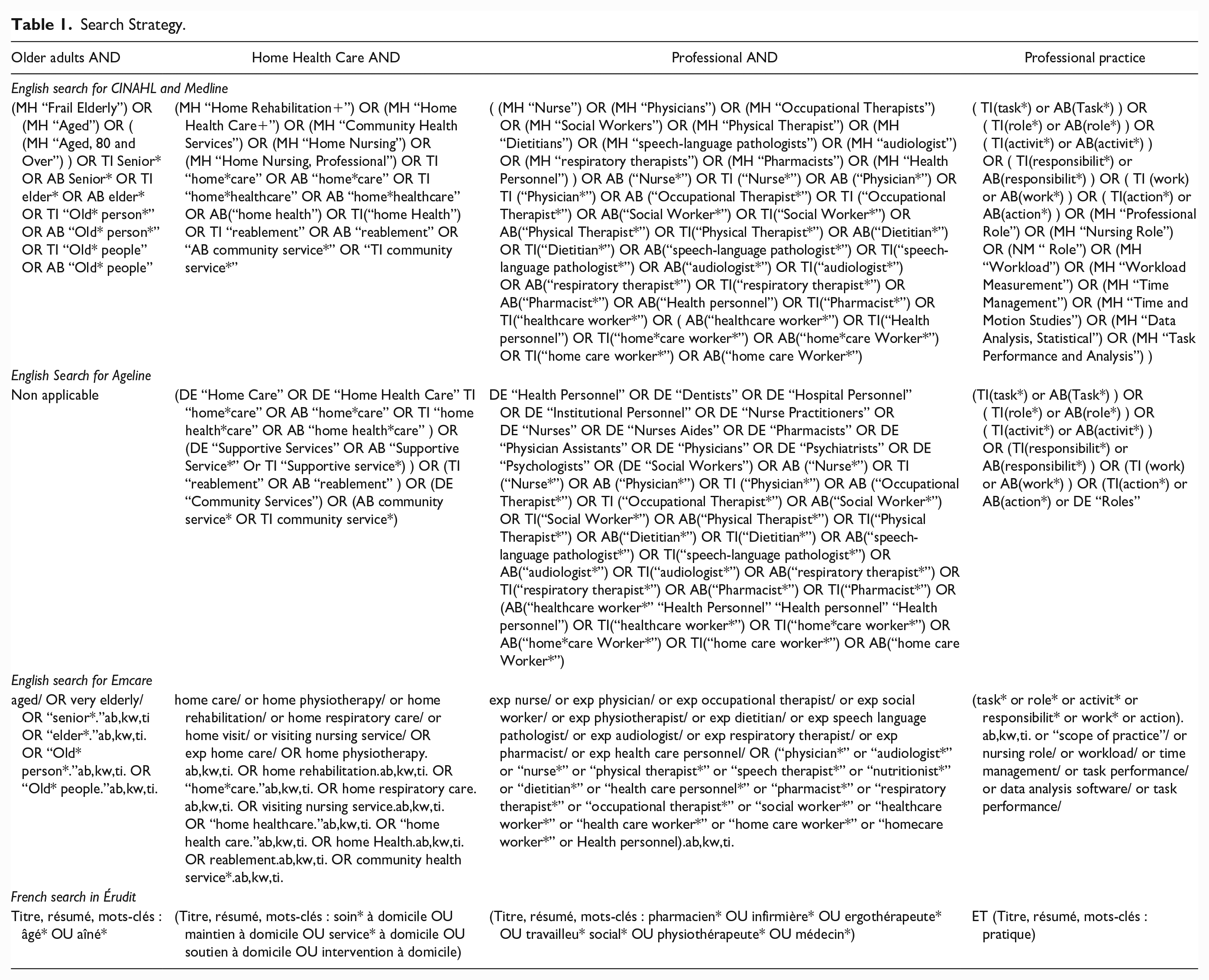
As suggested by Whittemore and Knafl, 34 the search strategy relied on different methods. The Emcare, CINAHL, Medline, Érudit and Ageline databases were searched. With the assistance of an experienced information scientist in aging, it was determined that the search terms would be inclusive in nature, encompassing a wide range of subjects related to HHC professional practice to minimize the risk of missing relevant documents. Thus, the search strategy included Mesh terms and key words related to HHC, professional practice, and older adults (Table 1). Additional documents were identified using 3 other strategies. First, the following journals were manually searched: Home Health Care Management & Practice, Journal of Gerontological Social Work and Home Health Care Services Quarterly. Second, the reference lists of the included documents were manually scanned to identify further references. Third, documents independently identified by co-authors were added to the review. This included documents such as master’s and doctoral theses, books, as well as research articles.
Search Strategy.
Included documents were written in French or English, published between 2011 and January 2023, and focused on the institutional context and professional practice in HHC for older adults, from the professionals’ perspective. This timeframe is of similar length to those of previous reviews in HHC.26,36 -38 It was also selected to reflect the recent state of HHC professional practice. Indeed, in many eastern and western countries, HHC have undergone major reforms in the past 10 years39 -41 and the profiles of HHC patients have changed.42,43 Beside these criteria, when applicable, documents needed to be written in a way that made it possible to extract the HHC professionals’ perspective from that of other, non-professional HHC workers, that is workers providing support and assistance with activities of daily living and routine personal care. 4 Also, elements of the institutional context had to be laws and regulations, the administration or the organization of work related to HHC services. 12 Finally, HHC services had to be provided to older adults. In line with integrative reviews, documents could be peer-reviewed or gray literature. Documents were excluded if they were about HHC in the context of palliative and end-of-life care, as the practices tend to focus on pain management,44,45 which are different practices than those in HHC, focusing on autonomy, satisfaction, and health. 21 Additionally, documents were excluded when they pertained to specific domains (e.g., foot care), because they focused on specific actions and thus, did not allow to have a comprehensive view of the HHC professional practice, which encompasses several domains. 46
To determine the full text inclusion and exclusion process, all authors read the first 30 titles and abstracts of the documents. All authors individually evaluated each document to determine if it was clearly ineligible or should be kept for full-text reading. An agreement of 80% had to be reached, which represented 24 documents out of 30. All authors discussed the remaining 6 documents until consensus and guidelines were established for the first author to continue the eligibility assessment process. Then, from all the eligible documents, all authors read the full text of 5 documents along with a research assistant (RA) experienced in HHC professional practice. When applicable, all authors and RA completed an extraction grid. All authors and RA then discussed the extraction grid and what should be extracted, and the first author continued the full text inclusion or exclusion process alone.
Data Evaluation
As all of the included studies were qualitative, an adapted version of the Critical Review Form - Qualitative Studies (Version 2.0) 47 was employed to assess their quality. This form generated a quality score out of 25. The first author and the RA independently assessed each document.
Data Extraction and Analysis
The first author and the RA conducted data extraction and analysis. They co-extracted relevant information for 13 documents in Microsoft Word by asking “Does this aspect of the institutional context seem to have any repercussion on HHC professional practice?” and, if so, “What is the repercussion?” For the repercussion, the first author and RA paid attention to whether the repercussion was an action (or lack thereof). If so, data was extracted.
The first step of the data analysis is to reduce the data. Thus, after extraction, the first author and RA coded the data independently and discussed discrepancies between codes until a consensus was reached. Coding consisted of putting a small description of what the data was about regarding the institutional context and practice. To do so, the first author and RA asked themselves “What is this institutional aspect?” and “What actions (or lack thereof) do HHC professionals put forth in relation to this institutional aspect?”
The second step of data analysis involved displaying the data in a matrix to obtain a broader view. As such, the first author and RA identified similar actions used by HHC professionals through codes and grouped them together.
The third step of the data analysis aimed to identify similar actions taken by HHC professionals. The first author and RA examined the grouped codes to identify patterns within similar actions used by HHC professionals. The questions “What is this action?”, “How is this action similar to the other ones here?” and “Could this action be considered as a strategy?” were used to guide the analysis.
The final step of the data analysis is drawing and verifying conclusions. The first author and RA wrote a summary of the strategies used by HHC professionals working with older adults to navigate the institutional context. To verify the conclusions, the first author consulted the primary sources (the documents) again to maintain accuracy and confirmability of the findings and the second and third authors validated the results by asking for clarifications and exploring potential rival explanations for the strategies.
Results
Characteristics of Documents
This review included 13 documents (Figure 1). Only one document by Perron 40 specifically addressed HHC professionals’ strategies. Others mostly studied the aspects of professional practice in HHC. Data collection methods were observations paired with interviews (n = 4), focus groups (n = 5) or interviews only (n = 4). Finally, 3 studies reported attaining data saturation or redundancy. Other contextual information about included documents are available in Table 2.
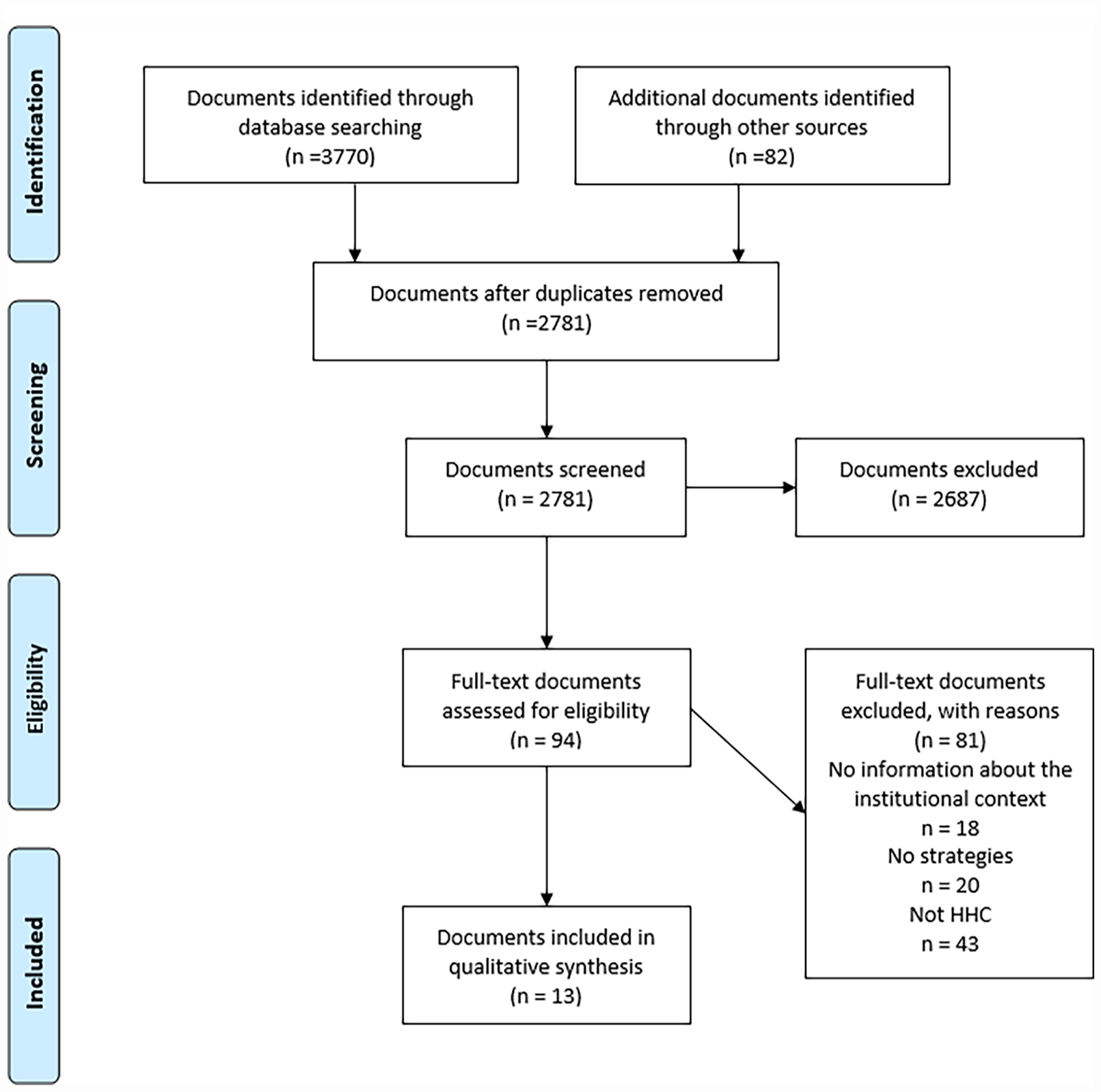
Prisma flowchart.
Contextual Information About Included Documents.
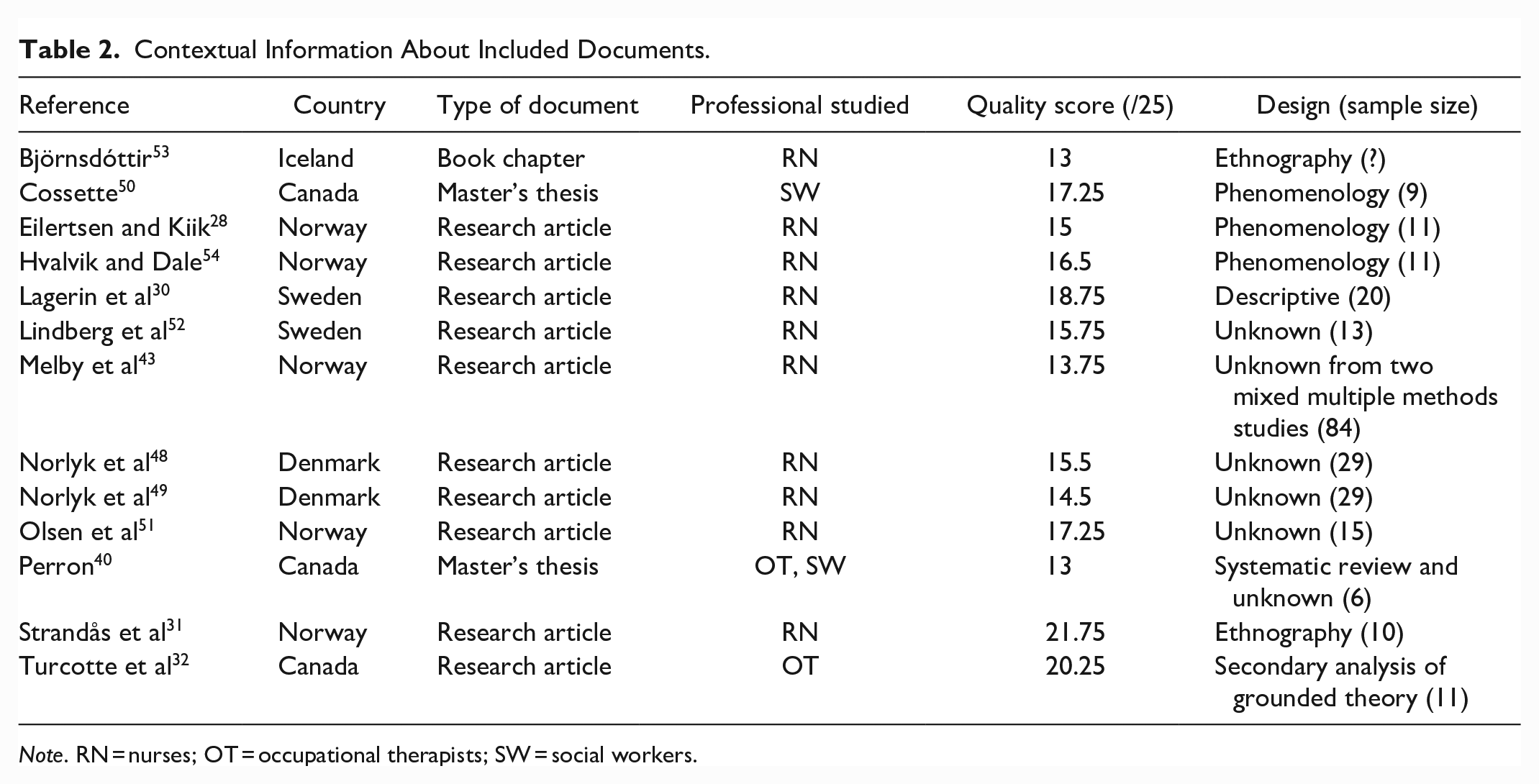
Note. RN = nurses; OT = occupational therapists; SW = social workers.
Strategies Used by HHC Professionals Working With Older Adults to Navigate the Institutional Context
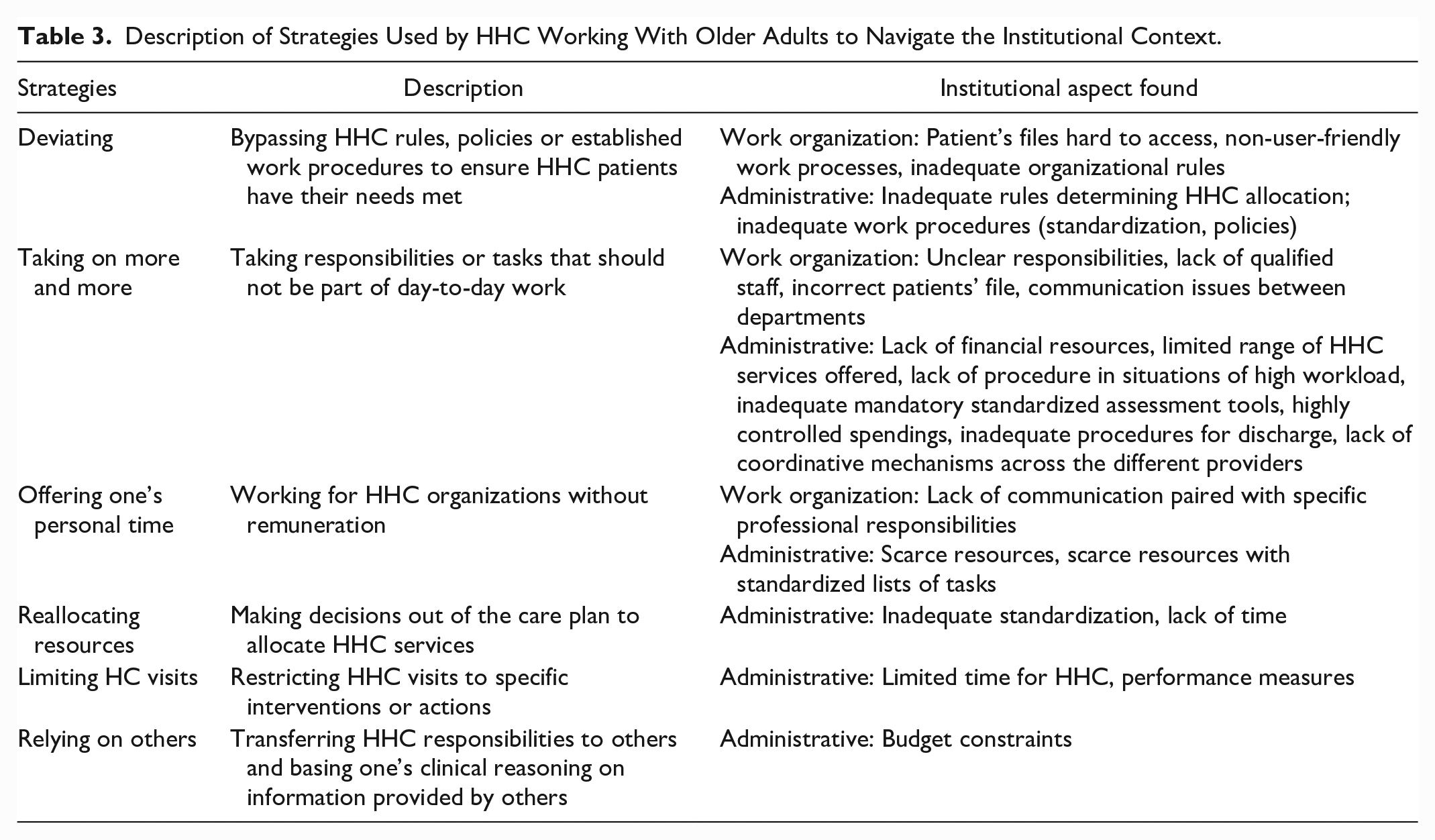
Six types of strategies were found. The most recurrent institutional aspects were as follow: Five strategies were related to administrative resources (time, money), 3 were related to standardization of the work, and 2 were related to inadequate work processes, access to the patients’ file and communication. Strategies and the institutional aspects are presented in Table 3 and described in more detail, below.
Description of Strategies Used by HHC Working With Older Adults to Navigate the Institutional Context.
Deviating
HHC professionals bypass established ways to do their work to meet the needs of HHC patients. This can occur when access to the HHC patient’s file is difficult 48 or when work processes prevent them from providing the best care or services for the HHC patients. 49 Some examples of deviating include reinterpreting HHC service allocation rules when the number of hours that can be allocated to HHC patients is standardized. 40 When work is highly standardized with a designated time for each task, HHC professionals may not document everything that was done during the visit or may tamper with work tools: “The most widespread way of gaming the system is manipulating the timers to show them using the exact amount of time that is assigned” (p. 10). 17 Overstepping the general practitioners’ authority is another way of deviating, which happens when organizational rules are inadequate. 49 Additionally, seeking support from political stakeholders outside the HHC organization, instead of the organization’s quality and complaints department, may also be considered a deviation when the solution deemed best for the HHC patient is not in line with organizational policies. 50
Taking on more and more
HHC professionals take on additional responsibilities or tasks that fall outside of their typical work duties. Additional tasks include dividing the completion of a mandatory standardized assessment in 2 HHC visits to reduce patients’ fatigue, 40 negotiating additional home support services with managers because spendings are highly controlled, 40 taking additional steps to correct mistakes and ensure the patient’s file has the right information, 51 and training other HHC workers on what information they need to look for.48,52 Another study also reported that following HHC municipalization, HHC professionals make additional phone calls when procedures for specific illnesses are not clearly defined. 43
Taking on additional responsibilities can happen for 7 reasons: (1) Responsibilities for each organization involved in HHC are not well defined.49,53 (2) HHC organizations lack qualified health and social service workers49,51,52,54 that can share relevant information about the patients.51,54 (3) Financial resources from the HHC organization are lacking. 40 (4) The range of HHC services is limited to specific interventions. 40 (5) The absence of clear procedures for prioritizing the workload can lead HHC professionals to take on responsibilities beyond their role. 52 (6) A lack of pre-discharge meeting between HHC professionals and patients. 48 (7) There is a lack of coordinative mechanisms across different providers. 43
Offering one’s personal time
In some situations, HHC professionals work without compensation: “To fulfill all their professional responsibilities, they sometimes stayed after work or made extra visits to check on a patient they knew would not contact them” (p. 575). 52 For example, they use their own personal time to care for HHC patients 40 and work during their breaks or after their work day has ended.17,52 Offering one’s personal time was found in 3 situations: (1) When resources are limited. 40 (2) When HHC professionals’ work is organized with lists of tasks and corresponding completion time, and they cannot meet these standards nor request overtime. 17 (3) When communication is inadequate between healthcare organizations and HHC professionals are responsible for the safety of HHC patients. 52
Reallocating HHC resources
HHC professionals sometimes “juggle” the assigned time between HHC patients to ensure that a greater number of them will have their needs met. For example, they may reduce home support services for one patient to allocate them to another one .17,40 On the days they have more available time, HHC professionals will also make up for past limitations by performing tasks that are not required or that the HHC patients are not entitled to, such as training with the patient. 28 This strategy is driven by inadequate standardization 17 and time pressure28,40: “The informants expressed feelings of inadequacy when they experienced time pressure. Several informants explained that they would compensate on the days that they had more time and perform tasks that were not mandatory or to which the patients were not entitled.” (p. 84). 28
Limiting HHC visits
HHC professionals might have to limit their practice to specific actions or interventions. This can involve not providing health prevention and promotion interventions, 32 avoiding 17 or limiting communication with HHC patients: “Instead they had to interrupt the older person and end the visit or stay longer than they should have.” (p. 474). 30 Time constraints17,30,32 lead HHC professionals to prioritize interventions they consider as essential.17,32 Furthermore, when their work is measured and evaluated, HHC professionals tend to focus more on performance-based tasks. 40
Relying on others
HHC professionals often need to transfer their responsibilities to community, for-profit and other HHC organizations when the number of home support services that HHC professionals can allocate to patients is limited, due to budget constraints: “[. . .] [HHC professionals] decision to redirect their patients to the community sector appears to us as a way to help them that is part of a long-term solution given the persistence of this situation [lack of budget].” (p. 87, free translation). 40
Discussion
In this integrative review based on 13 documents of various quality, 6 types of strategies used by HHC professionals working with older adults to navigate the institutional context were identified. The results will be discussed in 2 perspectives: (1) The methodological characteristics of included documents and (2) The rationale and consequences underlying the use of strategies.
Methodological Characteristics of Included Documents
Studies about professional practice using qualitative designs or data collection methods have allowed for the indirect documentation of strategies used by HHC professionals working with older adults to navigate the institutional context. Ethnography and phenomenology were the most common designs. Ethnographic designs are interested in the culture sharing of a group (here, HHC professionals). Phenomenological designs are interested in the common meaning of a shared experience (here, the HHC practice). 55 Thus, they are relevant to study HHC professional practice.
The data collected in the studies documenting professional practice in HHC were mostly gathered through observations, interviews, and focus groups. Because observations allow identifying what HHC do, they are valuable to pinpoint the strategies used by HHC in their context. In the included studies, observations were always paired with interviews. Interviews alone allow access to the observers’ perceptions. 56 Paired with observations, both methods provide the opportunity for researchers to further question on specific topics, and to ask for explanations and clarifications about observed events. 17 As with interviews, focus groups are useful because they allow accessing participants’ perceptions. Additionally, participants can hear what others have to say and adjust their statements, accordingly. 56 However, both interviews and focus groups can create possible omissions or post hoc rationalization 57 and social desirability 56 when professional practice is being studied. Consequently, to identify strategies used in relation to the institutional context, it seems necessary to triangulate observations with different data collection methods to ensure the credibility of the findings.
Rationale Underlying Strategies and Their Consequences
Documents included in this review were exclusively from western countries. Despite the fact that HHC does not share a common model (e.g., aims, basket of services), 21 these countries have implemented similar means to measure HHC delivery (e.g., performance indicators, quality assessments).12,58 -60 Thus, turning to strategies could reduce the discomfort of HHC professionals regarding the institutional context, especially those related to time pressures and performance indicators.40,58,61 -67 Performance indicators are measures of practice performance.68,69 In HHC, performance indicators often revolve around the number of visits made by professionals.40,70,71 They can be used to increase or assess the efficiency of HHC services12,58,59,62 or to control spending. 12 However, when organizations set performance indicators, they do not necessarily consider the quality of those visits 40 or their alignment with the HHC context.70,71 As the needs of HHC patients become more complex,19,27,30,32,43 it may be challenging for professionals to meet these performance indicators. Thus, the misalignment between organizational expectations (e.g., number of visits) and professional requirements (e.g., quality of care), could impact HHC professionals’ mental health, leading to a loss of meaning in their work. 72 Consequently, to provide significant service to HHC patients, professionals might use strategies 73 which could contribute to maintaining their health and well-being. 72
While strategies can help reduce discomfort for HHC professionals, their use can also have unintended negative consequences. The strategy of limiting HHC visits will be taken as an example to illustrate these consequences. Limiting HHC visits was operationalized as limiting home visits and restraining 30 or avoiding 17 communicating with HHC patients. This strategy seems to be frequently used by professionals 74 to address performance indicators 40 and lack of time for visits.17,30,32
The consequences of restricting HHC interventions to medical-centered interventions in response to the institutional context cannot be ignored. While some interventions may be shifted to non-professional workers, studies suggest that interventions shifted to non-professional HHC workers are predominantly focused on medical aspects.75 -79 The lack of a shift toward non-professional workers in HHC is concerning, as several studies indicate that professional practices within HHC have deviated from their original forms. For instance, social work, which was initially aimed at empowering vulnerable individuals, 5 has shifted to a more medically centered approach within HHC.63,80 -82 Social workers in HHC report focusing on discussing medication compliance and access to medical equipment, instead of providing social support, 83 thus doing very little social work.83,84 A similar pattern is observed for nurses and occupational therapists. Indeed, nursing encompasses autonomous and collaborative care of individuals by promoting health, preventing illness, and caring for people with illnesses and disabilities. 85 However, studies report that nurses in HHC tend to do nursing actions that are medically centered,86,87 with an increased need for medical follow-up in opposition to everyday-life care.88,89 Likewise, occupational therapists are concerned with what people do with their time that is fundamental to their health and well-being (occupations) 90 but rarely intervene in health prevention, promotion, social participation, and communication within HHC.32,91,92 They seem to spend most of their time on assistive devices,93,94 bodily functions, walking indoors, self-care and domestic life.91,95,96
Such a shift in the scope of practice can have significant implications for how the profession is perceived and may result in a loss of expertise. 97 This loss could then decrease the quality of HHC services, potentially putting patients at risk. Consequently, as HHC regulated by professional boards, professionals could be at risk of disciplinary sanctions. Additionally, with loss of expertise, some of the HHC patients’ needs will be left unanswered if no leadership is taken to protect those non-medical interventions, within the practice. Thus, in the long term, strategies seem to have negative outcomes for both the HHC professionals’ respective professions and for patients.
Strengths and Limitations
Despite the varying quality of the documents included in this review, all relevant studies were included, regardless of their low quality score, as done by Delgado et al. 98 However, it is important to note that most of the studies in this review were conducted in western countries and used qualitative methods only. Thus, this review cannot accurately reflect the prevalence or frequency of the use of certain strategies and establish a clear causal relationship between elements of the institutional context (such as lack of time) and the use of a particular strategy (such as limiting home care visits). Nevertheless, this review provides valuable insights and information to HHC professionals, stakeholders, and researchers on the strategies used by those professionals working with older adults, to navigate the institutional context.
Implication for Practice, Policies, and Research
At the practice level, HHC professionals should be aware of the potential consequences of using strategies in their respective institutional context, both at an individual (patients) and professional level. Limited resources, such as time and funding, are often cited as reasons for HHC professionals to resort to strategies. These are closely tied to performance indicators. As such, HHC professionals should be involved in defining what should be a representative performance indicator. Additionally, policies should be in place to guide HHC professionals in contexts with limited resources and to mitigate the adverse effects on their job satisfaction and well-being. Future research should focus on directly observing and documenting the strategies that HHC professionals use to navigate the institutional context through triangulated data sources when working with older adults.
Conclusion
The institutional context, that is the laws and regulations, administration, and organization of HHC services, can influence professional practice in HHC, making it necessary for HHC professionals to implement strategies to meet their patients’ needs. This integrative review synthesizes the strategies used by HHC professionals working with older adults to navigate the institutional context. Findings show that strategies used in HHC by professionals are rarely directly documented, and the quality of included documents is highly variable. From currently available research, the 6 types of identified strategies are: deviating, taking on more and more, offering one’s personal time, reallocating resources, limiting HC visits, and relying on others. Strategies often arise due to limited resources, such as time and money, and are necessary for HHC professionals to face the discomfort caused by the institutional context. However, the necessity to use some strategies such as those restricting the scope of practice can lead to HHC patients with unmet needs. This can also have detrimental consequences for the profession, especially when the strategies turn to favor “medically centered” actions. As such, HHC professionals should be involved in defining performance indicators that are relevant to HHC and be accompanied when resources become scarce to ensure their well-being at work.
Footnotes
Acknowledgements
The authors wish to thank Ms. Louise Tremblay for her valuable contribution to the analysis of this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fonds de recherche du Québec – Santé (FRQS) (#296650, #296437), and the Canadian Institutes of Health Research (#476590-71729).