
Abstract
Knowledge about care providers’ experiences of working in residential care of older people during times of downsizing and reorganisation is scarce, and it is not known whether/how their conscience is influenced by such changes. The aim was to describe care providers’ experiences of working in private residential care for older people during downsizing and reorganisation, focusing on troubled conscience. This study adopted a qualitative descriptive design based on interviews with seven care providers. A qualitative content analysis was used. The overall understanding was revealed as perceiving oneself as pinioned in between current circumstances to provide care and what one’s conscience conveyed. Care providers perceived: deteriorating working conditions as exhausting, downsizing and reorganisation as triggering one’s conscience when collaborating, troubled conscience when downsizing and reorganisation decrease the quality of care, and good management as crucial during downsizing and reorganisation. The results highlight that adequate communication strategies, well-functioning leadership and opportunities to know together and share what one’s conscience tells are aspects that need consideration.
Keywords
Introduction
People are living longer and healthier lives worldwide, partly due to improvements in healthcare, 1 and ageing populations are increasing in almost every country in the world. 2 Although this development is positive, it is also exposing societies to several major social and economic challenges, 2 and the need for a well-functioning organisation for care of older people seems urgent. Organisations all over the world are undergoing rapid, and often wide-ranging, changes which can become critical for those employed in the care of older people. 3 For example, studies have shown relationships between downsizing and/or reorganisation and burnout4,5 and burnout has been found to be positively associated with stress of conscience (i.e. stress from a troubled conscience). 6 The current study concerns care providers’ experiences of working in private non-profit residential care of older people (RCOP) in times of downsizing and reorganisation.
Background
In Sweden, as well as in many other countries (for example France and the UK)7,8 organisations for care of older people have been subjected to extensive changes over recent decades. 9 For example, during the 1990s there was a decrease in permanently employed healthcare personnel, in the number of beds in the healthcare system for older people and in financial resources. 10 In addition, between 2000 and 2012 the number of beds in RCOP decreased by approximately 29,500, which represents approximately a quarter of all beds. 11 Since the 1990s several Western countries have been selling off public services to private entrepreneurs, as a result of the reform movement known as New Public Management (NPM) gaining considerable influence over organisational concerns in welfare sectors in industrialised countries during the 1980s.cf.12 In the past two decades there has been a reorganisation of RCOP in the Scandinavian countries towards marketisation, pushed ahead by the NPM reform movement. One consequence of this reorganisation is that the proportion of beds in private RCOP in Sweden increased from 5% in 1993 to 21% in 2012. 13
Downsizing and reorganisation can have severe effects on employees within organisations and there is a lack of knowledge about care providers’ experiences of working in RCOP during these periods. Results from an interview study showed that, despite dealing with a changed working environment during organisational changes, care providers in RCOP are struggling to do their best – for example, by keeping residents’ needs in focus. 3 Quantitative studies conducted in various types of hospital setting have shown associations between downsizing/reorganisation and lower levels of job satisfaction,5,14 higher levels of distress and sick leave 14 and lower levels of work engagement. 5 Downsizing and reorganisation in hospital settings have also been found to be associated with increased intent to quit 5 and higher levels of burnout.4,5 Studies that have investigated care providers’ experiences of working in private RCOP during times of downsizing and reorganisation are lacking. However, there are some quantitative studies available that have investigated some aspects that may influence care providers’ work situations depending on the mode of operation. For example, it is known that a higher proportion (45%) of care providers working in private RCOP in Sweden are working part time because they have not obtained full-time work, which is 11% more than in public RCOP. Care providers working in private RCOP also have lower salaries compared to those working in public RCOP. 15 Other results have shown that there are no significant differences regarding perceived control among care providers depending on form of ownership in RCOP but employees in cooperatives report more participation than employees working in public and private RCOP. 16 Qualitative studies in private RCOP are scarce and it seems essential to further understand care providers’ experiences of working in private non-profit RCOP during times of downsizing and reorganisation as this area is understudied.
Further, studies have shown that even during times not characterised by downsizing and reorganisation, there are a lot of demanding issues that affect the healthcare personnel working in RCOP.17,18 Such issues include, for example, feelings of inadequacy and powerlessness, 19 experience of insufficiency, 20 time shortage and exhaustion 21 and troubled conscience. 22 Conscience has been described as, ‘an agent’s mode of consciousness and awareness of his or her own acts and their value or disvalue, their goodness or badness, their rightness or wrongness. It is often retrospective’.23(p.403) Demanding issues described in interviews as situations generating troubled conscience among healthcare personnel include: being caught between people’s various demands, being torn away from residents to do other work tasks, feeling unable to relieve residents’ suffering, and providing care that is perceived as wrong. 22 Results have shown that healthcare personnel working in RCOP self-rate the highest levels of stress of conscience as coming from lack of time to provide the care the residents need, being forced to provide care that feels wrong, having to deal with incompatible demands, and perceiving work in healthcare as being so demanding that one does not have the energy to devote oneself sufficiently to family. 6 Studies in care of older people have also shown that care providers with higher levels of stress of conscience report more health complaints 24 and also that there are positive associations between burnout and stress of conscience. 6 Stress of conscience has been found to be negatively associated with quality of care. 25 Furthermore, results indicate that levels of stress of conscience in healthcare personnel working in similar settings may have increased over time, as a recent study 6 showed markedly higher figures compared to figures reported in 2003. 17 There are, in fact, many demanding issues that affect those working in RCOP and, reasonably, such issues may be exacerbated in times of downsizing and reorganisation.
In summary, there is a lack of knowledge about care providers’ experiences of downsizing and reorganisation while working in private non-profit RCOP. No studies could be found that have explored how downsizing and reorganisation may influence their consciences. As troubled conscience among care providers may jeopardise their wellbeing and negatively affect the daily care of residents, it seems important to acquire a deeper understanding of their experiences of how/whether downsizing and reorganisation affect their conscience.
Aim
To describe care providers’ experiences of working in private non-profit residential care for older people during downsizing and reorganisation, focusing on troubled conscience.
Method
This study was part of a larger study aiming to explore troubled conscience in municipal and private care of older people.22,26 At the time the study started, by coincidence, the care unit under study underwent several changes, primarily financial, resulting in downsizing and reorganisation.
Participants
Participants were recruited from a private non-profit organisation for care of older people in an urban setting in Sweden, incorporating several care units. There were four specialist care units with 108 beds for people with dementia disease and the participants in this study were recruited from one of these. At this care unit, ten out of a total of 21 members of staff were made redundant and replaced with care providers who had worked for a longer time within the organisation. During the same period, six different ward managers worked at the unit before one was permanently appointed. A position as team leader was also introduced and the staff had to go from full-time to part-time employment (80%). Overlaps between morning and afternoon shifts were removed and the staff had to rely on data reports only. The removal of verbal reports meant less time for discussions about care. All care providers working daytime/evenings (n = 15) at the care unit were invited and seven enrolled nurses (ENs) agreed to participate (mean age = 52, range 40–63 years). In Sweden, ENs normally have a three-year education at upper secondary school focusing on nursing, or other equivalent education. The participants all worked part time (80% of full time) and the mean for their period of employment at the care unit was 14.6 years (range 9–26 years). Female participants were in the majority; due to ethical reasons the number of men is not reported.
Data collection
The interviews were carried out by an experienced researcher from the research project between December 2013 and March 2014 in a secluded room at the unit under study. The interviewer used an interview guide consisting of open-ended questions that was prepared by the research team. In order to encourage the respondents to feel confident in the interview situation and to facilitate narration, interviews started with broad overall questions in which care providers were asked to describe their daily work during periods of downsizing and reorganisation. For instance, overall questions such as ‘What are your experiences of the changes from the reorganisation and downsizing at your workplace?’ were included, as well as more specific follow-up questions when necessary, for example when care providers described they lacked time ‘Please describe what it means to get troubled conscience when you do not have the time to provide the care you want to provide?’. In order to promote progression in the interviews, probing questions were asked, for example ‘How did that make you feel?’, ‘So what then?’. The audio-recorded interviews lasted 5 hours and 28 minutes (median = 59 minutes).
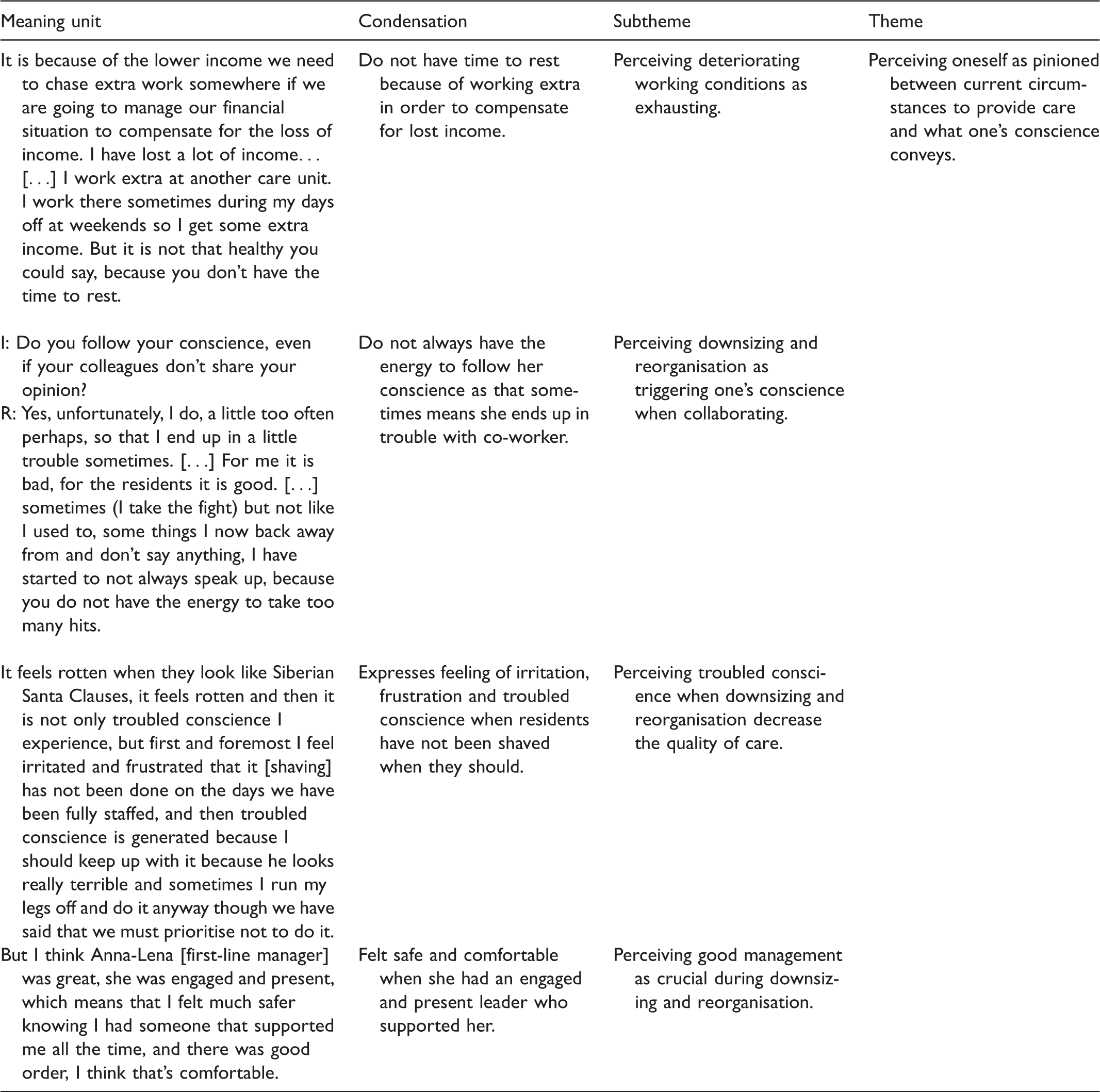
Data analysis
Examples of structural analysis.
Ethics
Participants gave informed consent to participate in the study. Participants were provided with written and verbal information regarding the fact that their participation was voluntary and that they could choose to withdraw participation without giving any reason. They were guaranteed confidentiality, that is, no specifics such as names were transcribed into writing and no unsanctioned persons had access to the data. Permission for this study was provided by the head management of the private non-profit organisation for care of older people and by the first-line manager. Ethical approval was received from the regional ethical review board.
Results
Perceiving oneself as pinioned between current circumstances to provide care and what one’s conscience conveys
Illustration of the subthemes and theme in the thematic analysis.
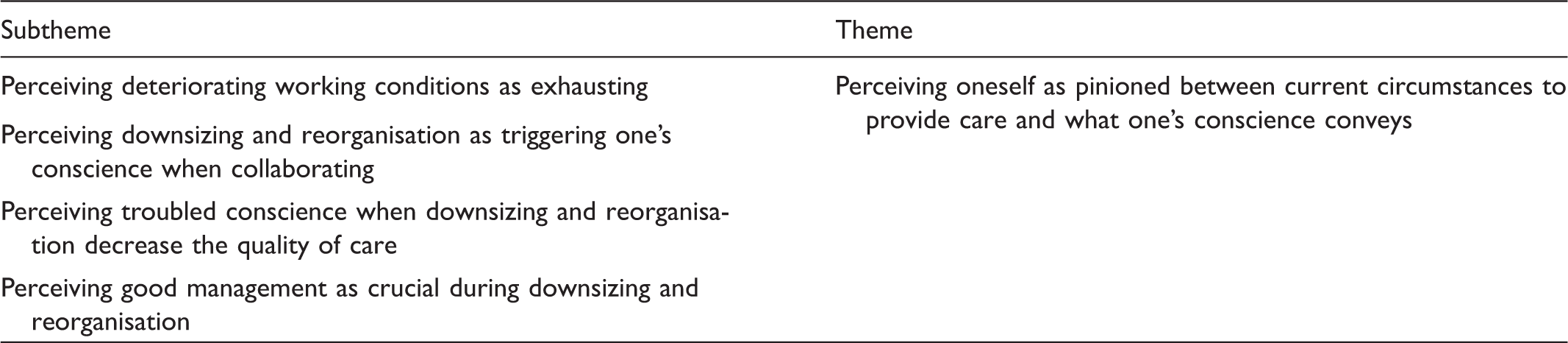
Perceiving deteriorating working conditions as exhausting
Care providers described how downsizing had caused deterioration in their working conditions, which had a negative impact on their own health, both physical and mental. These deteriorations were: a decrease in employment from full time to part time, sometimes longer shifts up to 13 hours, and no longer having permission to call in substitutes the first day someone was ill. These deteriorations resulted in increased time pressure as care providers had to perform more work tasks with less time available and sometimes with fewer members of staff. They expressed how the increased work pace took its toll on their bodies and how tired they sometimes felt during their long shifts. The stressful working climate could sometimes drain them of energy and negatively influence their ability to act professionally. They perceived that ‘money’ had greater significance than humanistic values during times of downsizing, which exerted a negative influence on their wellbeing and the quality of care. They expressed great concern for their personal finances as their employment rate changed, how they would cope on their decreased income and how this would affect their future pensions. They worked extra shifts to compensate for the decreased income and/or worked at other workplaces, which meant they did not get the rest they needed. R: It is because of the lower income we need to chase extra work somewhere if we are going to manage our financial situation to compensate for the loss of income. I have lost a lot of income… […] I work extra at another care unit. I work there sometimes during my days off at weekends so I get some extra income. But it is not that healthy you could say, because you don’t have the time to rest.
Perceiving downsizing and reorganisation as triggering one’s conscience when collaborating
Furthermore, care providers described how downsizing and reorganisation triggered their consciences. They expressed, on one hand, how important it was to follow one’s conscience, and, on the other hand, how their own shortcomings in doing so burdened their consciences. Care providers described their consciences as a moral compass and a guide that could help them to provide good care, know how to prioritise and know what is right and wrong. They also described how their consciences became troubled about others’ shortcomings, for example when they thought their colleagues had not done their work well enough and it affected the residents negatively. They perceived this as burdensome as they had to call attention to this and their colleagues might be offended or they might have to do the work instead of them. They described it as important to follow one’s conscience for the sake of the residents, even if their colleagues or managers did not agree and they sometimes ended up in conflicts. Care providers believed they sometimes were perceived as difficult and annoying by their managers when they followed their consciences by pointing out various deficiencies in the care of residents. This could make them scared of taking action in the future. Troubled conscience was described as a driving force in their work, but also as exhausting and depleting. I: Do you follow your conscience, even if your colleagues don’t share your opinion? R: Yes, unfortunately, I do, a little too often perhaps, so that I end up in a little trouble sometimes. […] For me it is bad, for the residents it is good. […] sometimes [I take the fight] but not like I used to, some things I now back away from and don’t say anything, I have started to not always speak up, because you do not have the energy to take too many hits.
Perceiving troubled conscience when downsizing and reorganisation decrease the quality of care
Care providers said that the values that care was supposed to be based on according to official documents (the organisation’s declared fundamental values) were nowadays only empty words that did not mean anything in practice. It says non-profit organisation on the website but it’s just the opposite [i.e. for-profit] and the question is if it is… what’s it called false marketing. […] No, it’s just the kind of rhetoric that they have, in reality they run it differently. It feels rotten when they [residents] look like Siberian Santa Clauses, it feels rotten and then it is not only troubled conscience I experience, but first and foremost I feel irritated and frustrated that it [shaving] has not been done on the days we have been fully staffed, and then troubled conscience is generated because I should keep up with it because he looks really terrible and sometimes I run my legs off and do it anyway though we have said that we must prioritise not to do it.
Perceiving good management as crucial during downsizing and reorganisation
The care providers described how important it was to have a good manager with well-functioning leadership during periods of downsizing. They stated that it was important for a good manager to be dedicated, orderly, present, energetic/active, fair, strong, someone that can be trusted, able to make decisions and to possess good communication skills. For a period of time during the downsizing they had a first-line manager with such qualities. They expressed how that manager provided them with a sense of safety, strengthened their feeling of belonging to a team where everybody worked to provide the best possible care for the residents and that everything became much calmer at their workplace. But I think Anna-Lena [first-line manager] was great, she was engaged and present, which means that I felt much safer knowing I had someone that supported me all the time, and there was good order, I think that’s comfortable. When I started to work here in 2005 so… it’s impossible to compare, then we [the staff] had respite, we had health care, we felt that they [head management] cared about the staff, but now we are just air, we are nothing.
Discussion
The aim of the study was to describe care providers’ experiences of working in private non-profit residential care for older people during downsizing and reorganisation, focusing on troubled conscience. To our knowledge there are no previous studies available that have shown that the consequences of downsizing and reorganization in private non-profit RCOP can generate troubled conscience. Our results show that the care providers described perceiving oneself as pinioned between current circumstances to provide care and what their conscience conveyed.
The results show that care providers perceived deteriorating working conditions as exhausting, downsizing and reorganisation as triggering one’s conscience when collaborating, also that they perceived troubled conscience when downsizing and reorganisation decrease the quality of care. They experienced increased demands, decreased control and lack of support at their workplace during the time of downsizing and reorganisation. The demand-control model, used in several studies since the late 1970s, has shown that the combination of low control and high demands is related to increased risk of developing stress-related illness. 28 Furthermore, results from a systematic literature review show how empirical evidence is concordant with the demand-control model as work demands such as workload, long hours, pressure, a lack of support from managers and lack of control over work are the most common work factors linked to work-related psychological ill health. 29 Consequently, as these kinds of work factors were described by the care providers it is not surprising that they described how this contributed to deteriorating physical and mental health. Another possible reason for which the care providers expressed such difficult experiences was that the changed working conditions from downsizing and reorganisation generated troubled conscience.
The results show that care providers described the importance of following one’s conscience for the sake of the residents by pointing out various deficiencies in the care of residents, even when their colleagues or managers disagreed. These disagreements sometimes lead to conflicts and made them scared of taking action in the future. When care providers speak out at their workplace it might be an expression of what they interpret that their conscience is telling them. One reason for speaking out in the workplace could be an experience of moral responsibility, 30 that is a factor of moral sensitivity. 31 The negative factor of moral sensitivity, sense of moral burden, has been found to be significantly associated with stress of conscience among healthcare employees. 32 One reflection is that if care providers do not dare to communicate what they regard their conscience is telling them, their own health can be threatened as they might start deadening their conscience in order to keep working in healthcare. Results from one study have shown that there are positive relationships between having to deaden one’s conscience in order to keep working in healthcare and stress of conscience. 6 Results from studies have also shown that stress of conscience may negatively influence the wellbeing of healthcare personnel 24 and the quality of care. 25 It is problematic if the experiences of increased demands, low control and perceptions of decreased quality of care described increase the risk of care providers beginning to deaden their conscience. This may have serious consequences as care providers’ consciences are essential to the provision of high-quality care and because of the negative consequences associated with having to deaden one’s conscience. Sharing and reflecting with others on difficult situations that generate troubled conscience can be helpful for care providers to learn to constructively deal with troubled conscience and to relieve the burden of troubled conscience and increase the quality of care. 33 Thus it seems important to make it possible for care providers to share what their conscience tells them. Care providers can, together with co-workers and their first-line manager, reflect on possible and meaningful measures to take in order to uphold the quality of care during times of downsizing and reorganisation. This, in turn, can relieve their burden of troubled conscience and reduce the risk of care providers deadening their conscience.
The results show that care providers perceived good management as crucial during downsizing and reorganisation. They described that having several changes of first-line managers during this period had a detrimental effect, and they remembered one manager who exercised good leadership and provided them with a sense of safety and togetherness. Care providers’ descriptions of how this good leadership was exercised may, for example, be viewed in the light of resonant leadership (i.e. emotionally intelligent leadership). Results from one study have shown that nurses who work for resonant leaders during hospital restructuring report significantly fewer negative effects from hospital restructuring, greater workgroup collaboration and more satisfaction with supervision than those who work for dissonant leaders (pacesetting and commanding). It was concluded that resonant nursing leaders can positively affect the wellbeing and health of nurses and the outcomes for patients. 34 Results from studies have also shown that leadership is important during times of reorganisation in order to involve employees in the process 35 and employee participation has been shown to be positively associated with employee work attitudes and wellbeing during downsizing. 36 Our findings suggest that it is important to avoid frequent changes of managers during times of downsizing and reorganisation when job demands are expected to increase. Carefully considering the exercise of leadership seems to be of great importance when downsizing and reorganisation are planned and implemented.
Additionally, care providers also narrated their experiences of not feeling appreciated or important in the eyes of the head management; in other words they described a lack of recognition. Results from another study have shown that recognition can be an important contributor to employees’ wellbeing 37 and a review showed that recognition for work achievements is an essential motivational factor. 38 One reflection is that these experiences of lack of recognition may partly be explained by the lack of information, that is, the lack of communication from the head management that the care providers described. Several authors have suggested that frequent communication that is timely, accurate, with relevant content and delivered using various techniques both verbally and in writing may buffer some of the negative effects related to downsizing and reorganisation.5,39 Numerous studies have also demonstrated that communication is essential in developing and maintaining trust.40,41 However, reorganisation and downsizing have been shown to be associated with declining trust in management. 42 It can be problematic if downsizing and reorganisation reduce trust in management as results from studies have shown that trust and good internal communication strategies are associated with several positive employee outcomes.43,44 It is likely a difficult task for management to provide the care providers with enough information in the burdensome climate of downsizing and reorganisation with frequent changes of first-line managers. If downsizing unleashes enough uncertainty among employees it is possible that no amount of information will feel sufficient. 45 The results point to great attention to the communication process being essential for management in order to relieve some of the potential harmful experiences the care providers described as consequences of downsizing and reorganisation. It also seems to be of vital importance that care providers continually receive recognition from both management and first-line managers during the burdensome period of downsizing and reorganisation in order to reduce negative effects.
Methodological considerations
Not all of the participants who were asked to interview agreed to participate. As the results showed the care providers wanted to work more than part time and expressed personal economical concerns. Consequently, a logical interpretation is that the topic under study was perceived by some care providers as too sensitive to talk about in interviews. However, the interviews were regarded as rich in content answering the aim of our study. This interview study used a qualitative descriptive design. This research design was chosen since it is considered to be an appropriate method when knowledge of the study topic is limited 46 and in order to elaborate on people’s experiences. 27 Qualitative content analysis was considered applicable with regard to the collected data.27,47 Qualitative content analysis has been criticised as being reductionist and there may be a risk that as the text is broken into pieces this changes the overall meaning. 48 The text was therefore read repeatedly and remained in focus during the analysis. Procedures to achieve trustworthiness, that is, dependability, credibility and transferability, have been used in accordance with Graneheim and Lundman. 27 In order to facilitate judgements regarding trustworthiness of the interpretations, representative quotations were used throughout the presentation of the results and we have tried to illustrate how meaning units, condensations and abstractions were made (see Table 1). Discussions about the analysis were conducted in a critical and open dialogue among the researchers regarding the construction of subthemes and the theme to establish trustworthiness. Some minor adjustments have been made in the presentation of results in order to guarantee confidentiality. In order to reach a more comprehensive picture of the situation under study, it would be interesting to study how managers, residents and relatives at this particular unit experienced the organisational changes during the described period.
Conclusions
Based on the care providers’ perceptions of downsizing and reorganisation it is logical to suggest that it is important to avoid frequent changes of managers at various levels. A well-functioning leadership was perceived as important by the care providers. One reflection is that well-functioning leadership may increase care providers’ feelings of recognition, enhance trust and facilitate their involvement in the process of change. The results also point to the importance of having well-functioning internal communication strategies as these may buffer some of the negative consequences of downsizing and reorganisation. A work environment in which care providers can express what their conscience tells them and together reflect on what possible and meaningful measures to take, may help maintain their wellbeing and, by extension, the quality of care during times of downsizing and reorganisation.
Footnotes
Ethical approval
Ethical approval to conduct the study was given by the Ethics Committee of the Faculty of Medicine, Umeå University (dnr 09-099M).
Acknowledgements
The authors would like to thank all the study participants as well as the participants in the research seminars for their valuable comments. We would also like to thank Berit Seiger Cronfalk for conducting the interviews.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the Swedish Research Council (Grant no. K2011-70X-21823-01-3), Swedish Council for Working Life and Social Research (Dnr: 210-0296) and the Medical Faculty, Umeå University.