
Abstract
Living in residential care facilities for older people is described in both positive and negative terms. To maintain care quality of a vulnerable group in a constantly changing care context, it is important to continually describe their experiences. This qualitative study aims to describe residents’ experiences of living in a residential care facility for older people in Sweden. Six residents were interviewed and the interviews were analyzed using qualitative content analysis. The analysis resulted in nine sub-categories, two categories and one overall theme. Living in a residential care facility for older people is revealed as ‘Struggling between a sense of belonging and a sense of alienation’. It is of great importance for care providers to explore and try to understand what individuals perceive as factors for feelings of belonging, thereby preventing alienation.
Introduction
Almost worldwide, the number of people over the age of 60 is expected to double by 2050, a fact that will require radical societal change, e.g. changes in healthcare systems. These changes mean moving from disease-based healthcare towards an older-person-centered and integrated care. 1 In Sweden, the life expectancy is increasing continuously and the proportion of persons 65 years and older is expected to be around 23% in 2030. 2 It is reasonable to assume that these changes also mean that the need for support and help for older people will increase. 3
In March 2018, about 81,400 persons aged 65 years and older were permanently living in residential care facilities for older people in Sweden. 4 These older people are usually of advanced age, often suffering from multi-morbidity simultaneously with dementia diseases, and in need of good quality care 24 hours a day. 5 Older peoples' experiences of living in municipal residential care facilities are not well described in the literature, especially not in Sweden. Due to older peoples' fragility and multi-morbidity, they often have difficulties in both answering questions and filling in surveys and it is often their relatives who answer questions about their experiences.6,7
Experiences of living in residential care for older people are described in both positive and negative terms. Feelings of safety and a sense of belonging are described when residents receive the help they need.8–10 To feel secure, respected and to have a sense of autonomy are regarded as positive factors by the residents.11,12 Feelings of being cared for, trust, and satisfaction with the service provided at the residences are also examples of positive experiences.12–15 Residents living in residential care describe negative experiences such as difficulties in developing new relationships and lack of relationships,8,9,13,16 loneliness,8,17,18 and lack of activities.17,19 Loss of autonomy and control,11,20,21 loss of independence, 15 fighting to uphold independence and control, 14 lack of privacy,10,11 and unsatisfactory self-determination,22,23 are also described. Feelings of being a burden and of less worth together with striving to be regarded as a worthwhile person are also described by residents living in residential care for older people.13,24 Residents’ experiences of care and help are described as a balance between sorrow and relief and a struggle to maintain control and connectedness. 25 Living in a nursing home is described as a ‘safe but lonely’ experience, 12 revealing ambiguous experiences. Wadensten 26 found that residents described very different views of their lives in nursing homes; some residents were more pleased with most things while others were dissatisfied with many things.
The staff have an important role in residents' lives, for example, when it comes to creating purposeful activities for the residents. 27 However, residents relate staff shortages and their consequences on care.13,14,16,28 Care providers are often described by residents as having too little time to keep them company due to a heavy workload8,10 and as too busy to be able to converse with the residents.15,29,30 Special moments are often described as being when care providers are conversing with residents about simple things such as their experiences of their everyday lives. Such interaction with care providers creates a special closeness to them, 31 and enhances residents' quality of life. 28
In summary, the findings from the studies mentioned above show that living in a residential care facility for older people is experienced both positively and negatively. Only a few of these studies have been conducted in Sweden. Residential care for older people in Sweden and in other parts of Europe has undergone major changes including downsizing. The changes also include an increase of knowledge requirements among care providers as residents in care facilities for older people grow older and sicker. Care providers now perform more nursing work and more skilled tasks. Therefore, the requirement for knowledge about older peoples' experiences of living in residential care facilities has increased.32,33 Along with these changes, it is also known that the staff often report deteriorating working conditions such as increased workload. 34 In order to uphold quality of care of a very vulnerable group in a constantly changing society, it is important to continually describe their experiences.
Aim
The aim of this qualitative study was to describe residents’ experiences of living in a residential care facility for older people in Sweden. The research question derives from the aim ‘What experiences do older people living in residential care facilities describe?’
Method
A qualitative method was considered suitable for this study. A qualitative approach is appropriate when people's experiences and/or perceptions of their world are in focus of the study.35,36 The method used for analyzing the interview text was qualitative content analysis.37–38 In content analysis, the researcher explores textual data with the aim of grouping together similar types of utterances. The method is appropriate when researchers want to identify key issues in data. 37
Participants
Characteristics of the participants.
Setting
The residential care facility, which provided 24-hour care, was divided into four units consisting of 52 single-resident apartments. All residents living in the units under study were very old and suffered from chronic illnesses and extensive disabilities. A total of 10–14 residents lived in each unit and four to six care providers were on duty in the daytime during the week and two were on duty in the evenings. At night two care providers were responsible for all 52 residents, and staffing levels were lower during weekends. Registered nurses and general practitioners were available during daytimes on a consultative basis. Registered nurses were also available on weekday evenings and nights as well as at weekends when they served several housing units. Each resident rented a single apartment, furnished with their own belongings. The apartment consisted of a combined alcove/minor living room with a small kitchen, a toilet and a wardrobe. The units had a shared kitchen and living/dining room, where residents ate their meals together if they preferred to. All residents were assigned a contact person who kept in touch with relatives. Occasionally, activities were performed at the units by people coming from the outside, e.g. churches. The responsibilities of the ENs and NAs consisted of customary duties, e.g. helping/supporting the residents with their daily hygiene, food and meals, and washing and cleaning.
Data collection
The interviews were carried out by the author and a co-researcher, both with extensive work experience in the field, but not at the current facility. They were held in the participants’ own apartments. Privacy was considered important because the residents might narrate about the care provided at the residence. 40 With the help of an interview guide, the individual interviews were conducted in April 2010 and in January 2012. Participants were encouraged to, in line with the aim of the study, narrate freely about their experiences. The opening question was ‘Please narrate your experiences of living in a residential care facility’. Probing questions were then used such as ‘So, what then?’ Participants were also asked to narrate their experiences of the care received, relations with the care providers and about their perceptions of the indoor and outdoor environment. It was of great importance to create a safe climate with the participants since speaking up may lead to feelings of jeopardizing care or personal welfare for the residents. The interviews, therefore, started with an introductory phase wherein the resident once again was informed about the study. Thereafter, a personalizing phase often started in which the participants commented on the research question in a personal context. 40 The interviews were recorded on a digital voice recorder and transcribed verbatim (except names and places), including indications of sighs, laughter, crying, and silence. The interviews lasted between 25 and 55 min and the total length of the interviews was 3 hours and 55 minutes.
Data analysis
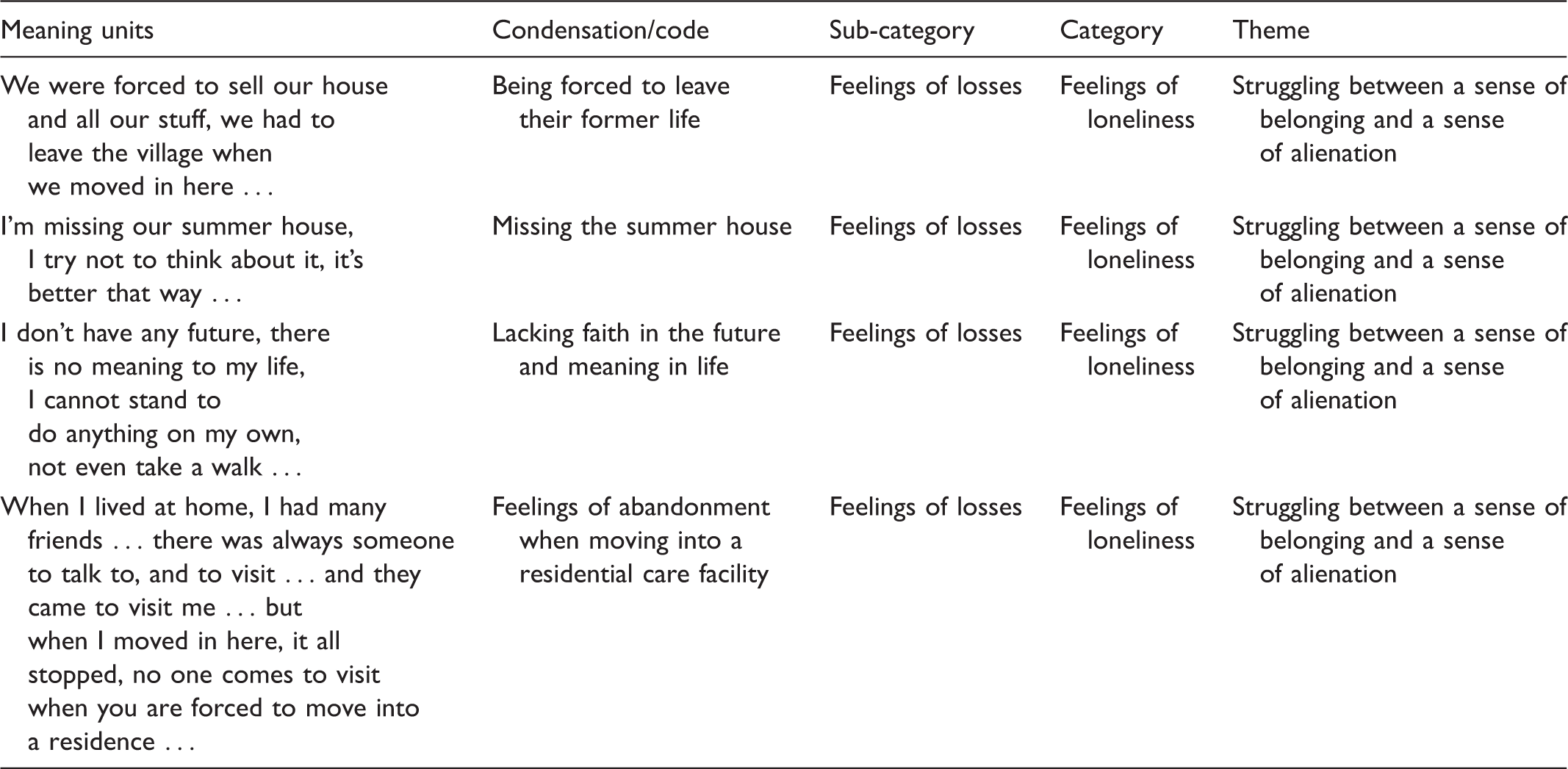
Example of the process of analysis in one sub-theme.
Ethical considerations
Permission to conduct the study was granted by the Regional Ethical Review Board (Dnr 09-099). Participants were given both verbal and written information about the study and gave their written informed consent to participate. Older people with extensive disabilities are vulnerable, and when informed consent was obtained it was important to provide the participants with a reasonable understanding of their participation in the study, i.e. to give a short description of the study and their involvement in the study. There was also a risk that the residents might feel uncomfortable expressing criticism about the care provided due to concerns about reprisals from care providers. 40 It was therefore important to create a safe interview situation. The participants were informed that participation was voluntary and that they could end the interview at any time without giving any reason. To guarantee confidentiality, minor revisions have been made in the presentation of the results, e.g. names of places have been deleted and the residents are given fictitious names. The interviews were stored in a locked cabinet where only authorized persons had access to them.
Findings
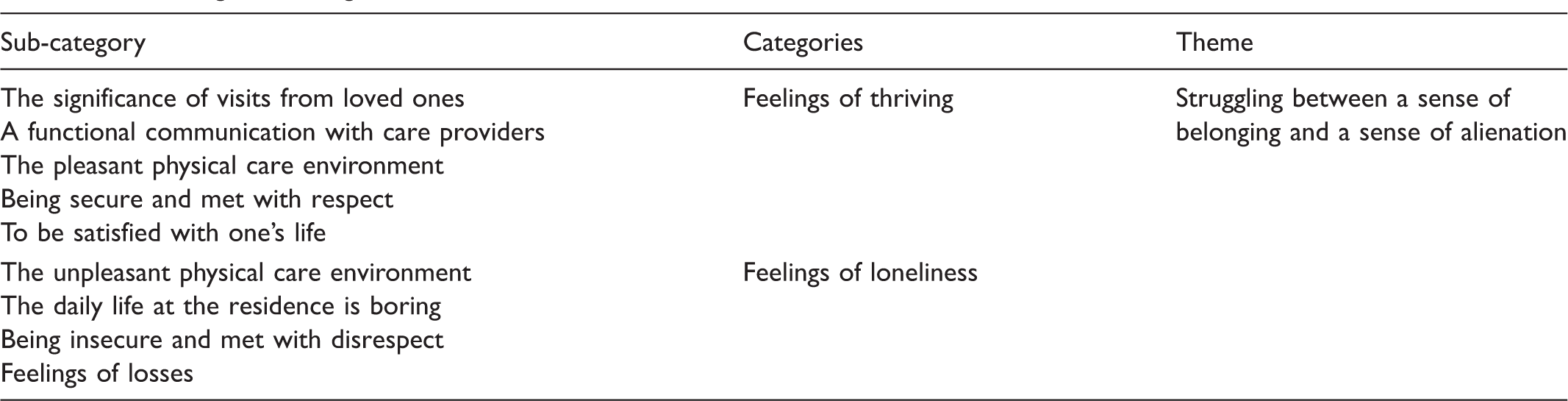
Sub-categories, categories and theme.
Struggling between a sense of belonging and a sense of alienation
The theme consists of two categories and nine sub-categories. The first category, ‘Feelings of thriving’, consists of the following five sub-categories: ‘The significance of visits from loved ones’, ‘A functional communication with the care providers’, ‘The pleasant physical care environment’, ‘Being secure and met with respect’ and ‘To be satisfied with one's life’. The second category, ‘Feelings of loneliness’, consists of four sub-categories: ‘The unpleasant physical care environment’, ‘The daily life at the residence is boring’, ‘Being insecure and met with disrespect’ and ‘Feelings of losses’. The categories and sub-categories are presented below and quotations are used to illustrate content from the interviews as a means of achieving trustworthiness in the study.
Feelings of thriving
The significance of visits from loved ones
Visits from loved ones were said to be very important, to be appreciated and made the residents feel connected to their roots and to the outside world. The residents described their happiness when their loved ones arrived on a surprise visit, and they could have coffee together. Sometimes the loved ones brought gifts, which were appreciated and made the residents feel cared for. The residents also mentioned that when they needed someone to talk to about difficult matters, they turned to their loved ones. It means a lot to me that they come to visit. I feel that they care for me. If I have ponderings, I talk to my sisters. (Resident Anna, female, 84 years)
A functional communication with care providers
This sub-category dealt with communication between the residents and the care providers. The residents appreciated when they understood what the care providers said to them, that they used simple language, and that they were easy to talk to. The residents also stated that it was important for them to be treated as equals in conversations with the care providers. A functional communication was described as pleasant and made them feel a connection to the care providers. One resident said that if she had something special on her mind she waited until her contact person was working because they had a functional communication. Interviewer: What about your contact person? Resident: If I'm pondering on something special, then I wait until she works the next day and then I talk to her. (Louise, female, 80 years)
The pleasant physical care environment
The home-like environment and being in their own apartment was described as pleasant. Some residents described that the planning of their apartment was pleasant, that the unit was clean and tidy, and that they had beautiful things to look upon at the unit. Well, the staff is cleaning, they really are perfectionists. (Resident Mary, female, 83 years)
Being secure and met with respect
The residents described that if they needed help and pressed the alarm button, the care providers responded almost immediately. They felt safe as they had access to help from care providers even during the night. Resident: They pop in at night and look after me. (Mary, female, 83 years) Interviewer: Does it feel safe? Resident: Yes of course, you never know when you will fall ill, I'm not a healthy person.
The residents described feelings of being paid attention to when the care providers had enough time to interact with them, when they came quickly to help, and when they listened to what they were telling them. To feel welcome at the dinner table was also described as a sign of being paid attention to. They are always greeting me when I come to the dining room, it feels like they see me. (Resident Louise, female, 80 years)
To be satisfied with one's life
Some of the residents described that they were having a good quality of life, i.e. being as healthy as possible, having the opportunity to live such a long life, and having the ability to contemplate life. One resident narrated about her gratefulness with being cognitively intact: I'm happy that I'm not so confused that I cannot talk to somebody, I'm grateful for that. (Resident Joanna, female, 87 years)
Feelings of loneliness
The unpleasant physical care environment
Some residents described an unpleasant outdoor environment, that their apartment was too big, or that there was too much time between cleaning sessions. Their perceptions of an unpleasant environment made them feel unhappy. It's problematic for me to get outside the building on my own [the unit is located on the second floor], it should have been a big ramp from here … and I think the outdoor environment is unpleasant, it's not fun at all. (Resident Elizabeth, female, 95 years)
The daily life at the residence is boring
The food that was served at the unit was described as boring with a lack of variety. Some residents described the boredom with the lack of activities at the unit and wanted more personnel employed so that more activities could be provided. Nothing is happening here and the food is always the same. (Resident Roger, male, 90 years)
Being insecure and met with disrespect
One resident said that he was insecure about whether he received the best available care. Insecurity was also described when confused co-residents were entering their apartments and other unauthorized persons were passing by the door into their apartment. Resident: If the door is open, then my confused co-residents may come in uninvited and that makes me feel unsafe … (Joanna, female, 87 years) Interviewer: Is it safer to lock the door? Resident: Yes.
The residents described that the care providers sometimes seemed stressed and were not listening to them. They also described that care providers sometimes lacked time to interact and that they sometimes had to wait for help. One resident described that nobody seemed to understand his illness. Resident: They haven't had time to sit down and talk for a while. (Anna, female, 84 years) Interviewer: What do you think about that? Resident: It would have been nice if they could sit down and talk, to learn more about each other … I feel abandoned.
Feelings of losses
The residents described that they were not able to do things they usually had done regularly before, e.g. visiting their summerhouse. Some residents described that they were missing their daily walks because they were dependent on help to go outside. They had no one to talk to among their co-residents who often suffered from disabilities that made communication difficult. They also expressed how they missed their partner, friends, and their former home. I love my wife, you know, and I want to have her living here with me. But they say it's impossible, she's also sick and we can't live together … it's not funny, you see. (Resident Roger, male, 90 years)
The residents described bodily impairments and a failing body. Mental impairments became evident after moving to the residence, their lives somehow ended. To be isolated from the outside world was described as shrinking them as humans. Some of the residents described their lives as meaningless and inhuman and that they wished to escape from everything. They felt that their self-esteem decreased and they described feelings of inferiority, not being good enough for anything, and not having any future. One resident said that she had gone to hell when she became sick and had to move to the residential care facility: You know, this is hell, it's inhuman to be here, sitting here day in and day out … it gets on my nerves … (Resident Elizabeth, female, 95 years) You lose your self-esteem in a way, you feel kind of inferior when you are always here in your apartment. (Resident Anna, female, 84 years)
Discussion
The aim of this study was to describe residents' experiences of living in a residential care facility for older people in Sweden. The findings in this study are in many ways similar to those of other studies in the same area; however, the interpretation of the findings is here illuminated with an emphasis on the interaction between residents and care providers that is evident in several sub-categories.
The findings show that living in a residential care facility is revealed as a struggle between a sense of belonging and a sense of alienation. A sense of belonging with the core message of thriving is interpreted when the residents receive visits from loved ones, when the communication with care providers is functional, when the physical care environment is pleasant, when they feel secure and met with respect and when they are satisfied with life.
A sense of belonging is a fundamental need in human beings 44 and may be described ‘as the experience of personal involvement in a system or environment so that persons feel themselves to be an integral part of that system or environment’.45(p.173) Higher levels of a sense of belonging are, among older adults, related to lower levels of mental ill-health 46 more reasons to live 47 and psychological well-being. 44 Lower levels of a sense of belonging have been found to be related to higher levels of depressive symptoms when living in a nursing home. 48 The core message in the sense of belonging was interpreted in the previous study as thriving. Researchers suggest a concept of thriving relevant to frail older people to include both physical and psychological aspects. The progressive loss of physical function, but also the older person's experiences of satisfaction must be considered. Instead of focusing on limitations in everyday life, it is important to enable the older person to focus on the life they have lived and what activities they still may accomplish. 49 Fundamental for thriving in nursing homes are personal relationships to specific care providers, 50 engagement in everyday activities, 51 higher quality of life and fewer physical and cognitive impairments. 52 An understanding of the findings is that it is of great importance for care providers to explore how the individual resident may reach a sense of belonging, together with the experience of thriving at the residence. Gathering information about a resident's life may be a useful tool to make them become an integral part of the system and environment in the residence.
As mentioned above, living in a residential care facility is revealed as a struggle between a sense of belonging and a sense of alienation. A sense of alienation with the core message of loneliness is interpreted when the physical care environment is unpleasant, when the daily life is boring, when residents are feeling insecure, are met with disrespect and experience losses. The process of alienation develops in an ongoing relationship between persons or groups, and may be described as an unexpected decline in the quality of results provided to a person from others. 53 A suffering person who cannot give voice to their suffering is predisposed to a state of alienation. Alienation may be described as negative connectedness 54 and involve feelings of meaninglessness, powerlessness, belonginglessness, 55 and rootlessness. 56 A study showed that nursing home residents described that the caring approach sometimes contributed to a sense of alienation. Feelings of being alone even though they met care providers daily were described. Shortfall of conversations about their lifeworld aroused strong feelings of loneliness and alienation. 57 The lives of older people living in nursing homes are characterized by feelings of aloneness in an unfamiliar place, which was interpreted as contributing to a sense of existential loneliness. 58 Successful interventions to prevent loneliness are in a review found to be animal-assisted therapy, group activities, digital technologies and person-centered care. 59 In the present study, a struggle between a sense of belonging and a sense of alienation about the experience of living in a residential care facility is revealed, i.e. two sides of the same coin. These findings stem from the interactions between the residents and the care providers. The findings point to a ‘dual nature’ of residential care for older people. The residence is filled with suffering, losses and isolation, at the same time providing the residents with security, relief and respect, 60 which point to the importance of functional relations between residents and care providers. According to the philosophy of Buber, the human being as a person emerges through entering into relationships with other persons, and the meaning of the relationship between two people is mutuality. The human being becomes through thou to an I. 61 Mutuality, that is mutual tolerance, trust and respect in the relationship between care providers and residents, is of great importance to enable older people living in residential care facilities to feel a sense of belonging at the end of their lives. It is the care provider's responsibility to provide person-centered care which maximizes the resident's feelings of a sense of belonging, for example conversations about their lifeworld, animal-assisted therapy and group activities. In this context, it is important to raise a note of caution about the effects of today's downsizing in care delivery. It takes time to develop a genuine dialogue framed by real attention, authentic meetings, total confirmation, and total presence, 62 time that may be scarce nowadays.
Methodological limitations
In this study, only six residents living in a small town in northern Sweden participated, a very small sample, and it is therefore difficult to draw conclusions about the transferability of the findings. However, the small sample may mirror the severe health condition of many residents living in residential care facilities in Sweden today. Participating in interviews may be difficult for older people with severe multi-morbidity and different communication problems, such as hearing loss and fatigue. However, these people can contribute with experiences that might benefit others in the future, including important knowledge about life in residential care facilities, that care providers can use to collaborate with residents and to increase their ability to provide individualized care.40–41 Standards for establishing trustworthiness were used in accordance with Lincoln and Guba. 63 Thus, an effort was made to carefully describe the process of the analysis, e.g. using direct quotations as examples of the results. To avoid breaking the data down into pieces, i.e. losing the integrity of the whole text, the whole text was read through several times so as to keep it in mind during the analysis. 37 Peer debriefing was used to enhance trustworthiness. Senior researchers in the area have, on several occasions, read the manuscript and provided feedback on methodological aspects as well as the analysis process and focus of the discussion. It is important to note that the six residents who participated in this study were those who managed to participate in interviews and conversations; we know nothing about those who were too ill or disabled to participate.
Conclusions and clinical implications
In this study, living in a residential care facility for older people is revealed as struggling between a sense of belonging and a sense of alienation. In this struggle, the interaction between the care providers and the residents is central. To enhance feelings of belonging and prevent feelings of alienation and loneliness, it is of great importance for care providers to explore and try to understand what the individual perceives as factors for a sense of belonging, maybe with support from the resident's life story. Interventions that may prevent feelings of alienation and loneliness in residents, e.g. conversations about their lifeworld, animal-assisted therapy and various kind of group activities, should be provided. Another important factor for enhancing feelings of belonging are care providers' responsibility to strive for mutual tolerance, trust and respect in the relation between the resident and the care provider. To enable reflection and exchanges of experiences about the care provided, natural meeting places should regularly be provided to care providers. These meetings would be an investment in quality of care during times of downsizing and increased workloads.
Footnotes
Acknowledgements
I would like to thank the participants in the study and our research colleagues in the ‘Stress of Conscience Study’, especially Professor Gunilla Strandberg who performed some of the interviews and contributed with valuable viewpoints.
Funding
This research was supported by grants from the Swedish Council for Work Life Research, the Swedish Research Council (VR), and AFA Insurance.
Conflict of interest
The author declares that there is no conflict of interest.