
Abstract
Medically unexplained symptoms (MUS) afflict up to 30% of patients who visit primary health care (PHC) services. The approach of health professionals is most important in encounters with these patients to accomplish a caring and effective treatment. The aim of the present study was to elucidate the meaning of patients’ lived experiences of encounters with PHC professionals when suffering from MUS. The study was based on ten narrative interviews with informants aged 24–61 years. Phenomenological hermeneutics was used as the method of analysis. Three themes emerged: Striving for understanding, Expecting to be taken seriously and Fear of being abandoned. The result can be seen as a call for health professionals to invite patients into an interpreting process to create a joint understanding of the patient’s body experiences and life situation. Thus the patient might also become reconciled with suffering and move on in life.
Keywords
Introduction
Medically unexplained symptoms (MUS) is a label that covers a range of conditions where patients’ subjective experiences cannot be explained objectively/medically. 1 The reported prevalence varies, but it has been estimated that up to 30% of patients suffer from MUS.2–6 Headache, fatigue, dyspepsia, dizziness, joint and back pain are examples of the most common symptoms of MUS.4,6 Patients with MUS also to a high extent report mood and anxiety disorders. 6
It is difficult to distinguish MUS from other complex conditions such as, for example, chronic pain, burnout and other symptoms involving unspecific physical and mental suffering. However, the PubMed MeSH definition of chronic pain limits the problem to a single symptom although research argues for the importance of seeing it as a complex involving bio-psychological factors.
7
Aching sensation that persists for more than a few months. It may or may not be associated with trauma or disease, and may persist after the initial injury has healed. Its localization, character, and timing are more vague than with acute pain.
8
Various theoretical models have been tested and used to explain the causes of these symptoms. One that is frequently mentioned is the bio-psychosocial model, which emphasises the interaction between an individual’s physical, psychological and social conditions in the development of MUS. 12 Beside antidepressant pharmacological treatment various therapeutic methods and programmes have been tested, for example, cognitive behavioural therapy (CBT) and re-attribution, both of which have been found to provide beneficial effects in the area of patients’ coping strategies.13–15 Other studies that have focused on finding strategies for involving patients in care planning have revealed that Collaborative Stepped Care and the development of Provider–Patient Relation (PPR) can increase patient well-being and reduce health-care consumption.15,16 However, at present there is no accepted evidence-based or holistic method used in general clinical practice. 1
It is well known that experiencing symptoms that cannot be explained by existing medical knowledge leads to frustration.13–18 Feelings of being a ‘medical orphan’ 16 or a burden 17 may impair the health process. Patients have also reported that the symptoms overwhelm life, restricting and making them dependent. Sveneaeus described this overwhelming feeling, from a bio-ethical perspective, as an existential matter of suffering. 19 With reference to Cassell, the author further claims that one reason for the inability to manage suffering in health care is that medicine is preoccupied with the causes of pain at the expense of the meaning of suffering for the person.
Still, some patients finally learn to identify and use personal resources to manage their changed life situation and to reinterpret their life story. This endeavour can be facilitated by appropriate support from friends, family members and/or health professionals, 20 where the clinical competence, empathy and communication skills are important for the patient’s experience of encounters in care.15,21,22 However, studies show that health professionals experience powerlessness when treating this patient group. 23 At times consultations even end up in a struggle when the patient’s interpretation of her/his symptoms conflicts with that of the professional.17,18
As most patients living with MUS never have their symptoms explained and receive no medical diagnosis, the health professionals’ approach in encounters with these patients is essential. Instead of getting caught up in a futile attempt to find explanations and a cure, health professionals should focus on a more health promotional perspective by highlighting the patients’ health resources and strategies in daily life. Hyvönen and Nikkonen described health professionals’ personality and attitude as ‘meta tools’ for establishing a basis for collaborating with the patient in care planning. 24 This is in line with a person-centred approach of viewing the person from a salutogenic perspective, acknowledging her/him as integrated and whole, with the capacity to take control over health factors in her/his life situation.18,25–27 Person-centred care has also been described as a partnership between the patient and health professionals who view patients as competent partners with their own resources, whose experiences of living with MUS and encounters with health professionals in the medical context are seen as the heart of care.25,27
This study is one part of the Symptom Contextualisation in Primary Health Care (SCPHC) project carried out at the Gothenburg Centre for Person-Centred Care (GPCC). The overall aim of the study was to describe how MUS are interpreted and managed in PHC settings. Various forms of data collection were thus employed involving interviews, recordings of consultations with physicians and documentation in patient records.
Aim
The aim of the present study was to elucidate the meaning of patients’ lived experiences of encounters with PHC professionals when suffering from MUS.
Method
Data were collected using narrative interviews 28 in order to capture the informants’ lived experiences of the studied phenomenon and analysed using a phenomenological-hermeneutic method inspired by Ricoeur. 29 The method focuses on the meaning of human experience and during the analysis the researcher elaborates on what the text says and what the text is talking about by means of a dialectical movement between the parts and the whole. 29 This process consists of three steps: naïve reading (resulting in naïve understanding); structural analysis (resulting in themes) and comprehensive understanding.
Selection of informants for the SCPHC project
The selection of informants for the SCPHC project took place at two PHC centres in a large city in Sweden from April to November 2011 for an average of two days per week. Patients who phoned the PHC centres were screened by a physician on the research team. The centres’ telephone system was computerised, which allowed calculation of the waiting time before a nurse returned the call. During the waiting time the patient’s computerised medical record was screened.
The patients included in the study were selected based on criteria developed by Smith et al., 30 i.e., aged between 18 and 64 years; having had at least eight consultations with PHC physicians or nurses in the last 12 months; no definite diagnosis; and at least 50% of the first ten symptoms during the past 12 months having no physiological explanation. Only one exclusion criterion was specified, i.e., patients who had been treated by or were in any way dependent on members of the research team. Potential informants who met the inclusion criteria were phoned back by a member of the research team during the waiting period. After a short presentation of the study the potential informant was asked if she/he would be willing to participate.
Selection of informants for the interview study
In cases where the informants were booked for a consultation with a physician, they were asked by a member of the research team (EL) to participate in the present interview study. If they agreed, a date and time for an interview were arranged at a location chosen by the informant. Written informed consent was collected prior to each interview. Of the 20 people who fulfilled the inclusion criteria, ten chose to participate; seven women and three men, aged between 21 and 61 years (mean 44 years). Seven of the informants were born outside Sweden.
Data collection
The interviews took the form of a dialogue in order to capture human experiences based on the informants’ life-worlds. 28 They were conducted in the informants’ homes (five), at the University (three), at the PHC centre (one) or at a public library (one). They lasted between 21 and 80 minutes, were recorded by means of a digital device and transcribed verbatim. To create a comfortable conversational climate the interviewer began by presenting herself and the aim of the study. She also told the informant that she had neither read her/his medical record nor had any previous contact with her/his physician. She then asked the informant to tell her a little about her/himself before enquiring about her/his experiences of encounters with PHC professionals. In order to obtain a comprehensive narrative, follow-up questions were posed, such as: ‘Could you give an example?’, ‘Could you please tell me more about that situation?’, ‘How did you/he/she act?’ and ‘How did you feel?’
Data analysis
The data analysis was carried out separately as well as in parallel by both authors. After listening to the audio recordings and reading the transcripts several times, the authors arrived at a naïve understanding based on their initial impressions of the text. 29 The authors endeavoured to use phenomenological language when describing the meaning of the informants’ lived experiences of encounters with PHC professionals. A structural analysis was then performed in order to verify or reject the naïve understanding. The narratives were analysed in a critical and distanced way by identifying meaning units, which were condensed and coded. Through a dialectical movement between the parts and the whole and by reflection on the similarities and differences between the codes, eight sub-themes and three themes emerged.
Finally, the transcribed text, the naïve understanding and the themes were read again in order to develop a comprehensive understanding of the informants’ narratives. According to Ricoeur, a text always has a surplus of meaning and many interpretations can be found.29.31 The researcher is responsible for choosing the one she/he considers the most trustworthy. In the interpretative process, the present authors’ various theoretical perspectives and conceptions, for example related to organisations, power and medical discourses, were considered suitable for illuminating the informants’ lived experiences expressed in their narratives. However, the final interpretation was a reflection about care, the caring relationship and their impact on suffering and hope.
Ethical considerations
The study was conducted taking into account the Helsinki Declaration 32 and was approved by the regional Ethics Committee in Gothenburg (No. 115–11). Oral and written informed consent was obtained from all participants. In order to protect the informants’ confidentiality, names and circumstances that could reveal their identities have been changed.
Results
Naïve understanding
The lived experiences of a person with MUS meeting PHC professionals seems to involve moving between satisfaction and frustration, with emphasis on the latter. Feelings of lack of confidence and trust, participation, continuity and availability lead to experiences of adversity and disappointment as well as to fear of being abandoned. The desire to reach a mutual understanding of one’s health and life situation with PHC professionals seems to be strong. Expectations of PHC professionals taking patients seriously and considering them trustworthy appear to be important. There is a great desire to be able to move on and/or accept life as it is, but if the encounter is dominated by a sense of being reduced to a medical problem, it becomes difficult to feel like a whole person and experience hope.
Themes
Overview over themes and sub-themes.
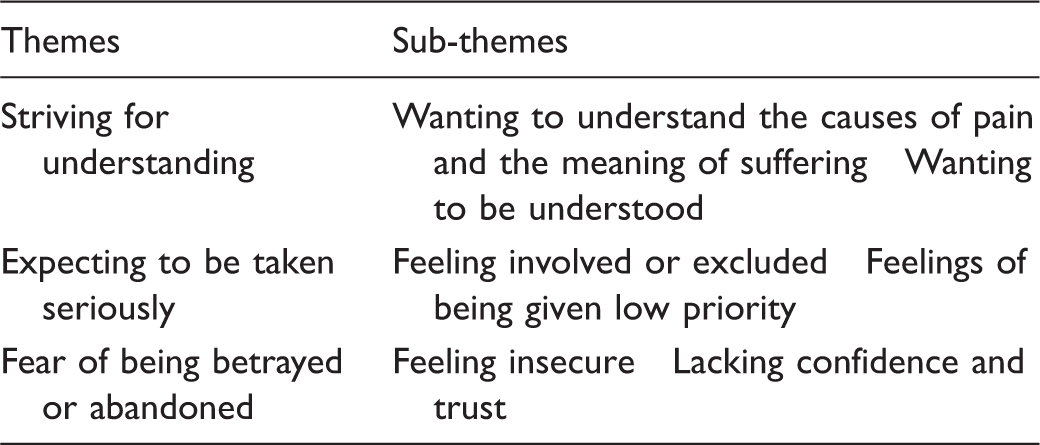
Striving for understanding
The narratives contained expressions of desires of understanding related to three levels. Firstly, the informants revealed a desire to gain an understanding of the causes and meaning of their suffering. Secondly, they expressed a wish to be understood by others; in this context the health professionals. Moreover, the patients tried to show understanding by taking account of the time constraints of the PHC professionals’ work situation.
Wanting to understand the causes of pain and the meaning of suffering
The desire to understand the cause and meaning of suffering appeared clearly in the informants’ narratives. One informant, Flora, told how she felt the need to understand the causes of her suffering in order to be able to tolerate the pain and become reconciled to it. She related that although she was familiar with medicine from her working life, she needed help to understand the emotional dimension of the pain and how it could be managed. … and you can say to your doctor: ‘I feel weak, I feel that now I have to accept that I must learn to live with my pain’ but although I have a lot of knowledge it is only intellectual, it does not help me emotionally.
Another informant, Alice, expressed that she needed to be convinced that a previously diagnosed tumour was gone. She described her fear when she experienced similar symptoms and pain. Although the tumour had been treated successfully, worries and concerns about it coming back remained. The fear created the need for explanations about why she still experienced pain.
Wanting to be understood
Being acknowledged by health professionals had an impact on the informants’ sense of self and their ways of managing their feelings. The narratives revealed that feelings of being misunderstood had a negative effect on their experiences of encounters with PHC professionals. For example, after a long period of sick leave, Gabriel needed help to return to work. Don’t give me a sick note. Help me to get out of here, from this situation. Then I will be strong and find something to do anyway.
Many narratives dealt with a desire to have their fear acknowledged. Flora expressed: You see … I think we forget that when a person becomes ill, the person becomes afraid. Of course if you have your leg in a cast, then everybody knows about it … but when it is psychological it doesn’t show. The physician said that ‘you’ve had so many doctors, so from now on I will take care of you’ – ‘thank you’ I said.
Expecting to be taken seriously
Expectations of being considered reliable and acknowledged as people were important to the informants. The impression of having low priority, being excluded from taking part in one’s own care and being questioned led to experiences of not being taken seriously.
Feeling involved or excluded
A wish to influence their own care was described in many narratives. For example, Johnny experienced being involved when given the opportunity to discuss research on medical improvements with his physician. On the other hand, several informants mentioned disappointments. For example, Hanna stated that she had no opportunity to discuss her thoughts with the physician, although she had previously worked as a health professional and felt well prepared to participate in care planning. Hanna: I think the doctors feel a bit threatened if you come up with suggestions yourself. Some doctors feel a bit threatened by it I believe. Interviewer: Why? Hanna: I don’t know if the hieri … hierarchy or whatever it’s called, the ranking [prevents them].
Feelings of being given low priority
Feelings of having low priority were revealed in many narratives. Betty and Gabriel had the impression that they were uninteresting and not prioritised because the physician ended the consultation abruptly. Betty: As I stood talking with him … then, I don’t know how to say it. He almost sent me out and I was so sad. Gabriel: The last time I was here I was very sad indeed and then she [the physician] said ‘I don’t have time to talk with you about this. No, it’s enough’. You felt almost thrown out.
Fear of being abandoned
The fear of being abandoned negatively affected encounters with health professionals and the narratives included descriptions of experiences related to lack of security, continuity and trust.
Feeling insecure
Lack of follow-up, continuity and availability was evident in the narratives when informants described their insecurity in various encounters. Flora reported a lack of long-term follow-up of various symptoms that the physician failed to investigate. She finally sought private care to obtain a medical diagnosis and pharmacological treatment but feared ending up in a similar situation once again: Flora: I felt that I didn’t get the help I needed and that I was left alone. Disappointment, frustration and all that and you try to cope on your own instead, do you understand what I mean? Interviewer: Yes Flora: you do not want to be disappointed again … Flora: … no … and that’s why, I also feel it now: do not leave me like the last time … I’m going to do my best, but do not leave me in that way.
The desire for greater accessibility of health professionals was prominent in the informants’ narratives, as they had experienced major difficulty arranging an appointment at the PHC centres. Obtaining access to specialist competence was also described as a long-term project and some informants revealed that they opted to pay for examinations and treatment in other countries.
Lacking confidence and trust
Due to the informants’ dependency, the need for confidence and trust in health professionals’ competence and willingness to help was clearly expressed in the narratives. Ida and Betty told how they lost confidence in the health professionals when their symptoms were misinterpreted. Despite the fact that physicians were reluctant to prescribe further examinations, they sometimes led to medical diagnoses and treatment, i.e. MUS could be changed to medically explained symptoms (MES). Alice described her worries about the financial constraints in the health-care sector and the consequences of possible incorrect examinations and treatment. She stated: I dread to be ‘really’ sick actually, eh I think many feel a little scared about it because you see how everything is getting worse all the time, people don’t have time, they listen less now. I don’t mean that doctors are less competent, … they are definitely not but there is a lack of time and perhaps lack of empathy because people are more stressed today.
Comprehensive understanding and reflections
The informants’ experiences of encounters with PHC professionals were described as moving between satisfaction and frustration. The narratives highlighted a desire to be understood as the person behind the diagnosis and become reconciled with the suffering. By achieving an understanding of the what and the why of suffering, the individual may obtain an opportunity to become reconciled with her/his suffering. Having one’s suffering acknowledged may help a person to move on and achieve reconciliation in her/his life but if the person’s experiences are disregarded, it can lead to changes in or loss of self.33,34 If, for example, a patient describes feelings of being medically homeless, health professionals need to establish a dialogue with the patient in a way that helps her/him to find her/his bearings in the situation. 34 Thus, Yoshida et al. stress the importance of preventing catastrophic thoughts but instead focusing on the patient’s capability. 35 The authors also point out the relevance of the context in assessment and treatment; some patients actually feel worse at home compared to being at work.
Effective treatment therefore needs to be based also on the patient’s own interpretation of their symptoms and what they consider would be a beneficial treatment in their specific situation.15,16 The importance of patients’ trust and confidence in the health-care system and in health professionals for the mobilisation of patients’ adjustment/coping strategies has been noted by Aamland et al. 1 and Edlund points out that there are many opportunities for health professionals to confirm the person; actions that might evoke feelings of being taken seriously and that acknowledge her/his dignity. 36 Failure to do so can violate human dignity, leading to a sense of isolation and abandonment. Ojala et al. call for vigilance, advise not to leave the patient and warn of the risk of suicide. 7
In the present study, the expectation of being taken seriously and considered an accountable and competent person emerged as an important dimension of the informants’ experiences of encounters with health professionals. The need to feel involved and be seen and heard as a person who lives in a specific personal and cultural context proved vital for the informants’ experiences of such encounters. This need was not always met, resulting in feelings of being excluded and abandoned.
The results of the present study are supported by those of other studies, demonstrating how patients with chronic pain struggle to defend their self-esteem and dignity in meetings with health professionals. 37 The informants in our study found it burdensome having to tell their stories over and over again due to encountering different health professionals at each consultation. They therefore used various strategies, such as seeking private care abroad, in an effort to be taken seriously. Experiences of being considered to be faking and/or hysterical as mentioned in the narratives in this study were also reported by Nettleton et al. 16 They also confirm that this is a challenge that might affect one’s sense of self and social identity. 16
In accordance with Bülow, 38 Nettleton et al. 16 also demonstrated that the questioning of symptoms may not only hinder recovery but also create more suffering33,39 and that the emotional aspects of care seem to be disregarded in standardised care settings. The meaning of suffering inflicted by health professionals and organisations, for example when the patient was not allowed sufficient time to express her/his emotions, was interpreted by Arman et al. as ‘not being seen as a person’ and ‘not being taken seriously based on own needs’. 40 Salmon also revealed that patients seeking emotional support ended up disappointed because of a medically reductionist perspective that increased suffering. 18
Svenaeus has highlighted the hermeneutic implications of problems in encounters between health professionals and patients when physicians interpret suffering human beings solely on the basis of medical expertise. 34 The author refers to the hermeneutics of Gadamer and Ricoeur and claims that establishing a diagnosis is neither the beginning nor the end of a medical interpretation. Instead, it should be based on the patient’s own understanding of her/his situation. This understanding can only be achieved if the caregiver sees the patient as a person and listens to her/his life-world story; an approach that may create hope for the future. 34 Bülow 38 and Svenaeus 34 claim that the quality of the patient’s encounter with health professionals not only has implications for her/his experience of suffering but is also of significance for her/his sense of self. Bülow states that suffering can be affected and changed in encounters with ‘others’ and that a suffering human being achieves understanding of her/himself through their relationships with other people. 38
The comprehensive understanding of this study highlights the fact that when people suffering from MUS encounter PHC professionals, they hope to be listened to and understood as opposed to being reduced to a mere diagnosis. The interpretation of the informants’ narratives in this study supports the benefit of person-centred care, where the ontological assumption emphasises the patient as a person with resources, who can act in partnership with her/his carers in a mutual relationship. 25 However, such a holistic perspective is rarely applied in clinical practice. 41 A person-centred approach can be difficult for various reasons. One could be related to organisational preconditions. Today, the health-care sector in large parts of the Western world is influenced by the New Public Management approach and thus exposed to competition. In Sweden, PHC centres are managed on the principle of economic incentives based on diagnosis-related compensation systems. It is a standardised and very time-optimised care system, where patients’ encounters with PHC professionals are restricted by scheduled appointments. In this organisational context the patient’s freedom to choose and the prerequisites for person-centred care can become very limited, especially for those with complex and long-term care needs. The worst scenario is when the encounter becomes solely a matter of prescribing medication and authorising sick leave. Another obstacle is neglecting patient education aimed at supporting a collaborative learning process based on the patient’s competence and resources, 20 which can also be due to organisational reasons. 42
Methodological considerations
Patients’ narratives about encounters with health professionals provide a way to approach their experience from a life-world perspective. The narratives allowed us access to the informants’ experiences of living with MUS and their relationship with health professionals in a PHC setting. According to Wiklund-Gustin, 43 narration is not only a re-telling of previous experiences but also part of the person’s interpretative procedure. The selection procedure was thoroughly considered and carried out by the research team based on the inclusion and exclusion criteria, 30 which is important for the reliability of the results.
As the description of the selection process reveals, a large number opted not to participate. As they were under no obligation to explain why they declined participation, any discussion about their reasons is purely speculative. However, it is well known that vulnerable groups are underrepresented in research studies.44–46 Barriers described include the sampling process and labelling of participants, which might be experienced as stigmatising. Nevertheless, it is of great importance to illuminate the health situation and conditions of vulnerable groups, despite the fact that the dropout rate can be high. 46
Every possible effort was made to support the informants’ self-determination and make them feel at ease in the interview situation. Thus, the time and place of the interviews were chosen by the informants.
The fact that Swedish was not the first language of seven of the ten informants could have led to the risk of misunderstandings, both during the interviews and in the course of the analysis. However, the authors endeavoured to be as open and sensitive as possible to the narratives and, during the interviews, continuously checked that they had understood the informants correctly by asking questions. Furthermore, in the course of the analysis the authors listened to the audio recordings again while simultaneously reading the transcripts.
The credibility of the study is strengthened by the fact that the interviewer (EL) had no access to the informants’ medical records, thus was not influenced by PHC professionals’ interpretation of the informants’ health conditions. The choice of the phenomenological-hermeneutic data analysis method was considered appropriate for searching for the meaning of the informants’ experiences. This method requires the researcher to bracket her/his own pre-understanding in order to approach the informants’ experiences. 43 In this study the naïve reading was validated by the structural analysis in order to increase the credibility of the results, which is seen as a standard control procedure when using this method. 29
Conclusion
The results show that patients are relying on health professionals to help them to make sense of their suffering related to bodily sensations and limitations in daily life. Therefore, encounters with patients suffering from MUS should be characterised by an ongoing underlying dialogue with the patient. This would be an opportunity to make a joint search for potential new storylines that could be found meaningful for the patient in her/his struggle for shaping a new life narrative. 19 This requires an approach to health care that involves other disciplines, in addition to the dominant medical perspective, that would contribute to a more holistic interpretation of patients’ symptoms.
On an individual level health professionals therefore need to critically reflect on their professional role in this context: What constitutes professionalism and how can it be achieved in practice? What is needed to support health professionals to dare to address the existential questions in encounters with patients? At an organisational level, continuity and availability should be guaranteed by long-term care planning coordinated by a designated health professional. Confidence and participation require that sufficient time is allocated for consultations to make room for the patients in their struggle to make meaning and re-interpret their life narrative. Health economic studies should be carried out to measure the consequences of various care models in primary care related to this vulnerable group of patients.
Footnotes
Ethical approval
The study was approved by the Ethical Committee in Gothenburg (Dnr 207–11).
Author contributions
Eva Lidén was responsible for data collection, supervision of the study and preparation of the manuscript. Kimia Sahba Yaghmaiy was responsible for the data analysis and for writing the article.
Acknowledgements
Profound gratitude is extended to the informants in this study who made it possible for us to carry out this study. We also thank Mrs Gullvi Nilsson at Översättningar AB for reviewing the English language. This study is part of the Symptom Contextualisation in Primary Health Care (SCPHC) project carried out at the Gothenburg Centre for Person-Centred Care (GPCC).
Funding
The study was funded by the GPCC.
Conflict of interest
The authors declare that there is no conflict of interest.