
Abstract
Introduction
This study examined the effects on upper limb function, activities of daily living, and stress responses when wearing a wrist orthosis made of padded fiberglass or thermoplastic and provided essential information for selecting an orthosis.
Methods
Thirty-one healthy adults performed two tests while not wearing a wrist orthosis, wearing a padded fiberglass wrist orthosis, and wearing a thermoplastic wrist orthosis. The Purdue Pegboard Test examined upper limb control. In the second test, the actions indicated by the Hand20 questionnaire were performed while wearing a wrist orthosis. An electrocardiogram was obtained before and after each test to identify any changes in sympathetic nervous system activity.
Results
The Purdue Pegboard Test scores were significantly higher when not wearing a wrist orthosis than when wearing wrist orthosis, and the Hand20 scores for all question were significantly lower. Thermoplastic wrist orthoses had fewer restrictions for upper limb function compared to padded fiberglass wrist orthoses, however activities of daily living were more limited. The low frequency/high frequency ratio and high frequency measures showed no significant differences.
Conclusions
Pegboard test scores and the Hand 20 scores suggest that a wrist orthosis causes restriction of upper limb function.
Keywords
Introduction
A wrist orthosis has various effects owing to its movement constraints on the wrist joint. For example, wearing a wrist orthosis can decrease hand power and dexterity, increase shoulder muscle activity, and lead to fatigue.1,2 Upper limb movement can be affected by wearing a wrist orthosis and may limit activities of daily living (ADL). Common orthosis types include volar, dorsal, radial gutter (thumb spica), ulnar gutter, and sugar tong. 3 There are differences in shape and material, such as padded fiberglass, plaster, and thermoplastic. Kim et al 4 suggested that the degree of movement restriction of the upper limbs varies depending on the type of orthosis; however, studies have not shown that one type of wrist orthosis is better than another. The reasons for selection are matters of availability, affordability, and personal preference. 3 The effect on upper limb function may vary depending on the type of orthosis used. Therefore, when providing orthoses to patients, it is necessary to be knowledgeable about the characteristics of each orthosis type. Padded fiberglass or thermoplastic wrist orthoses are commonly used in Japan. Padded fiberglass wrist orthoses are highly regarded for their low cost, strength, and ease of application; however, these have limitations including heavy weight, low breathability, and inability to get wet or be cleaned. 5 In contrast, thermoplastic wrist orthoses have the advantage of being light, and the ability to get wet or be cleaned in addition to the advantages of padded fiberglass. Moreover, regarding wrist orthosis shape, the distal side of padded fiberglass wrist orthoses is often proximal to the thumb palmophalangeal crease. Therefore, it is difficult to oppose the thumb of the arm bearing the padded fiberglass wrist orthosis compared to a thermoplastic wrist orthosis at the level of the distal side of the thenar crease. Therefore, when ADL require the use of the upper limbs, thermoplastic wrist orthoses are frequently used. However, there have been no studies comparing upper limb function and ADL when wearing a padded fiberglass wrist orthosis or thermoplastic wrist orthosis.
This study examined the effects on upper limb function, ADL, and stress responses when wearing a wrist orthosis made of padded fiberglass or thermoplastic and provided essential information for selecting an orthosis. We hypothesized that there would be no difference in stress response, though upper limb function and ADL would be less restricted when wearing a thermoplastic wrist orthosis instead of a padded fiberglass wrist orthosis.
Methods
Ethical considerations
This study was conducted with the approval of the Ethics Review Committee of Kawasaki University of Medical Welfare [approval number: 19–46]. The content and purposes of the study were explained in advance to the participants, and written informed consent to participate was obtained from the participants. This study was conducted according to the principles of the Declaration of Helsinki. The authors declare no conflicts of interest associated with this manuscript.
Participants
The participants were 31 healthy adults (mean age 21.6, standard deviation [SD] 1.3, years; 10 men) with no history of musculoskeletal disorders. The sample size was determined using GPower 3.1 for power analysis (effect size: 0.25, α error probability: 0.05, power: 0.8).
Wrist orthoses
A padded fiberglass wrist orthosis and a thermoplastic wrist orthosis were fabricated for the dominant hand. The wrist orthoses were developed to ensure design uniformity. All wrist orthoses were fabricated by the first author, who has more than 10 years of occupational therapy experience in the field of hand surgery.
The padded fiberglass wrist orthosis was fabricated using ORTHOGLASS® II (BSN Medical Luxembourg, Luxembourg) with the forearm in a neutral position and matching the front of the forearm. ORTHOGLASS® II is a fiberglass coated with hydraulic resin, and its surface is covered with a non-woven pad. The proximal side of the orthosis was at 2/3 of the forearm. The distal side was 5 mm proximal to the line connecting the radial end of the thenar crease and the ulnar end of the distal transverse palmar crease, and 5 mm proximal to the thumb palmophalangeal crease. The orthosis was fixed and entirely covered with an elastic bandage. Figure 1 shows the padded fiberglass wrist orthosis. A padded fiberglass wrist orthosis before fixing (A); after fixing (B) and distal side of the orthosis (C).
The thermoplastic wrist orthosis was made of a non-sticky solid type 3.2-mm thick Taylor orthosis (Smith & Nephew Rolyan Inc., Germantown WI, USA) with the forearm in a neutral position and matching the front of the forearm. The proximal side of the orthosis was at 2/3 of the forearm. The distal side was 5 mm proximal to the line connecting the radial end of the thenar crease and the ulnar end of the distal transverse palmar crease and thenar crease. The orthosis was fixed at 2/3 of the palm, wrist joint, and proximal to the metacarpal phalangeal joint, using a 2.5-cm Velcro hook and loop.
To assess the conformity of each orthosis, the first author used visual confirmation and a goniometer to ensure that the extension angle of the wrist joint was 10°, the orthosis material did not cover the metacarpophalangeal joint from the index finger to the little finger, covered 2/3 of the length of the forearm, and covered half the circumference diameter, and there was no pain when wearing. Figure 2 shows the thermoplastic wrist orthosis. A thermoplastic wrist orthosis before fixing (A); after fixing (B) and distal side of the orthosis (C).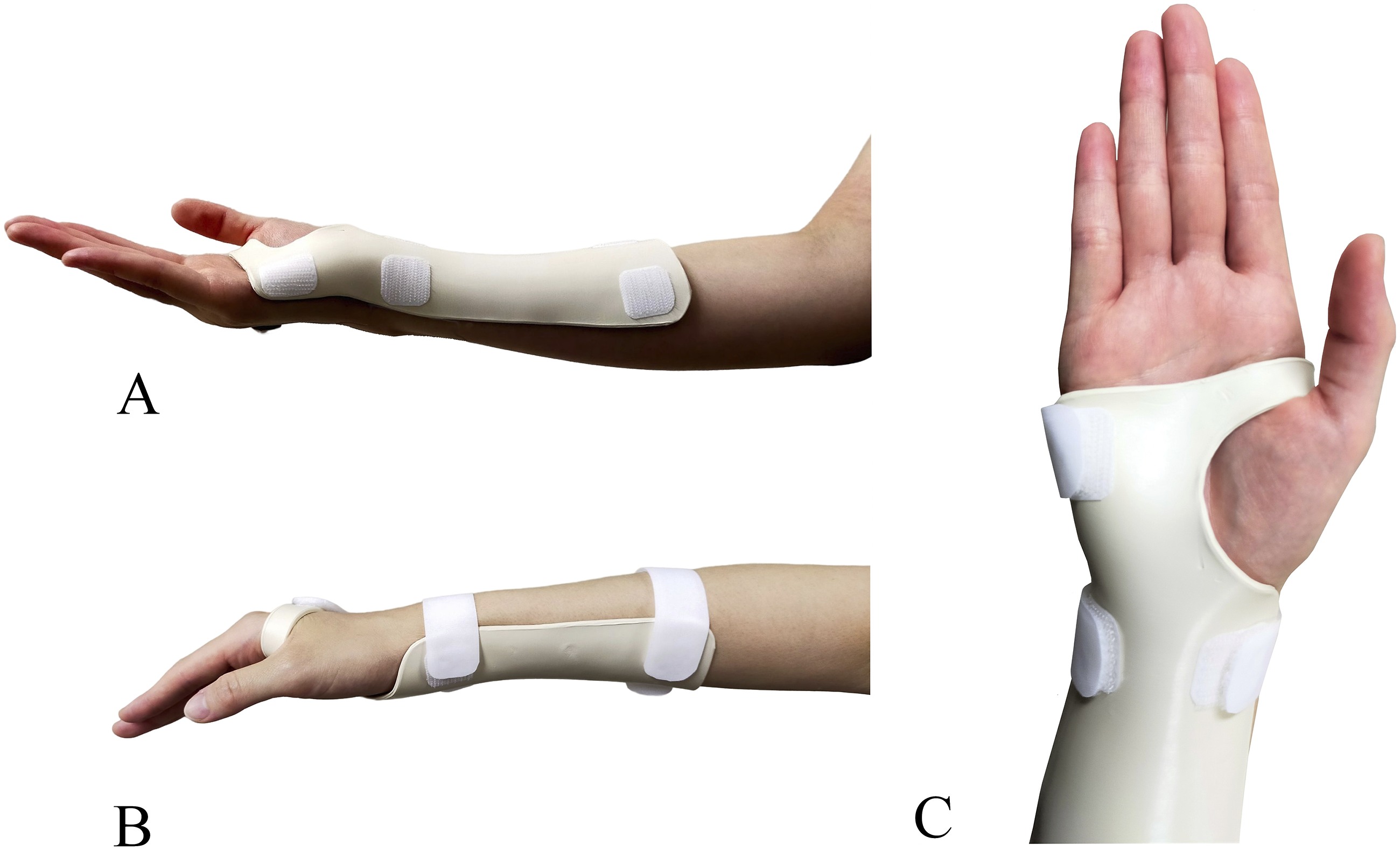
Procedure
All participants performed two tests with their dominant hand. Baseline data for all participants were measured without wearing an orthosis. Thereafter, the data of the two conditions, wearing a fitted with a padded fiberglass wrist orthosis and wearing a fitted thermoplastic wrist orthosis, were measured. The data for all three conditions were measured on different days with a least a 1-day interval. All participants were randomly assigned to groups that wore either the padded fiberglass or the thermoplastic wrist orthosis.
Measures
In the first test, upper limb function was measured using the Purdue Pegboard Test (PPT). This test was developed in 1948 to assess the manual dexterity and precision of applicants for industrial work and has been used in clinical and research settings for rehabilitation.6,7 The PPT was conducted to examine upper limb control by determining the number of pins that could be inserted in the pegboard holes in 30 s using the dominant hand. The number of pins placed in the pegboard within the time limit represented the test score. The experiment was performed twice and the average value was calculated for each condition. The number of experiments was determined considering the stability and reproducibility of the results, as well as fatigue and motor learning.
In the second test, the effect of wearing an orthosis on ADL was examined; the actions indicated by questions 1 to 18 of the Hand20 8 questionnaire were performed. The Hand20 questionnaire is a 20-item self-reported questionnaire that measures disability and upper limb extremity symptoms. The degree of difficulty of each action was indicated using an 11-point Likert-type scale (0 = no limitation; 10 = impossible) with 0 (no limitation) for performance in the absence of a wrist orthosis. The Hand20 score ranges from 0 to 100, with higher scores indicating greater disability levels. For questions 15, 17, and 18, the participants answered by imagining how much they could do. In addition, participants were asked to report their comfort when the orthosis was worn and ADL was performed.
Stress responses were measured by heart rate variability (HRV), which is used as an assessment method for cardiac autonomic modulation; HRV reactivity serves as an important index of the ability to self-regulate and react to stress in the environment. 9 HRV was measured using a wireless electrocardiograph attached to the chest (wireless biosensor RF-ECG2, GM3, Tokyo, Japan) before and after each experiment. The resulting electrocardiogram was calculated using LabChart 7.0 Software (AdInstruments, Dunedin, New Zealand) to calculate low frequency (LF) components in the 0.04 to 0.15 Hz range and high frequency (HF) components in the 0.15 to 0.40 Hz range. The LF/HF ratio and HF served as indices of sympathetic and parasympathetic nerve activity, respectively. 10 The participants relaxed for 15 min in a quiet, temperature-controlled room and did not smoke or consume caffeine or alcohol for at least 1 h before the tests.
Statistical analyses
In PPT scores, Hand20 scores and HRVs at the start of the experiment, baseline conditions, and those of wearing a padded fiberglass wrist orthosis and thermoplastic wrist orthosis were examined by multiple comparisons and adjusted using Holm’s method. Wilcoxon’s signed-rank test was used to compare HRVs before and after the experiment for each condition. The significance level was set at p < .05.
Results
The median PPT scores for baseline, wearing a padded fiberglass wrist orthosis, and thermoplastic wrist orthosis were 15.5 (interquartile range [IQR] 14.3 – 16.0), 13.5 (IQR 12.3 – 15.0), and 14.5 (IQR 13.8 – 15.5), respectively. The PPT scores were significantly higher when not wearing a wrist orthosis than when wearing a padded fiberglass wrist orthosis (p < .01) and thermoplastic wrist orthosis (p < .01). In addition, participants scored significantly higher when wearing a thermoplastic wrist orthosis than when wearing a padded fiberglass wrist orthosis (p < .01).
Hand20 score.

Data are shown as median (interquartile range).
As for wearing comfort of the padded fiberglass wrist orthosis, 10 participants reported “the padded fiberglass wrist orthosis had a soft surface” and 3 reported it was “easy to move,” while 6 reported “there was a feeling of pressure.” Thirteen participants reported that while wearing the thermoplastic wrist orthosis it was “easy to oppose the thumb” and 6 reported that it was “easier to move because there is less coverage than a padded fiberglass wrist orthosis.”
Heart rate variability.

Discussion
Our study examined the effects of wearing a wrist orthosis made of padded fiberglass or thermoplastic on upper limb function, ADL, and stress responses. The PPT scores were lower when wearing the wrist orthoses compared to when they were not worn. This result is similar to the study of Chang and Jung 11 who used the Jebsen-Taylor hand function test. King et al 12 reported that wearing a wrist orthosis requires a wider range of motion (ROM) of the shoulder joint for effective movement, inhibiting smooth movement of the upper limbs. The examiner’s manual 13 suggests that the Purdue Pegboard measures two types of dexterity, “one involving gross movement of hands, fingers, and arms and the other involving primarily what might be called ‘fingertip’ dexterity.” Therefore, we consider that the wrist orthosis diminished the ability to perform the PPT by increasing the demands on the shoulder for increased range and inhibiting smooth gross movement of the hands, fingers, and arms limbs. In this study, the score when wearing a thermoplastic wrist orthosis was significantly higher than that when wearing a padded fiberglass wrist orthosis. These results suggest that a wrist orthosis reduced upper limb performance due to motor limitations of the wrist joint, while a thermoplastic wrist orthosis had less performance degradation than a padded fiberglass. The thermoplastic wrist orthosis and padded fiberglass wrist orthosis used in this study differed in the shape of the distal side and the method of fixing the orthosis and forearm; these differences may have influenced the difference in performance. The distal side shape of each wrist orthosis is considered to be particularly involved in the movement of the thumb’s carpometacarpal joint; in a thermoplastic wrist orthosis, it is at the thenar transverse crease and in a padded fiberglass orthosis, it is 5 mm proximal to the thumb metacarpophalangeal joint crease. Thumb opposition is necessary for detailed object manipulation, and the thumb and fingers adjust their force vector directions in accordance with the mechanical properties of a grasped object. 14 A padded fiberglass wrist orthosis is considered to cover the carpometacarpal joint on the thumb and restrict opposition, making it more difficult to operate the pegs than when it is not limited. In addition, the method of fixing the thermoplastic wrist orthoses involved a Velcro hook and loop, and for the padded fiberglass wrist orthoses elastic bandages. The Velcro hooks and loops do not cover the joints, while the elastic bandages cover the metacarpophalangeal joints, which may have affected the fine manipulation of objects by limiting finger flexion. Operating speed is important in the PPT. Thumb opposition and finger movement are restricted, and performance degradation is substantial in movements requiring speed.
The results of the Hand20 in this study indicated that wearing a wrist orthosis interfered with ADL because the difficulty was increased in all items of the Hand20 by wearing a wrist orthosis. It has been reported that the ROM of the wrist joint required for ADL is approximately 70%, 15 and the restriction of the wrist joint when wearing a wrist orthosis is expected to interfere with ADL. One of the reasons patients stop wearing orthoses is impediments to ADL, 16 and it is important to reduce the impediment to ADL as much as possible. The results of the Hand20 in this study indicated that compared to wearing the thermoplastic wrist orthosis, it was less difficult to perform action when wearing the padded fiberglass wrist orthosis: “turn on/off the faucet with the affected hand.” A padded fiberglass wrist orthosis has a non-woven pad on the surface, and the softness of the material may allow for slight wrist joint movement during action. Nonetheless, there were negative opinions for wearing a padded fiberglass wrist orthosis and positive opinions for wearing a thermoplastic wrist orthosis; thus, it was not possible to conclude which orthosis was better for performing ADL. An elastic bandage is used with a padded fiberglass wrist orthosis to fix it with the forearm, which takes more time to remove compared to the Velcro hooks and loops. Furthermore, it is necessary to consider that a padded fiberglass wrist orthosis is not suitable for wet work. In this study, the activities of getting wet, such as “wash your face with both hands” and “wash your hair with both hands,” were performed by simulated activities without actually using water. It should be noted that the difficulty of these activities was not affected by the difference in the orthoses, but they did not represent real-life situations.
The LF/HF and HF measures showed no significant differences, indicating that the stress caused by wearing the wrist orthoses was low. The weight difference between the wrist orthoses and the covering area did not affect the stress responses. However, since these data was not measured in real-life situations, further examination is necessary to obtain accurate data.
Some of the wrist orthoses used clinically were not included in this study, and we believe that further research including these is necessary. However, in this study some knowledge was obtained regarding the adaptation to wearing wrist orthoses. There is no consensus on the criteria for determining whether a padded fiberglass wrist orthosis or thermoplastic wrist orthosis should be prescribed when fixing a wrist joint in Japan. The results of this study clarified that a thermoplastic wrist orthosis may be more suitable than a padded fiberglass wrist orthosis when work efficiency or precision work is required. However, wearing a padded fiberglass wrist orthosis was also advantageous over wearing a thermoplastic wrist orthosis for performing ADL. When providing orthoses to patients, we believe that it is important to consider the specific situations in which patients will use a wrist orthosis. However, in addition to the factors examined in this study, other factors determine orthoses’ prescription, such as the viewpoint of medical professionals, ease of molding, and cost. The patient’s viewpoint should also be considered when selecting a wrist orthosis.
This study had a few limitations. First, the orthoses were only worn for the limited time required for the experimentation, rather than in real life. Prolonged wearing may affect the difficulty in ADL and stress responses. Second, we excluded participants with upper limb dysfunctions. Therefore, symptoms such as swelling and pain which can affect the use of orthoses were not considered. Finally, this study only used wrist orthoses that support the palm side; those that support the dorsal side are also commonly used. These conditions should be examined in future studies.
Footnotes
Authors’ Contribution
JH conceived the idea of the study. JH and KI developed the statistical analysis plan and conducted statistical analyses. MY contributed to the interpretation of the results. JH drafted the original manuscript. KI supervised the conduct of this study. All authors reviewed the manuscript draft and revised it critically on intellectual content. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Grants-in-Aid for Scientific Research of Japan Society for the Promotion of Science, Grant Number JP19K19627.
Ethical Statement
Guarantor
JH.