
Abstract
Introduction
Approximately 30% of stroke survivors experience an upper limb impairment, which impacts on participation and quality of life. Gaming devices (Nintendo Wii) are being incorporated into rehabilitation to improve function. We explored the stroke survivor experience of gaming as an upper limb intervention.
Methods
Semi-structured, individual interviews with stroke survivors living within the UK were completed. Interviews were audio-recorded, transcribed verbatim and analysed using Framework methods. Transcripts were coded and summarised into thematic charts. Thematic charts were refined during analysis until the final framework emerged.
Results
We captured experiences of 12 stroke survivors who used Nintendo Wii. Gaming devices were found to be acceptable for all ages but varying levels of enthusiasm existed. Enthusiastic players described gaming as having a positive impact on their motivation to engage in rehabilitation. For some, this became a leisure activity, encouraging self-practice. Non-enthusiastic players preferred sports to gaming.
Conclusion
An in-depth account of stroke survivor experiences of gaming within upper limb rehabilitation has been captured. Suitability of gaming should be assessed individually and stroke survivor abilities and preference for interventions should be taken into consideration. There was no indication that older stroke survivors or those with no previous experience of gaming were less likely to enjoy the activity.
Introduction
Stroke is considered to be a major cause of serious, long-term disability in Europe. 1 Within the UK, hemiparesis affects up to 80% of the estimated 1.3 million stroke survivors 2 and is persistent, with 30–66% still experiencing difficulties with arm movement or function 6 months after their stroke. 3 Stroke upper limb impairment is a top research priority for stroke survivors and healthcare professionals. 4 Intensive, repetitive and functional movements are considered most effective in promotion of recovery 5 and commercial gaming devices (e.g. Nintendo Wii) encourage high repetition of arm movements. 6 Some stroke rehabilitation services have introduced commercial gaming devices to address upper limb impairment. 7 However, little information is available on the stroke survivor experience of this intervention. 8 In order to be able to inform future research and aid health professionals in making clinical judgements about suitability of intervention, optimising adherence and facilitating implementation, it is important to capture the perspectives of stroke survivors.
Celinder and Peoples 9 interviewed nine Danish stroke survivors who played Nintendo Wii within a pilot inpatient rehabilitation programme. The study focused on physical and cognitive rehabilitation and concluded that Nintendo Wii could be used to promote engagement in leisure activities. Wingham et al. 10 interviewed 18 stroke survivors who used Nintendo Wii as part of a home-based upper limb rehabilitation programme. They reported high usage rates within the home and the intervention was found to be acceptable to both stroke survivors and caregivers. Limited information was however captured on factors that influence engagement in upper limb rehabilitation. In addition, Lewis et al. 11 in their literature review (three articles including participants with chronic neurological conditions) concluded that use of virtual reality offered increased enjoyment and motivation compared to traditional rehabilitation. The aim of our qualitative study was to explore whether use of commercial gaming devices for upper limb rehabilitation was acceptable to stroke survivors and to capture their experience of this intervention. A pragmatic stance was taken to this study where investigations are not necessarily aligned to a particular qualitative research method.
Methods
Within this qualitative study a purposive sampling strategy was used to recruit stroke survivors who had used or declined the use of commercial gaming devices for stroke upper limb rehabilitation. A target sample size of 12 stroke survivors was identified, sufficient for interview studies analysing emergent themes. 12 In order to capture a range of experiences, nine stroke survivors who had experienced commercial gaming devices within their rehabilitation and three stroke survivors who declined this intervention were sought.
Recruitment took place via:
Stroke rehabilitation teams over three NHS Boards (responsible body for the provision of health care within a regional area) where therapists screened potential participants from caseloads Stroke clubs and groups (stroke survivors confirmed that they had used gaming as part of their upper limb rehabilitation).
Inclusion criteria were applied: stroke survivors had to be over 18 years of age and have received upper limb rehabilitation (either using or declining use of commercial gaming devices). Stroke survivors had to have capacity to consent and have sufficient communication skills to take part in a research interview (as per recruiting therapist’s observation). Stroke survivors were excluded if they used commercial gaming devices exclusively for other rehabilitation goals, such as improving balance or cognitive rehabilitation. Where gaming had been used, this was required to be in the previous four weeks to facilitate discussion of a recent experience. A participant information sheet and a consent form were posted to potential participants followed by a telephone call to arrange an interview date. Ethical approval was sought and obtained from a proportionate NHS Research Ethics Committee (13/NS/0061) to recruit stroke survivors who had used or declined the use of commercial gaming devices for stroke upper limb rehabilitation.
This study was completed as part of doctoral level studies. All members of the research team are health professionals with experience of qualitative research at masters (KT) or postdoctoral level (AP, CB, MB). The first author has a clinical and research interest in the use of technology within stroke rehabilitation. We referred to the consolidated criteria for reporting qualitative research (COREQ 13 ) to structure the presentation of our study findings.
Data collection
Following informed consent, individual, semi-structured interviews were conducted using an interview guide (Appendix 1) developed from a recent systematic review. 8 Questions included use and experience of gaming device with any issues raised by participants followed up within the interview. The interview guide was piloted with a stroke researcher, small revisions to the wording of questions occurred between the pilot and participant interviews following discussion with the research team. All interviews took place within one session, in stroke survivors’ homes (n = 8), stroke club (n = 2), hospital (n = 1) or via telephone call (n = 1) by the first author (KT, female occupational therapist). The interviewer had experience of conducting both clinical and research interviews. There was no prior relationship with study participants. Participants were informed that the researcher had an interest in the use of technology for rehabilitation. Interviews lasted from 30 to 50 min and were digitally recorded. Open, exploratory questions were used to encourage stroke survivors to answer freely; follow-up questions aimed to obtain a deeper and fuller understanding of the experience. Research memos were written after each interview to capture reflections on the interview process, assumptions made and points that required further discussion.
Data analysis
Framework analysis 14 was used to analyse data, using NVivo 10 qualitative data analysis computer software package 15 to assist with data management and the analysis process. Framework analysis involves several key stages including familiarisation, identifying initial themes, sorting themes and summarising data into thematic charts before moving on to detecting patterns and developing explanations. 16 Framework analysis was selected as the most appropriate method for data analysis as use of a structured system provided guidance for a novice researcher on the stages of data analysis, whilst not stifling the freedom required for creativity within the process. Framework analysis can assist in developing skills required for robust, transparent qualitative data analysis. 17 Interviews were transcribed orthographically (KT) and re-checked for accuracy following transcription against the audio file (KT). This initial stage also involved re-reading study information including the study protocol and research memos, a step described by Ritchie and Spencer 14 as familiarisation. Due to study time constraints, transcriptions were not returned to participants for checking. Following transcription, each interview text was read from start to finish with sections highlighted, which were grouped into common themes. This process was completed in a chronological fashion to ensure that all sections of text were considered. Themes were grouped under headings (or categories) as a first draft; this process was reviewed and repeated as additional transcripts were coded. Categories were reviewed with areas of overlap identified and themes merged or renamed. All initial themes were iterative although it is acknowledged that use of an interview guide influenced aspects of gaming discussed during interviews.
Preliminary coding was completed by the first author (KT), the second author (AP) reviewed this by reading the first three transcripts together with initial themes and categories. Changes were made to both themes and categories following feedback. After four transcripts had been coded an initial conceptual framework was created in NVivo 10 and exported into a Microsoft Excel workbook. The framework was reviewed by study authors and refined following discussion. The framework was then applied to raw data from the additional nine transcripts, a process described by Ritchie and Spencer 14 as indexing. Data were not discarded if they did not fit the conceptual framework or appear to meet the objectives of the study; instead data were kept and referred to throughout analysis. It was acknowledged that these data could take on new meaning as the data analysis progressed. 18
The next stage of data analysis was the creation of thematic charts. Using index categories and themes data were grouped together and summarised into a Microsoft Excel workbook. The initial stages of the data analysis process were considered to be the descriptive phase where analysis moved from looking at individual transcripts to a description of the full data set.
In preparation of descriptive accounts, the content and nature of themes were unpacked. By deconstructing themes, the meaning was fully examined. During this process, themes were explored from different angles by questioning the data. Different accounts were constructed and new insights emerged as data were mapped. This process was repeated a number of times until all themes were exhausted and no new information discovered.
Labels were assigned to text that moved away from the original wording as interpretation of data took place by the first author. The final stage of data analysis was the explanatory phase, where we attempted to interpret and create meaning from the dataset, as the final framework emerged. An explanatory account was developed, as summaries from each participant were recorded and a main pattern in the data was identified regarding types of player (enthusiastic and unenthusiastic).
Findings
We recruited 12 stroke survivors to the study (Figure 1), of which all had used a commercial gaming device as part of their upper limb rehabilitation. No stroke survivors who had declined gaming use consented to take part in the study.

Number of participants recruited to study.
Participants
Interviewees (9/12 male) ranged in age from 45 to 71 years old (Mean age 59, SD = ±7.6). At the point of interview, the length of time post stroke ranged from 2 months to 6 years (Mean months 17.3, SD = ±25.5). Stroke survivors recruited were predominantly new to gaming (9/12) and were classified as ‘new to gaming’. Those who had played gaming prior to stroke were classified as ‘gaming pre-stroke’. Half of stroke survivors (6/12) interviewed owned their gaming device. Others had received equipment on loan from rehabilitation services or used it within therapy sessions (Table 1).
Participant characteristics.

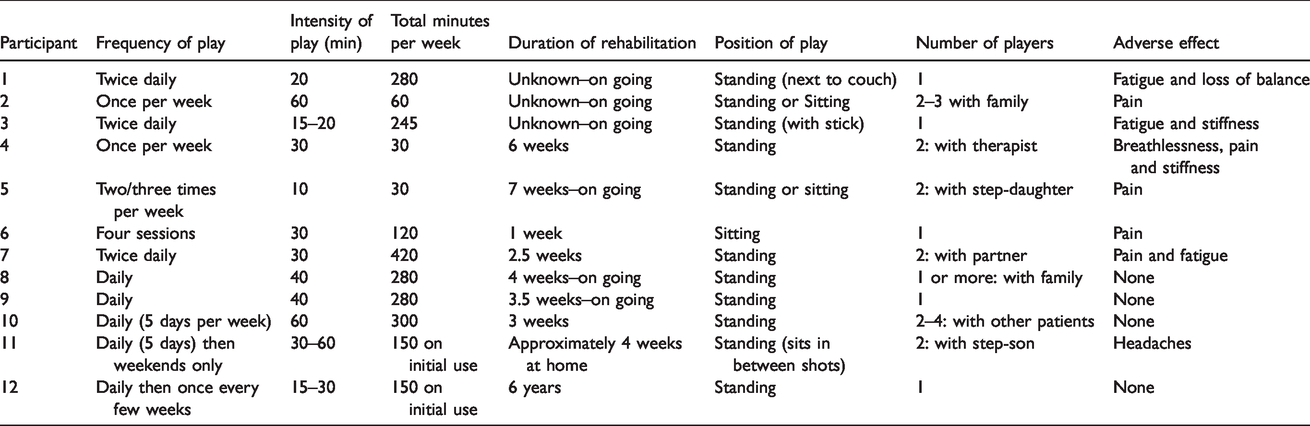
All stroke survivors used Nintendo Wii gaming device with Wii Sports, Play or Resort. In addition, three stroke survivors also used an iPad with games downloaded from App Store, which included balloon burst and word searches. Most treatment sessions were reported to take place unsupervised, with stroke survivors asked to play commercial gaming devices out with therapy led rehabilitation sessions. Detailed information on gaming use (as reported by participants) is presented in Table 2.
Pattern of commercial gaming device use.
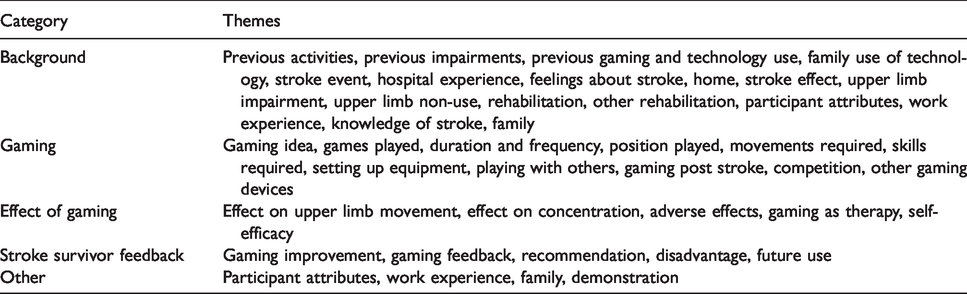
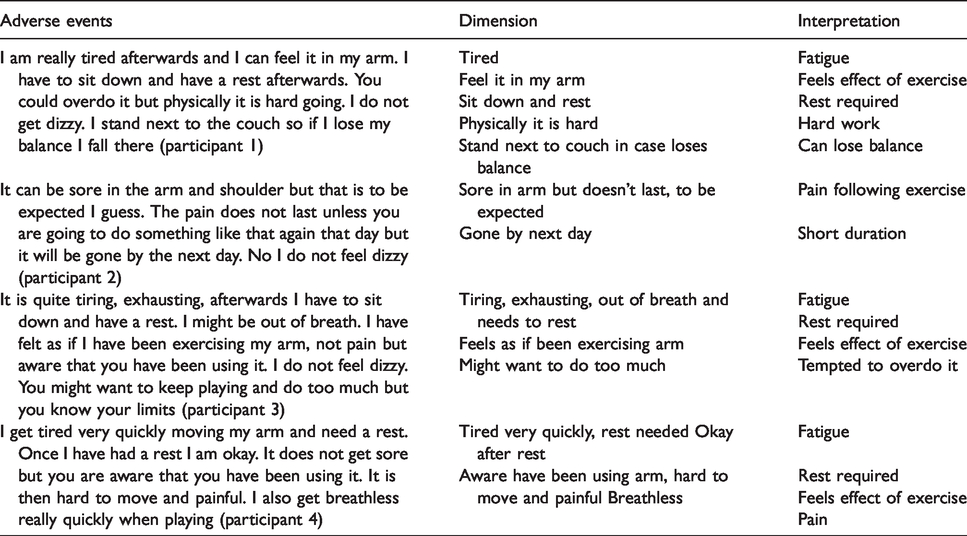
During the data analysis process an initial conceptual framework was created from identified themes and categories (Table 3). The next stage of data analysis was the creation of thematic charts (see Table 4 for an example). Labels were assigned to text that moved away from original wording as interpretation of data took place by the first author (see Table 5 for an example of interpretation). The relationship between emergent themes and subthemes were illustrated visually (Figure 2).
Initial conceptual framework.
Example of thematic chart.

Example of Interpretation.

Stroke survivor experience of gaming—overview of themes.
All stroke survivors commenced playing commercial gaming devices with the purpose of upper limb rehabilitation; however, some stroke survivors described a shift in focus, playing with the purpose of entertainment. Rehabilitation and entertainment formed two principal reasons why participants engaged with gaming. Five themes emerged from the categories of rehabilitation and entertainment including gamification, leisure activity, sports, relationships and innovation (Figure 2). In addition, four sub-themes were identified; three were from gamification (success, mastery and competition) and one from leisure activity (normalisation). Some players were identified as enthusiastic players whilst other appeared unenthusiastic about the use of commercial gaming as a stroke upper limb intervention.
Enthusiastic players
Enthusiastic players enjoyed playing commercial gaming devices and described the experience with terms such as ‘fun’, ‘fantastic’ and ‘brilliant’. They described becoming immersed in gaming and forgot they were exercising. On occasion enthusiastic players reported that they would play for longer than initially planned; only stopping when they felt physically tired from exertion. From 12 stroke survivors interviewed (who had used commercial gaming devices), 10 were classified as enthusiastic players. Of this group three players changed their purpose of play from rehabilitation to entertainment.
Unenthusiastic players
Unenthusiastic players only used commercial gaming devices on their therapists’ instruction. They tended to play only during therapy sessions or for short periods of time and reported that they preferred other rehabilitation activities (such as robotic therapy). They described gaming as ‘alright’ or ‘okay’ and identified that they were happy to stop playing at the end of their rehabilitation programme.
Entertainment
Two themes were identified from the category of entertainment (relationships and leisure activity), which contributed to stroke survivors’ sense of entertainment.
Relationships
Stroke survivors who primarily played gaming as entertainment identified that a key aspect of using commercial gaming devices was that family and friends could also share this experience. Commercial gaming was considered to be a social activity and stroke survivors actively involved their spouses, children and other family members within their rehabilitation. For one stroke survivor the opportunity to share this experience with children in the family became the primary purpose of sessions and encouraged interaction.
Sometimes I play with my niece’s son, we play ten-pin bowling. He knows how to play but he won’t tell me. My niece’s daughter will say it’s my shot, it’s my shot. My family has all been in, they’ve all tried it. I have managed three at the tennis and my niece’s daughter has made three too. The kids made my mini mii, it was good fun. I only play with the kids. (P2 (Participant 2), new (to gaming), enthusiastic (player)
Leisure activity
The use of commercial gaming devices became a leisure activity for some enthusiastic players. These players were confident they would continue gaming following rehabilitation and were in the process of purchasing their own equipment.
I’ve got friends that will play with the Wii, and they are round, and instead of playing cards like we used to do or playing board games, they will play a game of golf with the Wii. And I mean it will be a needle
a
match, with probably bets on the side. So eh I mean they will probably even have side bets on you know, 10p a point, who gets on the green first this sort of stuff. So I mean you could actually, you could turn it into something absolutely marvellous in terms of the entertainment. You could spend all night playing, and eh from my point of view, the only hazard I would be playing left handed, they are all playing right handed so I am at a disadvantage there. (P8, new, enthusiastic)
Normalisation (subtheme of leisure activity)
Some stroke survivors identified that playing commercial gaming devices felt like a normal activity compared to other rehabilitation interventions. “It was a very useful way of bringing therapy sort of, make therapy less sort of medicinal if you like, so it’s a way of making therapy more of a kind of normalising it in a way” (P10, new, enthusiastic).
Stroke survivors reported that they enjoyed the social interaction that the games offered and found that it provided a topic of conversation. As a result, it lifted the mood of those playing and offered variety within rehabilitation programmes.
The best thing about the Wii in that place was you felt normal, you just felt to be a part of a group, where before the Wii came in, there wasn’t much like conversation or that, so that helped because I have aphasia, so after the Wii came in they were all talking about it. It lifted the mood of the place you know and it gave people something to talk about so no, I felt great after it as a said before I felt normal. I know that sounds silly but I did, I felt normal. (P12, new, enthusiastic)
Gamification
The concept of gamification aims to engage players through both challenges and rewards to increase engagement and encourage further play. 19 Enthusiastic players expressed a desire to play and a number of factors (mastery, competition and success) contributed to this. Unenthusiastic players did not express any feelings of mastery or success but they reported that competition could be an incentive to play for others.
Mastery (subtheme of gamification)
Gaming posed a challenge for stroke survivors; games were not easily mastered and were not specifically designed for rehabilitation. They were however considered to be achievable and within the capabilities of stroke survivors. Goals that offer challenging tasks but are achievable can have a positive impact on motivation to engage in rehabilitation. 20 Stroke survivors identified a number of tasks that they found challenging, including grasping the Wiimote (controller), pressing buttons on the front and back simultaneously and having the co-ordination and sense of timing required to release the buttons at the right time. “I had to persevere with some of the Wii games (tennis), I couldn’t hit it at all to begin with, it takes a while, and you have to persevere” (P1, gaming pre-stroke, enthusiastic).
Enthusiastic players expressed a determination to achieve mastery, acknowledging that perseverance was required. The range of games available meant that different movements were practiced during different games. The games also required a variety of skill levels with stroke survivors classifying some games as easier than others. Bowling was reported as a good starting point with many stroke survivors commencing their rehabilitation with this game. Tennis was viewed as more challenging and was therefore seen to offer progression to another level of play. Stroke survivors reported that the more they practiced, the better their game play became and their scores improved.
Success (subtheme of gamification)
Enthusiastic players also enjoyed a feeling of success when participating in commercial gaming and this contributed to feelings of self-worth and encouraged further play. “After playing I am tired and out of breath but I feel as if I have done something positive towards my recovery” (participant 3, gaming pre-stroke, enthusiastic player).
The feedback that games provided also appeared to contribute to feelings of success.
When you get a strike and you get all the pins going down there is that wee feeling of elation. I think the way it is set up for us at the moment you are really just playing yourself, playing against the machine. It’s like all of these wee games that we have got on the iPad as well. You are trying to beat your best score but it’s amazing because you are playing against the opponent but you don’t know his capabilities and it’s quite good. (P8, new, enthusiastic)
Competition (subtheme of gamification)
Commercial gaming is designed to promote competition,
19
which had a positive impact on stroke survivors’ motivation to play. Most enthusiastic players described themselves as competitive and enjoyed beating their high score. Gaming included competitive elements in a number of formats; one example is stroke survivors beating their own high score or playing against friends and family.
I want to play good so it gives you an interest in trying to get a good score. Competition is important, I have a high score that I try to beat, it’s not the main purpose of using the Wii but it gives you an added incentive. (P3, gaming pre-stroke, enthusiastic)
Well I am competitive anyway so the score alone. I’ve always been competitive. I’ve played a lot of sport and all that so it’s me trying to beat my score will encourage me to go back to it you know. I’ll say Right I will go back to that and see if I can beat what it was the last time, well only if you get beat, if you get beat, I don’t like that part, we will be playing it over Christmas and I will be winning the bowling [laughs]. (P 9, new, enthusiastic)
Sports
Many of the games played had a sports focus such as bowling, tennis or golf. Some of the stroke survivors (both enthusiastic and unenthusiastic players) described themselves as sports enthusiasts, highlighting that they enjoyed both watching and playing sports. The use of gaming offered the opportunity to replicate a sporting experience in a virtual sense. In addition, stroke survivors felt that their sporting expertise assisted game play.
I think it’s a fantastic idea, it gives people an interest. The games are quite good. You can play in your own home any time. You don’t need to be a professional. Golf is great. It’s more for people who have done sports before. For me it’s more natural, playing sports helped. (P2, new, enthusiastic)
I played golf at the golf course, I didn’t use that [Wii], I went to the golf course to play golf which I can’t do now but I have given myself a year and I will be playing golf in a year. (P4, new, unenthusiastic)
It’s so realistic. You would honestly think you were playing, I mean we have all played ten pin bowling and you know just that idea of trying to get your finger out the hole in the ball and releasing the ball, now that same action is there in the Wii. It’s so realistic that it’s believable, you actually feel as if you are taking part in a game. (P8, new, enthusiastic)
Innovation
The use of commercial games is not new within stroke upper limb rehabilitation 21 but was seen as something new for stroke survivors, which they described as an innovation in practice. This innovation was seen as something different that rehabilitation had to offer and was viewed in a positive way by enthusiastic players. “It’s all new technology, I suppose it’s why it hasn’t been used because it is new isn’t it and everybody is just getting used to it now” (P9, new, enthusiastic).
It was also viewed as something modern, using up to date technology. “I felt a part of this century” (P12, new, enthusiastic).
Only one stroke survivor interviewed identified that commercial gaming devices had potential for their upper limb rehabilitation prior to it being offered by their therapist. Most stroke survivors expressed surprise at being offered commercial gaming as a rehabilitation intervention, including those who had previously played gaming devices.
The occupational therapist when she saw the Wii suggested using it. I think it is a good idea, not one I would have thought of but I can feel the benefit of using it. When the occupational therapist saw the Wii fit she said we would get that up and running too. I was going to give it away a few months ago cos it was lying here and I says to a guy. He’s never been over for it so he can’t be wanting it that bad. So I am glad that I kept it, it’s just as well. (P1, gaming pre-stroke, enthusiastic)
At first I thought oh God no I mean it’s, how the hell am I going to use it, I mean it’s for kids that’s what I thought oh gosh, it’s for, it’s a game, it’s something for kids but it’s not, it’s for universal age, it doesn’t matter as I say 90 year olds played it. (P12, new, enthusiastic)
Commercial gaming as an acceptable intervention
All stroke survivors interviewed stated they would recommend the use of commercial gaming devices to other stroke survivors as a rehabilitation intervention. The use of commercial gaming devices can therefore be considered as an acceptable intervention for stroke upper limb rehabilitation.
I would recommend it (the Wii) for anyone who is having trouble with their hand, arm, shoulder, anything like that. I would recommend it for the repetitive movements, doing the same movements all the time, I think it’s good. (P3, gaming pre-stroke, enthusiastic)
Adverse events
Most stroke survivors interviewed did not volunteer information on adverse events; instead this information was captured via probing questions. Most stroke survivors (n = 8) described adverse events including fatigue, muscle pain, breathlessness, headaches and a fear of losing balance whilst standing. Although a number of adverse events were identified this did not prevent any stroke survivor from continuing their rehabilitation using this intervention. One stroke survivor did however attribute their adverse event (headaches) to the amount of concentration required to play one game (Jet Ski) and changed game. Other stroke survivors attributed their adverse events to playing for too long and using their arm more.
Summary
This qualitative study gathered in-depth experiences of 12 stroke survivors who engaged with commercial gaming devices as part of their upper limb rehabilitation. This study identified that the use of gaming devices for upper limb practice is acceptable to stroke survivors. It was also found that varying levels of enthusiasm exist for gaming as a rehabilitation intervention, which has implications for implementation within practice settings. For those that were enthusiastic in gaming had a positive impact on their motivation to participate in upper limb rehabilitation. Enthusiastic players described being immersed in the activity, which they enjoyed playing with family and friends and for some this became a new leisure activity, which they intended to continue playing beyond their rehabilitation programme. Competition, mastery, feelings of success and use of sports related games encouraged stroke survivors to play for longer, return to play and share this experience with others. Within practice, it may be beneficial for therapists to consider if stroke survivors previously enjoyed sports when determining suitability for individual stroke survivors. In addition, involvement of family and friends in gaming sessions may increase motivation to engage in upper limb rehabilitation.
Findings in relation to previous research in this field
Other studies that have considered the stroke survivor experience of playing commercial gaming devices9–11 have also found that gaming has a positive impact on motivation and engagement in upper limb rehabilitation. The entertainment value of gaming, leading to a desire to continue use is similar to the findings of Fager and Burnfield 22 In their phenomenological study including 10 participants a desire to engage in further rehabilitation (using assistive technology) beyond traditional programmes was noted, which offers potential for the development of self-management programmes. Future research should consider the potential of using gaming devices as a self-management tool together with possible barriers to service delivery (for example time taken to set up the gaming device) within stroke survivors’ homes. In addition, the involvement of family members or friends within gaming sessions warrants further exploration.
The key components of gaming, which seemed to encourage play, were mastery, success and competition, these were labelled under the theme gamification. Similar components were identified in a number of studies that have considered engagement levels of stroke survivors using virtual reality during upper limb rehabilitation such as Burke et al., 23 as well as being identified as key criteria for effective stroke rehabilitation overall. 24
Not all stroke survivors were enthusiastic about use of commercial gaming devices for stroke upper limb rehabilitation and preferred undertaking real rather than virtual activities. These stroke survivors played for shorter periods of time (potentially receiving less therapeutic benefit) and only at their therapists’ request (rather than for their own enjoyment). Other studies have also found a preference for traditional rehabilitation such as Laver et al., 25 who captured qualitative data as an adjunct to a randomised control trial. They concluded that participants preferred traditional rehabilitation compared to use of Nintendo Wii Fit. 25
Limitations
An a priori sample size of 12 stroke survivors was declared in the research protocol. This number of interviews may not have been sufficient to gain a full account of the stroke survivor experience; however, no new information was gained from the final interview and responses gained provided sufficient depth and range for an explanatory account to develop.
Recruitment challenges were experienced within this study. Whilst every attempt was made to recruit stroke survivors who had declined use of a commercial gaming device this was unsuccessful. This may have been due to stroke survivors being unwilling to discuss reasons for declining an intervention. As a result, a full range of opinions regarding gaming devices may not have been captured, limiting our insight and presenting a bias towards technology users; however, both positive and negative opinions were evident within data captured. Unenthusiastic players also appeared to have difficulty expressing what they disliked about this intervention. Unenthusiastic players may have identified the author as a healthcare professional (from the style of interview and language used), which may have reduced their willingness to express dissatisfaction with a rehabilitation intervention. We did not gather information on participants’ upper limb function as a criterion for gaming access. Use of gaming as a rehabilitation intervention was a pragmatic decision by the treating therapists. We acknowledge that the severity of upper limb impairment may, for some participants, have impacted on their enjoyment or adherence to gaming.
In addition, one researcher analysed transcribed interviews into themes, which could have introduced researcher bias, however a number of actions were taken to overcome this. Coded text, interview transcripts and research memos were reviewed and discussed by the authors. Qualitative data analysis does however involve interpretation of data and it may be that (despite processes used) findings have unconsciously been influenced by the author’s beliefs concerning this intervention.
Study strengths
This qualitative study has captured and analysed data from 12 stroke survivors who chose to engage with commercial gaming devices as a stroke upper limb intervention. Our qualitative study appears to be one of the first to have identified the level of enthusiasm as influential for commercial gaming in relation to both gaming use and within rehabilitation programmes. The experiences described provide insight into the length of time stroke survivors engaged in gaming sessions unsupervised at home and the factors that influence engagement.
Conclusion
We have provided an overview of the stroke survivor experience of using commercial gaming devices for stroke upper limb rehabilitation. Experiences from stroke survivors who chose to engage in gaming indicated that commercial gaming devices are considered to be an acceptable intervention for stroke upper limb rehabilitation, regardless of stroke survivors’ age, previous gaming experience or technology use.
Varying levels of enthusiasm for commercial gaming devices as a rehabilitation intervention were evident, which may have implications for stroke survivor engagement in rehabilitation programmes. Enthusiastic players described being immersed in this activity, which had a positive impact on their motivation to participate in upper limb rehabilitation. Use of commercial gaming devices therefore offers potential as a useful and acceptable means of improving intensity of practice for stroke upper limb practice.
Clinical messages
Use of commercial gaming devices for stroke upper limb rehabilitation is considered to be an acceptable intervention but varying levels of enthusiasm exist. Enthusiastic players described gaming as having a positive impact on their motivation to engage in upper limb rehabilitation. There was no indication that older stroke survivors or those with no previous experience of gaming were less likely to enjoy the activity.
Footnotes
Declaration of conflicting interests
Alex Pollock, Marian Brady and the Nursing, Midwifery and Allied Health Professions (NMAHP) Research Unit are supported by the Scottish Government Health and Social Care Directorate’s Chief Scientist Office. The work presented here represents the view of the authors and not necessarily those of the funding bodies. Carol Bugge reports no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
KT
Contributorship
KT researched literature, conceived the study and recruited participants. All authors were involved in protocol development, gaining ethical approval and data analysis. KT wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
We would like to acknowledge the people who participated in this study.