
Abstract
Background and purpose
Upper limb dysfunction is a prevalent challenge post-stroke, necessitating innovative rehabilitation approaches. This pilot study evaluated the usability and feasibility of a novel multimodal virtual reality (VR) rehabilitation system that integrates an automated functional test for the hemiparetic upper extremity (FTHUE) assessment with personalized, task-oriented training in a clinical setting.
Methods
The single-center, parallel-group pilot trial was conducted at the Rehabilitation Hospital of Fujian University of Traditional Chinese Medicine. Ninety-eight individuals were screened, from which 15 occupational therapists (mean clinical experience: 3.87 ± 4.84 years) and 15 stroke patients with mild upper limb impairment (Fugl–Meyer assessment score: 56.00 ± 5.25) were recruited. The intervention (a 1-hour hands-on VR session) was consistent across all participant groups, which incorporated neuroplasticity-based principles to deliver integrated sensorimotor training and multisensory feedback. Usability was evaluated using the system usability scale (SUS) and a custom-designed questionnaire.
Results
All recruited participants completed the evaluation and were included in the analysis. Both groups exceeded the established usability threshold (SUS > 68). Therapists achieved a mean SUS score of 72.00 ± 6.69 (33% scoring ≥ 70) and patients scored 73.00 ± 7.69 (47% scoring ≥ 70). On the custom questionnaire (max 50), therapists scored 20.20 ± 2.74 and patients 19.20 ± 1.26. Therapists rated training enjoyment highest, exceptionally .superior to conventional therapy”u(4.47/5), while patients most valued ease of operation (4.20/5). No adverse events occurred during the trial.
Conclusions
The VR system demonstrated good usability and was well-accepted by therapists and patients. Integrating automated assessment with personalized training shows promise as a complement to conventional rehabilitation. These findings, while promising, require confirmation in a larger definitive trial. Future work should optimize adaptive difficulty mechanisms and explore implementation in community and home settings.
Trial registration
Chinese Clinical Trial Registration Center, ChiCTR2200060214. Registered May 22, 2022. https://www.chictr.org.cn/bin/project/edit?pid = 170137.
Introduction
According to the Global Burden of Disease (GBD) 2021 study, stroke remains the second leading cause of death worldwide, responsible for approximately 7 million fatalities, and the third leading contributor to disability-adjusted life-years (DALYs), with over 160 million lost. 1 While advances in acute care have increased survival rates, many stroke survivors experience lasting motor and cognitive impairments that substantially reduce quality of life and pose a considerable long-term socioeconomic burden. 2
Stroke rehabilitation aims to restore motor function through neural reorganization. Evidence confirms that task-oriented training within enriched environments enhances motor learning. 3 Virtual reality (VR) has emerged as a promising tool for upper limb recovery due to its ability to create immersive environments with high ecological validity reality (VR) has nt to which virtual environments accurately reflect real-world functional tasks that patients perform in daily life—enabling patients to engage in repetitive, functional activities within these settings safely. By presenting dynamic scenarios that require real-time decision-making, this approach aims to improve patients’ strategic cognition (i.e. the ability to plan and select effective motor strategies during task execution) and behavioral flexibility (i.e. the capacity to adapt movement patterns based on real-time feedback and task demands), thereby facilitating motor relearning, enhancing engagement, and promoting the transfer of acquired skills to daily living. Although VR-based rehabilitation can improve upper limb function and activities of daily living (ADL)—(ADL)apacity to adapt movement patterns based on real-time feedback and task4–6—(ADL)apacity to adapt movement patterns based on real-time feedback and task demands), thereb.7,8 Novel strategies, such as combining VR with non-invasive brain stimulation or developing home-based protocols, may help overcome the current plateaus in treatment efficacy.9,10
A significant theoretical foundation has been laid by Maier et al., who identified 15 motor learning principles (e.g. task-specific practice, multisensory input, adaptive progression) crucial for effective VR design. 11 Protocols incorporating these principles demonstrate improved functional outcomes and neural reorganization. 3
Nonetheless, current VR systems face four major limitations: lack of personalization, poor integration of upper limb and hand training, reliance on subjective assessments, and absence of automated, standardized functional assessment integration—such as the Functional Test for the Hemiplegic Upper Extremity (FTHUE-HK).12,13
This study introduces a multimodal VR system that intelligently integrates FTHUE-HK assessment with personalized adaptive training, forming a closed-loop evaluate-train-reevaluate workflow to address these gaps. A key innovation of this study is its dual-perspective approach, incorporating feedback from therapists and patients to evaluate system usability and acceptance comprehensively.
Thus, this research aims to validate the usability and feasibility of this integrated system within a clinical setting, from both therapist and patient perspectives, offering a promising complement to conventional stroke rehabilitation.
Methods
Part I: system description
Overall framework and workflow of the system
The VR rehabilitation training system consists of software and hardware. The hardware comprises a computer, an HTC VIVE Pro Eye VR headset (HTC Corporation, Taiwan, China), and an Azure Kinect DK sensor (Microsoft Corporation, Redmond, WA, USA). The software comprises data processing, peripheral communication, and an interactive interface module. The entire system uses the development environment of Visual Studio 2019 and the sensors of the Azure Kinect SDK for operation. 3Dmax and Unity 3D are used to build scenes and characters, and Kinect motion gesture recognition are used to transmit the patient's instructions to the scene for training.
The system workflow is as follows: data acquisition and motion tracking of the patient's motion information is carried out through Kinect, and feature extraction and gesture recognition are carried out to achieve the patient's control of the target in the virtual scene game. The game platform has also become a source of visual feedback for patients, who can directly see their rehabilitation training process. See Figures 1 and 2 for details.
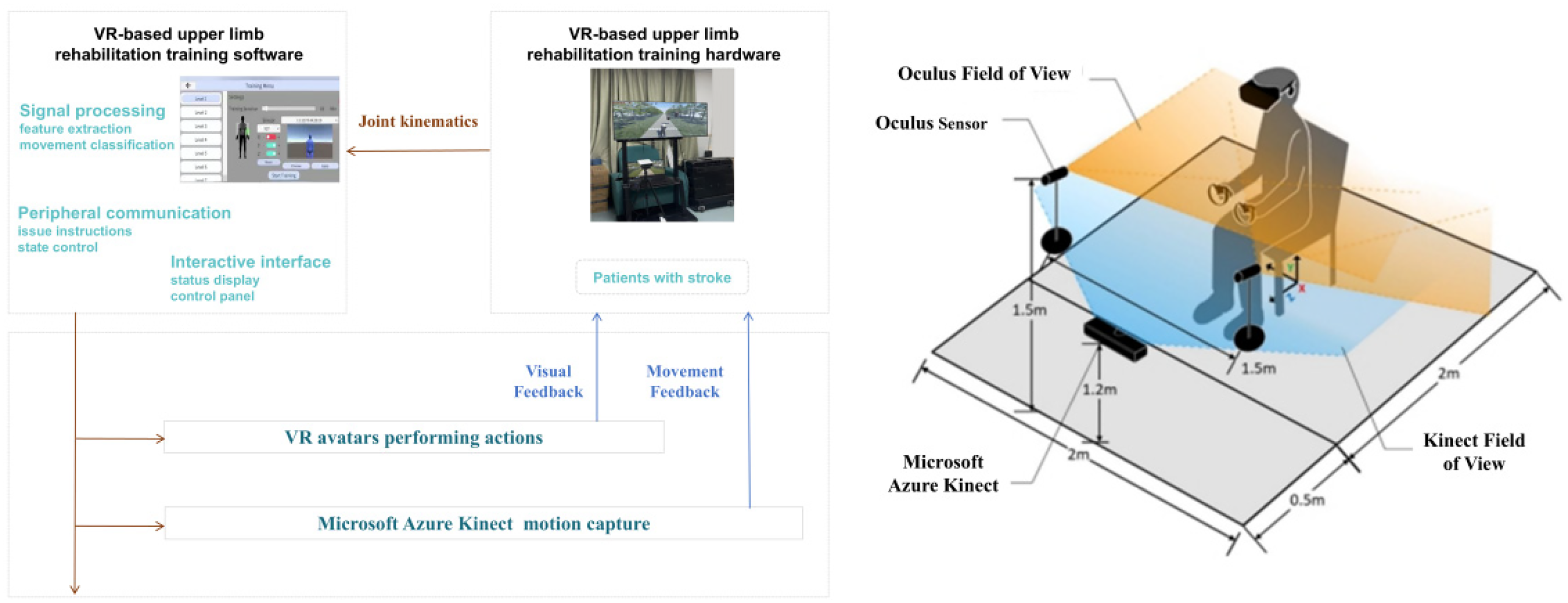
System framework diagram.
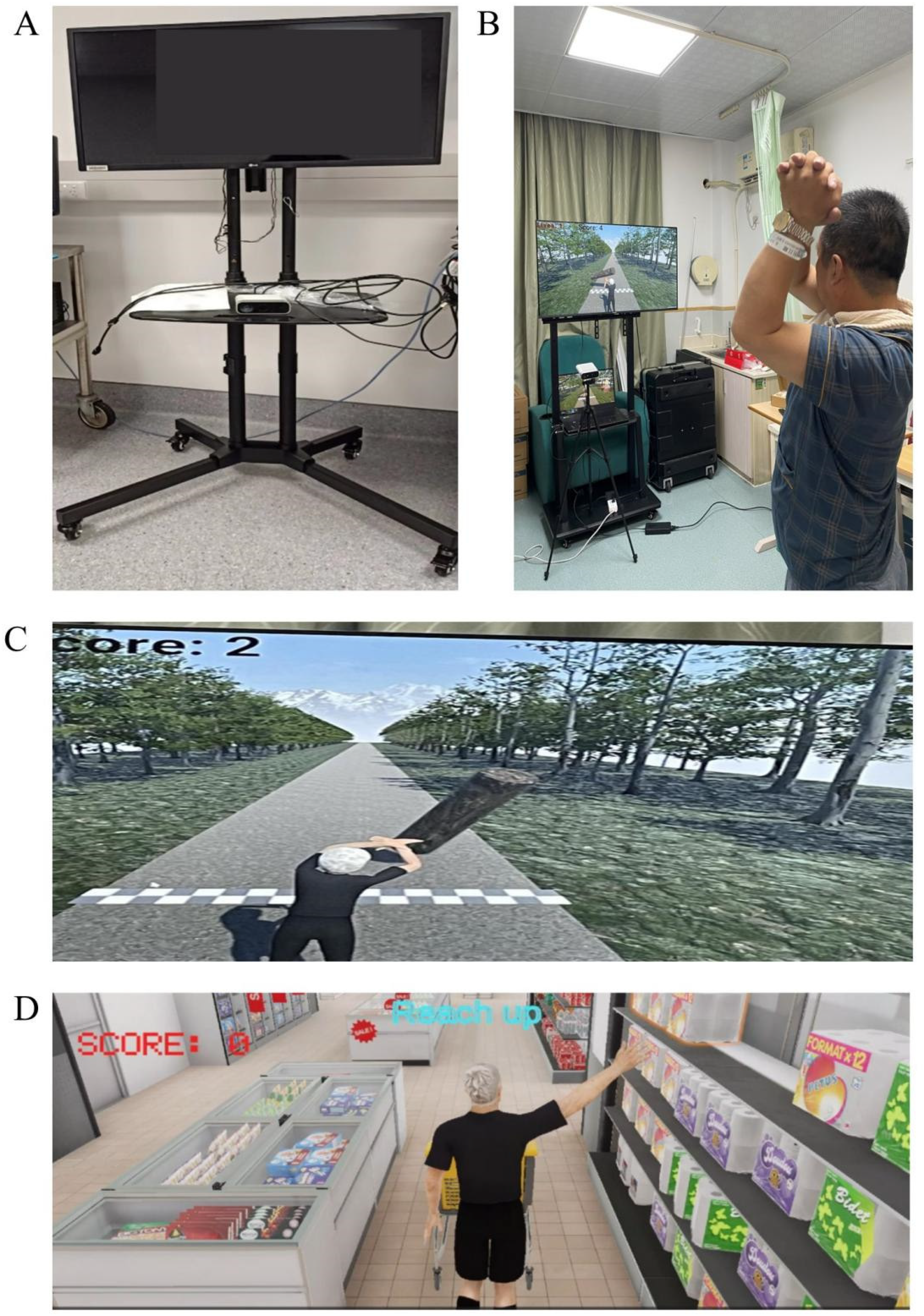
Clinical application scenarios of the system. (A) System hardware. (B) Real-world implementation scenarios. (C) System software interface 1. (D) System software interface 2.
A dedicated data processing and analysis pipeline has been implemented to ensure accurate motion tracking and feedback. Raw skeletal data captured by the Azure Kinect DK is first filtered using a fourth-order Butterworth low-pass filter (cut-off frequency: 5 Hz) to eliminate high-frequency noise. From the filtered data, key kinematic features are extracted in real-time, including upper limb joint angles (e.g. shoulder flexion/abduction), velocity, acceleration, and movement smoothness (jerk). Gesture recognition is achieved using a rule-based classifier, where specific joint angle combinations exceeding predefined thresholds for a sustained duration (e.g. 200 ms) are classified as intentional motions.
Calibration and safety protocol
A comprehensive safety-centered protocol is integrated into the system to ensure measurement consistency and user safety.
Calibration and sensor alignment
Unlike systems that require explicit user-driven calibration procedures (e.g. striking specific poses), our system leverages the Azure Kinect SDK's robust built-in calibration and continuous self-correction mechanisms. The depth and RGB sensors are factory-calibrated, and the SDK's skeletal tracking algorithms perform real-time sensor fusion to maintain high tracking accuracy without user intervention. This approach simplifies the user experience and is particularly suitable for patients with limited mobility in clinical settings. The system initialization automatically loads these calibration parameters to ensure immediate and consistent tracking performance across sessions.
System latency and responsiveness
System latency is a critical factor for immersion and safety in VR. The end-to-end latency of our system was rigorously measured. This includes the time for sensor data capture, skeletal tracking computation by the SDK, avatar scaling and rendering logic, and final display output to the VR headset. The mean latency was found to be 55 ms. 14
Safety measures
Patient safety is paramount, and our multi-layered safety protocol incorporates continuous therapist supervisionorously measured. This includes the time for sensor data capture, skeletal tracking computation visual or auditory warnings as the patient approaches physical limits, as well as unrestricted access to a designated seated resting area within the virtual environment at all times, ensuring the patient can pause immediately if fatigued or uncomfortable. This integrated approach guarantees the system's accuracy and reliability while ensuring safety across diverse rehabilitation populations.
Training game and scene design
The training tasks and games are designed according to the FTHUE evaluation scale and rehabilitation program. The training must be simple, close to daily life, and suitable for older adults. The tasks are intended to train the movement ability of the patients’ shoulders, elbows, wrists, fingers, coordination, and reaction ability. Metrics such as task completion time, motion trajectory, and performance score are recorded. Since patients may have weak upper limb muscle strength, the unaffected limb is allowed to assist the affected limb during training.
Based on Unity3D and 3DMAX software, the rehabilitation scene is constructed according to the FTHUE training tasks. Patients receive multisensory proprioceptive feedbackware, the rehabilitation scene is constructed according to the FTHUE training tasks. Patientsbilitation training scene is designed to simulate a familiar daily living environment, incorporating typical actions to stimulate patient engagement.
The system guides patients through menu navigation and task execution using 3D virtual character animations that demonstrate each task beforehand. Real-time visual and audio feedback is provided, including trajectory error prompts, hand rotation guidance, and reminders regarding motion speed, elbow extension, and compensatory torso or shoulder movements. Auditory alerts and stimulus sounds are used to enhance attention and encourage efficient performance. Task difficulty can be adjusted by modifying parameters such as object distance, height, speed, sequence predictability, or accuracy requirements.
Kinematic data—including speed, completion time, postural errors (e.g. compensatory motions), and trajectory accuracy, postural errors (e.g.using 3D virtual character animations that demonstrate each task b's movement trajectories with ideal reference paths to provide constructive feedback. Therapists remain present throughout the session to manage and adjust the virtual environment according to the patient's performance and discuss results afterward. Patients interact in real time by controlling avatars through their movements and manipulating virtual objects, with possibilities for multi-user interactions such as passing a ball.
Part 2: usability evaluation of an upper extremity VR rehabilitation system
Participants
Between September and December 2024, we recruited rehabilitation therapists with therapist certification and stroke patients who met specific criteria to participate in the usability evaluation of the new system at the Rehabilitation Hospital Affiliated to Fujian University of Traditional Chinese Medicine. Patient inclusion criteria: (a) unilateral hemispheric stroke diagnosis; (b) age between 20 and 70 years; (c) ability to understand instructions and provide feedback verbally. Exclusion criteria: (a) presence of serious medical problems or comorbidities that may affect upper extremity function or cause severe pain; (b) speech and language dysfunction; (c) cognitive dysfunction. The rehabilitation therapists participating in the evaluation in this study were required to meet the following inclusion criteria: (a) hold a valid practicing certificate as a rehabilitation therapist; (b) have at least 1 year of clinical experience in stroke rehabilitation; (c) have no prior experience using the VR system employed in this trial.
This study was approved by the Institutional Review Board of Fujian University of Traditional Chinese Medicine Rehabilitation Hospital (2022KY-006-01). Potential participants were identified through hospital records and referrals from treating physicians. Eligible rehabilitation therapists and stroke patients who met the specific inclusion criteria were provided with detailed information about the study's purpose, procedures, potential risks, and benefits. Written informed consent was obtained from all participants prior to their involvement in the study. All methods were performed in accordance with the Declaration of Helsinki. The study protocol was conducted following the CONSORT extension statement for randomized pilot and feasibility trials.
Study design and implementation
This study is a single-center, parallel-group feasibility, and usability pilot trial. Participants were allocated to the intervention or control group in a 1:1 ratio. The primary objectives are to evaluate the feasibility of the trial procedures and the usability of the system, not to establish its clinical efficacy. This report follows the CONSORT extension statement for randomized pilot and feasibility trials. This study collected demographic data and patient clinical information (stroke type, side of lesion, time of onset) from rehabilitation therapists and stroke subjects. The primary purpose of including therapists was to collect their feedback on the patient's experience with the new system's operation, usability, and clinical applicability. Patients’ upper extremity motor function was measured by the Fugl–Meyer assessment (FMA-UE), administered by a trained researcher. Each subject experienced the various training modalities of the Upper Extremity Rehabilitation Training System with the assistance of the fellow, a certified rehabilitation therapist. Immediately after the experience, subjects completed the system usability scale (SUS) and a custom questionnaire to assess the user experience, acceptance of the new VR upper extremity rehabilitation system, and their views on its applicability to stroke rehabilitation.
Each participant completed a single usability testing session lasting approximately 60 minutes. The session comprised three phases: (a) System Introduction and Setup (10–15 minutes), where a research assistant provided necessary assistance with device wearing and calibration, and introduced the system's features and operation; (b) Hands-on Training and Testing (40–50 minutes), during which participants independently learned to use and tested all available training modes and tasks. To ensure the assessment reflected the system's intrinsic usability rather than external guidance, therapists refrained from providing active instruction during this phase; (c) Questionnaire Completion (5 minutes), where participants immediately completed the SUS and a custom-designed questionnaire.
During the training, the therapist provided necessary assistance only during the device setup and calibration phases. Once the task began, the therapist refrained from providing active instruction to ensure that the assessment results reflected the usability of the system itself rather than the effects of human intervention.
Measurement
System usability scale
We used this reliable and validated 10-item questionnaire 15 to assess users’ subjective experience and satisfaction with the Upper Extremity VR Rehabilitation System. The questionnaire was based on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The specific items are: (a) I think that I would like to use this system frequently; (b) I found the system unnecessarily complex (negative); (c) I thought the system was easy to use; (d) I think that I would need the support of a technical person to be able to use this system (negative); (e) I found the various functions in this system were well integrated; (f) I thought there was too much inconsistency in this system (negative); (g) I would imagine that most people would learn to use this system very quickly; (h) I found the system very cumbersome to use (negative); (i) I felt very confident using the system; and (j) I needed to learn a lot of things before I could get going with this system (Negative).
Custom questionnaire
An additional 5-item questionnaire, also on a 5-point Likert scale (1 to 5), was designed for this study. The questionnaire was designed to assess the user's experience with the Upper Extremity VR Rehabilitation System, including the following dimensions: (a) appropriateness of training difficulty; (b) game interactivity; (c) ease of operation; (d) degree of fun compared with traditional training; and (e) degree of motivation for training. The total score of the questionnaire ranges from 5 to 25, with higher scores representing better user experience.
The custom questionnaire was developed based on a literature review and interviews with three experienced occupational therapists to assess specific dimensions such as motivation and ease of use. Its content validity was evaluated and confirmed by an expert panel.
Statistical analysis
Descriptive statistics were used to present the data, including means ± standard deviation (SD), ranges, and frequencies for summarizing the demographic and clinical characteristics of the participants, as well as the results of the SUS and custom questionnaire assessments. In addition, the percentage of occupational therapists and stroke patients with SUS scores >70 (good usability) was calculated.
Results
Between September and December 2024, a total of 98 patients were assessed for eligibility. Of these, 30 met the inclusion criteria and were enrolled and assigned to the stroke group (n = 15) or the therapist group (n = 15). The detailed flow of participants through the study, including enrollment, allocation, and follow-up, is presented in Figure 3.
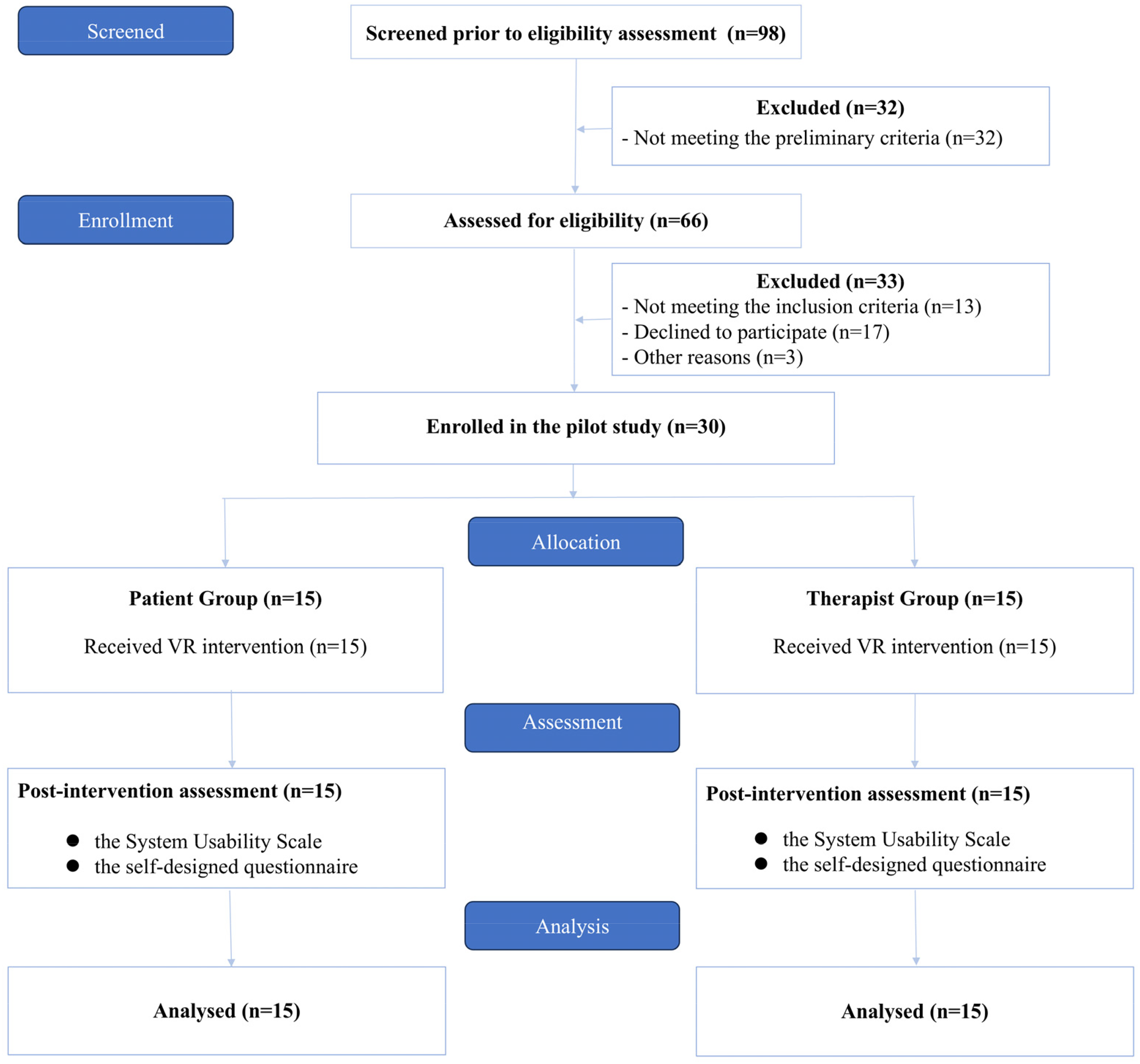
Study CONSORT flow diagram.
Demographic and clinical characteristics of participants
Fifteen certified rehabilitation therapists and 15 stroke patients were recruited for this study. The rehabilitation therapists had 1 to 13 years of clinical experience (mean ± SD: 3.87 ± 4.84), and 9 were female (Table 1).
Demographic characteristics of certified occupational therapists.

Abbreviations: F, female; M, male; SD, standard deviation.
In addition, all patients were right-handed dominant, and the majority of patients were male (n = 11). The age range of the patients was 34 to 76 years (mean ± SD: 53.73 ± 12.28), and the time of stroke onset ranged from 1 to 11 months. Ischemic and hemorrhagic strokes were diagnosed in 10 and 5 cases, respectively, with right hemisphere lesions in 7 cases and left hemisphere lesions in 8 cases. The total FMA-UE scores of the patients ranged from 46 to 64 (mean ± SD: 56.00 ± 5.25), indicating mild upper limb dysfunction (Table 2).
Demographic and clinical characteristics of stroke patients

Abbreviations: F, female; M, male; FMA-UE, Fugl–Meyer upper extremity evaluation; H, hemorrhagic; I, ischemic; L, left; R, right; SD, standard deviation.
Note: Higher FMA-UE scores indicate less upper extremity dysfunction.
Usability of the upper extremity VR rehabilitation system
Typically, participants used the VR system for approximately 1 hour daily. During this time, they learned the system's features, how to operate its hardware and software, and tested each training mode. Participants spent approximately 40 to 50 minutes testing and performing the training modes and tasks. They completed the SUS and a self-designed questionnaire at the end of the test.
Therapists’ experience and feedback
The mean SUS score for occupational therapists was 72.00 (Table 3). Five therapists had SUS scores above 70, which indicates good usability. Additionally, for therapists, the item with the highest SUS score was “I found the system very cumbersome to use” and the item with the lowest SUS score was “ I needed to learn a lot of things before I could get going with this system” (Table 4).
Usability of the Upper Extremity Stroke Rehabilitation System among stroke patients and occupational therapists.

Listed statistics are shown as mean ± standard deviation (SD) or frequency (percentage) appropriate to the data type. Abbreviation: SUS, system usability scale.
Note: Higher SUS scores indicate higher usability. Higher scores on self-designed questionnaires indicate a better user experience.
Mean ratings for each item of the system usability scale for occupational therapists and stroke patients.

The statistics presented are the mean ± standard deviation (SD).
Note: Transformed scores for each item range from 0 to 4. For odd and even items, higher scores indicate higher and lower agreement with the item statement, respectively.
In addition, the occupational therapists’ average score of the self-designed questionnaire was 20.20 (Table 3), indicating a good user experience. In addition, the item with the highest mean score on the self-designed questionnaire was “More interesting than traditional training” (Table 5). However, the item with the lowest mean score on the self-designed questionnaire was “Training difficulty is appropriate.”
Mean scores on items of the self-designed questionnaire for occupational therapists and stroke patients.

The statistics presented are the mean ± standard deviation (SD).
Note: Each item is scored on a scale of 1 to 5. Higher scores indicate greater satisfaction with the program.
Patient experience and feedback
The mean SUS score for patients was 73.00 (Table 3), and the percentage of SUS scores above 70 was 47%, indicating good usability. In addition, for the stroke participants, the item with the highest mean SUS score was “I needed to learn a lot of things before I could get going with this system.” The item with the lowest mean score on the SUS was “I found the various functions in this system were well integrated” (Table 4).
In addition, the stroke participants’ mean score for the self-designed questionnaire was 19.20 (Table 3), indicating a good user experience. In the self-designed questionnaire, the item with the highest mean score was “Good operating convenience” and the item with the lowest mean score was “Training difficulty is appropriate” (Table 5).
To identify specific areas for improvement, we conducted a detailed analysis of individual items from both the SUS and the self-designed questionnaire. Analysis of SUS items revealed distinct challenges for each user group. For therapists, the lowest-rated item was “I needed to learn a lot of things before I could get going with this system” (Item 10: 2.47 ± 0.92), indicating a perceived high initial learning cost. For patients, the greatest difficulty was expressed in “I found the various functions in this system were well integrated” (Item 5: 2.73 ± 0.88), suggesting a need for improved functional consistency and cohesiveness in the system design. Data from the self-designed questionnaire further refined this. The item “Training difficulty is appropriate” received the lowest scores from patients (3.13 ± 1.19) and therapists (3.80 ± 0.86), highlighting a common concern regarding the need for more adaptable difficulty settings.
Adverse events
No adverse events or unintended effects related to the use of the VR rehabilitation system were reported or observed in both groups during the trial period.
Discussion
Stroke constitutes a primary cause of long-term functional disability, with poor upper limb recovery severely compromising ADL. Although conventional rehabilitation therapies—such as constraint-induced movement therapy (CIMT), mirror therapy, and high-intensity task-specific training—are widely implemented, they face limitations, including prolonged treatment duration, suboptimal patient adherence, and high resource demands. The core neurorehabilitation strategy harnesses motor learning optimization principles—high repetition, task-orientation, motivational engagement, and enriched feedback—to drive neural plasticity. VR technology, by creating immersive, multisensory interactive environments, effectively integrates these critical elements, offering training paradigms that transcend conventional approaches to accelerate functional recovery. 16
This study evaluated an innovative VR system that integrates automated FTHUE assessment with personalized task-oriented rehabilitation protocols to enhance upper limb functional recovery in stroke patients. The system architecture rigorously incorporates neuroplasticity-driven mechanisms—including promotion of interhemispheric balance, strengthening of functional connectivity, and potential activation of mirror neuron systems17,18—synergistically with core VR design principles of motivational engagement, goal-directed paradigms, and adaptive personalization. 19
It should be noted that the current version of the VR system and its training protocols are primarily designed for unilateral stroke patients who retain some active motor function. For patients with bilateral stroke or those with severely weakened muscle strength (e.g. Brunnstrom stage I-II) who cannot generate effective active movements, the current system is not directly applicable. During the initial project phase, we focused our research scope and managed system complexity within controllable limits, prioritizing the functional training needs of the larger unilateral stroke population during rehabilitation. Our primary goal was to ensure the safety, accuracy, and immersion of active training.
Although the system is not equipped with physical assistive devices such as exoskeletons, it incorporates a task difficulty grading system through software-level innovation to provide essential support for patients with weakened muscle strength. Therapists can meticulously adjust the difficulty parameters of virtual tasks—such as enlarging target sizes or extending allotted completion time—based on the patient's specific functional level. This enables flexible adaptation to the training needs of patients with different muscle strength levels, ensuring training safety while promoting engagement and rehabilitation outcomes.
The core innovation of this system lies in its seamless integration of automated assessment based on the functional test for the hemiparetic upper extremity (FTHUE) and corresponding personalized rehabilitation programs, grounded in neurodevelopmental and motor relearning theories, within a VR platform. Compared to existing VR rehabilitation systems,6,1020–22 this system offers several significant advantages centered on patient-centered, task-oriented, and personalized training. Specifically, leveraging automated FTHUE assessment results matches the patient's functional impairment level to dynamically generate or select rehabilitation games, enabling highly individualized training plans.23,24 Crucially, the system emphasizes holistic upper limb-hand rehabilitation, training, and assessing the arm and hand as a coordinated functional unit, thereby effectively overcoming the standard limitation in existing systems of neglecting fine hand motor functions.25,26
Furthermore, it achieves a closed-loop integration of assessment and treatment: FTHUE results inform initial program formulation, directly guide subsequent training adjustments, and serve as objective outcome measures for efficacy evaluation, eliminating the disconnect between assessment and treatment. The system utilizes VR and advanced sensing technology (Microsoft Azure Kinect) to automate and objectify assessments like FTHUE, significantly reducing subjectivity to enable this precise evaluation. Regarding the training experience, it enhances engagement through diverse game scenarios providing visual, auditory, and tactile multisensory feedback, creating an immersive environment that boosts enjoyment, immersion, and patient motivation. Finally, employing relatively low-cost, portable, markerless sensing technology, the system demonstrates strong technical feasibility and accessibility, making it particularly well-suited for deployment in community and home-based rehabilitation settings, thereby significantly expanding the reach of rehabilitation services.
A preliminary usability evaluation was conducted involving 15 occupational therapists and 15 stroke patients with mild upper limb impairment. The mean SUS scores surpassed the established threshold of 70 for good usability in both the therapist and patient groups, indicating that the system was generally easy to learn and use. Participant feedback revealed favorable perceptions of the system's operational convenience and highlighted its significant enhancement of training enjoyment and engagement motivation; therapists particularly emphasized its distinct advantage in fun compared to conventional therapy. Results from the user experience questionnaire further corroborated the positive overall user experience. However, the evaluation also noted that some participants perceived room for improvement in the system's functional integration. Additionally, the adaptive matching of training difficulty (especially for patients) and the initial learning curve were identified as areas requiring attention and optimization.
It is important to emphasize that the current study primarily focused on validating the system's usability, while its clinical efficacy remains to be rigorously verified through well-designed randomized controlled trials (RCTs). Building upon the positive outcomes of this feasibility study, our next step will involve conducting a large-scale RCT. The primary outcome measures will include standardized clinical assessments such as the Fugl–Meyer assessment (FMA) and the Action Research Arm Test (ARAT) to rigorously validate the system's efficacy in upper limb functional recovery.
Looking forward, the long-term goal of this system is to establish a personalized rehabilitation platform covering different impairment levels and rehabilitation stages. Based on the success of this feasibility study, our plans include: (a) developing passive/assisted training modes: for patient populations with severely weakened muscle strength, we will integrate trigger mechanisms based on surface electromyography (sEMG) or force sensors. Patients will only need to generate minimal muscle activation or force to trigger the system to complete pre-set assisted motions, thereby facilitating the transition from passive to active training; (b) exploring integration with external assistive devices: we are planning data interface coordination with upper limb rehabilitation robots or functional electrical stimulation (FES) devices, using VR to provide immersive training scenarios while external devices offer physical assistance, thereby serving patients with more severe impairments; (c) extending to bilateral training: for bilateral stroke patients or those requiring bilateral coordination training, we will develop virtual tasks requiring bimanual cooperation in future versions.
The findings demonstrate the system's usability and provides a novel and engaging rehabilitation tool for stroke patients. This integrated VR system, combining assessment with personalized training, holds significant promise as a valuable complement to conventional rehabilitation: By generating highly individualized, task-oriented training plans based on objective assessment, it enables precise rehabilitation interventions; through its immersive, gamified experience, it significantly enhances patient motivation and training compliance, thereby addressing a key bottleneck in traditional rehabilitation adherence; and by leveraging portable technology to lower the barrier to application, it facilitates the system's adoption in community and home-based settings. Collectively, these features fundamentally enhance the accessibility and coverage of rehabilitation services.
Limitations
This study has several key limitations. Technologically, constrained by the precision limitations of current sensors (e.g. Kinect), the system's capability to capture fine motor movements of the wrist and fingers and to automatically identify abnormal compensatory movement patterns (such as trunk leaning) requires further development; this may impact training precision. Methodologically, the sample size was relatively small (n = 15 per group) and primarily comprised patients with mild upper limb impairment. It should be noted that, as a preliminary feasibility/usability study, its primary aim was to evaluate the system's usability, safety, and acceptability. The current sample size falls within the standard range for such studies (typically 10–30 participants), and the focus on patients with better functional levels was motivated by safety and operational feasibility considerations. This approach allowed for initial validation of the system's core functionality in a controlled-risk environment and laid the groundwork for future inclusion of patients with moderate to severe impairments. Therefore, the findings of this study are primarily applicable to stroke patients with mild hand dysfunction and cannot be readily generalized to populations with severe impairments.
Furthermore, it is essential to specifically note that the current version of the VR system and its training protocols are primarily designed for unilateral stroke patients who retain some active motor function. For patients with bilateral stroke or those with severely weakened muscle strength (e.g. Brunnstrom stage I-II) who cannot generate effective active movements, the current system is not directly applicable.
Additionally, the inclusion criteria covered a relatively wide range of time since onset (1is not directly applicable. are primarily designed for unilateral stroke patients who retain some active motor f’ recovery potential and movement patterns. It should be noted that this study's inclusion criteria relied on clinicians’ subjective judgment rather than standardized cognitive assessment tools, and patients’ education levels were not systematically recorded. This approach may introduce cognitive bias and selection bias, limiting the generalizability of the research findings. Future clinical studies will employ standardized scales such as MoCA or MMSE for rigorous screening and will evaluate the impact of education level on the usability of the VR system.
Furthermore, the usability evaluation did not control for confounding factors such as computer literacy and education level. Regarding validation depth, the study focused on system usability assessment; clinical efficacy has not yet been established through a RCT, and the training effectiveness for complex functions like finger dexterity requires further enhancement. Finally, the cohort of therapists participating in the evaluation was relatively young and had limited years of experience. Given that younger practitioners may hold more positive attitudes and higher familiarity with new technologies, this may introduce a positive bias in the evaluation results of the system's usability, potentially limiting the generalizability of the findings across therapist populations with varying ages and levels of experience.
Ethical and equity considerations
Despite validating the usability of the VR-based upper limb rehabilitation system in clinical settings, its broader dissemination and application must carefully consider the ethical and equity implications inherent to digital health technologies. Firstly, the system's reliance on specific hardware and high-speed internet connectivity may exacerbate the “digital divide,” potentially limiting accessibility for low-income populations, patients in remote areas, or older adults, replicating or even amplifying existing health inequalities.27,28 Secondly, variability in digital literacypeed int technology use barriers stemming from age, educational background, or cognitive impairments—necessitates that system design adhere to “inclusive design” principles. This involves integrating multimodal interactions (e.g. voice assistance, simplified interfaces, and multilingual support) to accommodate diverse user needs. Furthermore, continuous patient movement and physiological data collection during system operation mandate robust privacy protection, clear data ownership protocols, and cybersecurity risk mitigation through encrypted transmission, explicit informed consent, and ethically compliant data management strategies. To ensure equitable clinical translation, future research must proactively enroll patients from varied socioeconomic backgrounds, functional ability levels, and geographical distributions, while actively exploring community-supported and low-cost dissemination models. This approach ensures that VR rehabilitation technology is effective, equitable, responsible, and ethically grounded.
Future directions
Our usability evaluation not only confirmed the overall acceptability of the system but, more importantly, identified specific directions for its improvement, such as reducing the initial learning cost, optimizing functional integration, and providing a more flexible difficulty adjustment mechanism. These findings will provide direct and valuable input for developing the system's next version.
Building upon the current study's limitations, subsequent efforts will focus on three key areas: Technologically, by refining sensor fusion algorithms and integrating advanced gesture recognition technologies to overcome bottlenecks in fine hand movement capture, while concurrently developing a real-time feedback module for compensatory movement patterns to standardize training posture. Clinically, the focus will be on enrolling larger sample sizes encompassing stroke patients with varying degrees of impairment (exceptionally moderate to severe), and conducting subgroup analyses based on the time since onset (such as distinguishing between subacute and chronic phases) to investigate the system's applicability across different rehabilitation stages more precisely. Future clinical studies will employ standardized scales such as MoCA or MMSE for rigorous screening and will evaluate the impact of education level on the usability of the VR system.
On this basis, large-scale feasibility studies and RCTs will be carried out, combined with electrophysiological assessments (e.g. EEG), to systematically validate the system's effectiveness and sensitivity in functional recovery and neuroplasticity. In terms of application and dissemination, the operational workflow will be further simplified to enhance the user experience in community and home-based settings. Such a VR system, characterized by its deep integration of precise assessment and personalized training, holds significant promise for evolving into an efficient, accessible, and highly adherent innovative solution for upper limb stroke rehabilitation.
Conclusions
This study tested a VR-based upper limb rehabilitation system with personalized, task-oriented rehabilitation programs. Preliminary validation demonstrated its favorable usability in both stroke patients and healthy individuals. The system provides a novel approach to address key limitations observed in existing VR rehabilitation systems by establishing a closed-loop integration of assessment and therapy and delivering personalized immersive training. Looking forward, its modular design and reliance on consumer-grade hardware demonstrate strong scalability, laying a technical foundation for large-scale applications in community and home-based settings. Integration with existing rehabilitation processes is expected to establish a continuous “hospital-community-home” integrated rehabilitation model, which holds significant translational value for overcoming the spatiotemporal limitations of conventional rehabilitation and improving the accessibility and efficiency of rehabilitation services.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251386665 - Supplemental material for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives
Supplemental material, sj-docx-1-dhj-10.1177_20552076251386665 for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives by Qiurong Xie, Qi Zhang, Yanxin Zhang, Bo Sheng, Xiaoling Wang, Jia Luo and Jia Huang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251386665 - Supplemental material for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives
Supplemental material, sj-docx-2-dhj-10.1177_20552076251386665 for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives by Qiurong Xie, Qi Zhang, Yanxin Zhang, Bo Sheng, Xiaoling Wang, Jia Luo and Jia Huang in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251386665 - Supplemental material for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives
Supplemental material, sj-docx-3-dhj-10.1177_20552076251386665 for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives by Qiurong Xie, Qi Zhang, Yanxin Zhang, Bo Sheng, Xiaoling Wang, Jia Luo and Jia Huang in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251386665 - Supplemental material for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives
Supplemental material, sj-docx-4-dhj-10.1177_20552076251386665 for Research on upper limb motor function evaluation and rehabilitation training system of stroke patients based on artificial intelligence: A usability and feasibility study from therapist and patient perspectives by Qiurong Xie, Qi Zhang, Yanxin Zhang, Bo Sheng, Xiaoling Wang, Jia Luo and Jia Huang in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr Peter Fermin Dajime for his crucial role in designing and developing the exergames that formed the foundation of this study. They sincerely appreciate the essential contribution of all clinical research staff participating in this trial, whose commitment to participant recruitment and care was fundamental to its execution.
Ethics considerations
This study adheres to the ethical principles outlined in the Helsinki Declaration and has obtained approval from the Ethics Committee of the Rehabilitation Hospital Affiliated with Fujian University of Traditional Chinese Medicine (Approval No. 2022KY-006-01).
Consent to participate
Before enrollment, all participants will receive comprehensive information about the trial and must provide their consent by signing the informed consent form. Participants retain the right to withdraw from the study without penalty. Further details regarding ethical approval can be found in the supplementary documen
Consent for publication
All authors have agreed to publish this article.
Contributorship
QRX did writing—original draft, conceptualization, formal analysis, investigation, methodology.
QZ and JL did writing—review and editing, investigation.
YXZ and JH did writing—review and editing, conceptualization.
BS did writing—review and editing, methodology.
XLW did writing—review and editing, formal analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by grants from the National Natural Science Foundation of China (Grant Number 82305357) and the Natural Science Foundation of Fujian Province (Grant Numbers 2020J01752 and 2025J01948).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
To safeguard participants’ privacy, the data generated or analyzed in this study will remain confidential and not publicly disclosed. However, the data can be accessed by contacting the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.