
Abstract
Objective
Virtual reality (VR) has been used to improve upper limb function after stroke but there is little to guide product developers in building experiences that engage users in the sustained, repetitive training required. This research sought to understand the characteristics of VR scenarios best suited to engaging someone with a stroke during recovery to achieve therapeutic outcomes.
Methods
Five creative immersive VR scenarios were designed by an experienced VR content creator containing unique combinations of VR characteristics. The usefulness of the scenarios was reviewed by expert clinicians experienced in stroke rehabilitation. Following this review, seven stroke survivors participated in each experience and reported on their engagement and motivation. Outcome measures were the User Satisfaction Evaluation Questionnaire and the modified Intrinsic Motivation Inventory. Semi-structured interviews were conducted with five participants following their immersive VR experience and analysed thematically.
Results
Expert clinicians reported potential therapeutic value in the immersive VR scenarios by providing opportunities for repeated and graded practice of upper limb movements. Stroke survivors reported varied levels of enjoyment and engagement for each scenario. They recommended changes to the experiences, primarily relating to the tailoring of the scenarios to match varied upper limb capacities.
Conclusion
This study highlights the characteristics of immersive VR scenarios that are important in sustaining motivation and providing high-repetition task-specific movement experiences. Differences in the experience and preferences of stroke participants regarding the characteristics of immersive VR experiences indicate that a variety of experiences are necessary to engage and sustain participation in an immersive VR-related therapy programme.
Highlights
Clinician input into the development of rehabilitation VR scenarios is important.
This research identifies aspects of VR experiences that can address the task-specific repetition required to improve upper limb function post-stroke, and to sustain motivation during rehabilitation.
Embedding the repetition required into the VR experience is challenging.
Varied experiences are important in engaging users in VR therapy.
Background
Stroke is a common health condition worldwide with one in four adults over 25 years of age to expect the condition during their life and over 101 million people in the world experiencing the aftermath of stroke. 1 The cost of stroke rehabilitation is estimated to be USD72 billion 2 with 5.3% of all disability adjusted life years attributed to the condition. 3 Upper limb impairments after stroke occur between 49% 4 and 75% 5 of people. These upper limb impairments limit functional recovery and adversely affect individuals in many areas including performing activities of daily living, work-related activities and quality of life. 6 No single therapeutic approach is recognised as being consistently effective for functional recovery in those who have survived a stroke long term. However, interventions that embed repetitive, active use of the affected arm align with evidence-based protocols involving high levels of volume and intensity of practice. 7
Immersive VR is a technology that is increasingly been used in health care. 8 Immersive VR has been used as an intervention with people for a variety of conditions such as Parkinson's Disease, 9 pain,10,11 and mental health conditions12,13 and cognitive decline. 14
VR intervention has been shown to improve upper limb impairment after stroke.15–17 Immersive and non-immersive VR systems have been developed or adapted to improve upper limb function after stroke using simulated interactive experiences in specifically designed virtual environments. 18 They allow multisensory stimulation and different forms of user interaction through movements and speech19,20 and are designed to keep the user engaged in movement for as long as possible. Immersive VR hardware can be portable and easily transportable making its use possible in both a clinical setting and a home environment. 19 Importantly, immersive VR, when used with conventional rehabilitation can provide an environment where the task-specific repetition required to improve motor skills function after stroke can occur. 21
While some useful recommendations exist in relation to the end user and therapist engagement in VR and rehabilitation 22 there is little guidance available to developers when designing VR scenarios specifically designed for post-stroke use. This gap is a significant one given the poor outcomes for people with upper limb impairment after stroke experience. In order to be a useful component of post-stroke therapy. VR scenarios need to be both therapeutically powerful and engaging and motivating for the user group. Evaluation of VR scenarios to identify their therapeutic potential is important in understanding their value as a part of stroke rehabilitation. An exploration of the experiences of stroke survivors using VR approaches to therapy is also required to understand the factors most likely to lead to sustained engagement and optimal therapeutic outcomes.
The aims of this project were therefore to;
To elicit the opinions of therapists experienced in post-stroke rehabilitation in relation to the use of immersive VR. To describe the experiences of people post-stroke after undertaking immersive VR.
Methods
This was a mixed methods study conducted between January 2020 and November 2022. Data analysis was conducted between December 2022 and April 2023. This research was approved by the University of Canberra Human Research Ethics Committee (HREC 2096).
Participants
Participants consisted of two distinct groups; expert clinicians and post-stroke survivors. The clinician participants were familiar with the Australian and New Zealand Living Clinical Guidelines for Stroke Management 7 and associated evidence regarding upper limb rehabilitation following stroke. Clinicians with more than five years’ experience in stroke rehabilitation were sought from the local health service and two who met these criteria consented to be the clinician participants.
A convenience sampling method was used to recruit people with upper limb impairment following a stroke through social media advertising and snowballing. Informed written consent was obtained from each participant. To be included in the study, participants needed to:
Have a diagnosis of any type of stroke at any time previous to the study commencing Have self-reported upper limb impairment Be able to sit for 30 min and be able to answer detailed questions about their experiences. For this reason, people with poor sitting balance and/or significant cognitive or communication deficits were excluded.
Materials
A Pico 3 VR headset with a head-mounted display and hand controls was supplied by Recovery VR Figure 1.

Pico 3 VR headset and hand controls.
Five scenarios used in this project were developed prior to the project by an expert VR content creator. The VR content creator liaised with the research team to design scenarios that could be done bilaterally or unilaterally, done in sitting or standing and were modified following discussion with the research team. The VR scenarios varied with regard to seven main characteristics (see Table 1). Each scenario combined these features in unique ways, allowing participants to identify the features they found most and least engaging. This enabled participants to compare and contrast the potential therapeutic value and level of engagement in each experience. VR scenarios are referring to what was designed, whereas VR experiences refer to what the participants went through, and VR therapy refers to the specific or potential use of VR as a therapeutic modality. As we wanted the participants to comment on the self-guided aspect of the experience a therapist was not present to provide assistance, rather a trained research assistant was present to set up the scenarios and for safety supervision.
Characteristics of the VR scenarios.

Intervention
The intervention occurred in two phases. In the first phase, the expert clinicians participated in all of the VR experiences and then critiqued each of those experiences based on their knowledge of stroke rehabilitation, and the Clinical Guidelines for Stroke Management.
7
Specifically, clinicians:
Were orientated to the use of the VR system through a 3-min adjustment phase during which they had the appropriate technology fitted and tested. Adverse reactions were monitored during this period. Engaged in five 5–10 min VR experiences with a 3–5 min interval between each. During the interval, the technology was removed. Participated in a 45-min face-to-face semi-structured interview conducted immediately following their VR experiences. Interviews were audio recorded and transcribed verbatim for data analysis. The interview was designed to elicit the expert's thoughts and opinions about the experience in relation to usefulness, applicability to best practice, appropriateness for the user, and pragmatic considerations. See Appendix 1 for the semi-structured interview guide. Were orientated to the VR system through a 3-min adjustment phase during which they had the appropriate technology fitted and tested. Adverse reactions were monitored during this period. Engaged in the scenarios for 50 min. Participants had preferred scenarios in which they engaged in more than others, however, participants were asked to try all scenarios with 3–5 min intervals between each scenario. During the interval, the technology was removed, and participants completed the modified IMI regarding their experience. Completed the User Satisfaction Evaluation Questionnaire following completion of the final VR experience. Participated in a 45-min face-to-face semi-structured interview conducted following their VR experiences. Interviews were audio recorded and transcribed verbatim for data analysis. The wording of some of the questions in the interview guide were modified based depending on participant preferences.
Phase 2 engaged seven post-stroke participants in each of the five VR experiences. Following written consent, the post-stroke participants:
Outcome measures
The modified IMI 23 is a validated 45-item tool with a 7-point Likert scale response for each question. The IMI has been used for assessing subjective experiences of participation and is designed to be customised to the target activity. Four items per scale were chosen from an item bank to customise the tool to suit the VR experiences used in this study. The IMI was used to evaluate markers of intrinsic motivation related to interest/enjoyment, perceived competence, effort/importance, pressure/tension, perceived choice and value/usefulness. Markers related to relatedness were only gathered for the tea-making scenario because it was the only scenario that provided interaction with a facilitator.
The USEQ 24 is a validated tool designed to evaluate the satisfaction of users of virtual rehabilitation systems. This six-item questionnaire has demonstrated acceptable levels of reliability and internal consistency. 24 It was administered to participants immediately following the completion of all five VR scenarios. The USEQ asks participants to rate their satisfaction with a variety of aspects of an experience including enjoyment, success, control, clarity, comfort and therapeutic potential on a five-point scale which is converted to a continuous scale, with 6 being the lowest score possible and 30 the highest. This provides information about overall satisfaction with the VR experience.
Analysis
Quantitative data
Demographic information was analysed descriptively for age, sex and time post-stroke.
Results from the IMI and USEQ were analysed using IBM® SPSS Statistics for Windows. 25 Data from the IMI is reported using medians and interquartile ranges with means and standard deviation for the USEQ.
Qualitative data
Qualitative data from both expert-clinician participants and post-stroke participants were transcribed verbatim. The transcriptions were reviewed for accuracy and analysed independently by three authors (CP, SI and HH) using the framework approach. This deductive approach to analysis is appropriate to use with small data sets where the aim of the research is to answer specific policy or implementation questions. It is an approach well suited to mixed methods when quantitative data is also available. 26
The steps followed as per Pope et al. (2020) commenced with familiarisation, when all authors read the transcripts to familiarise themselves with the data obtained from the interviews. The next steps resulted in the construction of a thematic framework, followed by labelling and sorting to merge those themes that were similar or had overlap, and finally reviewing data extracts to look for coherence across the two groups.
Results
Two expert clinicians were recruited from a local rehabilitation and recovery hospital. One physiotherapist and one occupational therapist with 18 years experience and 11 years experience respectively in post-stroke rehabilitation. The physiotherapist had doctoral qualifications in stroke management. One of the expert clinicians had used immersive VR previously, the other had not.
Seven post-stroke participants (four females and three males) were also recruited for this project. Demographic data from only five participants were collected. Their mean age was 64 (SD 8.45). The mean years since the individual's stroke was 10.5 (SD 4.0). None of the post-stroke participants had used VR previously.
The two clinicians participated in January 2020. Due to Covid-related delays, the post-stroke participants were shown the VR scenarios in March 2021 and were interviewed between one day and one week following their experience. Two post-stroke participants elected not to undertake an interview (Table 2).
Post-stroke participant demographic information.

Participants had varying degrees of upper limb function with some being able to use their hemiplegic upper limb during the VR experiences and other participants not able to easily use the controller. Table 3 qualitatively describes the participant's upper limb function when engaging in the activities.
Qualitative description of participant's upper limb function during the VR experiences.
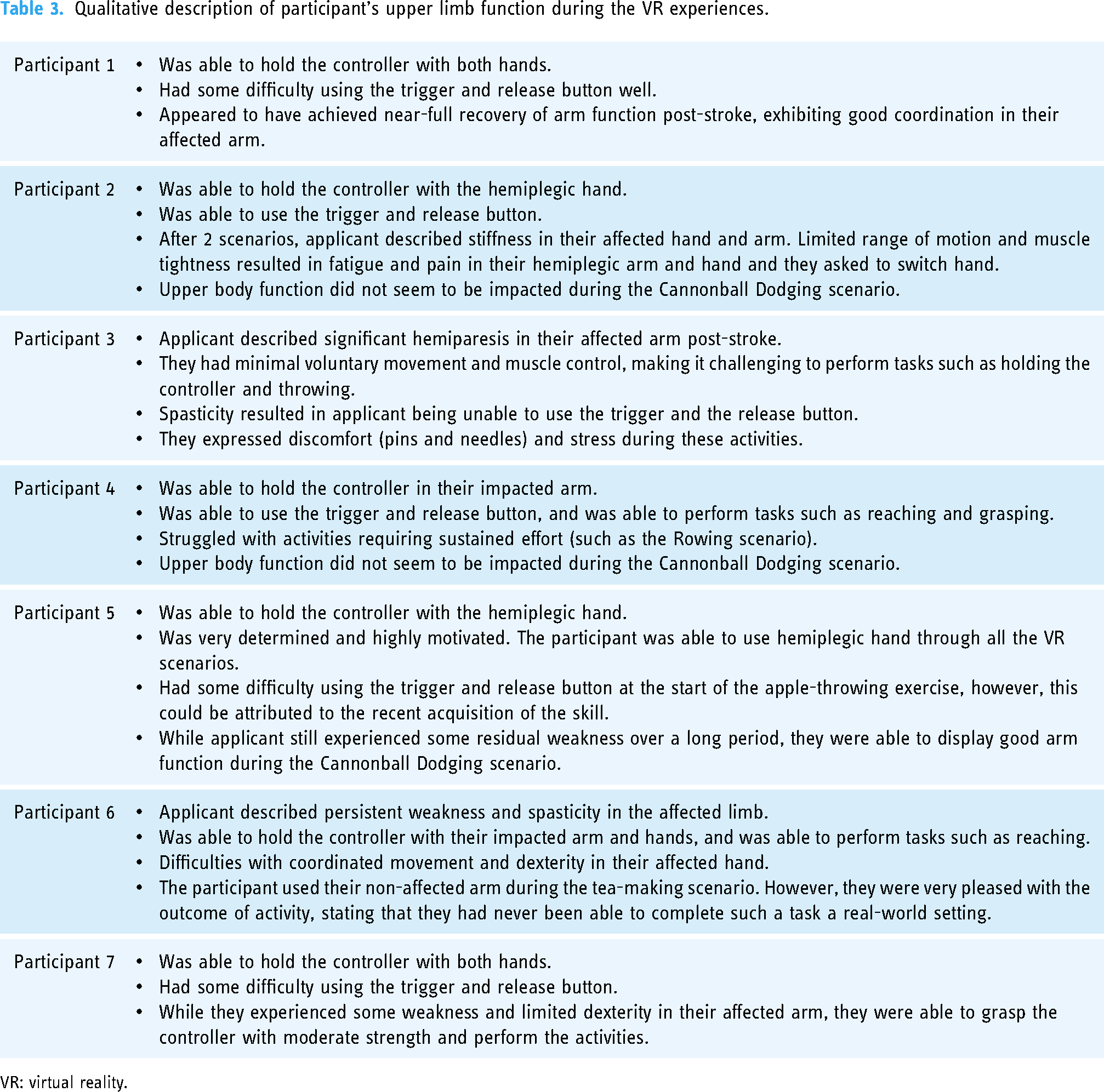
VR: virtual reality.
Based on an expert-clinician review of the VR scenarios, the developers made some modifications to the scenarios prior to use with post-stroke participants to optimise their experience and overcome technical issues. These modifications are presented in Table 4.
Modifications to the VR scenarios.

Post-stroke participants completed the IMI following their experience of each scenario. The IMI results can be seen in Table 5.
Results of the intrinsic motivation inventory.

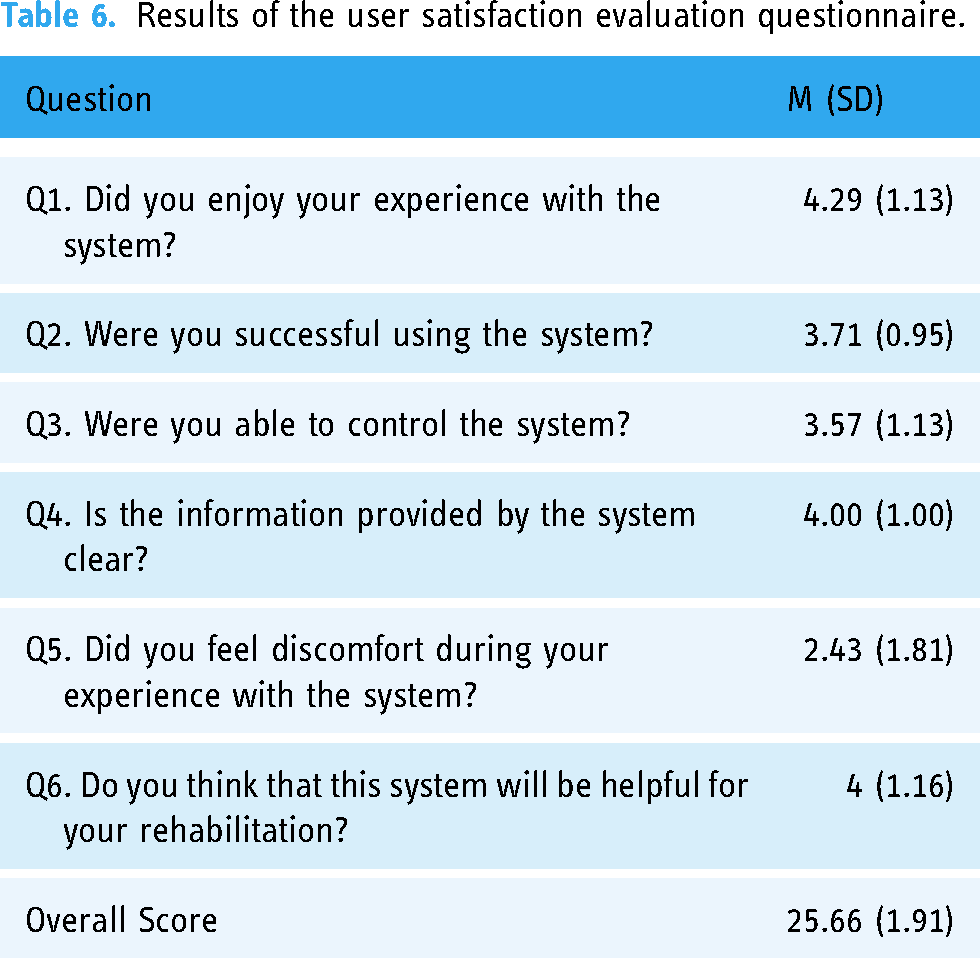
At the completion of all scenarios, post-stroke participants were asked to complete the USEQ. The mean overall satisfaction score for the VR experience was 25.66/30 (SD 1.91). Satisfaction with different aspects of the VR experience was variable, ranging from 2.43/5 (SD 1.81) for discomfort, to 4.29/5 (SD 1.13) for enjoyment. Results from the USEQ are summarised in Table 6.
Results of the user satisfaction evaluation questionnaire.
Qualitative results
There were five themes arising from the expert-clinician interviews and five themes from the post-stroke participant interviews. These themes are presented in Table 7,
Thematic framework for stroke participants and clinician participants.

VR: virtual reality.
The framework approach, which addressed the aims of the project, elicited similarities and contradictions between the two groups. Both groups expressed an openness to the value of VR in stroke rehabilitation. The elements that both groups valued and thought needed further development was having VR that related to and transferred to everyday activities. P4: For an instant, I guess the belief was that like making tea it's like a normal activity like a sort of an almost day-to-day activity. So replicating that reality within this virtual environment, maybe that would give people a bit more motivation to do things I guess. C1: So I think the realism is probably the only one that I can probably directly relate to is the making cup of tea because it is obviously a real-life scenario and something that typically everybody does on a day-to-day basis. So it's highly transferable.
The challenge of this was also highlighted by both groups but with differing perspectives. The clinicians reported that using VR was a way to grade return to activity for patients who were not yet ready to attempt the real-life version. C1: I think if we had a lower functioning person, then we would utilise more of that implied mental practice could be utilised more for those sorts of patients then. But those who maybe do have some more mild to moderate impairment, maybe we would have more physical, their ability to actually pick up that kettle and pour and so on and so forth. C2: And if someone was up to the level of making a cup of tea, I don’t think I’d be using that activity with them. And really, if someone was up to manipulation, I don’t think I would be using any of those games with them. C2: I think that the difficulty that I found with some of the games in general, in a suite of games, is that, some of the games are easier or harder depending on what they are. And so you don’t want them all to be very realistic and functional, that are hard or easy or whatever it is. You need the grading of difficulty in the different types of games maybe.
Related to this was the suggestion that a greater ability to grade the VR would be therapeutically beneficial. C2: I think that the difficulty that I found with some of the games in general, in a suite of games, is that, some of the games are easier or harder depending on what they are. And so you don’t want them all to be very realistic and functional, that are hard or easy or whatever it is. You need the grading of difficulty in the different types of games maybe.
The participants on the other hand were concerned about attempting the VR too soon in their recovery journey, preferring to have a higher level of ability or function before VR is introduced. P3: I’m thinking that if I’m able to improve my arm by other means before, before I do any more of the VR, I need to get this arm a little bit better to do the right …. Yeah, I think I think it's a very personal thing. The ability of the person needs to be assessed before the scenarios are introduced. Maybe so that whether the person is capable of. P5: It requires two hands and when the test subject doesn’t have the luxury of two hands which is just dumb, asking someone to utilise a hand they can’t use …. There's such a, such a wide, you can’t just go You can’t lump all of our stroke volunteers, stroke survivors into one bucket, which is what I think they’re doing.
The clinicians and the participants were in agreement that it was not realistic to expect that VR post-stroke would be utilised at home. The reasoning was somewhat different, with the participants reasoning that they did not have the time or ability to undertake the activities themselves. P5: To regain function you need to practice literally all day, every day. And who's got the time for that, who's got the money for that. For someone like me, I was a single mother, with no income coming in and no support service in Canberra. I don’t have time to do a physio activity all day every day.
The clinicians were of the view that patients do not tend to do prescribed exercise programmes to the level required so VR would be no different C1: Because there are a lot of patients who are wanting to do things outside of the gym but don’t engage well in our more standard home exercise programme. So you know, we get a lot of patients home exercise programmes and they don’t all do them. Probably more people don’t then do. C2: Like I presume that you’re aware of the observational studies that basically show people hardly practice in therapy. So unless there's someone engaging them to do it, it's quite hard to do that.
Both groups brought up the topic of therapist assistance when utilising VR. The clinicians saw the potential for reducing the demands on their time, whilst acknowledging that safety concerns were a factor. C2: I would think about it in the sense of that, it should be a component of therapy that I would anticipate that it would need some therapist instruction at the beginning. But I would want it to be something that you could then leave with someone to practice, and that to me is the benefit of it. C1: In an ideal world if it was, I think we would need to do some introductory work with them, so we need to teach them how to utilise it, maybe make some recommendations around games, how long they should be playing it, but then I think I would like to see this as something that they do outside of the gym, or they do Independently come into the gym and do. But not necessarily under the strict supervision of a therapist or an allied health assistant.
Participants expressed the view that having support to start VR as well as ongoing therapist support was important. P3: I think there would still need to be some live therapist visits at times, to check that everything is going okay. P7: Yeah, it's like giving a little bit more detailed instructions as well, I guess that that would be helpful in pointing out that connection in your body. If you get given the, the, I guess, the right instruction from an OT as well, I think the OT instruction because you know that it's sequenced. And it's real, and it's professional, you know, somebody who knows what they’re doing, this is the way you do it, your fingers will be them this form shape, your brain, my brain or connection would connect with that.
Discussion
The expert clinician participants in this study reported that the VR scenarios had the potential to improve upper limb function after stroke. They noted that the range of VR experiences provided allowed for the opportunity to engage in task-specific repetition, which is often very difficult to achieve in a normal environment. They also recognised that while the VR scenarios provided opportunities to address general limits in upper limb function, it was more difficult to use it to address specific issues with hand control and fine motor skills.
Expert clinicians recommended that VR therapy be used as an adjunct rather than a replacement for traditional forms of post-stroke therapy. Responses from post-stroke participants also acknowledge the importance of effective set-up and grading of VR experiences, which suggests that VR therapy should not be a stand-alone approach to stroke recovery. While post-stroke participants indicated an interest in using VR therapy at home, expert clinicians were concerned that it might be difficult to monitor performance, ensure appropriate grading of VR experiences and address any technical issues relating to set-up from the home context. While acknowledging the potential benefits, the expert clinicians highlighted that grading of activities, safety and progression were all critical clinical reasoning steps required when using VR as an intervention. These results are consistent with literature that reports important clinical and contextual considerations, including thoughtful matching of client abilities and goals to the VR experience.22,27
This research suggests that VR scenarios informed by clinicians, resulted in good client engagement and motivation to complete the tasks but mixed results in relation to usability and enjoyment. The USEQ scores showed participants were very satisfied with the overall VR experience, however there were varied responses to specific characteristics of the experience. Post-stroke participants found the experience enjoyable and easy to understand and believed it would make a positive contribution to their recovery, however, they were less satisfied with their experience of using and controlling the experience. The mean score on the USEQ for the question ‘did you feel discomfort during your experience was lower than the scores for the other questions (2.43)’. Two of the participants in particular reported some discomfort (pins and needles) they associated with their upper limb weakness and spasticity. This article did not aim to investigate the correlation between the VR experience, discomfort and specific upper limb impairment after stroke but this finding should be investigated in future studies.
Results from the IMI provide an understanding of post-stroke participants’ experience of individual scenarios. The apple barrel scenario was highly regarded across all measures, indicating a high level of intrinsic motivation generated during the experience. While highly rated on most factors, the lack of perceived choice was reported as limiting motivation. Tea-making was the only scenario that provided a sense of relatedness to the therapist, but post-stroke participants identified limits in perceived competence on the task. The cannonball and painting scenarios were both seen to provide a sense of interest, competence and importance in an experience that was free of pressure but was limited in perceived choice and usefulness.
The results from the IMI, along with qualitative feedback from the post-stroke participants, indicated they enjoyed their experience and found some of the experiences (especially apple barrel, rowing and tea-making) valuable, useful and enjoyable. This builds on other findings 28 by further analysing the positive impact of head-mounted display VR for upper limb rehabilitation.
According to Ryan et al. (2006) virtual environments themselves can be highly motivating 29 due to their goal-orientated tasks and multisensory feedback particularly where the individual can perceive autonomy and competence, and this can increase motivation. This was reflected in the responses from post-stroke participants highlighting that the VR experience removed some elements of physical risk allowed them to practise activities (like tea making) in an environment that allowed for safe transferable skills practice. The ability of the VR experiences to engage people in this type of task-specific repetition is an important factor contributing to improved upper limb function post-stroke. 7
Feedback from both the expert clinician and post-stroke participants identified the importance of person-centred comprehensive assessment prior to the implementation of VR. Care must be given by the clinician to match current upper limb function with the client goals and skills and interest in using technology. Furthermore, both stroke participants and clinician participants stressed the value of making the VR activities transferrable and/or relatable to everyday life. This is consistent with literature that reports the importance of aligning client goals, interests and context to the VR intervention. 27 Adjusting the parameters of the VR experience in terms of the type of experience, grading the difficulty and matching feedback in conjunction with the client is vital to ensure the relevance to the person and requires a degree of skill and professional reasoning from the clinician. 30
While there was general agreement that the VR experiences were engaging and valuable, there were individual differences in the experience of VR reported by each post-stroke participant. There was no universally accepted factor that promoted engagement and motivation. Given that each VR scenario contained unique blends of realism, gamification, scoring, coaching and feedback, this suggests that an effective VR therapy platform needs to provide opportunities for choice amongst a range of scenarios. This will enable the design of individualised VR therapy programmes in line with personal preferences. In addition, there was recognition by both expert clinicians and post-stoke participants that it was important to be able to scale VR experiences to match the movement capacity of the user. This tailoring is perhaps the single most unique feature of VR therapy in that it enables participants to complete tasks in a virtual format that they are unable to complete in a traditional therapeutic context.
Both clinicians and participants identified modifications to the programme or equipment to improve its functionality, with the main point being that end users should have significant input into the process. This is consistent with literature that highlights the importance of involving both therapists and clients in the development and application of VR experiences. For example, a study 27 examined four cases of therapist/client involvement in VR and augmented video game research and found that involving both clinicians and clients in this process led to a better appreciation of the pragmatic barriers that exist when implementing VR therapy in a clinical setting.
In this study, improvements suggested by the clinicians included allowing for graduated activities and different movements, better qualitative and/or quantitative feedback to the client, and the ability to be able to log in and monitor client progress and to build in experiences with lower levels of function. Importantly the improvements were mainly aimed at ensuring that the required task-specific repetition required to improve motor function after stroke was maintained or improved. These strategies are consistent with the literature on improving clinician control, functionality of the VR and user support. 27 Interestingly, post-stroke participants and clinician participants recognised the importance of making the VR scenarios fun and relatable would encourage the high-volume practice and performance monitoring needed. In addition, post-stroke participants identified a need for therapists to be available to address technical and physical access issues when participating in VR therapy.
The average post-stroke time of the participants in this study was 10.4 years. While it is known that most motor recovery occurs between 3 and 12 months post-stroke, recovery can still occur two years and longer after stroke28,31
Limitations
Because this study commenced at the beginning of the COVID-19 pandemic, data collection was halted multiple times as restrictions to working with research participants affected the research site. This caused a delay between gathering clinician data and stroke survivor data, and then an extended period of data collection for stroke survivor experiences. The small sample size of participants means the results can be used as a guide only rather than being generalisable. A restricted set of VR experiences were available to participants and these were influenced by the content developer's understanding of stroke therapy needs. While rich data was gathered from each of the participants, the limited number of participants restricts the generalisation of findings beyond the scope of this study. While the suite of VR scenarios provided a range of experiences for participants and incorporated a number of relevant VR characteristics, it cannot be assumed that these reflect the limit of possibilities for VR therapy. Due to COVID-19 restrictions, there was a 12-month break in data collection which may have impacted the results and temporal association between the views of the clinicians and participants who enrolled before the break and after.
This study investigated the potential of VR experiences to enable stroke survivors to engage in activities that could improve recovery of upper limb function, however, no evaluation was made of the effectiveness of this form of therapy and so the therapeutic power of VR as a component of rehabilitation from stroke requires subsequent investigation.
Conclusion
This study aimed to describe the experiences and opinions of two expert clinicians and seven post-stroke survivors in relation to five VR experiences. Differences in the experience and preferences of stroke participants regarding the characteristics of the VR experiences indicate that a variety of experiences are necessary to engage and sustain participation in VR-related therapy programmes. Tailoring therapy to accommodate for individual differences in upper limb capacity was seen to be an important factor in supporting the widespread use of VR therapy. Further evaluation of the efficacy of VR programmes in addressing therapy goals is indicated.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241251634 - Supplemental material for Virtual reality after stroke: Identifying important characteristics when designing experiences to improve engagement in upper limb rehabilitation
Supplemental material, sj-docx-1-dhj-10.1177_20552076241251634 for Virtual reality after stroke: Identifying important characteristics when designing experiences to improve engagement in upper limb rehabilitation by Stephen Isbel, Helen Holloway, Craig Greber, Kelly Nguyen, Jane Frost, Claire Pearce and Nathan M D’Cunha in DIGITAL HEALTH
Footnotes
Contributorship
CG and SI conceived the study and researched the literature. KN and HH collected the data. CG wrote the first draft of the manuscript with all authors reviewing manuscript drafts and approving the final version.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CD owns Recovery VR who provided the VR headsets and co-funded the research. CD was not involved in the data collection or analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a University of Canberra TIGER grant.
Ethical approval
This research was approved by the University of Canberra Human Research Ethics Committee (HREC 2096).
Guarantor
SI.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.