
Abstract
The paper presents a multisensory and multimodal device for neuromuscular rehabilitation of the upper limb, designed to enable enriched rehabilitation treatment in both clinical and home environments. Originating from an existing low-cost, variable-stiffness rehabilitation device, it expands its functionalities by integrating additional modules in order to augment application scenarios and applicable clinical techniques. The newly developed system focuses on the integration of a wearable neuromuscular electrical stimulation system, a virtual rehabilitation scenario, a low-cost unobtrusive sensory system and a patient model for adapting training task parameters. It also monitors the user behavior during each single session and its evolution throughout the entire training period. The result is a modular, integrated and affordable rehabilitation device, enabling a biomechanical, neurological, and physiological-based training of patients, including innovative features currently unavailable within off-the-shelf rehabilitation devices.
Keywords
Introduction
Motivation
Neurorehabilitation can take advantage by the exploitation of robotic devices specifically designed to assist the patient and the medical personnel during the recovery. Patients can typically benefit of a period of hospitalization in the first weeks after stroke, during the acute and part of the subacute phase, in which neuroplasticity plays an important role in the recovery process. However, after this period, they require to continue intense and assisted rehabilitation therapies at home. In fact, experimental studies show that plasticity phenomena can be stimulated by robotic intervention even in the chronic phase thus underlying the importance of rehabilitation after discharge.1–3 Some clinics can afford the purchase of expensive, complex and cumbersome devices, but these same aspects make such devices not suitable to be installed and used at patients’ home and in low-resource settings. Such a situation urges to the prompt identification and adoption of low-cost solutions enabling a rationalization of the health service resources, in order to allow a wide diffusion of rehabilitation devices. 4 A rehabilitation practice based on the use of low-cost devices may meet the needs of low-resource settings, both in developed and developing countries, in some cases characterized by lacking health care systems and insufficient medical personnel. Rehabilitation devices aiming at being used intensively and largely should be intuitive, easy, fast to set-up, and have a reasonable price. They should moreover feature assist-as-needed and adaptable control strategies, explicitly designed to provoke motor plasticity. 5 In fact, each neurological patient has different impairments, functional abilities and recovery capabilities. Interactive and adaptable functionalities allowing personalized levels of assistance represent a looked-for feature, currently hardly available in affordable rehabilitation devices. Their capability of adapting rehabilitation parameters according to the actual functional level of patients can represent a breakthrough solution to increase the overall quality of recovery for a large amount of stroke patients and, additionally, favor an autonomous use by patients, without requiring a continuous direct intervention of the medical personnel.
State of the art
Different upper-limb low-cost rehabilitation devices are currently available, but they are typically passive or passively gravity-balanced. 6 Despite the effectiveness of these solutions, the lack of actuation and of an assist-as-needed support precludes them to be effectively used by patients with low-medium motion capabilities. The vast majority of robotic devices are used only in therapeutic institutes because they require supervised assistance from qualified personnel, and their price is often prohibitive for domestic environments and, in general, for low-resource settings. 7
Since the invention of the MIT-Manus, 8 force-feedback and force-based control are standard features of neurorehabilitation devices,5,7 enabling them to sense and react to patient interactions with the robot and adapt the level of physical assistance provided to the patient. In fact, a rehabilitation procedure pursuing high-impact training must be characterized by the possibility of customizing the training task and optimizing the difficulty for each patient. However, mere position and force control of the robotic device are inadequate to determine comprehensively the appropriate level of task difficulty. A multisensory and multimodal bio-cooperative controller, able to infer the appropriate level of challenge, difficulty and complexity of the training task most suitable for the user, is known to be beneficial. This approach was first demonstrated by Novak et al., 9 exploiting a multimodal virtual environment with adjustable difficulty levels. 10 The bio-cooperative control approach requires a multisensory system for measuring kinetic, kinematic and physiological parameters. The use of state-of-the-art wearable sensors to close the loop from a physiological point of view has already been applied, 11 but those sensors were difficult to attach.
Focusing on the mechatronic actuation schemes of rehabilitation devices, rigid mechanical actuations coupled with force sensors or back-drivable transmissions are typically employed to infer the interaction force between the device and the patient. However, in recent years, the effectiveness of adding mechanical compliance to the actuation system is being explored. The use of variable-stiffness actuators (VSAs) can represent a promising technology,12–14 owing to their inherent adjustment of the mechanical stiffness, force estimation, and robustness to external perturbations in physical human-robot interacting scenarios. Referring to devices for rehabilitation, examples of VSA-based devices are exoskeletons for the upper limb,15,16 a bipedal robot exploiting VSA to control the knee stiffness, 17 a variable-stiffness treadmill (VST) for the investigation of gait, 18 and one-degree-of-freedom end-effector devices for upper-limb reaching rehabilitation.19,20
Finally, hybrid assistive systems, which have been realized with the aim of combining advantages of both functional electrical stimulation (FES) and electromechanical actuation, have been proven to be an optimal method for promoting the recovery of the upper-limb function in hemiplegic individuals. 21
Specifically referring to transcutaneous electrical stimulation systems, they can elicit sensory feedback in conditions of electrotactile feedback, or elicit muscle contraction with higher intensity stimulation. Vibroelectrotactile solutions allow parallel sensory information coding in healthy subjects, 22 but the amount of vibratory information perceivable by neurologically compromised subjects is limited. 23 On the contrary the electrotactile sensation by means of transdermic stimulation is in general more preserved on a variety of neurological patients.
LINarm++
In this context, an affordable, adaptable, and hybrid-assistive modular device for upper-limb neurorehabilitation is being developed with the aim of fulfilling requirements of low-resource settings, with a set of features enabling a multi-modal rehabilitation paradigm. Its modularity enables it to be configured according to the actual needs and budget capabilities of the actual usage environments. LINarm++ (Figure 1) is an advanced version of the previously developed LINarm, a VSA robotic device for the rehabilitation of the upper limb.
19
LINarm++ features robot–FES hybrid rehabilitation and assist-as-needed functionalities based on a constantly updated model of the patient, based on kinematic, kinetic, and physiological quantities. The work is organized as follows. The LINarm++ architecture is described in the next section. In the subsequent section, the modules directly interacting with the patient and their specific functionalities are described in detail. Then, the control system and the patient model are described, focusing on the adaptability of training parameters according to patient performances. Conclusions and suggestions for future work are presented in the last section.
The prototype of the LINarm++ rehabilitation platform. (a) Detailed view of the LINarm++ mechatronic device. (b) Use of LINarm++ with the virtual environment and the sensorized handle.
The LINarm++ rehabilitation platform
The LINarm++ rehabilitation platform is a multisensory and multimodal system made up of the following set of optional modules interacting with the patient (Figure 2).
a redesigned version of the mechatronic device LINarm,
19
namely LINarm2, characterized by an optimized design and embedding a novel VSA architecture; a low-cost unobtrusive sensory system for measuring the patient’s physical activity and his physiological state, in order to obtain and constantly update a comprehensive state of the patient; an easily wearable FES system, allowing selective and effective stimulations of upper-limb muscles; engaging online adaptable rehabilitation scenarios and virtual environments, which adapt during the training to the level of difficulty that is most appropriate for each individual subject, to ensure the best level of subject’s activity in terms of motor and cognitive engagement.
Representation of the LINarm++ rehabilitation platform.

The entire platform is managed by a central control system in charge of synchronizing and updating rehabilitation parameters in accordance with a patient model. The patient model is in charge of determining training task parameters in relation to the user’s performance and the physical/physiological state, in order to influence the user’s engagement and performance, with the aim of fulfilling the actual needs of the patient during the therapy.
The platform is made up of a set of modules summarized hereafter and depicted in Figure 3.
UML representation of the LINarm++ architecture.
The medical personnel control and supervise all the system through the LINarm++ GUI (graphic user interface). The LINarm++ manager is in charge of coordinating all the sub-modules according to the selected control modes and functions. It receives streams of different data, as kinematics, physiological parameters and level of assistance, dispatches them to other devices and applies control logics and functioning modes.
The patient is interfaced to the system in a multimodal way. The LINarm mechatronic device physically supports the execution of rehabilitation tasks, a set of physiological sensors measures different physiological data, a set of neuromuscular electrical stimulation (NMES) electrodes controlled by an electrostimulator constitutes a FES system and a monitor is in charge of rendering game scenarios to engage the patient.
All data collected by the LINarm++ manager are made available to the patient’s model device in charge of estimating the patient’s state and the required assistance level, exploited to determine both the robotic and the FES assistance to be given to the patient.
The communication among the nodes of the architecture is performed exploiting USB and UDP communication protocols, exploiting the robotic operating system (ROS) framework to facilitate the integration of the modules.
Multi-modal interacting modules
The four main submodules directly interfaced to the patient are described in detail hereafter.
LINarm2
The rehabilitation platform embeds LINarm2 (Figure 4), a new version of a previously developed VSA robotic device for the rehabilitation of the upper limb.
19
Its seemingly simple linear movement has been defined in accordance with the following rationale. Considering that the upper limb is an incredible adaptive organ capable of performing numerous functional tasks in an infinitive number of kinematic solutions, it is recommended to select a set of primitive movements to be trained in order to minimize the complexity of a rehabilitation device and maximize its affordability and portability. As most actions involving the use of the upper limb are performed to interact with objects positioned in front of the subject and to eventually take them towards the body, two movements become of particular interest, namely and, respectively, the reaching and the hand-to-mouth. These two functional movements, which are representative of ADLs like reaching for objects and eating, are correlated with the activity capacity level after stroke.24,25 Although these movements are quite complex, in the author’s experience wrist trajectories may be approximated to straight lines.
26
Hence the choice to realize the linear device. In order to facilitate the radial and ulnar deviation movements, typical of the hand-to-mouth, the LINarm2 handle will be provided with a turning joint in the near future.27
The LINarm2 mechatronic device. (a) Assembled view of LINarm2. The motion of the mobile unit is constrained linearly by two linear guides. Two motors actuate two antagonist wires connected to the VSA mechanism. A spherical joint allows orientation of the device along different directions, as depicted in Figure 5. (b) Mobile unit of LINarm2. A single shaft supports the cams, constrained by torsional springs, of the VSA actuation architecture.
LINarm2 can be fixed on a table or a tripod supported by a spherical joint installed at one of its extremities, enabling it to be oriented along different directions allowing the execution of reaching movements along different inclinations (Figure 5(a)), hand-to-mouth movements, and also movements along other directions as lateral movements normal to the sagittal plane (Figure 5(b)).
Examples of installation of LINarm2 to perform movements parallel and normal to the sagittal plane. (a) Frontal reaching. (b) Lateral movement.
The mechatronic device is controlled by an Arduino DUE, a low-cost general purpose board featuring a Cortex M3 microcontroller. The real-time controller features passive and force-based control strategies, inferring that the force applied by the user is known from the force–displacement characteristic of the VSA embedded in the device (see Figure 9).
Linear wire wrapped cam VSA
LINarm2 embeds the linear wire wrapped cam VSA (hereafter LinWWC-VSA), a novel agonist–antagonist VSA mechanism based on two nonlinear springs realized by a hinged cam constrained by a torsion spring and actuated by a wire-based transmission (Figures 6 and 7). A comprehensive description and analytical details of the LinWWC-VSA can be found elsewhere.
28
The nonlinear spring embedded in LINarm2. The nonlinearity of the virtual spring kl is obtained by a hinged spiral cam c, wrapped by a wire w and constrained by a torsion spring kt. The spring elongation ΔxE denotes the displacement along x of E w.r.t. the configuration with the cam completely wrapped by the wire, i.e. T coincident with B. Frontal view of the LinWWC-VSA embedded in the mobile body of LINarm2. The two coaxially hinged cams c1 and c2 realize two nonlinear springs, as represented in Figure 6.

Leaving out details about the cams profile and the torsion springs embedded in LINarm2 for sake of brevity, the stiffness kl as a function of its elongation ΔxE (Figure 6) is represented in Figure 8.
Translational stiffness of the virtual spring kl as function of its elongation ΔxE. The ratio between the maximum and the minimum stiffness is about 10.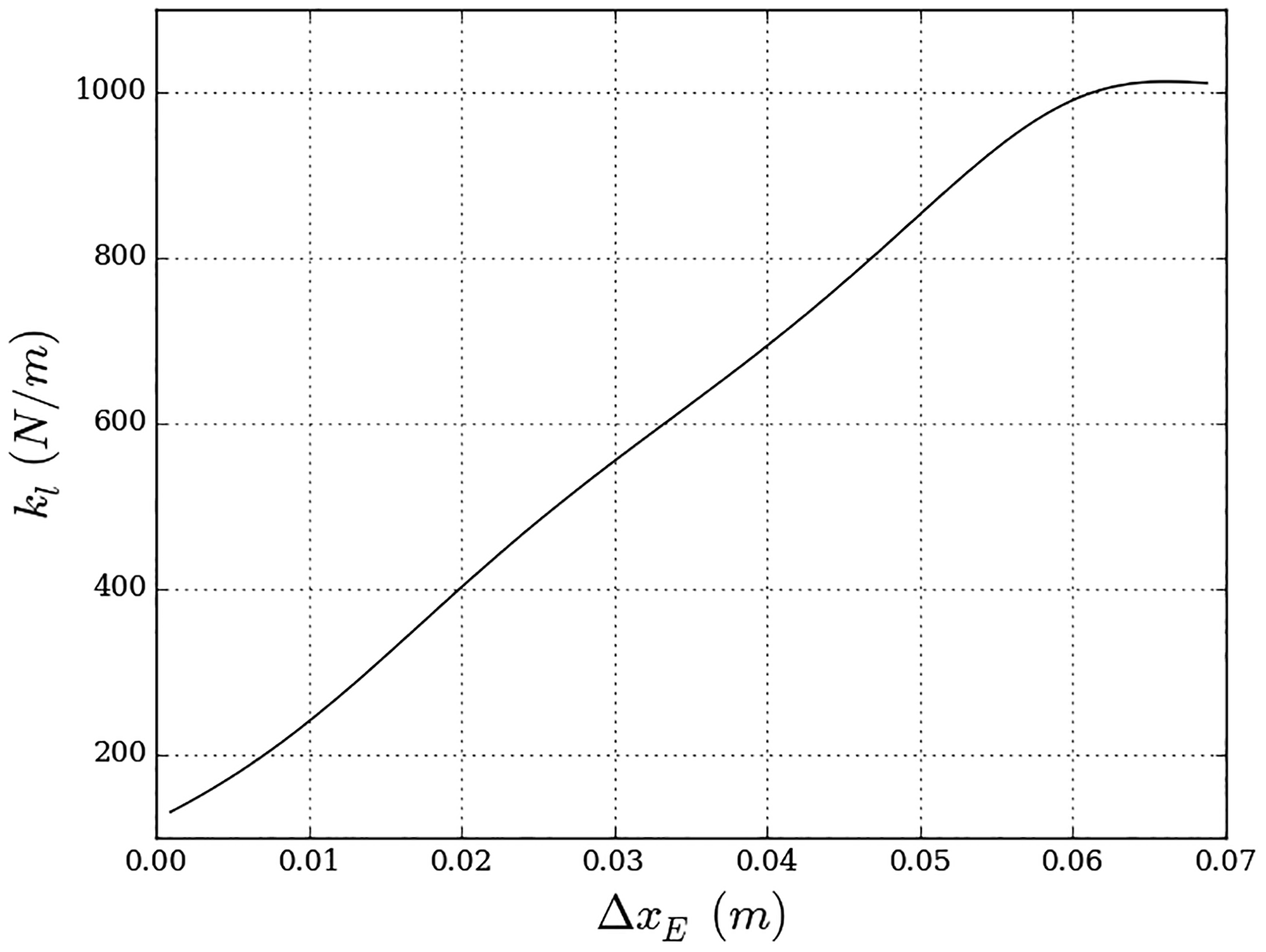
Let us denote by ΔxE,1 and ΔxE,2, respectively, the elongation of the two cams c1 and c2 coaxially hinged as represented in Figure 7. In order to analyze the force and the stiffness of the VSA, it is convenient to define the variation of distance between E1 and E2 as


The resulting force fa and stiffness ka of LinWWC-VSA as a function of δ and ξ are reported in Figure 9. Both fa and ka grow with the growth of δ, keeping ξ constant. The maximum value of fa is achieved with the highest value of ξ, with δ = ξ. The maximum value of ka is achieved with the highest value of δ with ξ = 0. In conclusions, the stiffness of the mobile body can be tuned actuating the agonist–antagonist mechanism. Moreover, fa can be conveniently used to estimate in real-time the force externally applied by the patient to the mobile body, given δ and measuring ξ.
Physiological sensors
In order to measure physiological parameters targeting home rehabilitation, an unobtrusive physiological measurement system consisting of low-cost sensors have been developed. It is designed in such a way that it does not need to be attached to the user, do not requires instructions and, in the best case, the user will not even need to be aware of the sensors. Sensors are integrated into the handle (Figure 1(a)), which is the interaction point (also serving as the attachment point if user’s hand needs to be fixated to the robot) between the user and the training device. Three primary physiological measurements, obtained by proper sensors, have been chosen: electrocardiography, skin conductance and peripheral skin temperature. Other physiological sensors, as the one for measuring the respiration rate, were not included in the system in order to respect the requirement of unobtrusiveness to facilitate the autonomous use of the system by impaired people. A prototype with sensors embedded into the handle was tested against a high-quality reference measuring system manufactured by g.tec (Graz, Austria). The aim was to show that the low-cost system with sensors embedded into the handle can provide results, which are comparable to results acquired with a high-quality and costly solution. The validation was performed in different operational conditions. Tested were two handle shapes that require different grasping configurations. A cylindrical handle (c-handle) requires a power grasp, while a hemispherical shape (s-handle) allows the hand to rest on the handle. The two configurations therefore change the force that is applied on the physiological sensors during measurement. The system was tested in four tasks that were designed as different combinations of physical and cognitive (different game dynamics) loads: Task 1 (low physical load and low dynamics), Task 2 (low physical load and high dynamics), Task 3 (high physical load and low dynamics), and Task 4 (high physical load and high dynamics). Figure 10 shows the validation results for three physiological parameters: (a) mean heart rate (HR), (b) standard deviation of NN intervals (SDNN); and (c) mean skin conductance level (SCL). All results are presented as a difference from baseline interval when the subject was resting quietly. Results show good matching between the low-cost and the reference sensory system. The differences in the measured SCL are mainly the consequence of placements of electrodes in different positions (reference measurement on the right hand and the validated system on the left hand) due to the physical and electrical constraints.
Force fa and stiffness ka of the LINarm2 mobile body as function of δ and ξ. Validation results for three physiological parameters: (a) mean heart rate (HR), (b) standard deviation of NN intervals (SDNN); (c) mean skin conductance level (SCL).

Neuromuscular electrical stimulation system
NMES can be conveniently modulated both to assist the subject in the movement and to provide perceptive cues.29,30 In fact, if delivered at low frequencies with intensity below the motor threshold can be used for eliciting a sensory response, if delivered at intensities above the motor threshold (e.g. at 30 Hz), can induce muscle contraction regardless the ability of the subject to recruit volitionally the targeted muscle. For simplicity of wearing and parsimony of the overall number of channels, minimizing the requirements of the electrostimulator, only two muscle groups are elicited by NMES in each exercise and are empirically chosen as the proximally dominant and distally dominant muscle for each action. Hand-to-mouth assistance relies on the stimulation of the biceps brachii and of the brachioradialis, whereas reaching assistance uses the deltoid anterior and the triceps. On the basis of this rationale and to fulfill the ease-of-installation requirement, the NMES system comprises an electrical stimulator (Rehastim One, Hasomed GmbH, Magdeburg, Germany), standard transcutaneous electrodes and customizable sleeves which aims to simplify the positioning of the electrodes on the subject (Figure 11).
Wearable for FES motion assistance. (a) The muscles targeted by FES are the deltoid anterior (DA), triceps (TR), biceps brachii (BBR), and brachioradialis (BRA). (b) The targeted muscles use a pseudomatrix, made with commercial electrodes (Pals, Axelgaard Inc) on a plastazote foam (Ottobock Healthcare Inc). The pseudomatrix is fixed inside the garment on the targeted muscles. (c) Alternatively, a custom matrix can be used (silver screen printing on 300 µm Mylar, EPFL).
The active component of each exercise is split in two independent tasks. The active component of each exercise is split in two independent tasks. NMES has to elicit, for each task, a response able to support motion in the main expected direction. The optimal location of stimulation and intensity is obtained through a ranking process. Each targeted muscle uses a multi-electrode wearable containing four independent active electrodes and a common reference electrode.
The selection of the current intensity i and of the location of stimulation in the multi-electrode is performed during the calibration phase, compensating for sub-optimal positioning or avoiding to stimulate areas that could elicit adverse sensations.
Since each muscle is deemed responsible for a specific task, t, the calibration procedure aims at finding the best responsive electrode, e, which is able to elicit the force Φ t expected to be necessary for the task.
The scan proceeds sequentially for each task, for each electrode, with the current ramping in intensity up to I = imax, or interrupted with the pain button.
During the identification procedure, the stimulation frequency is set to F = 30 Hz and the pulse width is set to half of the dynamic range of the stimulator. The stimulation parameters for each task t are identified as the combination of location et and the minimum current It,e necessary to elicit the target force. If more than one electrode per matrix is suitable to induce motion without discomfort, the one with minimal current is chosen.
The stimulation able to induce motor contraction is used in a non-patterned fashion and the stimulation profile is continuous with the movement. Once location and current intensity are defined, the stimulation intensity is obtained by means of pulse width modulation. The NMES assistance can be modulated in accordance with the percentage of the LINarm2 movement cycle and according to preset activation profiles, chosen among a set of approximated biomimetic responses.
Virtual feedback
Post-stroke patients tend to suffer from a lack of interest in the ongoing rehabilitation procedure. In order to ensure adequate motor ability improvements and sufficient engagement, the use of dedicated computer games can guarantee that the subject’s attention is properly gained and maintained throughout the rehabilitation task. LINarm++ embeds a set of games sharing a common concept: the aim is to intercept a virtual object whose trajectory crosses the direction of movement of the virtual object controlled by the patient. The active component of each exercise is split in two independent tasks. The parameters which can influence the difficulty are the speed of the moving object and the dimensions of the moving and user-controlled object.
The scenarios continuously adapt to the most appropriate level of difficulty, to ensure the best level of subject’s activity. In accordance to the patient’s skill and level of impairment, difficulty adaptiveness is in terms of not only motor but also cognitive challenge, in order to increase the overall subject engagement. Figure 12 shows two games, in the first the subject has to catch the falling balls (motor challenge), while in the latter the subject needs to move the robot, represented as the ball, to the correct answer (motor and cognitive challenge).
Two examples of games. (a) Only motor challenge. (b) Motor and cognitive challenge.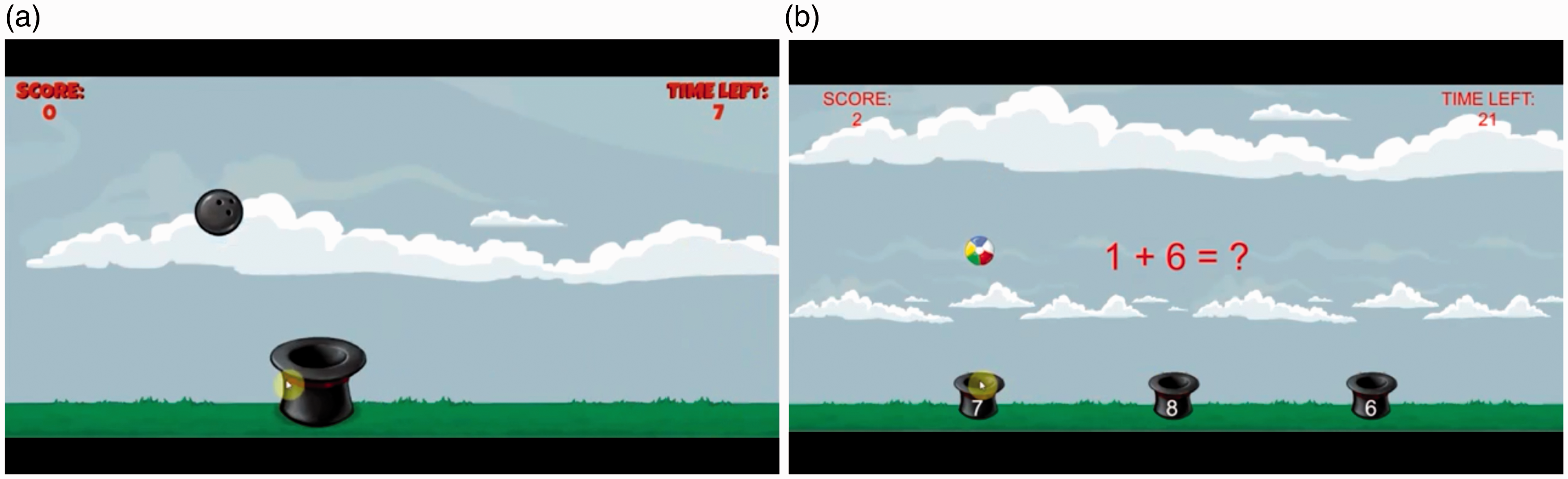
For details about the assistance force, generated towards the virtual moving object by the mechatronic device, refer to the next section.
Adaptable hybrid assistive control
In addition of executing real-time control algorithms, the control system is in charge of modifying control parameters according to information provided by the patient model (Figure 3). The patient model makes use of the collected sensory information to optimize the parameters of the training task on the basis of the user’s physical and physiological state, and activity. In particular, it exploits the information gathered by the following sensors installed on the LINarm++ device: three rotary encoders are installed on the LINarm++ mechatronic device to measure in real time the position of the motors and of the mobile handle, leading to evaluation of power, velocity, interaction force, movement smoothness, and deviation from the ideal trajectory planned by the motor control; one grasp sensor and three physiological sensors are embedded in the handle of the device to measure the grasping force, the heart rate, skin conductance, and temperature.
Since the data collected from sensors are raw signals and the outputs need to be parameters of the training scenarios, the algorithm is organized in several steps:
Signal pre-processing (filtering, noise removal, bias removal, normalization, etc.). The output signals are fed into the patient model. The patient model is divided into two sub-models:
– The patient performance model estimates various parameters related to physical activity and task performance. – The physiological model fuses data from sensors (embedded into the handle), which measure physiological signals. Outputs are parameters summarizing the information about the physiological state of the user. The main focus is on observation of trends of physiological parameters in order to optimize training activity. Output of patient model are analyzed both in terms of absolute parameters and, more importantly, in terms of trends of signals. Based on that training, settings should be optimized in order to keep the parameter values within the adequate boundaries.
The patient model is organized by a decision tree (see Figure 13) with three distinctive layers of nodes:
Task performance index (TPI) layer calculated from various parameters related to performance in the particular game (score, time to complete the task, number of errors). Scores can be computed differently according to the specific game played, e.g. number of objects correctly caught or placed on the target. Motor performance index (MPI) layer calculated from various parameters related to movement and force (power, velocity, interaction force, grasp force, movement smoothness, deviation from ideal trajectory, robot support). Physiological trend index (PTI) layer calculated from various parameters measured by physiological sensors (heart rate, heart rate variability, temperature, skin conductance response, and skin conductance level). All the parameters are differences between baseline levels and levels measured during the task.
Decision tree of the patient model with the equation for calculating the assistance level a.

Each index is a linear combination of the parameters used to calculate the index. An index is limited to values between 0 and 1. The weights for parameters included in calculation of the particular index are determined algorithmically by using linear classifiers (e.g. linear discriminant analysis, Naive Bayes classifier). This requires a learning set gathered using preliminary experiments with fixed values of difficulties.
An example for PTI is given by following equation


Cognitive challenge is adjusted using questions or cognitive tasks (e.g. Figure 12(b)) divided into two distinctive levels by difficulty. Cognitive tasks are taken from established psychological tests used to test the cognitive load. The level of cognitive challenge is adjusted based on user’s score. A fixed threshold is used to change the difficulty of the cognitive task. If the user answers correctly to a series of cognitive tasks the difficulty is increased and vice versa.
The assistance provided by both the LINarm2 device and the NMES system is determined by the assistance level a calculated by the patient model. As schematized in Figure 14, a is used to calculate the robot assistance level ar and the FES assistance level af, exploiting the two parameters kr and kf, respectively. The medical personnel define 0 ≤ kr ≤ 1 (robot assistance gain) and 0 ≤ kf ≤ 1 (FES assistance gain), enabling to define the amount of robot and FES assistance according to specific patient’s needs and impairment. The robot assistance ar is used to determine three parameters of the mechatronic device: km is proportional to the mechanical stiffness of the VSA embedded in LINarm2, ka is the gain of the admittance-based control, kt is the gain of the assistive controller, in charge of assisting the patient to reach the target represented on the virtual scenario. The combination of these three parameters (Figure 14) determines the following notable conditions: ar = 1 stiff robot (km = 1; ka = 0) and high assistance by the controller (kt = 1) to achieve a behavior similar to continuous passive motion devices; ar = 0 compliant robot (km = 0; ka = 1) and no assistance by the controller (kt = 0) to achieve the maximum transparency for free movements; ar = −1 stiff robot and low assistance (km = 1; ka = 0) and no assistance by the controller (kt = 0) to realize a resistive controller to increase the patient’s challenge in achieving targets. The FES assistance af controls the pulse width defining the stimulation intensity (see previous section) according to the patient’s needs.
Parameters defining robotic and FES assistance are computed starting from the assistance level a.
In conclusion, all the parameters defining both the mechatronic and the FES assistance are derived by the assistance level, inferred by the patient model, in turn defined by a set of continuously updated kinematic and physiological parameters, and game scores.
Conclusions
LINarm++ realizes a multifunctional hybrid assistive system for upper-limb rehabilitation, aiming at supporting hospitals and clinics to treat the inpatients in a personalized way, featuring modularity and adaptation to the actual patient’s needs. Both the mechanics and electronics have been specifically designed to fulfill low-cost requirements. Hardware and software modularity meets the need of satisfying the requirements and budget availability of different clinical centers. Its affordability and semi-autonomy in targeting patient’s needs can enable more than one patient to be treated simultaneously, increasing labor productivity and improving the overall services for the patients. These same characteristics facilitate its use in a domestic environment, giving the patients the chance of being treated directly at home with challenging and personalized exercises, exploiting device adaptability to conditions and improvements of each specific patient. The platform features self-adaptation of rehabilitation parameters during its functioning and includes auto-tuning procedures during the setup, as the one to identify the muscles to be stimulated by the NMES system, allowing a rough positioning of the electrode pseudomatrixes on the arm, without requiring deep medical knowledge. Nevertheless, a proper training of patients and caregivers will be required, especially where highly-specialized medical staff is not available as in developing countries, providing appropriate anatomical tables for a correct use of the device. In general terms, the system aims at satisfying the increasingly larger request of more and more effective and affordable technologies complementary to traditional rehabilitation techniques, to face population ageing and the related increase of neurological diseases. The first LINarm++ prototype is currently available, technical and its clinical assessment is planned in the near future.
Footnotes
Acknowledgements
The authors would like to thank Joao Carlos Dalberto for supporting the mechanical design and the realization of the mechatronic prototype, Roberto Bozzi for its electrical wiring.
Funding
This work was partially supported by the European Commission with the collaborative project number FP7-ICT-601116, ECHORD Plus Plus – The European Coordination Hub for Open Robotics Development_within the LINarm++ Experiment.