
Abstract
People with multiple sclerosis (pwMS) have an increased risk of infection. As disease-modifying therapies (DMTs) and other treatments may interact with the immune system, there may be concerns about vaccine efficacy and safety. Therefore, it is important to evaluate possible interactions between DMTs and vaccines. The fumarates, dimethyl fumarate, diroximel fumarate, and monomethyl fumarate, are approved for the treatment of relapsing multiple sclerosis. This review assesses the evidence on vaccine response in pwMS treated with fumarates, with a particular focus on COVID-19 vaccines. Treatment with fumarates does not appear to result in blunting of humoral responses to vaccination; for COVID-19 vaccines, particularly RNA-based vaccines, evidence indicates antibody responses similar to those of healthy recipients. While data on the effect of fumarates on T-cell responses are limited, they do not indicate any significant blunting. COVID-19 vaccines impart a similar degree of protection against severe COVID-19 infection for pwMS on fumarates as in the general population. Adverse reactions following vaccination are generally consistent with those observed in the wider population; no additional safety signals have emerged in those on fumarates. Additionally, no increase in relapse has been observed in pwMS following vaccination. In pwMS receiving fumarates, vaccination is generally safe and elicits protective immune responses.
Introduction
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease of the central nervous system and is the most common non-traumatic disabling neurological disease in young adults, affecting approximately 2.5 million people worldwide. 1 Currently, there are several different classes of disease-modifying therapies (DMTs) available for the treatment of MS, which selectively modulate or suppress the immune system. 2
People with MS (pwMS) are at increased risk of infection compared with the general population, 3 potentially as a result of immunosuppression due to treatment or as a consequence of MS-related functional limitations and disability.4–6 The risk of serious infection is most highly increased in pwMS with more severe disability and in those with progressive MS. 6 Therefore, the risk of infection in this patient population highlights the importance of mitigation strategies to prevent infections, including vaccination, and risk–benefit assessment in the selection of suitable DMTs.4,7,8 However, there may be some degree of hesitancy to get vaccinated due to fears of relapse and other safety concerns, along with insufficient or inaccurate knowledge about vaccines.9,10
Vaccination in patients with MS
Increasing protection against infectious diseases in pwMS has received much attention since the global COVID-19 pandemic was declared in 2020, not least because the use of certain DMTs has been associated with a higher risk of infection and increased severity of COVID-19. 11 Numerous studies have indicated an increased risk for severe COVID-19 in people treated with anti-CD20 monoclonal antibodies (mAbs) compared with other DMTs.11–13 Pivotal trials for both the Moderna mRNA-1273 and Pfizer/BioNTech BNT162b2 demonstrated >90% efficacy at preventing symptomatic COVID-19, and nearly eliminated severe disease.14,15 In a study of 317 pwMS, full vaccination against COVID-19 (n = 97) was associated with a significantly decreased risk of severe COVID-19 infection at a median of 5 months post-first vaccination compared with unvaccinated patients. 16
With this review, we sought to examine the available evidence regarding the vaccine response in pwMS receiving treatment with oral fumarates, with a particular focus on influenza and COVID-19 vaccines, and with consideration given to dosing and timing of DMT. Briefly, literature searches were conducted using PubMed from March 2022 and carried out periodically until June 2023 to identify any key developments. Searches were conducted using combinations of the following terms: “COVID-19”; “vaccine”; “vaccination”; “multiple sclerosis”; “MS”; “disease-modifying therapy”; “DMT”. Searches specifically related to fumarates included the term “fumarate.” Additional references were sourced based on the author group's own knowledge of the area. Recommendations from MS groups and societies were accessed manually.
Vaccine response with DMTs
While it is evident that COVID-19 vaccines are effective at reducing the risk of severe infection, prior or concomitant treatment with DMT may impact vaccine efficacy. Some DMTs, particularly anti-CD20s and sphingosine-1-phosphate receptor modulators (S1PRMs), appear to blunt humoral responses both to vaccines in general,17,18 and specifically to COVID-19 vaccines.19–21 Furthermore, T-cell responses are preserved with anti-CD20s, glatiramer acetate, natalizumab, fumarates, and other DMTs, but may not be preserved with S1PRMs.20–22 Accordingly, studies have revealed differences in the clinical efficacy of COVID-19 vaccines dependent on the type of DMT a patient receives. Post-vaccination, pwMS on anti-CD20 therapy or fingolimod demonstrate significantly higher risks of breakthrough COVID-19 infections compared with pwMS on other DMTs and compared with the general population.23–25 COVID-19 vaccine efficacy was preserved in pwMS receiving other DMTs, including dimethyl fumarate (DMF), glatiramer acetate, interferons (IFNs), natalizumab, and teriflunomide.23,25 Interactions between DMTs and the immune response present a significant concern for the timing of vaccination and the preservation of vaccine efficacy in pwMS. Vaccination is an important component of patient care and is recommended by several MS groups and societies worldwide, with considerations for timing based on the vaccine type, infection risk, and specific DMT class (Table 1).26–32
Guidelines for vaccination in pwMS.
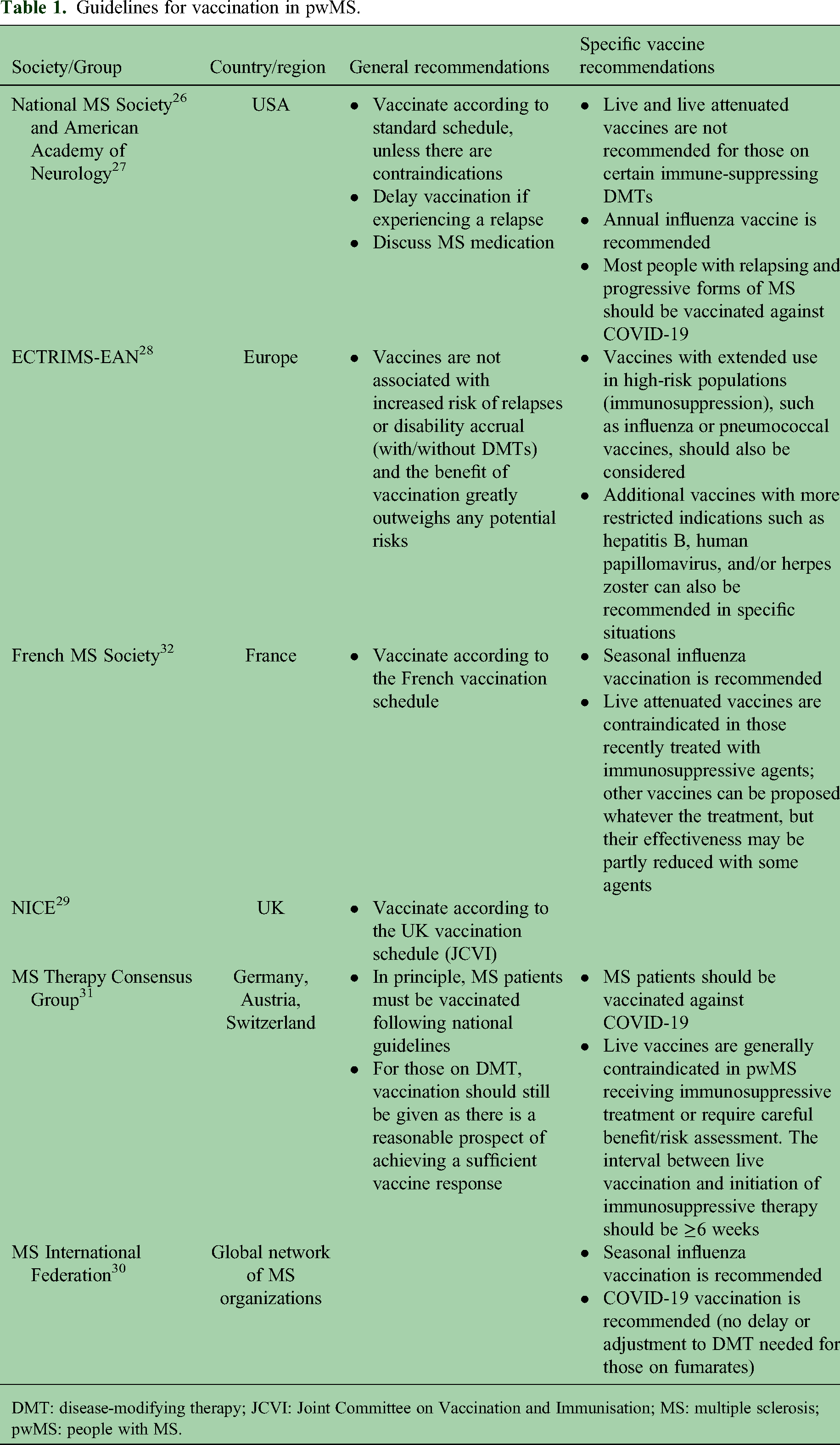
DMT: disease-modifying therapy; JCVI: Joint Committee on Vaccination and Immunisation; MS: multiple sclerosis; pwMS: people with MS.
DMF and diroximel fumarate (DRF) are oral DMTs that have been approved in Europe and the USA, as well as in other countries, for the treatment of relapsing forms of MS, 33 and share the same active metabolite, monomethyl fumarate (MMF). MMF is itself approved in the USA as an oral DMT for the treatment of relapsing forms of MS. The approved therapeutic doses of DMF (240 mg) and DRF (462 mg) produce bioequivalent exposure of MMF; therefore, comparable efficacy and safety profiles are expected at these doses. 34 It is anticipated that individual oral fumarate DMTs would have similar effects on vaccine response, although the data for DRF and MMF are currently limited.
Effects of fumarates on immune response and vaccine response
Mechanisms of action and immunological effects of fumarates in patients with MS
Fumarates demonstrate anti-inflammatory and antioxidant activity and appear to exert their therapeutic effects in pwMS through multiple mechanisms. In the central nervous system, fumarates may have a neuroprotective effect through the induction of antioxidant proteins via the nuclear factor erythroid-2-related factor 2 (Nrf2)-dependent pathway. 35 In the peripheral immune system, treatment with fumarates is associated with a decline in absolute lymphocyte counts and subsequent stabilization after 24 weeks.36–39 Depletion of T and B cells, and a subsequent reduction in pro-inflammatory cytokines, may be the immunological process by which DMF and DRF impart their effect on MS disease activity.39–41 However, specific subsets of T, B, and natural killer (NK) cells are affected to varying degrees.38,39 With DMF treatment, the most significant declines from baseline occur in memory subsets of T-cell and B-cell populations.39,41 In contrast, subsets of naive T and B cells increase, and the proportions of regulatory T cells are maintained.39,41 These changes may be mediated via immunoregulatory CD56bright NK cells, since the increase in the proportion of CD56bright NK cells with DMF treatment is correlated with reductions in CD8+ T cells, CD4+ and CD8+ memory T cells, and cytokine-producing CD4+ and CD8+ T cells.38,40 Overall, this represents a general shift away from pro-inflammatory lymphocytes and toward an anti-inflammatory profile, with increases in naive cells potentially being beneficial for generating an effective response to vaccination (Figure 1). The declines in CD4+ and CD8+ T cells and memory B cells and the shift to an anti-inflammatory response may be associated with the improvements observed in MS disease activity with DMF treatment.39,41 The end result more closely resembles immune homeostasis rather than an overt blunting of the immune response, as might occur with the depletion of immune cell populations. Accordingly, innate immune cell activation and antigen presentation are not expected to be impacted by fumarates, and the capacity to mount effective T-cell responses to antigens would be preserved. 20

Fumarates and the immune response to vaccination. Treatment with fumarates is associated with a shift away from a pro-inflammatory profile and an increase in naive/anti-inflammatory lymphocytes.
Response to vaccines in patients with MS receiving fumarates
Numerous studies have assessed the effect of fumarates on immune response in pwMS; current evidence regarding the impact of DMF and DRF on various vaccine types is summarized in Table 2. In a prospective study including 20 pwMS treated with DMF, the efficacy of the seasonal inactivated influenza vaccines 2020/2021 was assessed in pwMS based on the proportions who reached cut-off for seroprotection (hemagglutination inhibition assay of ≥1:40) or had an antibody increase of 4-fold for at least two of the four influenza strains. All pwMS were responders 30 days after immunization with the influenza vaccine, indicating an adequate humoral response. 42 As a marker for neuroaxonal damage, serum neurofilament light chain (sNfL) levels were assessed as the primary safety outcome and indicated no change from baseline to 30 days after vaccination in pwMS on DMF, possibly signifying that no reactivation of MS occurred. In addition, no significant differences were observed in sNfL level between people on DMF and healthy controls. 42 Following COVID-19 infection in two healthy controls and one pwMS, sNfL levels increased by more than 10 pg/ml in both control participants, but remained stable in the patient on DMF. 42
Evidence on the effect of treatment with DMF or DRF on response to selected vaccines.

DMF: dimethyl fumarate; DMT: disease-modifying therapy; DRF: diroximel fumarate; GA: glatiramer acetate; IFN: interferon; IgG: immunoglobulin G; MS: multiple sclerosis; pwMS: people with MS; RBD: receptor binding domain; S1PRM: sphingosine-1-phosphate receptor modulator; sNfL: serum neurofilament light chain.
An open-label study of patients receiving DMF or IFN for treatment of MS evaluated the immune response to three vaccines: tetanus–diphtheria toxoid to assess T-cell-dependent humoral response; pneumococcal 23-polyvalent vaccine to assess T-cell-independent humoral response; and meningococcal oligosaccharide CRM197 conjugate to assess T-cell-dependent neoantigen response. 43 Between DMF and IFN groups, responder rates (≥2-fold rise in anti-tetanus serum immunoglobulin G [IgG] levels) were comparable for all tested vaccines and no meaningful differences were observed between groups when stratified by age category or lymphocyte count. 43 These outcomes support that patients treated with DMF can mount humoral responses following vaccination comparable to those of patients on IFN. 43
Response to COVID-19 vaccines in patients with MS receiving fumarates
Most of the published data regarding efficacy in pwMS of vaccines developed against COVID-19 were generated in those who received mRNA vaccines, specifically Pfizer/BioNTech BNT162b2 and Moderna mRNA-1273. Since their authorizations for use, various studies have assessed the effect of DMTs, including DMF, on the immune response to these vaccines.
In a study of pwMS in Sardinia, Italy, it was observed that IgG titers elicited following two doses of Pfizer/BioNTech BNT162b2 in patients receiving DMF (n = 151) were similar to those of healthy controls (n = 63). 46 A real-world study of 322 pwMS from the USA, Germany, and Spain, who were vaccinated against COVID-19, also showed IgG response to be preserved in all patients who were treated with fumarates (DMF, n = 32; DRF, n = 5). 45 Most of these patients (92%) had received an mRNA vaccine, either Pfizer/BioNTech BNT162b2 or Moderna mRNA-1273. 45 Similarly, in a prospective, open-label, observational study of pwMS at a single center in the USA treated with fumarates, natalizumab, ocrelizumab, or IFN, all patients who received fumarates (n = 11; DMF or DRF) generated detectable anti-COVID-19 spike receptor binding domain (RBD) IgG titers 8 weeks after the initial dose of the Moderna mRNA-1273 COVID-19 vaccine, and mean IgG titers were similar to those in patients receiving natalizumab or IFN. 44 In an observational cohort study of pwMS receiving DMT (n = 338) at a center in Israel, all those on DMF (n = 35) demonstrated detectable anti-COVID-19 IgG after receiving the Pfizer/BioNTech BNT162b2 mRNA vaccine, with similar levels of IgG antibodies to healthy vaccinated subjects and in patients with untreated MS. 21 An Austrian study of pwMS on DMT who received COVID-19 vaccines reported seroconversion in 62 of the 63 patients who were on DMF, a rate of 98.4%. 19
The Oxford/AstraZeneca ChAdOx1-S and Johnson & Johnson/Janssen Ad26.COV2.S COVID-19 vaccines are adenoviral vector vaccines. Data for pwMS treated with DMF who received these vaccines are more limited compared with mRNA vaccines—for example, in the real-world study reported above 45 only three out of 37 patients receiving fumarates received a recombinant viral vector vaccine (ChAdOx1-S, n = 1; Ad26.COV2.S, n = 2)—however, some outcomes have been reported. In a study of pwMS at centers in the UK, for patients who were on DMF, seroconversion rates were greater in those who received the Pfizer/BioNTech BNT162b2 vaccine (100%; n = 14/14) compared with those who received the Oxford/AstraZeneca ChAdOx1-S vaccine (80%; n = 12/15). 48 However, the corresponding rates in people with untreated MS (BNT162b2: 100% [n = 41 out of 41]; ChAdOx1-S: 93% [n = 27 out of 29]) suggest the suboptimal seroconversion rate observed was more likely a consequence of adenoviral vector vaccine type, rather than due to treatment with DMF. 48
Due to the complex nature of cellular immunity, T-cell responses are more challenging to characterize and quantify than antibody responses, 49 resulting in fewer studies and smaller sample sizes in the published literature on COVID-19 vaccine response. A prospective, observational study of 80 pwMS in the USA indicated that those treated with DMF mounted humoral and cell-mediated responses to COVID-19 vaccination (BNT162b2, mRNA-1273, or Ad26.COV2.S) similar to those of untreated MS patients. 20 Post-vaccination, spike-specific CD8+ T cells were significantly increased in the DMF patient cohort. However, these outcomes were based on a small group of patients with DMF (n = 5), and therefore, further data on the T-cell response following vaccination in pwMS receiving DMF would be valuable. 20
Few studies have assessed the responses in pwMS on DMF following booster doses of COVID-19 vaccines, but outcomes reported so far for humoral responses indicate IgG titers and seroconversion rates comparable to those in healthy controls.50,51 In an observational study, all 15 pwMS on DMF who received booster doses of BNT162b2 or Sinovac vaccines were seropositive at least 2 weeks afterward. 50 Median IgG titers in 11 pwMS treated with DMF were comparable to those observed in healthy controls, 21 days after a third dose of BNT162b2. 51 However, a study assessing IFN-γ response to severe acute respiratory syndrome-coronavirus-2 spike protein antigens as a marker for the cellular response found that responses were not significantly different in pwMS on DMF following a booster vaccine, and responder rates were similar after two or three doses (68.4% and 71.4%, respectively). 52
Meta-analyses of COVID-19 vaccine response in pwMS found no significant effect of DMF on the serological response or seroconversion rates post-vaccination compared with untreated patients.47,53 Based on the reported data, there is considerable evidence that the humoral response to COVID-19 mRNA vaccines is preserved in pwMS treated with fumarates; however, data are predominantly for patients receiving DMF rather than DRF. Further understanding of specific aspects would also be of significant benefit, including the effects of fumarates on the overall response to recombinant vector vaccines and on the cellular response to COVID-19 vaccines, as well as their impact on the overall clinical protection conferred by vaccines, including the risks of severe disease.
Safety of vaccination in patients with MS treated with fumarates
Most vaccine types do not present safety concerns for pwMS receiving treatment with DMTs. However, the reactivation of MS following vaccination remains a concern among pwMS. A 2021 review found little evidence to support vaccination triggering autoimmune responses in pwMS, with the exception of yellow fever (live attenuated) vaccine. 54 However, two retrospective cohort studies, including 128 pwMS (all relapsing-remitting MS) and 23 pwMS (20 with relapsing-remitting MS and three with primary progressive MS), respectively, indicated that yellow fever vaccine was not associated with worsening MS.55,56 Across 178 pwMS who had predominantly received either the inactivated COVID-19 Sinovac-Coronavac vaccine or the Pfizer/BioNTech BNT162b2 mRNA vaccine, no significant change in relapse rate was observed in the 8 weeks post-vaccination compared with the 8 weeks prior to vaccination. 57 A further study of pwMS who received the BNT162b2 vaccine found no increase in disease activity and rates of relapse consistent with those in non-vaccinated patients. 58
As described earlier, sNfL levels, when assessed as a marker for disease activity in 20 pwMS on DMF who received the seasonal influenza vaccine, did not change significantly in the 4 weeks post-vaccination compared with baseline, and showed no significant difference from levels observed in healthy controls. 42 In addition, in the 4 weeks following vaccination, there were no relapses, neurological deteriorations, or gadolinium-enhancing lesions, while 80% (n = 16 out of 20) of patients showed no new/newly enlarging lesions compared with the most recent magnetic resonance imaging prior to vaccination. 42 Together, these outcomes indicate that in pwMS treated with DMF, there was no exacerbation of clinical or subclinical disease activity post-vaccination. 42
In addition to concerns about vaccine-induced relapses, general tolerability may also be of concern for those who are considering vaccination. In pwMS who received tetanus–diphtheria toxoid, pneumococcal 23-polyvalent vaccine, and meningococcal oligosaccharide CRM197 conjugate vaccines, vaccination-emergent adverse events occurred in 42% of patients on DMF and 55% of patients on IFN; most were mild or moderate. 43 Adverse event profiles of the recently approved COVID-19 vaccinations in pwMS appear to be generally consistent with safety profiles observed in the general population.10,57 In an observational study of 719 pwMS who received a COVID-19 vaccine (BNT162b2, mRNA-1273, ChAdOx1-S vaccine, or Ad26.COV2.S), 64% and 74% of the study population experienced reactions 24 h after the first and second shots, respectively, including pain at the injection site, fatigue, and headache. 10 The same three adverse events were found to be among the most common in 11 pwMS on DMF or DRF who received the mRNA-1273 vaccine in a prospective observational study of 45 pwMS, consistent with the events observed in those receiving natalizumab, ocrelizumab, or IFN beta. 44 Multivariate regression suggested that people receiving fumarates may have a lower risk of reactions after a second vaccine shot compared with those not on DMT. 10
Summary
There is substantial evidence accumulating that pwMS treated with fumarates will mount adequate humoral responses to vaccinations, similar to healthy controls and pwMS treated with IFNs.42,43 Furthermore, smaller studies have shown that spike-specific CD4+ and CD8+ T-cell responses remain intact in pwMS treated with DMF. 20 In pwMS receiving fumarates, reactivation of disease activity has not been observed following vaccination. 42 Most vaccines have been shown to be safe in MS, perhaps with the exception of the yellow fever vaccine, which might contribute to disease activity. 54 Since vaccine hesitancy is common among pwMS, this presents an opportunity for improving patient education. 9
However, some data gaps remain to be addressed. Compared with the Pfizer/BioNTech BNT162b2 and Moderna mRNA-1273 vaccines, data relating to the effects of fumarates on vaccine response are less complete for other vaccines. Specifically, there are limited data available relating to immunization with live attenuated vaccines in patients receiving fumarates. Further study of the T-cell response following vaccination in people receiving fumarates for MS is required to elucidate how vaccine efficacy could be affected by these agents, especially for those with on-treatment lymphopenia. Finally, data on the overall effectiveness of COVID-19 vaccines in preventing severe disease and hospitalizations in pwMS on fumarates would be of value to prescribers and patients.
Clinicians should use their medical judgment and assess recommendations for vaccination on an individual basis for pwMS. The decision of whether or not to vaccinate should be determined based on the risks of infection and the risks of vaccination, as well as any relevant lifestyle factors that may influence a patient's exposure to a pathogen. 54 For non-live vaccines such as those against COVID-19, which significantly reduce the likelihood of severe infection and hospitalization, based on the currently available evidence in pwMS we recommend that no interruption or delay in treatment with fumarates is needed.
Footnotes
Acknowledgements
Medical writing support, based on input from authors, was provided by David Pertab, PhD, Excel Scientific Solutions (Glasgow, UK), and funded by Biogen.
Author contributions
The authors had full editorial control of the paper and provided their final approval of all content.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MAT received research funding support from Biogen; consulting fees for medical advisory boards from Alexion, Biogen, Genentech, and TG Therapeutics; and speaker fees from Genentech. SV received lecturing fees, travel grants, and research support from Biogen, BMS-Celgene, Janssen, Merck, Novartis, Roche, Sandoz, Sanofi-Genzyme, and Teva. MS and AG employees of and held stock/stock options in Biogen at the time of this work. IB and SL are employees of and hold stock/stock options in Biogen. PW received funding for travel and honoraria (for lectures and advisory boards) from Biogen, Celgene/BMS, Janssen-Cilag, Merck, Novartis, Roche, Sandoz, Sanofi-Genzyme, and Teva.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Biogen.