
Abstract
Background
Recent data suggest that lymphopenia is more prevalent than reported in relapsing–remitting multiple sclerosis (RRMS) patients taking dimethyl fumarate (DMF).
Objective
The objective of this study was to investigate the effect of DMF on lymphocyte subtypes in RRMS patients with and without lymphopenia.
Method
A retrospective study compared lymphocyte subtypes in DMF-treated RRMS patients with low (G1, n = 35) and normal lymphocyte counts (G2, n = 24).
Results
Fifty-nine patients were identified, with mean age 49, 71.2% females, and average DMF duration 20 months. Age, sex, baseline white blood count, disease and treatment durations were similar between groups. Prior interferon therapy and baseline lower normal lymphocyte counts were more frequent in G1. Mean lymphocyte counts were 0.8 ± 0.2 × 109/L in G1 and 1.6 ± 0.3 × 109/L in G2. CD3+, CD4+, and CD8+ T cell mean counts were lower (p < 0.0001), while CD4/CD8 ratio higher (p = 0.03) in G1 than G2. Mean CD19 + B cell counts were normal; however, values were lower in G1 (p = 0.04). After adjusting for confounders, significantly positive correlations were noted between lymphocyte counts and CD3 + , CD4+, CD8+ T, and B cell counts. Negative correlation was observed between lymphocyte counts and CD4/CD8 ratio driven by low CD8+ T cell counts.
Conclusion
DMF treatment predominantly impacts T cells, in particular CD8+ subtype. This finding may have implications in this population’s immunocompetence.
Introduction
Dimethyl fumarate (DMF) was approved for the treatment of relapsing–remitting multiple sclerosis (RRMS) in March 2013 based on its efficacy and safety profile documented in the two pivotal trials, DEFINE and CONFIRM.1,2 Severe lymphopenia, as defined by lymphocyte count less than 0.5 × 109/L was seen in approximately 5% of patients in these studies and was reported not to be associated with any serious or opportunistic infections.1,2
Since then, further studies in patients with MS have reported a larger fraction of patients who have developed severe lymphopenia while on DMF,3–5 in particular older patients and those taking the drug for more than one year. 3 In addition, the recent reported cases of progressive multifocal leukoencephalopathy (PML) and other viral infections in fumarate-treated patients make it imperative to elucidate which patients are at risk.6–13
It is well known that both humoral and cellular immune responses are involved in the defense against viral infections, prompting our interest in investigating the effects of DMF on lymphocyte subtypes in RRMS patients with and without lymphopenia.
Materials and methods
We performed a retrospective chart review of all DMF-treated RRMS patients seen at the Lahey Multiple Sclerosis Clinic from April to July 2015, who had a complete white blood count (WBC) and lymphocyte subtypes done during this time interval. Lymphocyte subtypes were incorporated in to our routine blood work evaluation of MS patients treated with DMF after the first reported case of PML in this population. 6 Lymphocyte subtypes, including CD3+, CD4+, and CD8+ T cells, CD4/CD8 ratio, CD19+ B cells, and natural killer (NK) cells, were evaluated by using flow cytometry.
We compared the lymphocyte subtypes between two groups: group 1 – patients with lymphopenia defined as lymphocytes less than 1.2 × 109/L; group 2 – patients with normal lymphocytes (lymphocytes equal or greater than 1.2 × 109/L). Absolute cell counts were used for subtype analyses, except for NK where percentages were used.
Statistical analysis was performed using the statistical package SAS for Windows version 9.4 TS Level 1M2 (Copyright 2002-2012 by SAS Institute Inc., Cary, NC, USA). Patient’s demographics, time since MS diagnosis, prior immunomodulator treatment, duration of DMF exposure, complete WBC at baseline, as well as white blood and lymphocyte counts with subtype analysis at the time of evaluation were compared between the two groups by using Pearson’s chi-square test for binary and Student’s t-test for continuous outcomes. Raw and partial correlations were used to assess the strength of association between absolute numbers of lymphocyte subtypes and total lymphocyte count. Adjustments were made for age, prior interferon exposure, and duration of treatment.
This study was approved by the Institutional Review Board at Lahey Clinical Medical Center, Burlington, MA.
Results
Sixty-three patients with RRMS receiving DMF were seen in our MS clinic during the study period. From those, 59 patients fulfilled our inclusion criteria and were evaluated. The patient’s mean age was 49 years and 71.2% of them were females. Group 1 (lymphocyte count less than 1.2 × 109/L) had 35 patients and group 2 (normal lymphocyte count) had 24 patients. Patients had an average of 20 months of exposure to DMF. Subtype lymphocyte analysis was available in 58 patients; one patient’s specimen was not evaluated due to technical reasons. This patient was part of group 1, with a lymphocyte count at the time of the evaluation of 0.91 × 109/L.
Demographics, disease characteristics, and baseline white blood count (WBC) with differentials.

White blood count (WBC) and lymphocyte subtypes during DMF treatment.

NS = not significant.
Correlation between absolute lymphocyte and subtype counts.
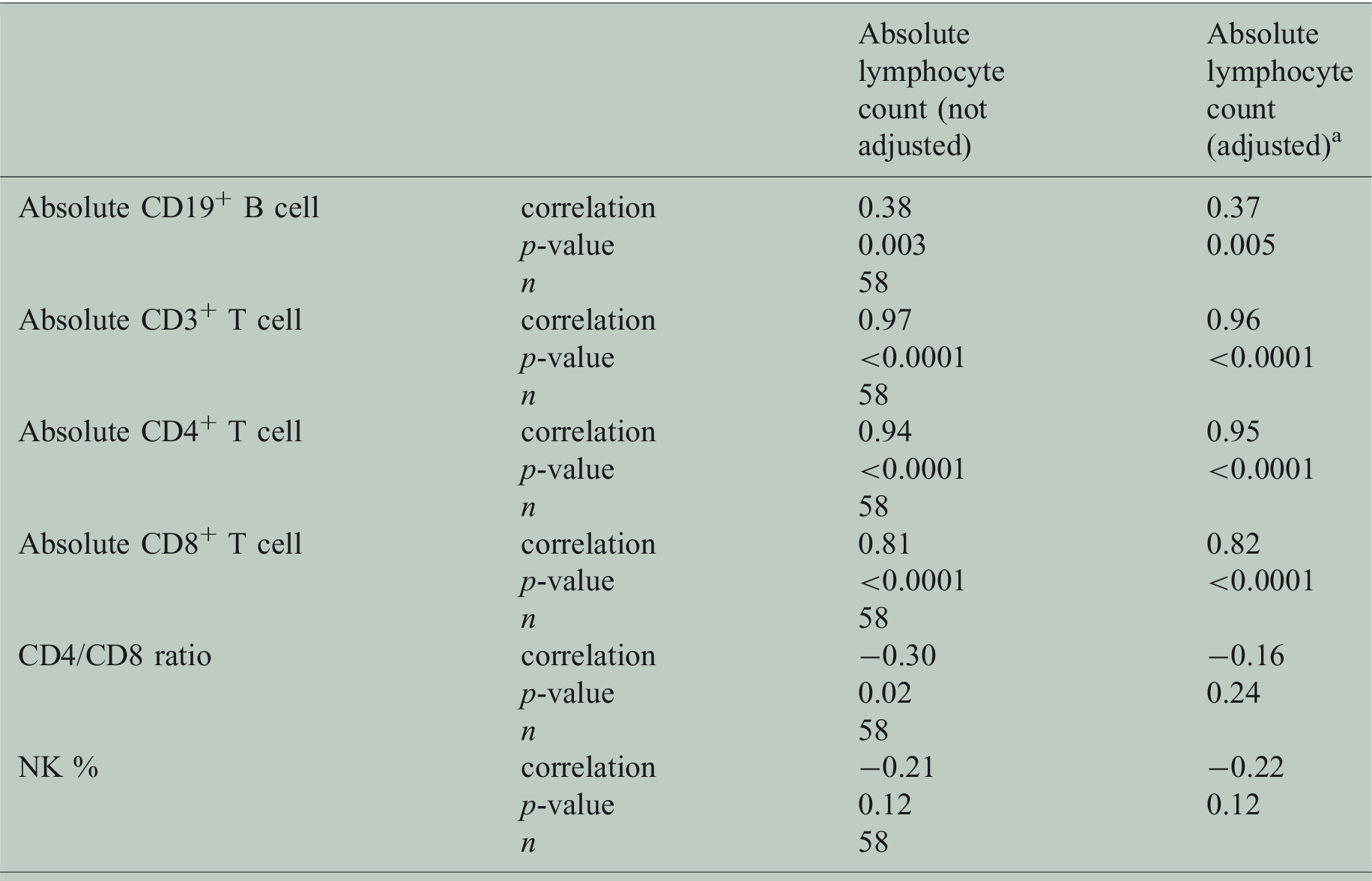
Correlations after adjustment for age, DMF treatment duration, and prior interferon exposure.
Discussion
Decrease in mean white blood cell and lymphocyte counts were documented in both DEFINE and CONFIRM studies mostly during the first year of treatment,1,2 with leucopenia grade 2 or higher (<3.0 × 109/L) and lymphopenia grade 3 or higher (<0.5 × 109/L) occurring in 10% and 5% of the patients, respectively. 2 In a pooled analysis of both studies, the percentage of patients with worst post-baseline grades 1, 2, and 3 lymphopenia were 10%, 22%, and 6%, respectively, without any clear pattern of higher incidence of infections identified in the lymphopenic patients. 14 However, recent reports of infections, such as PML,6–10 disseminated varicella zoster, 11 West Nile encephalitis, 12 and human herpes-virus 8-related Kaposi’s sarcoma, 13 in RRMS and psoriatic patients treated with fumarate or its compounds, with or without severe lymphopenia,6–13 have raised the question of a potentially greater role for lymphocyte subpopulations rather than absolute lymphocyte count as a better indicator of an increased risk for infections.12,15–18
In our study, 59.3% of patients had lymphopenia grade 1 or higher at a mean DMF exposure of 20 months. This incidence is higher than the pooled analysis of the pivotal trials, 14 but similar to the study from Spencer et al., 15 where at month 12 50% of the patients had lymphocyte counts below the lower limit of normal. A possible explanation for our higher incidence is the potential role of older age increasing the risk of lymphopenia in DMF-treated patients; 3 our patients were at least one decade older than the patients from the pivotal trials.1,2 The high incidence of decreased lymphocytes and its subtypes around 20 months after DMF initiation seen in our study supports prior inferences that the percentage of lymphopenia might increase with a longer duration of treatment.4,6
Lower normal baseline lymphocyte count was more frequent in the lymphopenic group, as documented by Longbrake and Cross. 3 However, different from their study, prior exposure to interferon-beta, not to natalizumab, was significantly more common in the lymphopenic patients. Lymphopenia is well known to be associated with use of interferon-beta therapy, but the decrease in number of lymphocytes is usually mild and intermittent.19,20 The significance of the higher risk of lymphopenia in our patients with prior exposure to interferons is unclear, and this finding will require validation in a larger cohort study.
In our population, lymphopenic patients had significantly lower levels of CD3+, CD4+, and CD8+ T cells, as compared to patients with normal lymphocyte levels, even though a more modest decrease in CD8+ T cells was also detected in some patients without lymphopenia. This finding was also demonstrated by the higher positive correlation between absolute lymphocytes and CD3+(r = 0.97) as well as CD4+ (r = 0.94) T cells counts as compared with CD8+ (r = 0.81), supporting the preferential impact on CD8+ T cells by DMF, independent of the total lymphocyte count. Mean CD19+ B cell counts were less involved, and within the normal range in both groups, however, values were in general lower in the group with lymphopenia, with a significant positive correlation with the absolute lymphocyte counts. These findings are consistent with prior studies of DMF in RRMS patients showing a more significant reduction of CD8+ T cells as compared to CD4+ T and CD19+ B cells.12,15–17 No significant differences were seen in the percentage of NK in both groups, supporting the lack of effect of DMF on this subpopulation of lymphocytes, as described by others. 15
Our study demonstrates a distinct effect of DMF treatment on T cells, particularly decreasing CD8+ T cells more dramatically in patients with lymphopenia, raising the concern of its potential impact in cell-mediated antiviral immunity and central nervous system immune surveillance. Further research to determine the mechanisms of DMF-induced lymphopenia and its potential long-term consequences are needed.
Footnotes
Conflicts of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.