
Abstract
Background
Fatigue and pain are prevalent symptoms of multiple sclerosis (MS) and frequent complaint in MS patients, which reduce their quality of life. This study aimed to assess the effect of massage therapy on pain and fatigue in MS Patients.
Method
The original and Persian databases were searched included PubMed, web of science, embase, ovid, scopus, and the Cochrane Library, SID, and Iranedex from inception to November 2020. Studies that reported the effect of massage on fatigue and pain were included. Two investigators extracted all relevant data, independently. For deriving analysis, mean difference (MD) and standardized mean difference (SMD) were used.
Result
Ten studies were eligible acoording criteria. The effect of massage on fatigue showed significant improvement (−1.62; 95% CL −2.40, −0.83; p < .00001), also results of the systematic review showed a significant reduction in pain severity.
Conclusion
Massage as a complementary and non-pharmacological therapy might have been associated with alleviating fatigue and pain in M.S. patients. Based on the current study, massage intervention for MS patients could have possible clinical value for palliating pain and fatigue and improving quality of life; however, this matter needs further and more significant trial studies.
Introduction
Multiple sclerosis (MS), as a chronic, inflammatory, immune-mediated disease of the central nervous system, sickening over two million people worldwide. 1 MS, as a complex disease with a wide diversity of symptoms, 2 can disturb patients’ daily living activities. 3 Two of these disruptive symptoms are Fatigue and Pain. 4 Fatigue is considered among the most frequent causes of disability and decreased quality of life in MS patients. 3 About 67%–95% of MS patients suffer from fatigue, and 50%–60% of MS patients experience it as the worst symptom, and 4%–15% consider it the most incapacitating symptom. Alongside fatigue, pain is another irritating symptom that causes problems for MS patients. 4 Pain is another significant and common symptom in many patients with MS. 5 There are different forms of pain; some types of them directly related to MS itself, other types of pain may be produced by MS effects on the body. So, MS patients can experience pain that unrelated to their disease. 6 Pain is a multi-factorial symptom. 7 Thus, the distinction of MS-related pain from pain with other origins is hard. 5
The presence of pain in MS patients can associate with higher levels of dysfunction, depression, and fatigue. 6 So, pain or fatigue may impact the quality of life and daily activities.1,8 fatigue and pain make people with MS less mobile and interact with their everyday tasks; these conditions cause more difficulty and lower the quality of life (QOL) among MS patients. 9 As pain and fatigue increase in MS patients, QOL decreases.9–11 On one hand, there is no cure for MS and proper treatment for MS patients’ pain or fatigue. 4 On the other hand, MS patients are expected to live a nearly complete lifespan with this chronic condition, so it’s needed interventions to relieve these symptoms without complications and try to improve QOL in people with MS. 12 In addition, most of the MS patients and their caregivers are concerned about the risk of narcotic addiction, which can be a result of pain management. 6
Since medication administration is accompanied by adverse effects, and the conventional therapies do not help manage some MS symptoms, the use of non-pharmacological methods for treating these two symptoms seems sensible.1,8,13,14 As a result, the number of MS patients who are switching to or use alternative and complementary treatment is increasing. 3 Complementary therapies can shorten the disease's duration, suppress it, reduce the number of aggression, or delay the attacks. 3 One of the most common and important types of Complementary & alternative medicine (CAM) is MT.15–17 A third of MS patients report applying massage therapy (MT) as an adjunct to their medical treatment.13,14 Furthermore, the medications for managing pain and fatigue are expensive, and MT may provide an accessible and quite cheaper option for relieving these symptoms. 4 Other studies showed MT could improve MS patients’ QOL4,14,18–21 and decrease pain and fatigue in other patients with different diagnoses.22–28
However, MT is one of the most frequently used complementary and alternative treatment methods by MS patients. 29 But the evidence on the efficacy of MT in MS patients is insufficient.1,30,31 there is little empirical evidence that supports symptom management for MS patients by MT. 4 In the literature review, we found few Randomized clinical trials(RCT) in this area. During treatment, massage therapists manually touch and apply pressure to the patient's body. 32
At the beginning of the 19th century, the Swedish physician Pehr Henrik Ling developed Classical massage 33 which consists of the techniques as follows: Petrissage, friction, vibration and tapotement.33,34 Other types of MT have been described as follows; Friction massage or deep, transverse massage and Tui na, 34 Thai massage, Traditional Chinese medicine massage, Swedish massage and etc. 35 Nowadays, a wide range of various massage techniques and styles arising from all around the world are common. 34 This widespread use of MT might be due to complex reasons, but the concept of MT being safe plays an important role. 34 Additionally, the massage therapist uses different methods, such as the creation of friction, pressing, rubbing, grabbing, and kneading 35 and use MT techniques based on their experience and the desired clinical advantag. Weerapong’s study stated that, the most common form of massage is the Swedish massage or Classic Western massage, and the combination of Western techniques in the majority of research has been used to assess the effects of MT. 36 So, there are no systematic reviews about the effectiveness of MT in relieving pain and fatigue in MS patients. Therefore, the present study was conducted to investigate the efficacy of MT in alleviating fatigue and pain among MS patients.
Methods
Search strategy
The initial search was conducted from inception to 1 November 2020 to find relevant studies in databases, including Web of Science, PubMed, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), Ovid, Scopus, and the Global Index Medicus. We also searched Iranian databases such as Magiran, SID, Iranmedex for finding relevant Persian articles. We used the following terms for searching in English language databases: “Massage OR Non-pharmacological OR Complementary medicine” AND “Multiple sclerosis OR MS” AND “Fatigue OR Pain”. Equivalent Persian group terms were searched in Persian language databases. We only included articles that were published in English and Persian languages. We also carried out searches in key journals, reference lists of related studies, Google Scholar, and conference abstracts after a preliminary investigation of databases as grey literature resources to avoid missing valuable data.
Eligibility criteria
randomized controlled trials (RCTs), comparative studies and quasi-experimental studies on MT and its effects on pain and fatigue were included in the present study. Massage was defined as the manipulation of the soft tissues of the body by hand to affect the muscular, vascular, and nervous systems. No restrictions were put on the conceptual bases or cultural practices of massage. The massage might have been applied by nurses, therapists, or other healthcare professionals. Only publications with control groups were included. Control groups might have received placebos or other standard treatments. Reports that assessed fatigue and pain with standardized and efficient instruments during and after intervention were included. Inclusion criteria include MS patients 18 years old or older who had been diagnosed according to standard diagnostic criteria, a cut-off score based on validated questionnaires, diagnoses made by physicians, or by other valid criteria in all stages of the disease. Also, Studies were included that employed massage as an intervention. Exclusion criteria include Observational studies, diagnostic studies, prognostic studies or about theoretical frameworks, Studies that were applied different intervention in addition to MT, a second publication of the same study, studies were unpublished or non‐peer-reviewed, and full‐text was not available in English.
Data collection
According to the selection criteria, the results of the search were screened for relevant titles and abstracts. The relevant abstracts were chosen for full-text review. After that, data extraction was done individually by the two authors mentioned above. Also, references of relevant articles were screened for relevance. Duplicates were removed. Then, for extracting the following information from included studies, a standardized data collection form was used: first author, study design, year of publication, sample size, and characteristics of included participants.
Quality assessment
To assess the quality of the studies, two reviewers (MH and KF) separately assessed each study using the Cochrane Collaboration tool for RCTs and quasi-experimental studies. The Cochrane Collaboration tool assesses the following seven domains: sequence generation, allocation concealment, blinding of the participants and personnel, blinding of the assessors, incomplete outcome data, selective reporting, and other biases. Each domain was rated as being of a low risk of bias, a high risk of bias, or an unclear risk of bias. Since the information that permits a definitive rating of high risk or low risk is often unavailable, a designation of “probably yes” and “probably no” was proposed to make more specific declarations on the separately risk of bias possible. Domains rated as “unclear” were designated as “probably high risk” or “probably low risk” to make it easier to understand the quality of the added studies. 37
Statistical analysis
Statistical analyses were conducted using Cochrane Collaboration’s Review Manager Software (Review Manager 5.3). For dichotomous outcomes, relative risks (RR) were reported with 95% confidence intervals (CI). For continuous outcomes, the data were pooled using the mean difference (MD) with a 95% CI if different rating scales were used in different trials for the same outcome. The heterogeneity among studies was evaluated using Cochrane's Q statistic, which used a more liberal p-value cut-off of 0.10 to indicate statistical heterogeneity. The data were synthesized using random-effects models, considering the potential for heterogeneity among the included studies. 38
Results
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines for conducting this systematic review and meta-analysis. The study concluded with 866 citations, of which 304 were duplicates, and 269 were excluded for reasons of inappropriacy. Then 35 potentially eligible articles were investigated for further assessment. Among the 35 articles, 10 studies on the application of MT for multiple sclerosis in adults were included, while the remaining articles were excluded (Figure 1). Overall, six Studies were included in quantitative synthesis (meta-analysis).

Screening flowchart and selection of qualified articles according to PRISMA guidelines.
Characteristics of the included studies
Table 1 shows the characteristics of the ten included studies.4,6,8,39–45Among them were three RCTs and six quasi-experimental studies. Six of the studies had been done in Iran, 2 in the United States and the United Kingdom, 1 in Turkey, and 1 in Ireland. The sample size ranged from 17 to 75, with a sum of 421 patients. All studies mentioned more female than male patients. Among the ten studies, no articles reported dropouts. The criteria used to diagnose MS varied among the studies. In 7 studies, massage was compared with usual care, in 2 studies, with relaxation therapy, and in 1 study, with another type of massage. In 7 studies, MT was compared with usual care, in 2 studies, with relaxation therapy, and one study, with another type of massage.
Characteristic of included study.

According to the included studies, the duration of the MT intervention ranged from 5 to 20 min, with 25 min being the most common. The number of treatment sessions ranged from 1 to 8. The frequency ranged from once a day to once per week, with the most frequent being twice per day. Two studies applied Slow Stroke Back Massage (SSBM) for alleviating pain and fatigue,42,44 two studies performed sham reflexology,39,40 one study applied Swedish MT and exercise therapy, 41 and other studies used the protocol of their medical center to perform massage. In all included studies, the massage was performed by the researcher and the executive team that was a nurse and licensed physical therapists and licensed massage therapists.
Outcome measures
Outcome measures varied among the included studies. The most frequently used outcome measure was fatigue (6 studies). All of the studies used the Fatigue Severity Scale (FSS) for fatigue assessment. The other outcome was pain, for the assessment of pain, three studies used the Visual Analogue Scale (VAS), one study used the Pain Effects Scale (PES), (PES) and one study used the Numeric Rating Scale (NRS).
Effect of MT on fatigue and pain
Out of the 10 studies, six were entered into the meta-analysis. All of the included studies measured the total fatigue score using FSS. The standardized mean difference (SMD) and the random-effect model were used because the studies were heterogeneous (P < 0.00001, I2= 86.1%). The results demonstrated that the effect of MT on fatigue in MS patients was statistically significant (SMD = -1.62, 95% CI -2.40, -0.83], P = 0.0001) (Figure 2). Four of the studies were included in the systematic review. One study investigated both pain and fatigue. 4 Three studies showed that there was a significant improvement in the severity of pain (p < 0.05).6,39,41 Backus et al. showed that there was a significant improvement in pain (p < .01) and there was a significant correlation between the mean change in the scores on the Pain and the use of the intervention (r = 0.532, p < .01). 4 Negahban also showed that MT resulted in a significantly greater pain reduction (p = 0.001). 41 However, two of the studies found no significant differences among the mean pain intensity scores among the groups.6,40,41 No studies reported adverse events.

Forest plot of the effect of massage on fatigue. The 95% confidence interval for each study is shown in the form of horizontal lines around the central mean and midpoint of the dotted line represents the mean of the overall score and the lozenge shape shows the confidence interval of the estimate of this disorder.
Publication bias
In the present study, publication bias was examined at three levels. A funnel plot was used as the first level. The second level included the Begg and Egger tests, and finally, the third level used the trim and fill method. According to the funnel plot, the accumulation of studies showed that there was a significant publication bias in the studies. However, the results were not significant in the Begg test (p = 0.26). Due to the different results obtained from these two tests, the trim and fill test was also performed. In the trim and fill test, a study was added to the included studies (SMD = 1.195, (CI = 0.278-2.113) versus SMD = 1.607, (CI = 0.815-2.398)). Therefore, publication bias was significant in the present study (Figure 3).
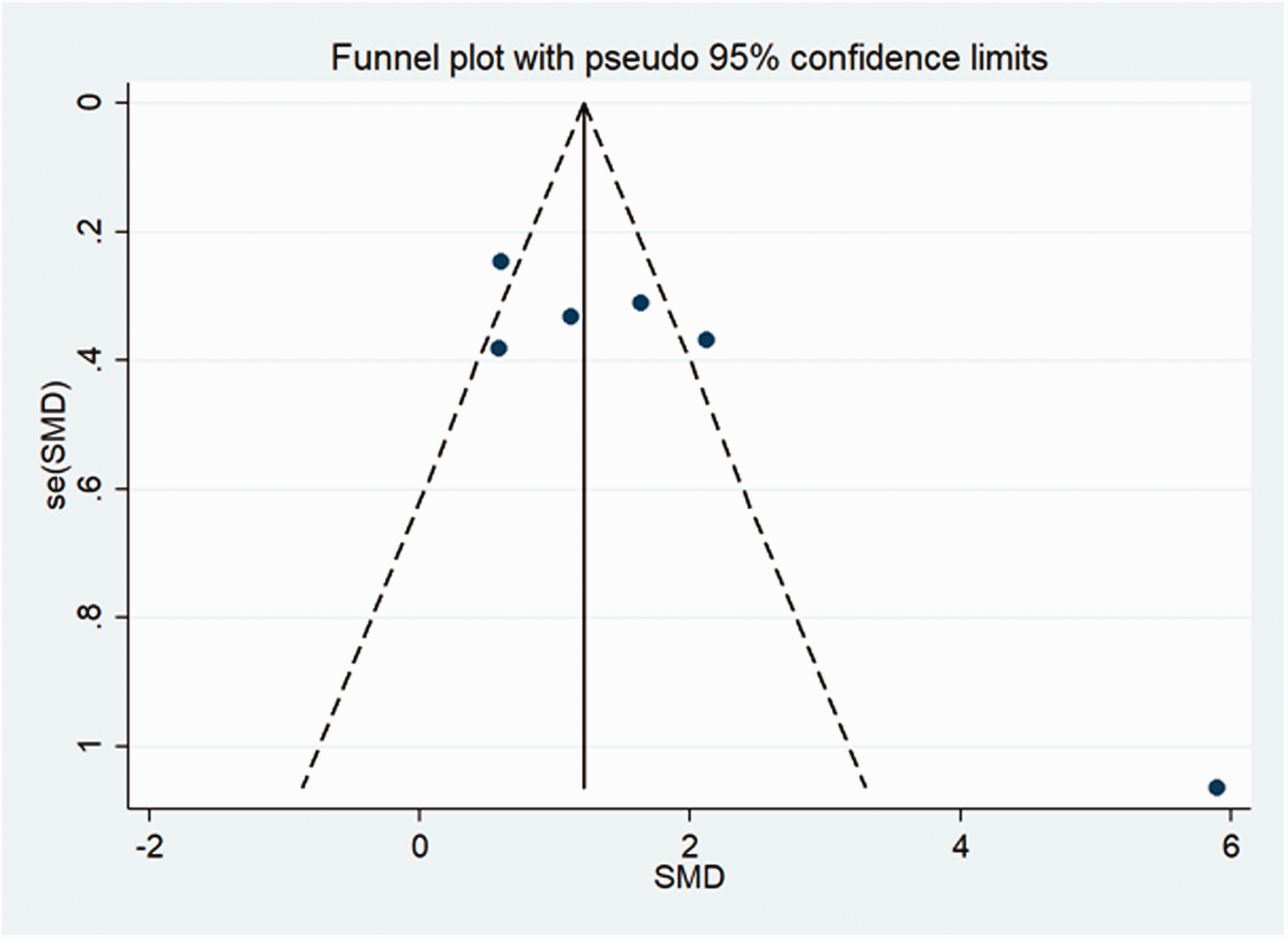
Funnel plot of publication bias among studies.
Discussion
This study was the first systematic review and meta-analysis to evaluate the effectiveness of MT on fatigue and pain in MS patients. The results revealed that fatigue and pain may be decreased in MS patients by MT. In comparison with the control group, MT was more useful in reducing fatigue and pain in MS patients. The present study also demonstrated that reflexology as a type of MT beneficially alleviated the severity of MS patients' pain.
Although reflexology is not an effective intervention for any medical condition, 46 The findings of Other interventional studies confirmed reflexology is safe and without adverse effects 47 and can relieve MS symptoms such as pain6,39,43 and fatigue. 40 Reflexology may affect the release of endogenous opiates that cause in the reduction of pain 47 and decrease of fatigue. Because Fatigue, reduced QOL, depression, and anxiety are strongly correlated with the presence of pain. 7
Other reviews confirmed this finding that MT may relieve pain and fatigue in MS patients. Amatya et al. conducted a review on non‐pharmacological treatments for reducing chronic pain in MS and suggested that MT was effectively relieved chronic pain. Meanwhile, Amatya indicated that MT was significantly effective in soothing fatigue and pain. 48 Also, The Arab’s study showed MT could reduce fatigue in MS patients. 1
MT, in contrast to exercise which, causes a stressful physiological condition (such as increased pulse rate and blood pressure), improves blood flow in completely relaxing conditions; it, also increases the intake of nutrients and oxygen and removes more cellular waste. 49 Massage is effective even on paralyzed and inactive muscles. This technique makes the muscles sensitive to nerve waves and, as a result causes them to react faster and move more efficiently. Massage is one of the most practical and valuable treatments for physical fatigue. 50 Therefore; it, can be said that MT directly affects muscle fatigue. 3
Our results reveal that pain and fatigue were both crucially lessened in MS after MT. The primary fatigue origin in MS is not fully understood and is unclear, 51 and each person's experience of fatigue is different and variable throughout the disease. In other words, fatigue is affected by the influence of pro-inflammatory cytokines, central nervous system lesion load, cortical atrophy, abnormal patterns of cerebral activation, poor endocrine influences, and axonal injury that make it difficult to recognize their mechanisms. 52 Besides, muscle fatigue has been observed in MS patients 25 and may contribute to the overall fatigue reported by individuals with MS. Thus, this lack of clarity related to fatigue in MS makes it hard to understand the potential mechanisms by which MT may have a positive impact on fatigue.53–55 MT has also been shown to be effective for decreae the severity of neuropathic pain in some people with spinal cord injury.39,41 Some studies have reported that light to moderate MT intensity leads to a decrease in the sensitivity of spinal nociceptive reflexes, which is often elevated in chronic pain syndromes. 56 Although potential mechanisms for the changes seen in MS patients were not explored in the present study, MT may also be effective in lowering pain in people with MS. 6
Huntley et al. conducted a review about complementary and alternative treatment for relieving the chronic symptoms of multiple sclerosis and mentioned that MT could be effectively reduce fatigue and pain severity, but no favorable effects were found in the meta-analysis of the same studies. 57 The present study is different from other meta-analyses because it assessed studies involving different instruments for evaluating variables.
Ernst, et al. performed a systematic review to consider the effect of MT in patients with different medical conditions. Three of the studies suggested that reflexology had significant effects on pain alleviation in MS Patients. Other studies mentioned that MT is effectively reducedpain relief in diabetes, premenstrual syndrome, cancer, and multiple sclerosis.35,46,58 Besides, Baykal et al. conducted a review to assess the efficacy of abdominal massage on the constipation management in patients with neurologic disorders. It has been declared that abdominal massage for an average of 15 minutes per day for the duration of 3 to 6 weeks in patients suffering from neurological conditions such as MS reduces pain and digestive problems. 58
The present systematic review has some limitations; First, only quasi-experimental studies were included in the meta-analysis with possible selection bias and could not perform further analysis on the pain variable. Second, discrepancies across studies were observed probably due to methodological issues. Third, there was significant heterogeneity in studies, with varying durations and frequencies for MT, and most importantly varying primary outcome measures. Finally, another limitation is that the analyses did not combine different measurement time points. The results might have been different if the analysis was restricted to a particular duration of time after treatment. In summary, a systematic review and meta-analysis were performed to evaluate the effects of MT in MS patients suffering from fatigue and pain. It was found out that MT intervention has a significant impact on fatigue and pain shortly after applying of the intervention. However, since long-term studies about the effectiveness of MT are not available, the number of studies included in the analysis was small. well-designed studies with longer follow-up periods are needed to be able to draw firm conclusions about the effectiveness of MT in pain and fatigue relief in MS patients.
Conclusion
As a complementary and non-pharmacological therapy, Massage may be associated with the alleviation of fatigue and pain in MS patients. Due to the small number of available studies and potential methodological issues, the long-term and objective effects of massage therapy are still not fully explored. Based on the current study, massage intervention for MS patients could have possible clinical value for palliating pain and fatigue and improving quality of life, however it need further and more significant trial studies.
Supplemental Material
sj-pdf-1-mso-10.1177_20552173211022779 - Supplemental material for Effectiveness of massage therapy on fatigue and pain in patients with multiple sclerosis: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-mso-10.1177_20552173211022779 for Effectiveness of massage therapy on fatigue and pain in patients with multiple sclerosis: A systematic review and meta-analysis by Shahin Salarvand, Mohammad Eghbal Heidari, Kazem Farahi, Erfan Teymuri, Mohammad Almasian and Saeid Bitaraf in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Authors’ contributions
All of authors cooperated in different stages of study. MA: revised it critically for important intellectual content and translated to the English language. The authors read and approved the final manuscript.
Acknowledgement
We are grateful to all of authors for cooperating with us.
Availability of data and materials
All datasets analyzed during this study are available from the corresponding author on reasonable request
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.