
Abstract
Introduction
Cognitive rehabilitation includes a set of programs to train the brain, which leads to the improvement of mental and neuro-psychological functions. This meta-analysis was conducted with the aim of investigating the effectiveness of cognitive rehabilitation in comparison with routine rehabilitation methods in patients with multiple sclerosis (MS).
Methods
The Cochrane Library, ProQuest, PubMed, PsycINFO, and Web of Science databases were searched from inception to August 2022. Google Scholar was used to find relevant sources and complete the search coverage. Two authors independently selected studies based on predefined inclusion criteria. Data analysis was performed using RevMan (version 5.3).
Results
Out of the 578 studies found, 20 studies were finally included in this review. The results of the meta-analysis on four outcomes (Paced Auditory Serial Addition Test (PASAT), Brief Visuospatial Memory Test (BVMT), MS Neuropsychological Screening Questionnaire (MSNQ), and Beck Depression Inventory (BDI)) indicated that the outcome was significant in favor of the cognitive rehabilitation group. However, for five outcomes (Controlled Oral Word Association Test (COWAT), California Verbal Learning Test (CVLT), Everyday Memory Questionnaire (EMQ), Symbol Digit Modalities Test (SDMT), and Expanded Disability Status Scale (EDSS)), the differences between the two groups were not significant.
Conclusion
The results of this meta-analysis showed that cognitive rehabilitation has an effect on improving the performance of patients with MS. However, further studies with more accurate methodologies are required to determine which of the outcomes cognitive rehabilitation has a greater effect on.
Introduction
Multiple sclerosis (MS) is a chronic, immune-mediated, demyelinating disorder of the central nervous system (CNS). MS can cause a wide range of potential symptoms, including problems with vision, arm or leg movement, sensation or balance. Although the course is highly variable, many people develop irreversible disability and MS remains a major cause of neurological disability in young adults. 1
Cognitive rehabilitation includes a set of programs to train the brain, which leads to the improvement of a person's mental and neuro-psychological functions. As a result, personal progress is made in areas such as education, job and social relations. 2 Cognitive impairment is a common clinical feature of MS in the early and later stages of the disease,3,4 and its prevalence is between 43 and 70%.5,6 Studies have shown that MS negatively affects various aspects of cognitive function, including aspects related to attention, information processing efficiency, executive function, processing speed, new learning, and memory. 7 Cognitive dysfunction is closely related to functional status in MS. Rao et al. 6 found that people with MS who were cognitively impaired participated less in social and professional activities, were less employed, had more problems in doing routine household chores, and they were more vulnerable to mental illnesses than people with physical disabilities. Functional impairments also include difficulties with independent shopping, completing household chores, cooking, driving and using public transportation. 8 Such changes in the personal, professional and social lives of patients have a detrimental effect on their quality of life (QoL). For this reason, the development of therapeutic measures to alleviate such deficits should be a priority in MS research. 9
The aim of cognitive rehabilitation is to reduce cognitive deficits and improve patients’ awareness, the ability to consider their cognitive deficits in daily life activities and promote neurobiological changes. Historically, most of the interventions implemented for MS patients involved learning and memory-based interventions, but more recently, the focus has shifted to other domains such as executive function and attention, as these cognitive functions have the greatest impact. 9
Many interventional studies have evaluated the effectiveness of cognitive rehabilitation treatments in relation to cognitive deficits in MS, but the number of systematic review studies and meta-analysis were few in this field. Therefore, this meta-analysis was conducted with the aim of investigating the effectiveness of cognitive rehabilitation in comparison with routine rehabilitation methods in patients with MS.
Methods
This systematic review and meta-analysis studies are reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 10
Search strategy
This review considered all relevant literature published in English from inception to August 2022. The following five databases were searched: Cochrane Library; ProQuest; PubMed; PsycINFO; and Web of Science. Google Scholar was used to find relevant sources and complete the search coverage. Two independent reviewers conducted the search based on the search strategy. This strategy was adapted for the different databases as required. Search terms related to “cognitive rehabilitation” and “multiple sclerosis” were entered into the title, abstract and keyword fields. The studies obtained from the electronic search and manual search were organized using EndNote software.
Study selection
Articles obtained from all databases were searched and entered into EndNote 20, and duplicates were removed. Two authors independently selected studies based on predefined inclusion criteria. Titles and abstracts were reviewed first, and irrelevant studies were excluded. Then, the authors screened the full text. Any disagreements were resolved by discussion among the two authors with the possibility to involve a third author as a consultant to make a final decision.
Eligibility criteria
All studies published in English that evaluated cognitive rehabilitation in patients with MS were included. Moreover, the excluded articles met the following criteria: 1. The study was not an intervention. 2. The minimum follow-up time was 2 weeks. 3. The study was not an empirical study. 4. The intervention was not targeting a cognitive domain. 5. The article was not in English. 6. The article included populations other than those with MS.
Data extraction and quality assessment
Data were extracted via Microsoft Forms into an Excel spreadsheet. The two reviewers used the same data extraction sheet to report the following aspects: study information (title, publication year and first author), country of the study population, study design, number of participants, patient demographics, follow-up period and main findings.
Study quality was assessed by two independent reviewers. The quality assessment of included studies was performed using the Cochrane quality assessment tool and RevMan 5.3 software. In this tool, five important types of bias (selection bias, performance bias, detection bias, attrition bias and reporting bias) that are likely to occur in clinical trial studies were investigated.
Statistical analysis
The Cochrane Collaboration's Review Manager Program (RevMan version 5.3, Cochrane collaboration) was used for data analysis. Mean differences (MDs) and corresponding 95% confidence intervals (CIs) were estimated by a fixed-effect meta-analysis. A random-effect meta-analysis was used if heterogeneity is more than 50%. The chi-square test for Q and the I2 quantity were used to test heterogeneity between studies. Significant results were considered if the P-value for the chi-square test was ≤0.1 and I2 ≥ 50%. 10
Results
Study selection and study characteristics
The PRISMA flowchart shows the identification, screening, eligibility and inclusion phases of the literature search (Figure 1). The search returned 643 studies. After removing duplicates, 578 studies remained. After screening of titles and abstracts, the full text of 89 studies was assessed for eligibility.

Flow diagram for the selection of studies for the systematic review and meta-analysis (PRISMA diagram).
In the 20 studies included in the meta-analysis, the number of participants ranged from 10 to 93, the follow-up times of the results ranged from 2 weeks to 1 year, and the average age of the participants ranged from 30 to 55 years. These studies were conducted between 2007 and 2020. Of these 20 studies, 4 studies were published in the United States, 7 studies in Italy, 3 studies in the United Kingdom, 2 studies in Germany, 1 study in Finland, 1 study in Switzerland, 1 study in Greece, and 1 study in Iran. Table 1 shows the main characteristics, and Table 2 shows the outcomes and main results of the 20 included studies.
Main characteristics of included studies.

Outcomes and main results of included studies.

QoL: quality of life.
Risk of bias assessment
The results of the evaluation of the quality of the studies showed that, in general, all 20 included studies have an acceptable quality (Figure 2).

Risk of bias summary of studies included: low risk of bias, high risk of bias, and unclear risk).
Meta-analyses
Performance outcomes (cognitive function)
Auditory processing speed and flexibility
Paced Auditory Serial Addition Test (PASAT). This test is typically used to assess information processing and sustained and divided attention. In this task, subjects are presented with a number every 2, 3 or 4 s and they are asked to add the number they have heard now with the number they have heard before and say it out loud. Studies have shown that in addition to being challenging, this task is also stressful.
Primary data related to the outcome of PASAT were reported in 13 studies.11–16,18–20,24–27 The results of the meta-analysis of these studies with a sample size of 333 patients in the cognitive rehabilitation group and 300 patients in the control group indicated that the outcome was significantly in favor of the cognitive rehabilitation group (MD = 3.74, 95% CI: 2.02 to 5.47, P < 0.0001). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 0%, P = 0.72) (Figure 3).
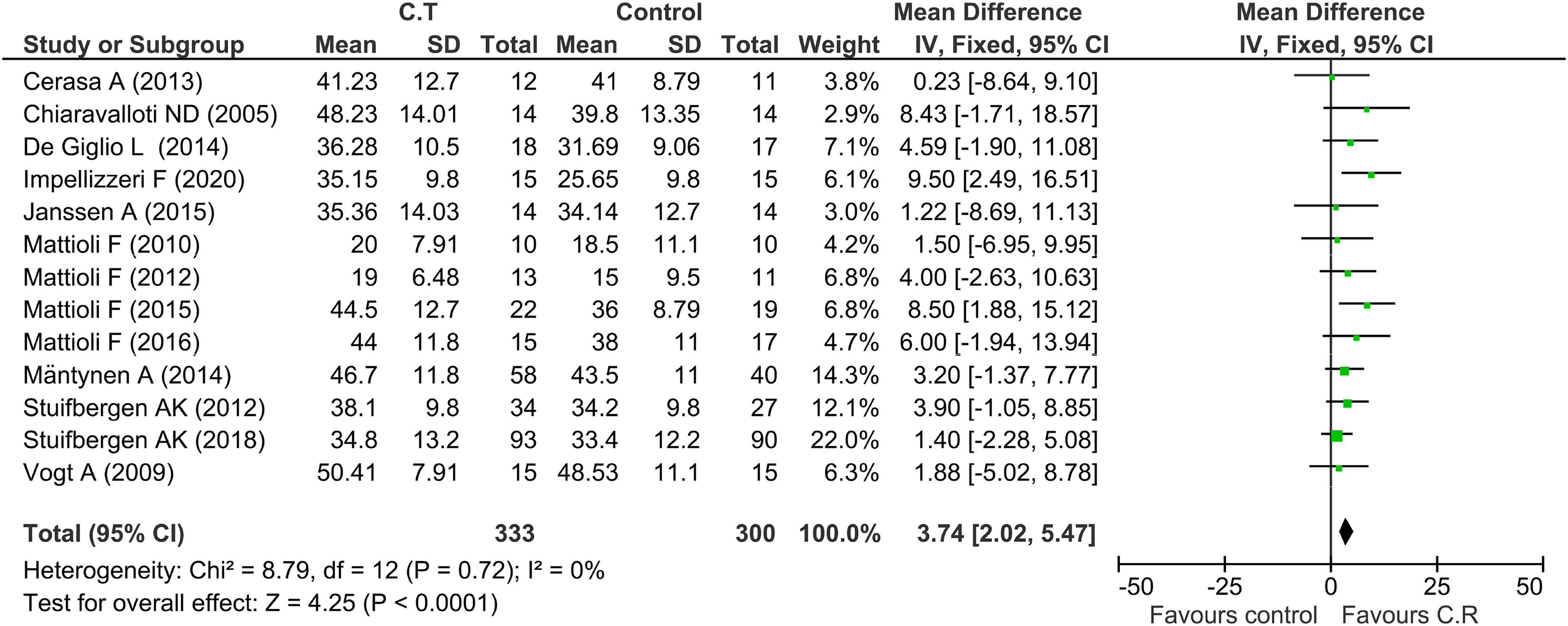
Forest plot analysis of the PASAT.
Nonverbal learning and memory
Brief Visuospatial Memory Test (BVMT). The researchers used the BVMT, in which patients were asked to represent six abstract shapes in a 2 × 3 grid. The participants were given 10 s to learn the shapes and their positions. In addition, they were required to draw the shapes on a piece of paper using a pencil without a time limit. It should be noted that the test was repeated three times (T1, T2, T3). Each drawing was allocated a score of 0, 1, or 2 based on the accuracy and positioning criteria of the six shapes.
Primary data related to the outcome of BVMT were reported in 4 studies.11,12,17,23 The results of the meta-analysis of these studies with a sample size of 176 patients in the cognitive rehabilitation group and 161 patients in the control group indicated that the outcome was significantly in favor of the cognitive rehabilitation group (MD = 2.72, 95% CI: 0.62 to 4.81, P = 0.01). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 51%, P = 0.11) (Figure 4).

Forest plot analysis of the BVMT.
Verbal fluency
Controlled Oral Word Association Test (COWAT). The COWAT is an oral fluency test in which the participant is required to make verbal associations to different letters of the alphabet by saying all the words which they can think of beginning with a given letter. Three letters of progressively increasing associative difficulty are presented successively as stimuli. The difficulty level of each letter is defined in terms of the relative frequency of words beginning with that letter in each language, as found in standard dictionaries of the language.
Primary data related to the outcome of the COWAT were reported in 4 studies.11,12,16,27 The results of the meta-analysis of these studies with a sample size of 199 patients in the cognitive rehabilitation group and 171 patients in the control group indicated that the outcome between the two groups was not significant (MD = 1.53, 95% CI: −0.54 to 3.61, P = 0.15). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 0%, P = 0.85) (Figure 5).

Forest plot analysis of the COWAT.
Verbal learning and remembering
California Verbal Learning Test (CVLT). This test starts with learning the first list of 16 words from four semantic categories (List A) over five trials. Words from the same category are not presented consecutively. At the end of each trial, the subject is asked to recall the words freely. A new list of words (List B) is then learned and freely recalled in a single trial. This interfering list contains new words belonging to two semantic categories present in List A, while the others belong to two new categories. The test continues with a free recall and a cued recall of List A (with the names of the categories serving retrieval cues). Finally, after a 20-min delay, List A is again tested with a free recall task, a cued recall task, and finally a yes/no recognition task.
Primary data related to the outcome of the CVLT were reported in 5 studies.11,12,17,21,22 The results of the meta-analysis of these studies with a sample size of 172 patients in the cognitive rehabilitation group and 174 patients in the control group indicated that the outcome between the two groups was not significant (MD = 0.86, 95% CI: −0.06 to 1.79, P = 0.07). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 0%, P = 0.64) (Figure 6).
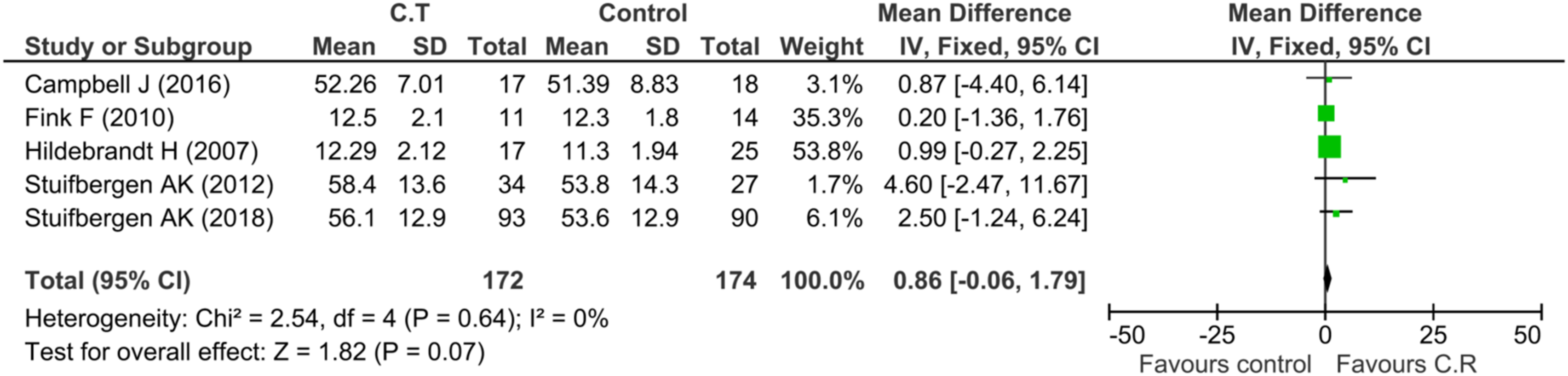
Forest plot analysis of the CVLT.
Scanning and visual tracking
Symbol Digit Modalities Test (SDMT). The SDMT is a screening instrument for the presence of brain damage. It requires individuals to identify nine different symbols corresponding to the numbers 1 through 9, and to practice writing the correct number under the corresponding symbol. Then they manually fill in the blank space under each symbol with the corresponding number.
Primary data related to the outcome of the SDMT were reported in 9 studies.11–15,17,23,24,27 The results of the meta-analysis of these studies with a sample size of 249 patients in the cognitive rehabilitation group and 232 patients in the control group indicated that the outcome between the two groups was significant in favor of the control group (MD = 2.99, 95% CI: 0.98 to 4.99, P = 0.004). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 0%, P = 0.65) (Figure 7).

Forest plot analysis of the SDMT.
Self-report outcomes
Everyday Memory Questionnaire (EMQ)
EMQ questionnaire is a 28-item questionnaire assessing general memory and attention aspects. Each item was scored from 0 to 5 according to the frequency of problems reported. High scores indicate more memory problems.
Primary data related to EMQ outcomes were reported in 3 studies.28–30 The results of the meta-analysis of these studies with a sample size of 72 patients in the cognitive rehabilitation group and 70 patients in the control group indicated that the outcome between the two groups was not significant (MD = 1.45, 95% CI: −0.84 to 3.74, P = 0.21). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 0%, P = 0.9) (Figure 8).

Forest plot analysis of the EMQ.
MS Neuropsychological Screening Questionnaire (MSNQ)
The MSNQ was used as a measure of neuropsychological competence with activities of daily living. Respondents rated how often they experienced each of the 15 items during the last three months. The items include common problems reported by persons with MS (e.g. being easily distracted, difficulty following conversations, and forgetting appointments).
Primary data related to the outcome of MSNQ were reported in 2 studies.11,16 The results of the meta-analysis of these studies with a sample size of 92 patients in the cognitive rehabilitation group and 67 patients in the control group indicated that the outcome was significant in favor of the cognitive rehabilitation group (MD = 3.94, 95% CI: 0.68 to 7.19, P = 0.02). The heterogeneity test did not show a significant difference in terms of heterogeneity (I2 = 0%, P = 0.6) (Figure 9).

Forest plot analysis of the MSNQ.
Beck Depression Inventory (BDI)
The BDI is a 21-item, self-report rating inventory that measures characteristic attitudes and symptoms of depression.
Primary data related to the outcome of BDI were reported in 6 studies.13,15,16,22,27,30 The results of the meta-analysis of these studies with a sample size of 143 patients in the cognitive rehabilitation group and 132 patients in the control group indicated that the outcome was significant in favor of the cognitive rehabilitation group (MD = −3.27, 95% CI: −6.97 to 0.43, P = 0.08). The heterogeneity test showed a significant difference in terms of heterogeneity (I2 = 79%, P = 0.0002) (Figure 10).

Forest plot analysis of the BDI.
Functional scales
Expanded Disability Status Scale (EDSS)
The EDSS is a way of measuring how much someone is affected by their MS. The EDSS has a range from 0 to 10. Scores are in half-unit steps, that is, 3, 3.5, 4, and so on. The greater the level of disability, the higher the score out of ten.
Primary data related to the outcome of the EDSS were reported in 3 studies.13,15,22 The results of the meta-analysis of these studies with a sample size of 43 patients in the cognitive rehabilitation group and 50 patients in the control group indicated that the outcome between the two groups was not significant (MD = 0.3, 95% CI: −0.39 to 1.00, P = 0.39). The heterogeneity test shows a significant difference in terms of heterogeneity (I2 = 0%, P = 0.65) (Figure 11).

Forest plot analysis of the EDSS
Discussion
Based on the inclusion and exclusion criteria, 20 studies were finally selected for meta-analysis from the 578 studies that were initially reviewed. Therefore, all RCT studies that compared the effectiveness of cognitive rehabilitation with a control group in MS patients were included in this meta-analysis.
After evaluating the quality and extracting the relevant data, meta-analysis was performed on 6 outcomes. The results of this meta-analysis showed significant effectiveness in PASAT, BVMT, MSNQ, and BDI outcomes. Although no statistically significant correlation was observed in the results of COWAT, CVLT, EMQ, SDMT, and EDSS, it seems that if the sample size is increased or the follow-up time is increased or the number of treatment sessions is increased, effective results can also be observed in these results.
The results of this meta-analysis have shown that cognitive rehabilitation has an effect on the cognitive functions of patients with MS. The outcomes related to the working memory of patients with MS were investigated and analyzed separately. The obtained results showed that there is a significant improvement in working memory by the cognitive rehabilitation program of working memory. In explaining this recovery, it can be said that the CNS always deals with the damaged circuit and the person's performance improves somewhat after the injury, which may occur as a result of changes in the nervous organization in response to the injury. A systematic review by Mhizha-Murira et al. 31 showed that the quality of reporting of cognitive rehabilitation for memory, attention and executive function for MS was poor across a wide range of study designs. Klein et al. 32 have investigated qualitative studies of patient perspectives for memory, attention and executive function problems in people with MS by conducting a meta-synthesis. This synthesis of qualitative studies indicates that people with MS who experience cognitive deficits benefit from cognitive rehabilitation programs. The results of other review studies showed that cognitive rehabilitation is generally effective in patients with MS. 33
The results of the meta-analysis showed that cognitive rehabilitation creates changes in working memory, which is probably a result of changes in synaptic functions and related brain areas, and due to the overlap of the areas involved in working memory and selective attention, the conclusion that cognitive rehabilitation of working memory causes improvement of selective attention is also confirmed. Because the involvement and recovery of a similar brain region can be observed in the results obtained from the meta-analysis of the outcome of selective attention, and of course, this issue will require further investigations.
One of the limitations of this meta-analysis was the lack of reporting of some statistical data in the included studies for analysis. One of the important statistical data for meta-analysis of continuous outcomes is the standard deviation. Due to the fact that the studies included in the meta-analysis of continuous outcomes reported mean outcomes without standard deviation, some studies were not included in the final analysis of the meta-analysis. If the standard deviation was reported in these studies, meta-analysis of the results will bring more accuracy and confidence. Despite the efforts made to contact the authors responsible for these studies, we did not obtain any results.
Another limitation of this meta-analysis was the short follow-up time of the results in the included studies for analysis. In the scope of our knowledge and based on the included studies, there was no evidence that investigated functional outcomes in long-term follow-up times (more than one year), and there is a gap in studies in this case. It seems that in order to make a more realistic decision and judge about the role of cognitive rehabilitation on the memory functions of a patient with MS, it is necessary to conduct quality studies with a follow-up time of more than one year.
Conclusion
The Results of this meta-analysis showed that cognitive rehabilitation has an effect on improving the performance of patients with MS. However, further studies with a more accurate methodology are required to determine which of the outcomes cognitive rehabilitation has a greater effect on. Since cognitive functions improve with the application of cognitive rehabilitation training, it is suggested to use interventions based on cognitive rehabilitation in addition to psychological interventions as an integrated, practical and supportive treatment approach along with drug therapy.
Footnotes
Acknowledgments
The authors would like to thank the following individuals who have contributed at various stages through the development of this project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local ethical committee (code: IR.SBMU.RETECH.REC.1401.408) and the Helsinki Declaration was respected across the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Physical Medicine and Rehabilitation Research Center at Shahid Beheshti University of Medical Sciences.