
Abstract
Objective
The objective of this study was to characterize the use of cannabis-based products (CBPs) by multiple sclerosis (MS) patients who attend the University of British Columbia Hospital (UBCH) MS clinic.
Methods
All patients attending the UBCH MS clinic from January to March 2018 were invited to participate in an anonymous survey that included: patient demographics (sex, age and employment status), self-reported MS-specific data (subtype, disease duration, previous and current disease modifying therapies, symptomatic medications) and CBP use (formulation, frequency, perceived benefits/side-effects). A second cohort of retrospective patient data (CBP use, sex, age, disease subtype and Expanded Disability Status Scale) was extracted from the UBCH MS clinic electronic medical record (EMR).
Results
Of 600 surveys distributed, 188 were returned with completed CBP usage. CBP use was daily for 19% (n = 37), weekly for 6% (n = 11), monthly for 4% (n = 7), rarely for 21% (n = 39) and 50% (n = 94) never used. Of the CBP users (daily, weekly and monthly), CBP use included: oral (n = 43/55), smoked/vaporized (n = 42/55), topical (n = 14/55) and mucosal (n = 5/55). EMR data was available for 561 MS patients where cannabis use/non-use was documented. CBP users represented 19% (107/561).
Conclusions
CBP use is common based on volunteer reporting, with approximately one out of four patients who attend the UBCH MS clinic using CBPs.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system which can cause substantial morbidity. 1 Cannabis-based products (CBPs) have been studied in MS patients for the symptomatic management of pain, bladder symptoms, tremor, mood, sleep, spasticity and ataxia.2–6 A systematic review concluded that CBP may have modest benefits for pain and spasticity, with insufficient evidence to support its use for other symptoms. 7 However, there is concern about negative effects of CBP including worsening cognition8,9 and posture/balance, 10 in an already vulnerable patient population. 11
Despite the uncertainties, cannabis usage in Canada is high with 40% of Canadians reporting lifetime use, and 25% reporting doing so for medicinal purposes. 12 Within Canada, CBP use is highest in the province of British Columbia. In October 2018, cannabis was legalized for recreational use throughout Canada representing a fundamental shift in cannabis usage in the country. The University of British Columbia Hospital (UBCH) Multiple Sclerosis clinic is located in Vancouver, British Columbia, Canada and offers specialized longitudinal MS care to over 6000 patients. In this study, we attempt to gain further insight into the state of CBP use in MS prior to legalization, through both an anonymous patient survey and analysis of self-reported patient data prospectively recorded in the electronic medical record (EMR).
Methods
The study was approved by the UBC Clinical Research Ethics Board and the Vancouver Costal Health Research Institute (H17-02221 & H18-02820). There were two cohorts: patients who completed a survey on CBP use and analysis of the EMR records pertaining to CBP use.
Survey cohort
Patients attending the UBCH MS clinic from January 2018 to March 2018 were invited to participate in an anonymous survey. Upon arrival for a scheduled clinic appointment, patients were offered a survey and then returned it to the front desk after completion. In total, 600 surveys were distributed (see Supplementary Material).
The survey included: participant demographics (sex, age and employment status), self-reported MS-specific data (subtype, disease duration, patient determined disease steps (PDDS)1,3), previous and current disease modifying therapies, symptomatic medications and CBP use (products, frequency, perceived benefits/side-effects and effectiveness). Additional questions included: if CBP usage had been discussed with the patient’s MS neurologist, if the CBP had been prescribed by a physician and if the respondent was a regular CBP user prior to their MS diagnosis.
For analysis of the results, ‘CBP users’ included the responses: ‘daily’, ‘weekly’ or ‘monthly’. ‘Non CBP users’ included ‘rarely’ and ‘never’. First line medications included: Interferons, Glatiramer Acetate, Teriflunomide and Dimethyl Fumarate. Second line medications included: Rituximab, Ocrelizumab, Fingolimod, Alemtuzumab and Natalizumab. Survey results were entered into a standardized data collection spreadsheet by two individuals (AS, VV). Of the completed surveys 15% underwent a second validation process to ensure accuracy of data entry.
EMR cohort
Patients were asked by their neurologist to self-report about CBP usage (yes/no) as part of the social history and this was recorded in the EMR at each clinic visit. Inclusion criteria were patients assessed by a single clinician (RC), from April 2017 to September 2018 and had a confirmed diagnosis of MS. Sex, age, disease subtype and Expanded Disability Status Scale (EDSS) scores were also extracted. Data for a random sample of 20% of included patients were validated by reviewing the EMR records.
Statistical analysis
For both cohorts, statistical analysis comparing CBP users to non-users was done using a Fisher’s Exact Test with a significant difference being p < 0.05 by an independent third-party statistician. Patients who did not complete the CBP usage on the survey, and those with incomplete CBD usage in the EMR, were removed prior to the analysis. Any missing data for the other variables (i.e. sex, age, disability, etc.) were removed for the analysis of that variable only. In the survey cohort, CBP usage, products used and cannabinoid ratio was broken down by sex and compared using a Fisher’s Exact Test.
Results
Survey cohort
Of 600 surveys distributed, 259 were returned and completed. Those with a diagnosis other than MS (n = 14) and the 57 respondents who did not provide their level of CPB use were excluded from analysis. A total of 188 respondents were included in the final analysis. Responders were 75% female. The mean age was between 42.4 and 51.7 years (range midpoint 47.05) and the median age between 46 and 55 years (range midpoint 50.5).
CBP usage
The CBP users (daily, weekly or monthly) represented 29% (n = 55/188) with non-CBP users (rarely or never) representing 71% (n = 133/188) (Table 1). Oral and/or smoked were the most common formulations (78 and 76% of the CBP users respectively), and THC (tetrahydrocannabinol) > CBD the most common cannabinoid ratio.There was no statistically significant difference in sex for CBP usage, products used or cannabinoid ratio.
Survey results (n = 188) showing frequency of cannabis-based product (CBP) use and, of the CBP users (n = 55), types of products used and preferred cannabinoid ratio. Un-adjusted p-values for sex differences for each variable is listed.

THC: tetrahydrocannabinol.
Perceived benefits and side-effects
Of the CBP users (n = 55), the most common reasons for initiation of CBPs were pain (n = 39, 71%) and sleep (n = 39, 71%) (Table 1). Respondents indicated that CBPs led to symptomatic improvement for 95% (n = 52) of individuals. The most common perceived side effects were memory disturbance (n = 11, 20%) and brain fog (n = 10, 18%) (Table 2). Many respondents reported no side effects (n = 31, 56%).
Survey results (n = 55): symptoms leading to cannabis-based product (CBP) initiation and perceived side effects.

CBP users compared to non-users
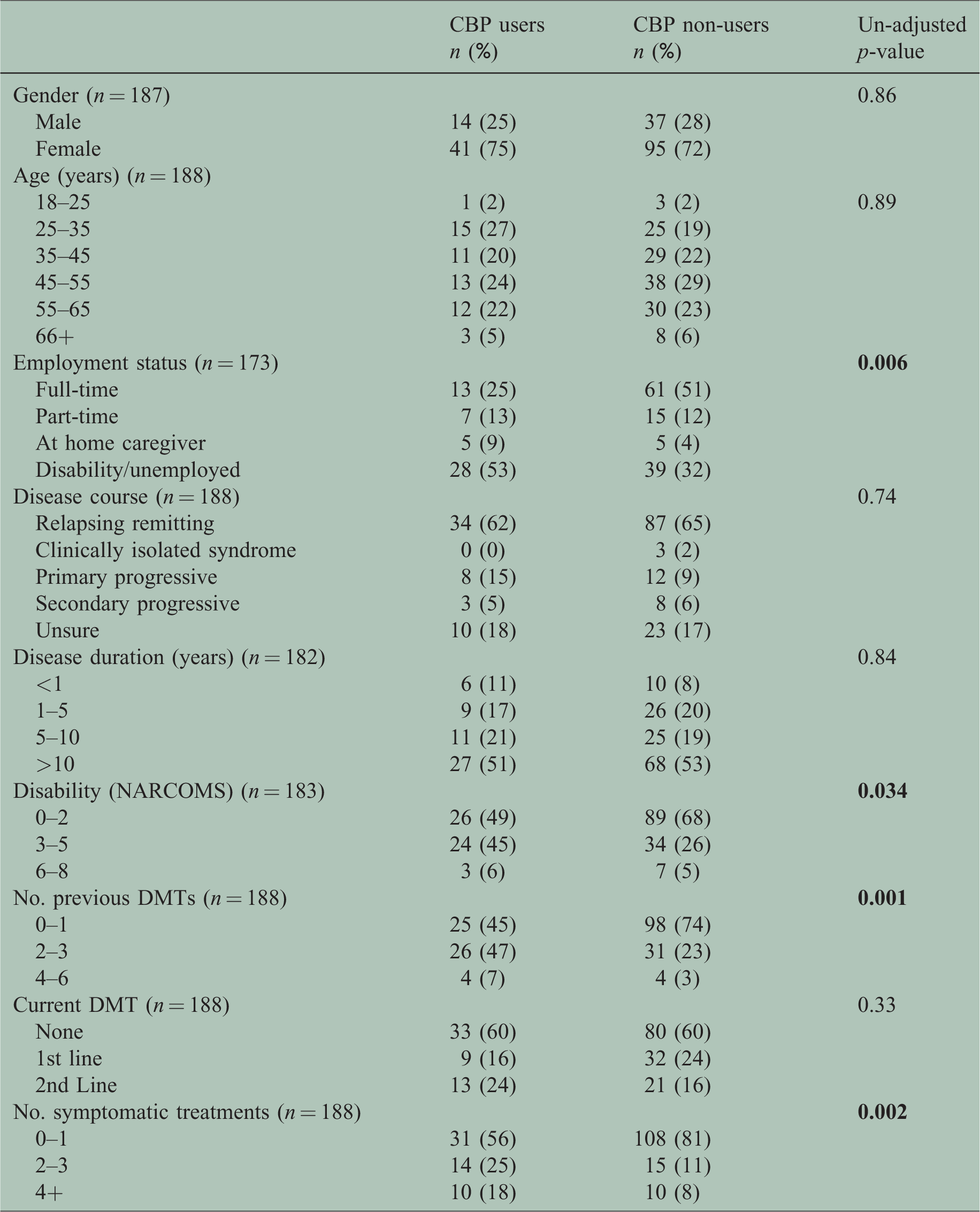
There was no statistically significant difference in: sex, age, disease course, disease duration and current DMT use between CBP users and non-users. More CBP users were unemployed, had greater disability and had tried more disease modifying and symptomatic treatments (Table 3).
Survey of cannabis-based product (CBP) users (n = 55) compared to non-users (n = 133): demographics, MS-specific data, previous and current disease modifying treatments (DMTs) and symptomatic treatments.
Additional questions
Of the CBP users, 51% (28/55) of respondents discussed CBP usage with their MS neurologist, 18% (10/55) had the CBP prescribed/authorized by a physician and 33% (18/55) regularly used CBPs prior to MS diagnosis.
EMR cohort
Data from 667 individuals followed by a single clinician (RC) who routinely acquires patient reported CBP usage was extracted from the EMR. Those with a diagnosis other than MS (n = 82) and with missing cannabis usage information (n = 24) were excluded from analysis. Of the 561 that remained, 73% were female. The age range was 19–89 years with a mean of 52.8 years and a median of 54 years.
CBP usage
CBP users represented 19% (107/561) while non-users represent 81% (454/561). There was no significant difference in EDSS scores between users and non-users. More CBP users were male, younger and had relapsing MS (Table 4). Disease course, disease duration and medication use were not analyzed in this component of the study, as this information was not available.
Electronic medical record patient database results (n = 561) comparing cannabis-based product users (n = 107) to non-users (n = 454) for sex, age, disease course and Expanded Disability Status Scale (EDSS).

Discussion
CBP usage is common in this representative Canadian MS cohort study, with 29% of survey participants and 19% of patients with self-reporting documented in the EMR. This cohort has an overall higher percentage of CBP usage in Canadian MS patients than previous surveys (done between 2004–2016), that report 14–19.5% of patients using CBPs.13–15 Given that prior research suggests that the majority of patients support the legalization of cannabis for medicinal purposes,15–17 the recent legalization of cannabis in Canada (October 2018) may further influence use, highlighting the need for continued assessment regarding the benefits, harms and safety profile of CBPs.
Male gender has previously been associated with CBP use.13–14 While the EMR cohort showed more males in the CBP users group compared to the non-users (40 v. 24%), the survey cohort showed a similar gender distribution in both CBP users and non-users (25 v. 28% male). This possible shift away from male predominance may represent changing attitudes towards CBPs. Another significant difference from previous surveys is the increasing use of non-inhaled CBPs. A 2016 survey in Toronto, Ontario, reported smoked CBP to be the most common method of use (59%), with oral methods used by only 11%. 15 While smoked/vaporized CBP use was still high (76%) in the survey cohort, oral administration was also very common (78%).
Current guidelines support CBP use for the symptomatic management of pain and spasticity in MS, without enough evidence to recommend its use for other MS symptoms.7,18 The survey results align with these recommendations with 71 and 40% of individuals using CBPs for pain and spasticity, respectively. Patients at the UBCH MS clinic are also using CBPs for sleep (71%) and mood (44%). Interestingly, 95% of the survey CBP users felt that CBPs lead to symptomatic improvement. CBP users have tried more symptomatic medications compared to non-users (p = 0.002), 35% of CBP users have not tried any other symptomatic medications and 56% have tried one or less. The motivation for trying CBPs for MS symptom management may vary significantly amongst individuals and cannot be fully addressed by the current study.
Our survey showed that CBP users had greater disability and higher levels of unemployment compared to non-users (p = 0.034, p = 0.006). This finding, however, does not imply causation, as higher disability may result in increased need for symptomatic medications (including CBPs) and unemployment may also reflect increased disability. Another interesting finding is that while CBP users had higher disability compared to non-users, 49% of CBP users only had mild disability (patient perceived disability of 0–2), 1 indicating that CBP use is not limited to those with higher levels of disability. There was no difference in age between users and non-users (p = 0.89). The EMR cohort showed no significant difference in EDSS scores (p = 0.34), and the CBP users were younger compared to non-users (p < 0.001). The motivation for using CBP over other symptomatic treatments requires further study.
Of the 188 responses from the 600 surveys distributed, 55 (29%) indicated current, regular CBP use. Of this group of 55 CBP users, 33% (18/55) used CBPs prior to MS diagnosis, suggesting that 67% initiated CBP use after MS onset. Yet, only half discussed CBP usage with their physician, and only 18% had it authorized or prescribed by a physician, indicating a gap in communication between patients and physicians. CBPs do appear to have a role in symptomatic treatment of MS,7,18 and the use in Canada could become more common given the recent legalization of cannabis. In order to effectively guide patient care and future research, bridging the gap between the patient understandings, perceived benefits and data regarding harm is of the outmost importance.
There are several limitations with this study that relies on volunteer participation and self-reporting. While the survey was offered to all patients, there was a potential completion bias in which patients who are using CBPs were more likely to return the survey, thus leading to an over estimation of CBP use. Reporting errors in surveys also could bias results. Patients may have under-report their usage during clinic visits that were recorded in the EMR prior to legalization of cannabis in October 2018. Furthermore, there may be a perception amongst patients that their physician would not support the use of alternative therapies, leading to further under-reporting. This may account for the discrepancy between CBP use reported between the survey and EMR cohorts (29 v. 19%). Given the potential completion bias for the survey sample and potential under-reporting bias for the EMR sample, p-values have limited interpretation. It should also be noted that the survey cohort and EMR cohort are not mutually exclusive groups, and that some of the patients may be represented in both cohorts.
Conclusions
Using data gathered from both an anonymous survey and EMR patient encounters, CBP use by MS patients who attend the UBCH MS clinic appears common. Based on the biases of each methodology, the true prevalence of CBP use is approximately one out of four MS patients in our local cohort (between 19 and 29%). Pain and sleep were the most common symptoms treated and perception of benefit was high (95%). Further study of CBP use in this patient population is warranted.
Supplemental Material
MSO869360 Supplemental Material - Supplemental material for Cannabis-based product use in a multiple sclerosis cohort
Supplemental material, MSO869360 Supplemental Material for Cannabis-based product use in a multiple sclerosis cohort by AJ Schabas, V Vukojevic, C Taylor Z Thu, A Badyal, JK Chan, V Devonshire, A Traboulsee, AL Sayao and R Carruthers in Multiple Sclerosis Journal–Experimental, Translational and Clinical
Footnotes
Acknowledgements
The clerical staff at the University of British Columbia Multiple Sclerosis clinic for distributing the survey.
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.