
Abstract
Background and objective
Study evaluating Betaferon(R)'s safety and tolerability in paediatric patients with multiple sclerosis (BETAPAEDIC) is a prospective, open-label observational multicentre study to assess the safety and effectiveness of interferon beta-1b in paediatric patients with relapsing–remitting multiple sclerosis.
Methods
Treatment-naïve patients (12–16 years) scheduled to start interferon beta-1b were enrolled with follow-up visits every six months for two years. Effectiveness was evaluated by annualised relapse rate, Expanded Disability Status Scale progression, cranial magnetic resonance imaging and cognitive testing. Fatigue was assessed by the Fatigue Severity Scale.
Results
Sixty-eight patients were screened and 67 enrolled, with mean (standard deviation) age 14.2 (1.3) years (n=65 in the effectiveness analysis). Mean disease duration was 11 months before study enrolment; at baseline, mean (standard deviation) Expanded Disability Status Scale was 0.6 (1.0); T2 lesion number 18.3 (15.1). Mean annualised relapse rate during the study was 0.7 (n=57), 28/57 patients (49.1%) had no relapses and for 40/52 (76.9%) no Expanded Disability Status Scale progression was observed; 23/56 (41.1%) were relapse- and progression-free to last follow-up. Neuropsychological test and fatigue scores were within normal ranges (baseline and last follow-up). Eighteen patients had fatigue at some point. New T2 and gadolinium-enhancing (Gd+) lesions were seen in 43/55 (66.2%) and 29/55 (52.7%) patients respectively. Most frequent adverse events were influenza-like illness, headache, injection-site reactions and elevated liver enzymes.
Conclusion
Interferon beta-1b is an effective treatment with a favourable safety profile for paediatric patients.
Introduction
Approximately 3–10% of all patients with multiple sclerosis (MS) experience symptom onset before the age of 18 years, most often as relapsing–remitting MS (RRMS). 1 Most paediatric patients with MS show good recovery after relapse, but usually have accumulated disabilities within 15 years of the initial episode and therefore at an earlier age compared with adult-onset patients. 1 Initially, presenting symptoms can vary. The spectrum may include optic neuritis or sensory, motor, cerebellar or brainstem dysfunction, with approximately 50–70% of children being polysymptomatic at presentation. 1
Paediatric patients with MS face unique challenges, including physical disability, cognitive impairment, fatigue and psychological impacts. 2 Paediatric patients will typically have higher relapse rates and be more disabled at a younger age than patients with adult-onset MS.3,4 In addition, fatigue may impact school attendance. 2 Deficits in cognitive processing speed, concentration, verbal working memory, abstract reasoning and visual-motor integration can also occur.5–7 Disease milestones are also mostly reached at a younger age for paediatric patients with MS, with one study showing conversion to secondary progressive MS (SPMS) typically occurring at a median age that was 10 years younger than in adult patients. 4
The International Paediatric MS Study Group (IPMSSG) recommends early disease-modifying treatment for paediatric patients with RRMS due to the benefits seen in adults.8,9 Small retrospective studies and case reports in paediatric populations indicate that interferon beta-1b has a favourable safety profile, similar to that seen in adults, and may reduce relapse rates and delay disease progression.10–12 Based on the results of these and other studies that also included interferon beta-1a as well as those assessing glatiramer acetate, IPMSSG recommends that all paediatric patients with MS be considered for treatment with an interferon beta formulation or glatiramer acetate. 8
Study evaluating Betaferon(R)'s safety and tolerability in paediatric patients with multiple sclerosis (BETAPAEDIC) is the first prospective, international, multicentre, non-interventional post-authorisation safety study of interferon beta-1b in paediatric patients with MS. This observational real-life study had an open-label, single-arm design. The objectives of BETAPAEDIC were to examine the safety, tolerability and effectiveness of interferon beta-1b in paediatric patients with RRMS.
Methods
Treatment-naïve adolescent patients aged 12–16 years who were diagnosed with RRMS according to revised McDonald (2005) or Poser criteria were enrolled in 14 academic hospitals/MS centres in Austria, Belgium, Finland, Germany, Israel and the UK. All patients were scheduled by the investigators to be treated with interferon beta-1b with a recommended dose of 250 μg administered subcutaneously every other day. Dose titration at the start of treatment was recommended and could be implemented at the discretion of the treating physician. Patients with contraindications to treatment with interferon beta-1b according to local labelling (i.e. contraindications, warnings and precautions) were excluded. Informed consent was collected from parents or legal guardians after the decision to treat with interferon beta-1b was made. Institutional review board approval was obtained from all participating centres.
Patients were observed for two years, with visits every six months. At the initial visit, investigators assessed demographics, disease history and relevant medical history according to available patient reports and clinical records, disability status, fatigue, and cranial magnetic resonance imaging (MRI) findings if they were available. Subsequent visits measured fatigue, MS disease course including relapses and Expanded Disability Status Scale (EDSS) progression, disability and adverse events (AEs). Neuropsychological function was assessed only at baseline and after two years to avoid practice effects. If a cranial MRI was conducted, findings were recorded. Clinical effectiveness was evaluated by assessment of relapse rates and EDSS progression (defined as ≥1.0-step increase from baseline). Tests of neuropsychological function included measures of intelligence, attention and concentration, and visual-motor integration. Intelligence was assessed using the Wechsler Intelligence Scale for Children – Fourth Edition (WISC-IV)13,14 and Raven’s Standard Progressive Matrices (SPM; Classic, Parallel and Plus version). 15 The d2 Test of Attention (d2 Test)16,17 was used to assess attention and concentration. Visual and motor integration was measured using the Beery-Buktenica Developmental Test of Visual-Motor Integration, Sixth Edition (Beery VMI). 18 Fatigue was measured using the Fatigue Severity Scale (FSS). Cranial MRI findings (number of new T2 or gadolinium-enhancing (Gd+) lesions) were included if available.
All AEs and serious AEs (SAEs) that started during treatment with interferon beta-1b from the intake of the first dose up to 30 days after the last dose within the study were recorded and summarised using the medical dictionary for regulatory activities (MedDRA) coding system. Investigators assessed the seriousness, duration, relationship to study drug, action taken and event outcome. AEs were categorised according to relation to treatment, seriousness, discontinuation of therapy and outcome. Rates for AEs were based on the total number of documented patients validated for safety assessments.
Results
Sixty-eight patients were screened and 67 were enrolled at 14 centres in six countries (one patient was excluded because he did not meet the minimum age requirements for the study). An additional two patients had interferon beta-1b exposure prior to study entry that exceeded the maximum allowed and therefore only their safety-related data were analysed and reported here. After two years, 34 patients (52.3%) had completed the fourth follow-up visit. Baseline and demographic characteristics are shown in Table 1. Among all patients, the age group of 15 years represented the largest group in this cohort (n=26, 40%). Fifty patients (76.9%) were female and 15 (23.1%) were male giving a female-to-male ratio of 3.33:1. Mean (standard deviation (SD)) time since disease onset was 11 (18) months with a mean (SD) time since diagnosis of five (17) months. During the two years before study entry, patients had experienced a mean (SD) of 2.2 (1.4) relapses (based on information retrieved from hospital documentation). Twenty patients (30.8%) were diagnosed according to revised McDonald (2005) criteria while 45 (69.2%) fulfilled Poser criteria.
Demographic and baseline clinical and magnetic resonance imaging (MRI) characteristics.

BMI: body mass index; EDSS: Expanded Disability Status Scale; SD: standard deviation.
aBased on information retrieved from hospital documentation
On-study relapse data were available for 57 patients. Frequency of relapses during the study seemed to have decreased relative to prior to study start, with a mean (SD) number of relapses of 1.0 (1.4) from baseline up to the patient’s last follow-up visit. Mean (SD) annualised relapse rate during the study was 0.7 (1.1) (median (Q1, Q3) 0.4 (0.0, 0.9)). In the subgroup of patients with ≥1 year of disease duration before start of the study (n=17), ARR was 0.7 on-study compared to 1.6 prior to study entry (Figure 1). When calculating an ARR in those patients with ≥6 months of disease duration before the study start (n=29), ARR was 0.8 on-study compared to 2.4 prior to study entry. The overall mean (SD) number of relapses per patient was lower during the study (1.0 (1.4)) than in the period prior to enrolment (2.2 (1.4)) even though the average time period on-study (mean (SD) 1.7 (0.6) years) was longer than the pre-study period (mean (SD) 0.7 (0.6) years). Up to their last follow-up visit, 28 patients (49.1%) were relapse-free in the total cohort with relapse data, while 29 (50.9%) reported relapse occurrence since baseline. Complete recovery from relapse by the last follow-up visit was reported in 10 of 20 patients (50.0%) who had relapses (information not given for nine patients).

Annualised relapse rate (ARR) prior to and during the study. ARR in the two years before the start of study and during the observation period of the study evaluating Betaferon(R)'s safety and tolerability in paediatric patients with multiple sclerosis (BETAPAEDIC) study. Overall, ARR tended to decrease during treatment with interferon beta-1b relative to the pre-study period. Patients with disease duration <6 months were not included in pre-study ARR calculations to avoid overestimation.
For 40 patients (76.9% of the 52 patients with data available) no EDSS progression (defined as a 1.0-point increase in EDSS) was recorded up to their last follow-up. Mean (SD) EDSS score at the last follow-up visit was 0.6 (0.9) and mean (SD) EDSS change from baseline score was 0.0 (0.9). No patients converted to SPMS (data available from 57 patients). Twenty-three patients (41.1% of 56 with data available) were relapse- and EDSS progression-free from baseline to last follow-up visit (no evidence of disease activity (NEDA-2).
Neuropsychological performance including intelligence, visual-motor integration and attention, was within normal ranges at baseline and at the last follow-up visit (Table 2). Mean (SD) total FSS score was 3.0 (1.3), mean FSS visual analogue scale was 3.7 (2.8) (n=29), indicating no symptoms of fatigue (Figure 2) at last follow-up visit. In 18 of 49 patients with data available (36.7%), mean total FSS score was >4 (indicating the presence of fatigue) at some point during the study.
Cognitive measures at baseline and at last follow-up, mean (SD).
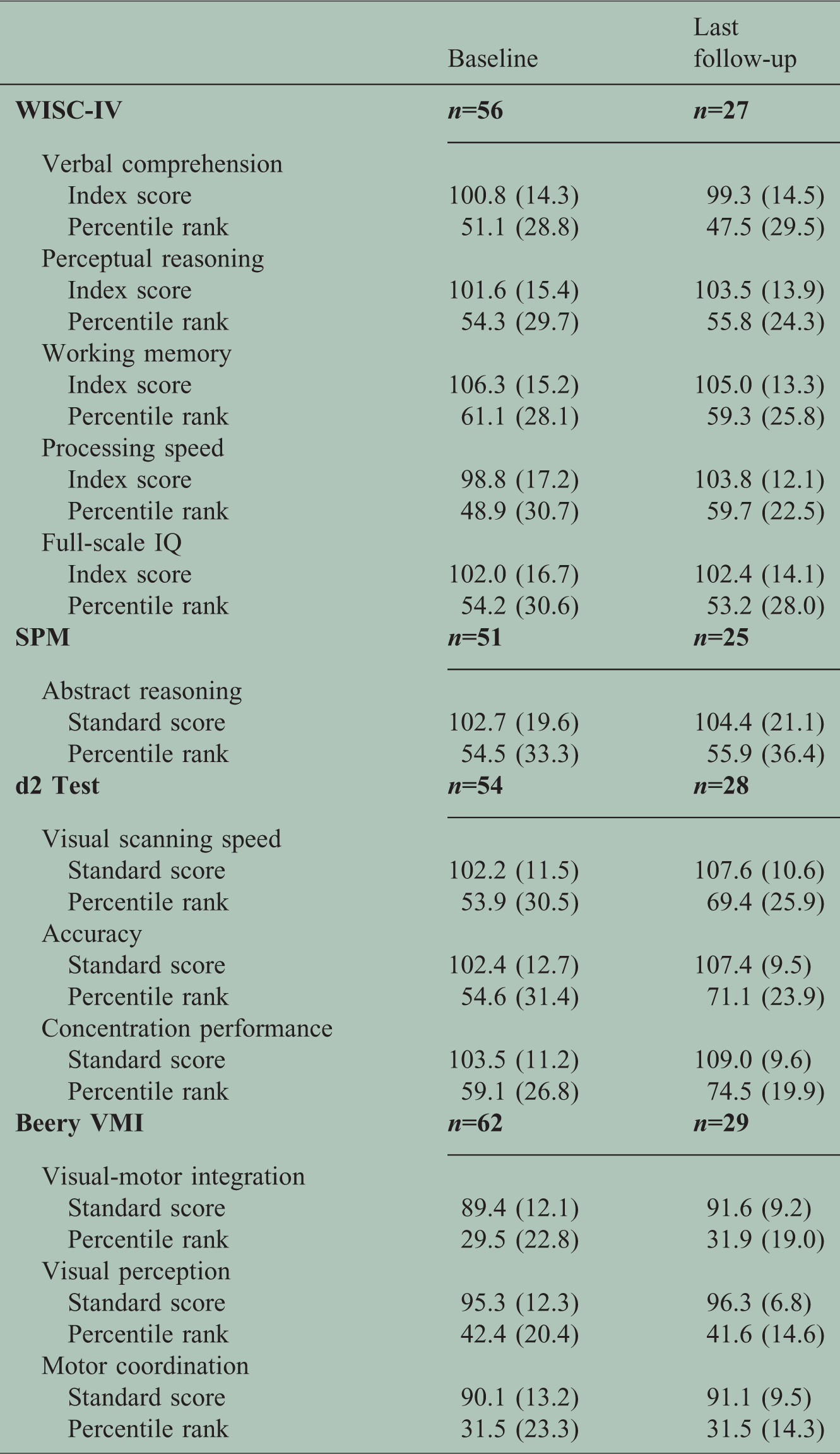
Beery VMI: Beery-Buktenica Developmental Test of Visual-Motor Integration, Sixth Edition; d2 Test: d2 Test of Attention; SPM: Raven’s Standard Progressive Matrices; WISC-IV: Wechsler Intelligence Scale for Children, Fourth Edition.
Beery VMI standard score: 100 (15); d2 Test standard score: 100 (10); SPM standard score 100 (15); WISC-IV standard score: 100 (15). Percentile rank indicates the percentage of scores in a population distribution equal to or below the given score.

Fatigue Severity Scale (FSS) scores. FSS scores at baseline and the last follow-up visit (mean (standard deviation (SD))). Items 1–9 consisted of questions related to fatigue during the past two weeks that were answered by the patient on a scale of 1–7 in which higher scores indicated more severe symptoms of fatigue. The 100-mm Visual Analogue Scale required patients to mark a line to indicate the severity of their fatigue in the past two weeks (higher numbers indicated more severe symptoms of fatigue).
Cranial MRI data were available from 48, 43, 38 and 29 patients respectively at the first, second, third and fourth follow-up visit. From those 55 patients who underwent MRI assessment at the last individual follow-up visit, 43 (78.2%) had new T2 lesions and 29 (52.7%) had new Gd+ lesions. Six of those 56 patients with MRI had no new T2 and Gd+ lesions (NEDA-3) up to the last visit.
Sixty-one of 67 patients included in the safety population (91.0%) reported in total 294 AEs during the study period. Of these AEs, 12 (4.1%) were classified as serious (SAEs), either because of the need for hospitalization (10 AEs (3.4%)) or because of another medically important event (two AEs (<1%)). Interferon beta-1b was considered to be related to 152 AEs (51.7%) in 51/67 patients (76.1%), but little change to the medication dose or schedule was required for most patients. The interferon beta-1b dose remained unchanged after 267 (90.8%) reported AEs (i.e. in 59/67 patients (88.1%)), with six (2.0%) necessitating temporary treatment interruption (i.e. in 4/67 patients (6%)), six (2.0%) requiring dose reduction (i.e. in 4/67 patients (6%)), and two (<1%) leading to discontinuation of interferon beta-1b treatment (i.e. in 2/67 patients (3%)).
The most frequently reported drug-related AEs (in n(%) patients) were influenza-like illness (31 (46.3)), headache (13 (19.4)), injection-site reactions (11 (16.4)) and elevated liver enzymes (eight (11.9)) (Table 3). The AEs leading to discontinuation of interferon beta-1b were influenza-like illness (one patient (1.5%)) and Henoch-Schonlein purpura (one patient (1.5%)). The SAE incidence rate was 11.9% (12 events in eight of 67 patients). In three patients (4.5%) SAEs were considered drug-related by their physician. These were benign intracranial hypertension, depression and nephrotic syndrome, and these cases were all recovered/resolved. There were no patients with fatal outcomes. Overall, the safety profile of interferon beta-1b in paediatric patients appeared to be similar to that which has been seen in previous clinical trials of adult patients with MS; no new safety signals were reported.
Drug-related adverse events (AEs) reported in ≥2% of patients.

Multiple responses per patients could be included.
Defined using local laboratory cut-off values.
Discussion
The results of this two-year study in treatment-naïve paediatric patients with MS who started early treatment with interferon beta-1b showed that disability remained stable over the study period, relapses on average appeared less frequent than prior to study entry, on average no indication of fatigue was present, and cognitive performance was within normal ranges. Some degree of disease activity was observed on cranial MRI in those patients who underwent MRI assessment. The findings in this cohort of paediatric patients with MS treated with interferon beta-1b are particularly important given that higher disease activity, including cognitive impairment (which is found in 30–50% of patients), has been previously described in paediatric MS.4,19
The AEs reported in BETAPAEDIC were consistent with the known safety profile of interferon beta-1b, with few patients requiring changes to dosing or discontinuation of treatment. Influenza-like symptoms, injection site reactions, or headache are known to occur in adult patients taking interferon beta-1b and can be managed through various interventions without disrupting treatment for MS. 20 Thus, the findings from BETAPAEDIC suggest that paediatric patients with MS are not vulnerable to different or more severe AEs when compared with adults undergoing treatment with interferon beta-1b.
Overall, these results are in accordance with other studies that assessed the safety and effectiveness of interferon beta formulations in paediatric patients with MS. As summarised recently by Ghezzi et al, 21 early intervention with interferon beta-1a or -1b reduced relapse rates relative to pre-study baselines and prevented the accumulation of additional disabilities in several smaller observational trials. In light of this evidence, interferon beta formulations are a recommended choice for the initial treatment of paediatric patients with MS.8,21 The rationale for interferon beta-1b in this setting is further strengthened by the results of the BETAPAEDIC study.
Limitations of this study include the relatively small patient population, the lack of a comparator arm, the relatively short follow-up period and the collection of MRI data according to clinical practice which limited MRI follow-up to a subset of the overall cohort who may have had more clinically active disease. Although the number of patients enrolled was appropriate for a rare paediatric disease but rather small compared with clinical trials in adult patients with MS, and limited to a single-arm, non-randomised design, BETAPAEDIC represents the largest prospective trial of interferon beta-1b for paediatric patients conducted to date. The trial therefore adds significant knowledge to the body of evidence on the treatment of this comparatively rare patient population. Since interferon beta-1b is an established first-line therapy, BETAPAEDIC is an open-label post-authorisation safety study providing real-life evidence data beyond a randomised clinical trial with comparator but in a more restricted setting. However, the relatively short follow-up period of only two years may not be sufficient to assess the full impact of early treatment with interferon beta-1b for paediatric patients with MS and therefore additional long-term follow-up data would be helpful to guide physician decision making.
In conclusion, the two-year results from BETAPAEDIC suggest that interferon beta-1b is an effective treatment for paediatric patients with MS. In addition, interferon beta-1b has a favourable safety profile in paediatric patients that is similar to what is seen in adults who are taking this medication. This combination of safety and effectiveness findings and results from randomised clinical trials with interferon beta-1b in adults10–12 supports the use of interferon beta-1b in paediatric patients early in the disease.
Footnotes
Conflicts of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J Gärtner has received honoraria and consultancy fees from Bayer, Biogen, Teva and Novartis, and has received research grant support from Novartis and Biogen. W Brück has received honoraria for lectures from Bayer, Teva Pharma, Sanofi-Aventis, Genzyme, Novartis, Biogen, Roche and Merck-Serono, and is member of Advisory Boards for Teva, Genzyme, Novartis and Biogen. He has received research grants from Teva Pharma, Genzyme, Novartis and Biogen. A Weddige has received consultancy fees from Bayer AG. H Hummel has received honoraria from Bayer AG for a lecture. C Norenberg is a salaried employee of Bayer AG. JP Bugge is a salaried employee of Bayer AG.
Acknowledgements
The authors are grateful to the patients, their guardians and the BETAPAEDIC investigators for their continuing contributions to the study. Robert C Ristuccia of Precept Medical Communications provided editorial assistance that was funded by Bayer HealthCare Pharmaceuticals. Members of the BETAPAEDIC Study Group are: Austria: Eduard Auff (Allgemeines Krankenhaus der Stadt Wien), Michael M Benedikt (MS-Zentrum); Belgium: Souraya El Sankari (University Hospital St Luc); Finland: Tuula Lönnqvist (Helsinki University Hospital); Germany: Marc-Oliver Baur (Universitätsklinik Mannheim), Astrid Blaschek (Dr von Haunersches Kinderspital der Universität München), Jutta Gärtner (Georg-August-Universität Göttingen), Peter Hofstetter (Klinikum der Johann Wolfgang Goethe-Universität), Michael Karenfort (Universitätsklinikum Düsseldorf), Janbernd Kirschner (Universitätsklinikum Freiburg), Thomas Lücke (St Josef Universität, St Elisabeth Hospital GmbH), Hermine Schmidt (Caritas Krankenhaus Bad Mergentheim GmbH); Israel: Anat Achiron (Sheba Medical Center, Tel Hashomer); UK: Cheryl Hemingway (Great Ormond Street Hospital).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Bayer HealthCare Pharmaceuticals.
Supplementary material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.