
Abstract
Introduction
The Physiological Profile Assessment (PPA) is used in research and clinical practice for assessing fall risk. We compared PPA test performance between people with multiple sclerosis (MS) and healthy controls, determined the fall-risk profile for people with MS and developed a reference database for people with MS.
Methods
For this study, 416 ambulant people with MS (51.5 ± 12.0 years) and 352 controls (52.8 ± 12.2 years) underwent the PPA (tests of contrast sensitivity, proprioception, quadriceps strength, reaction time and sway) with composite fall-risk scores computed from these measures. MS participants were followed prospectively for falls for 3 months.
Results
The MS participants performed significantly worse than controls in each PPA test. The average composite fall-risk score was also significantly elevated, indicating a “marked” fall risk when compared with controls. In total, 155 MS participants (37.3%) reported 2 + falls in the follow-up period. Frequent fallers performed significantly worse than non-frequent fallers in the contrast sensitivity, reaction time and sway tests and had higher PPA composite scores.
Conclusions
In line with poor PPA test performances, falls incidence in people with MS was high. This study provides comprehensive reference data for the PPA measures for people with MS that could be used to inform future research and clinical practice.
Introduction
Falls are common among people with multiple sclerosis (MS) and knowledge about fall-risk factors in MS has increased significantly in the last decade. About 60% of people with MS will fall at least once and more than 30% will fall three or more times across a 3–12-month period.1–3 Identified risk factors associated with falls include advanced disease status,1,3,4 balance impairments,2,5,6 slow choice stepping reaction time, reduced walking speed, reduced executive functioning, 2 weakness in the lower limbs, 6 use of walking aids,6–8 fear of falling,9,10 forgetfulness, 9 bladder incontinence 9 and fatigue. 11
A number of tests have been used to estimate fall risk in this group. These have included clinical assessments such as the Berg Balance Scale (BBS) and the Timed Up and Go (TUG) Test 12 and laboratory-based tests such as posturography involving moving force-plates and visual surrounds. 13 There is some evidence that the clinical assessments can discriminate between people with MS who do and do not fall,14,15 but these tests have limitations in that they are restricted to measures of functional balance, and not broad-ranging physiological impairments. It has been shown the BBS has a ceiling effect in higher-functioning adults 16 and the predictive capacity of the TUG test is at best moderate in community-ambulant older people. 17 Other simple tools, such as the Physiological Profile Assessment (PPA) 18 may complement functional balance tests and have value in evaluating fall risk in people with MS.2,3
The PPA provides quantitative measures of key physiological risk factors for falls, including lower limb strength, sensation, balance during quiet standing, vision and hand reaction time. The PPA was designed to be low-tech, portable, simple and quick to administer and able to produce valid and reliable quantitative measures. 16 The PPA generates quantitative scores for each test domain as well as a summed, weighted total risk score. PPA component and fall-risk scores have been shown to have good predictive ability of falls in community-dwelling older people and clinical groups, including people with MS.2,3
The aims of this study were to (a) examine whether PPA component and composite test performance scores discriminate between frequent and non-frequent fallers in people with MS, (b) compare these scores of people with MS with data from age-matched healthy controls and (c) develop a reference database of PPA fall-risk scores for people with MS. These findings could help identify people with MS at increased risk of falling and be used to evaluate the effectiveness of fall prevention programmes aimed at improving physical performance outcomes.
Methods
Protocol approvals and participant consent
The data used in the current analysis were obtained from prospective cohort studies of fall risk in people with MS carried out in Australia (AUS), United Kingdom (UK) and the United States (US). These studies were approved by local ethics committees and written informed consent was obtained from all participants.
MS participants
Data from 416 people with MS were included in this analysis: 210 participants from AUS, 148 from the UK and 58 from the US. Common inclusion criteria for all samples were: (a) participants were diagnosed with MS using standardized criteria for MS diagnosis19,20 and (b) participants were aged 18 years and older, without restriction of any MS subtypes. Common exclusion criteria were inability to understand and sign an informed consent or being unable to follow test instructions.
Additional inclusion criteria for the Australian sample were ability to stand unsupported for 30 s and ability to walk 10 m with or without a mobility aid (i.e. Disease Steps 0–5, 19 Appendix 1). The UK participants were restricted to an Expanded Disability Status Scale (EDSS) score between 3.5 and 6.5, and full recovery from any recent relapse was required for inclusion. The US sample included participants with an EDSS score of 6.0 or less, an upper age limit of 50 years, being relapse free for 30 days prior to baseline examination, and ability to walk at least 100 m. EDSS was assessed either face-to-face by a trained clinician or by self-report using a telephone interview. 20 Disease severity was measured by the EDSS 21 in the samples from the UK and the US. In Australia the Disease Steps scale 19 was used and converted to EDSS by mobility criteria.
The Australian sample was recruited from an outpatient MS physiotherapy clinic in Sydney. Participants in the UK sample were recruited via invitation letters from their local neurologist and an advertisement in the newsletter of the South West Impact of MS (SWIMS) project, which is accessed by over 1500 people with MS living in the South West of England. 22 The US sample was recruited from patients receiving medical care at specialty MS centre outpatient clinics at a Department of Veterans Affairs medical centre and a university medical centre, and from the surrounding area, in the Northwest of the United States.
Demographic information including age, gender, number of years diagnosed with MS and type of MS was collected using a structured questionnaire. Trained therapists also assessed participants’ level of disability (EDSS scores 21 or Disease Steps 19 ).
Control participants without MS
Data for 352 age-matched healthy participants were randomly selected from the databases of research studies conducted at Neuroscience Research Australia23,24 and the University of Queensland.25–28 Participants for these studies were generally representative of the general population and were recruited via the electoral roll, health insurance databases and convenience sampling. Exclusion criteria were: having a neurological condition such as MS, Parkinson’s disease or stroke, a Mini-Mental State Examination (MMSE) score < 24 (indicating probable dementia) 29 and speaking no or very little English.
Physiological Profile Assessment
The PPA comprises five sensorimotor and balance measures: visual contrast sensitivity, proprioception, quadriceps muscle strength, hand reaction time, and postural sway.
Visual contrast sensitivity was assessed using the Melbourne Edge Test, which presents 20 circular patches containing edges with reducing contrast. Correct identification of the orientation of the edge on the patches provides a measure of contrast sensitivity in decibel units, where 1 dB = 10 log10 contrast. Proprioception was measured using a lower limb matching test, where difference (in degrees) in matching the great toes was recorded using a vertical clear acrylic sheet inscribed with a protractor placed between the legs. The proprioception test was administered as quickly as possible and rest periods were provided between trials to minimize fatigue influencing the test. Quadriceps muscle (isometric) strength in kilograms was examined in the more affected leg using a spring gauge while participants were seated with the hip and the knee joints at 90° of flexion. Hand reaction time in milliseconds was assessed using a light as a stimulus and a finger-depression of a switch as the response. Postural sway area (maximal anterior-posterior and medio-lateral sway in mm) was quantified using a sway meter that measured the displacement of the body at waist level while participants stood for 30 s on a foam rubber mat with their eyes open. This area measurement was subsequently converted to an estimate of sway path (a more precise measure and better discriminator of fall risk in both older people and people with MS2,18) using a regression equation from large population studies.
The five PPA components were weighted to compute a composite PPA fall-risk score expressed in standard (z-score) units. In studies of older people, PPA fall-risk index scores discriminate between multiple and non-multiple fallers with accuracies up to 75%, with scores of less than 0 indicating a low risk of falling, 0 to 1 indicating a mild risk, 1 to 2 indicating a moderate risk, and scores of 2 or more indicating a high risk of falling.
Falls definition and follow-up
In this study two fall definitions were used. For the sample from Australia a fall was defined as “unintentionally coming to the ground or other lower level and other than a consequence of sustaining a violent blow, loss of consciousness, sudden onset of paralysis as in stroke or epileptic or seizure”. 30 For samples from the UK and US a fall was defined as “a slip or trip in which participants came to rest on the ground or floor or lower level”. 31 Following the assessment, participants were asked to prospectively record any falls in the next 3 months using a diary system. 32 Participants received monthly falls diary sheets, written instructions and reply-paid return envelopes. A reminder telephone call or email was sent to participants whose diary returns fell behind schedule. 32 Previous studies of older people have found that recurrent falls are more likely to indicate physiological impairments and chronic conditions than single falls, and are therefore more clinically important. In line with previous studies, frequent fallers were defined as those who had ≥2 falls in the follow-up period. 3
Statistical analysis
Descriptive data for the PPA component tests and composite risk scores are presented. These include percentiles for those aged 20–39, 40–49, 50–59 and ≥60 years. The proprioception, quadriceps strength, reaction time and sway variables were positively skewed, and were log transformed to allow further parametric analyses. Pearson correlations were used for assessing PPA performance scores, age, and years since MS diagnosis. Group t-tests were used to compare the differences in these measures between men and women and between frequent fallers (two or more falls in 3 months) and non-frequent fallers (zero or one falls in 3 months). Finally, PPA performance scores were contrasted between the MS sample and age-matched healthy controls without MS using General Linear Models, adjusting for age and gender. Data were analysed with SPSS (version 22) for Windows (SPSS, Chicago, IL, USA).
Results
Demographic characteristics of the MS sample
Demographic characteristics of each sample from the three countries.

EDSS: Expanded Disability Status Scale; RRMS: Relapsing–Remitting Multiple Sclerosis; SPMS: Secondary Progressive Multiple Sclerosis; PPMS: Primary Progressive Multiple Sclerosis
Comparison with age-matched controls without MS
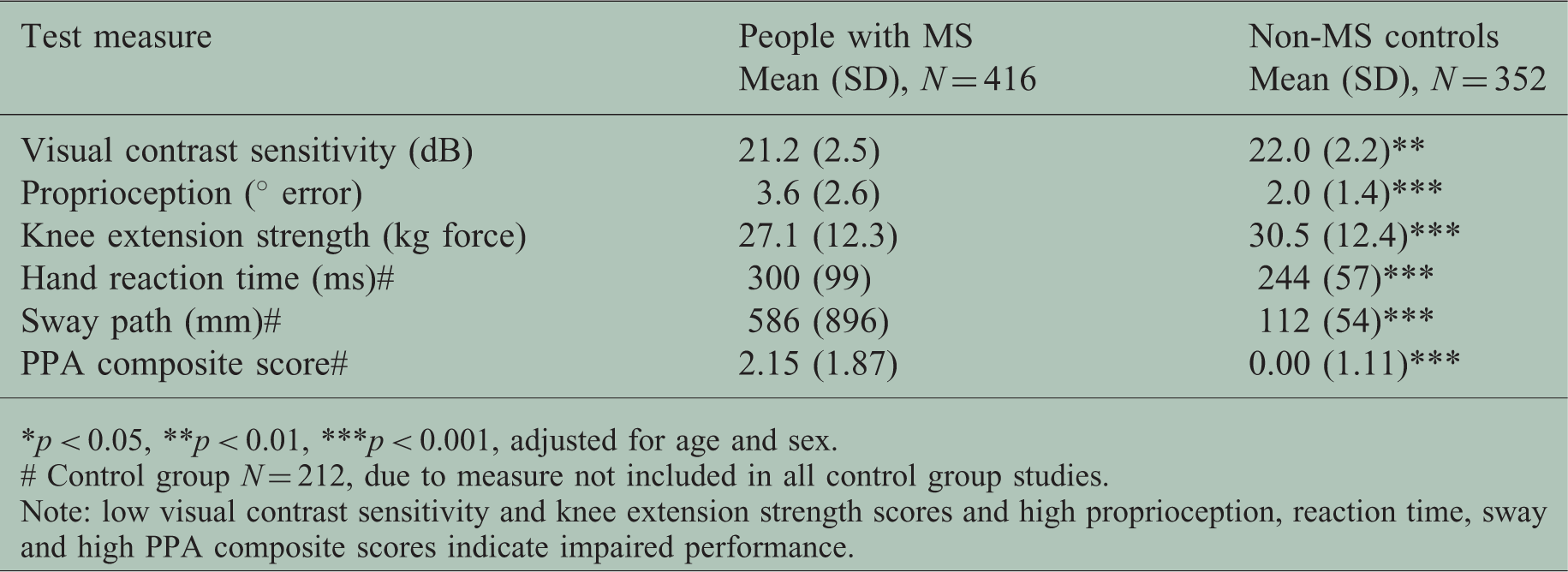
The age-matched control participants without MS sample (n = 352) comprised 274 women (77.8%) and 78 men (22.2%) with mean age 52.8 years (SD = 12.2, range = 21–84). There were non-significant trends for the MS sample to be younger (51.5 (SD = 12.0) years vs. 52.8 (SD = 12.2) years, t1,766 = 1.44, p = 0.150 and comprise fewer women (73.3% vs. 77.8%, χ2 = 2.10,df = 1, p = 0.15) than the control group. The participants with MS performed significantly worse than the control participants without MS in each of the PPA tests and had higher PPA composite scores, after adjusting for age and gender in general linear model analyses (Table 2). Figure 1 shows mean PPA composite scores for the age-bands presented in the MS PPA reference database in relation to composite score norms for healthy control participants without MS.25–28
Relationship between the risk of falls in people with MS derived from the PPA and age. PPA test and composite scores: MS–control group comparisons. p < 0.05, **p < 0.01, ***p < 0.001, adjusted for age and sex. # Control group N = 212, due to measure not included in all control group studies. Note: low visual contrast sensitivity and knee extension strength scores and high proprioception, reaction time, sway and high PPA composite scores indicate impaired performance.
PPA reference values for people with MS
Reference values (percentiles) for PPA component and composite fall-risk scores for the MS sample.

Note: low visual contrast sensitivity and knee extension strength scores and high proprioception, reaction time, sway and PPA composite scores indicate impaired performance.
Correlations between physiological and functional tests and duration of MS disease and age.

Note: low visual contrast sensitivity and knee extension strength scores and high proprioception, reaction time, sway and PPA composite scores indicate impaired performance.
p < 0.01, ***p < 0.001
PPA test scores in relation to MS subtypes and disease severity
PPA test and composite scores: MS sub-group comparisons.
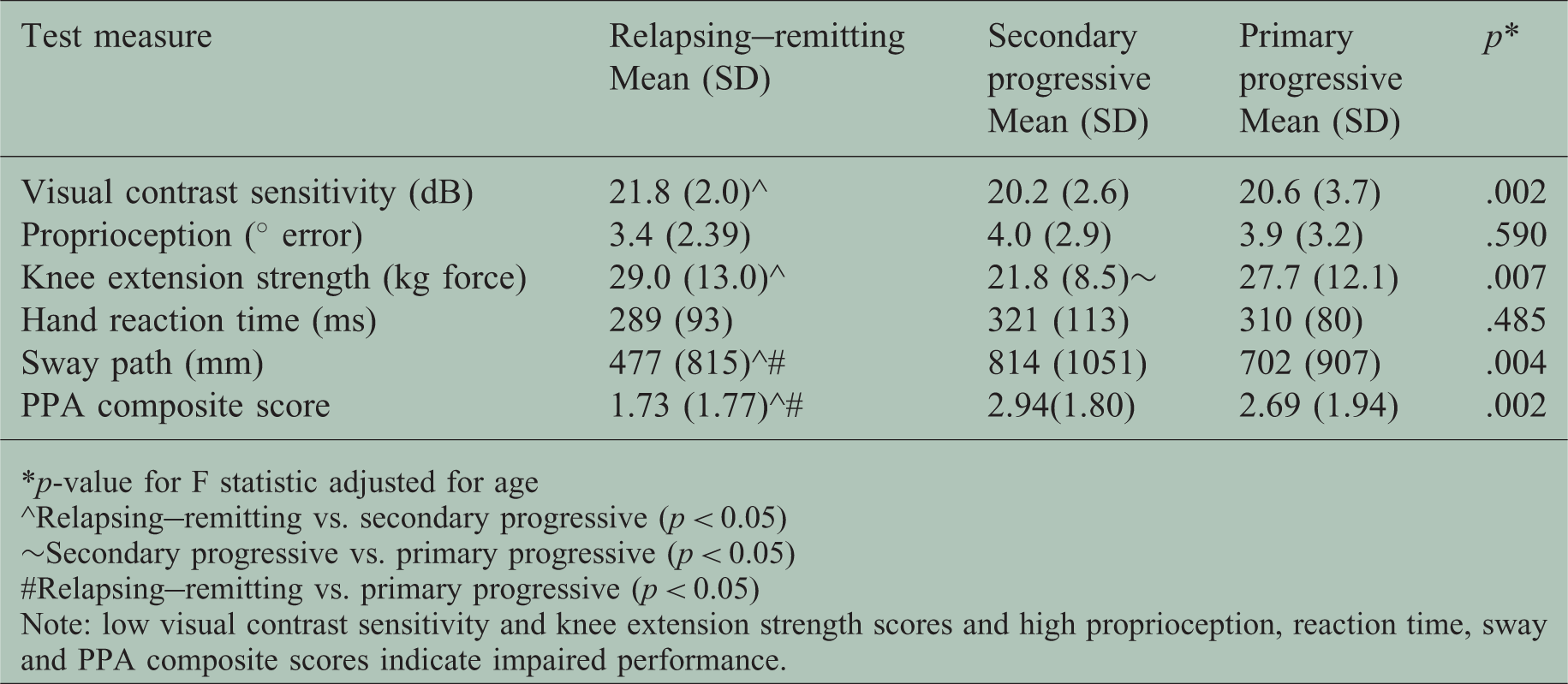
p-value for F statistic adjusted for age
^Relapsing–remitting vs. secondary progressive (p < 0.05)
∼Secondary progressive vs. primary progressive (p < 0.05)
#Relapsing–remitting vs. primary progressive (p < 0.05)
Note: low visual contrast sensitivity and knee extension strength scores and high proprioception, reaction time, sway and PPA composite scores indicate impaired performance.
Figure 2 shows the relationship between PPA composite scores and EDSS categories. The Pearson correlation coefficient for this association was 0.478 (p < 0.001), and this was only slightly attenuated when adjusting for age in a partial correlation analysis; r = 0.405, (p < 0.001). PPA and EDSS scores did not differ significantly by gender (p = 0.103 and p = 0.792, respectively).
Relationship between PPA composite scores and EDSS categories.
Prospective falls
PPA test and composite scores: faller group comparisons # .

# Number of falls participants suffered in the 3-month follow-up.
Group t-tests comparing test scores for non-frequent (0, 1) and frequent (2+) fallers; *p < 0.05, ***p < 0.001.
Note: low visual contrast sensitivity and knee extension strength scores and high proprioception, reaction time, sway and PPA composite scores indicate impaired performance.
Discussion
Our study compared fall-risk scores of people with MS with those of a healthy control population and examined whether PPA component and composite test performance scores discriminated between frequent and non-frequent fallers in this population. We found that the MS sample performed significantly worse than the age-matched control participants without MS in all PPA tests. Overall, 62% of the MS sample had PPA scores of one or higher (moderate fall risk) and 47% had PPA scores of two or higher (high fall risk). This indicates that most people with MS are at an increased fall risk when compared with normative data, and as shown in Figure 1, fall risk is significantly elevated across the adult lifespan.
Fall risk was also evident by the high fall rate reported, with over 50% of the cohort reporting one or more falls and over 37% reporting two or more falls in the 3-month follow-up. Frequent fallers performed significantly worse than the non-frequent fallers in three of the five component tests: visual contrast sensitivity, hand reaction time and postural sway, and had higher PPA composite scores. In contrast, there were only trends for the MS sample to have reduced lower limb proprioception and knee extension strength. This suggests these measures may be less important for fall risk in people with MS compared with older people – the population group in which the PPA was developed. For knee extension strength, in particular, it appears that performance may be adequate in both frequent and non-frequent fallers in people with MS.
PPA composite scores were significantly associated with EDSS scores when adjusting for age, and differing fall-risk profiles for people with different MS subtypes. The relapsing–remitting group performed best in all PPA tests, and significant between-group differences were evident for the visual contrast sensitivity, knee extension strength and postural sway tests and PPA composite scores. Noticeably, the secondary progressive group had significantly poorer knee extension strength than both the relapsing–remitting and primary progressive groups and may be a distinguishing risk factor for this group.
Strengths of this analysis include the rigorous prospective falls surveillance and the recruitment of a large sample drawn from three countries with EDSS scores ranging from 1 to 6.5, covering ambulatory people with few symptoms to those with major balance and gait impairments. We also acknowledge that while the physiological tests were able to distinguish frequent fallers from non-frequent fallers, the area under the receiver-operator characteristic score for the composite PPA–frequent faller association was only moderate, and there are undoubtedly other general and disease-specific measures such as strength of other muscle groups, fine motor control, spasticity, fatigue and dynamic balance steps (such as voluntary and reactive stepping) that may have provided additional insight into the fall-risk profile in people with MS. Further research could provide additional reference data to add to the current fall-risk profile. Second, due to the differing methods of recruitment within both the MS and healthy control groups, it is not possible for us to present data on response rates. Third, while no participants were unable to complete the lower limb proprioception test due to not being fully able to extend either leg due to weakness or fatigue, it is acknowledged that as this test involved movements against gravity, test results may have been affected by reduced muscle strength in some participants. Finally, the data presented for sway path are indirect as they were estimated from a regression equation from measured maximal anterior-posterior and lateral sway measurements from the sway meter. This more robust measure was included in the reference database as it can now be measured simply with a mobile application (www.neura.edu.au/apps/ppaswaypath) as used in a recent randomized controlled trial. 26
Clinical implications and conclusions
This study illustrates the value of a physiological profiling approach to identifying sensory and motor impairments and documenting overall reduced physiological performance in people with MS. 25 The compiled reference database for the PPA component and composite scores should assist future studies using the PPA in evaluating balance performance and evaluating effectiveness of interventions in people with MS. Further, as the PPA comprises simple “low-tech” tests it has scope for widespread use in clinical settings.
Footnotes
Funding
Phu Hoang was funded by Multiple Sclerosis Research Australia; Stephen Lord were funded by National Health and Medical Research Council (NHMRC) Australia. Michelle Cameron was funded by the US Department of Veterans Affairs Rehabilitation Research & Development Service. Hilary Gunn and Jenny Freeman were funded by a grant from the Physiotherapy Research Foundation (Chartered Society of Physiotherapy, UK).
Conflict of interests
Stephen lord declares the Physiological Profile Assessment (NeuRA FallScreen) is commercially available through Neuroscience Research Australia.