
Abstract
Objective
Dental neglect, oral health values, Oral Health-Related Quality of Life (OHRQoL), and HbA1c levels are interconnected factors that significantly impact the overall health and well-being of individuals with diabetes. The aim of this study was to evaluate the health nursing guidance based on phone applications of oral hygiene and glycemic control on health-related outcomes among diabetic patients.
Methods
A quasi-experimental research design was used. A purposive sample of 76 adult diabetic patients was divided into a study group (n = 38) and a control group (n = 38). Data collection for the study sample was conducted in the medical clinic of the university hospital (MU) and Shebin El Kom Teaching Hospital. The total study period was 6 months, from September 2023 to March 2024, while the follow-up period lasted 12 weeks.
Results
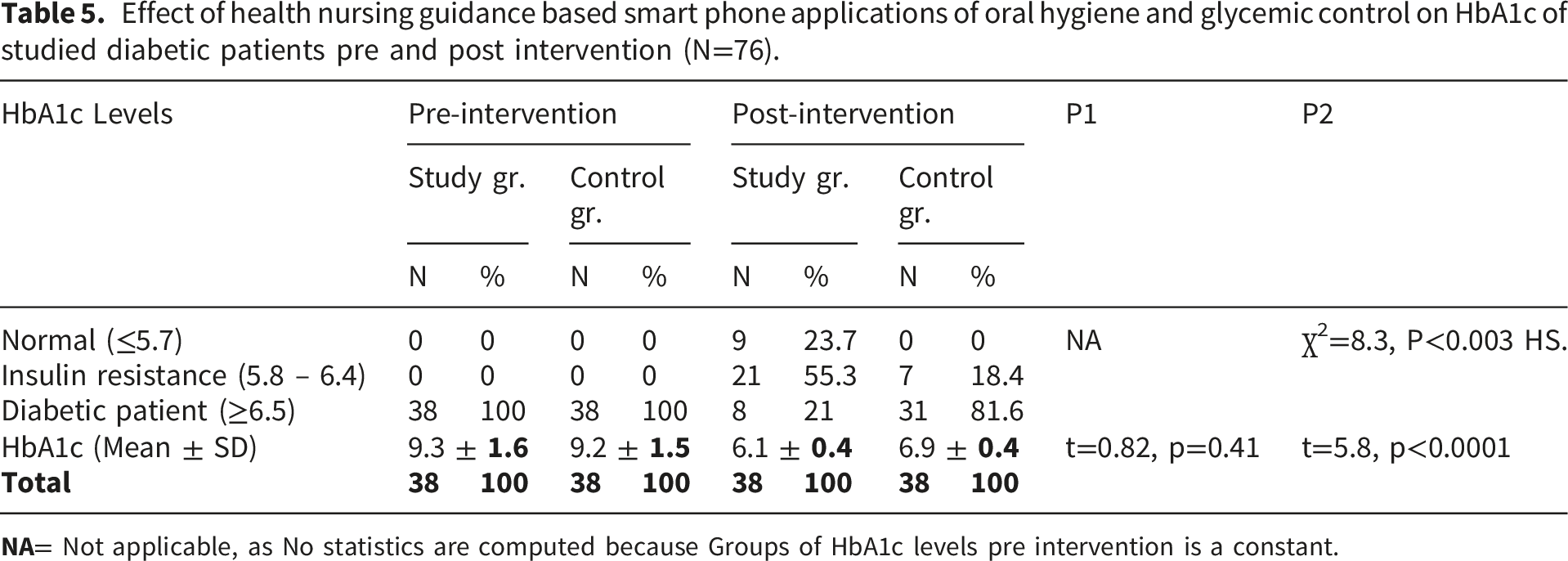
Approximately 45% of study group patients were aged 30-39 years (42.1%), with a mean age of 38.8 ± 11.9 years (range, 18-59 years). After the intervention, there was an incredibly apparent enhancement with p< .0001 in all study diabetic outcome items except total Oral Health Value with p< .01. After smartphone application intervention, there was an incredibly apparent enhancement with p< .0001 in all study diabetic outcome items except total Oral Health Value with p< .01 including total oral hygienic behaviors, Dental Neglect scale, total OH-QoL scale, total Oral Health Value scale, Glycated Hemoglobin (HbA1C). Among the study groups, the mean HbA1c score post-intervention decreased from 9.3 ± 1.6 (pre-intervention) to 6.1 ± 0.4, while in the control group, it decreased from 9.2 ± 1.5 (pre-intervention) to 6.9 ± 0.5 post-intervention.
Conclusion
The study concluded that mobile health applications (mHealth) for oral hygiene and diabetic control instructions have a significant, positive effect on improving Oral Health Values and Oral Health-Related Quality of Life in the study group compared to the control group. There was a decrease in the Dental Neglect score and HbA1c levels among the intervention group compared to the control group.
Keywords
Introduction
Smartphone applications in health offer a wide array of tools and functionalities to support various aspects of healthcare and wellness management. These tools range from simple fitness trackers and medication reminders to more complex applications for managing chronic diseases and remote patient monitoring. 1 In recent years, smartphone applications in healthcare have been used for patient motivation and education on oral health. 2 Various applications and text-messaging services make it easier to motivate patients to maintain their oral care. Furthermore, social media platforms, in addition to smartphone applications, are also encouraging patients to maintain better oral health. 3 These applications are designed for use during downtime and offer benefits to patients who can utilize their sense of control to maintain better oral health. 4 Several smartphone apps can remind patients to take care of their teeth by sending those messages. 5
Diabetes ranks among the most prevalent chronic conditions; it is a progressive disease that affects an increasing number of people. Approximately 422 million individuals around the globe are living with diabetes. 6 The number of diabetes cases and the rate of prevalence have been consistently on the rise in recent decades. Expectations indicate that the number of people affected by the disease around the world is approximately 700 million, in addition to the disease causing more than 4 million deaths annually, resulting from complications. The number of people with the disease in the Middle East and Africa region has reached approximately 73 million. Diabetes mellitus (DM) is widely regarded as a contemporary epidemic worldwide and is a significant public health concern in Egypt.7,8
Oral health issues include dental caries, xerostomia, periodontal disease, sensory impairments, taste abnormalities, dysfunctional salivary glands, and oral infections, which are highly prevalent in people with diabetes. Periodontal disease, a most common chronic inflammatory condition, is characterized by the deterioration of the connective tissue encircling teeth, leading to eventual tooth loss. Into the bargain, a periodontal infection may make a person more susceptible to DM problems. 9 Various oral issues can be observed in both types of diabetes mellitus (DM), including dental implant problems, lichen planus, geographic tongue, periodontal diseases, oral candidiasis, tooth loss, xerostomia, halitosis, delayed wound healing, burning mouth syndrome, salivary and taste dysfunction, and tooth decay. 10 The extent of periodontal tissue deterioration is influenced by how well diabetes is managed and how long it has been controlled, which affects the frequency and occurrence of periodontal disease according to Iwasaki et al. (2019). 11
Compared to people without diabetes, Patients with diabetes have a greater likelihood of experiencing Dental caries. The buildup of microbial plaque flora and demineralization leads to dental caries. In addition to lowering calcium levels that encourage tooth decay, decreasing salivary flow in diabetic individuals impairs cleansing and buffer capacity and lowers resistance to germs that cause cavities.12,13 Additionally, saliva from people with diabetes has elevated glucose levels, which raises the quantity of carbohydrates that oral bacteria can ferment. DM II patients have a higher prevalence of dental caries than non-diabetic people. However, most research on DM I patients offers the majority of the information currently available regarding the relationship between DM and caries. 11
Diabetes primarily affects the abnormalities in saliva secretion, as well as periodontal disease and gingival disease. Variable oral and dental consequences, such as xerostomia and periodontal disease, are associated with diabetes mellitus. Consequently, oral health-related quality of life (OHRQoL) and oral status can be affected by diabetes, as noted by the International Diabetes Federation. 14 Diabetes has been linked to a variety of oral and dental health complications, including gum disease, dental caries, periodontal abscesses, periodontitis, xerostomia, vesiculobullous lesions, oral fungal infections, a higher risk of post-operative infections, and poor wound healing. These complications can have a significant impact on quality of life. 15
It was discovered that oral symptoms were present in almost 90% of diabetic individuals. It is well recognized that diabetes mellitus (DM) causes substantial damage to oral tissues, leading to a variety of conditions, including caries, xerostomia, periodontal disease, delayed wound healing, lichen planus, geographic tongue, and candidiasis. Regretfully, a low proportion of diabetic patients attend the dentist for regular dental checkups, and many are ignorant of the link between diabetes mellitus and oral health. 16
Significance of the study
Smartphones in healthcare applications have impacted the way nursing education and practice are conducted. Nurses are moving toward empowering their patients by utilizing mHealth applications to enhance patients’ health and support them in making healthy lifestyle adjustments, including those related to oral health. By increasing their patients’ awareness and usability, these apps may support proactive and evidence-based healthcare. Integrating mobile technology into nursing education and practice continues to face various challenges and obstacles that hinder its optimal infusion into the field of nursing. With continued research focusing on this topic, numerous opportunities lie ahead that can be leveraged to enhance the conditions of mobile technology and mHealth applications for patients, health educators, and practitioners.
Additionally, it is believed that mobile learning, particularly using smartphones, is a suitable application for nursing education. A smartphone’s high degree of portability and accessibility enables the promotion of active learning and self-regulation. 17 A study conducted by Kim et al. (2019) aimed to determine the benefits of these technologies in maintaining health and preventing further complications. 18
Oral health issues associated with diabetes mellitus can be effectively prevented by modifying lifestyle habits (including blood glucose control and self-care practices), scheduling routine dental checkups with a focus on periodontal examination, and reinforcing oral health guidance. Patients with diabetes can improve their glycemic control with scaling and accurate planning. 19
Recent research on the use of smartphone technology for diabetes self-management has shown that these devices can effectively regulate hemoglobin A1c (HbA1c) levels, particularly in individuals with type 2 diabetes (T2D). 16 Besides the cost of direct medical care, healthcare facilities, and hospitals, its complications also burden care and increase costs related to its oral manifestations and complications. Egypt is one of the top 10 countries in the world for the number of DM patients. According to estimates from the International Diabetes Federation (IDF), there are around 2.2 million pre-diabetics and 7.5 million diabetics in Egypt. 19
Study hypotheses
H1: Diabetic patients who receive health nursing guidance on oral hygiene and glycemic control will improve all hygiene behaviors and Oral Health Related Quality of Life scores post-intervention. Diabetic patients who receive health nursing guidance on hygiene and glycemic control will experience a decrease in Dental Neglect and Oral Health Values scores, as well as a decrease in Glycated Hemoglobin Level (HbA1c) post-intervention.
Methods
Research design
A quasi-experimental research design (pre-post/study-control group) was undertaken.
Study setting
The current study was conducted at the diabetic outpatient clinics of Menoufia University Hospital and Shebin El Kom Teaching Hospital, Egypt.
Subjects
A purposive sample of 76 diabetic adult patients was involved in the existing study according to the inclusion criteria. The total sample was classified into two equal groups (n = 38) for the control group and (n = 38) for the study group. They were assigned to each group according to their level of education and Glycated Hemoglobin Level (HbA1c), based on the following sample calculation formula.
Sample size
To calculate the sample size required to assess the Impact of evaluate health nursing guidance based smart phone applications of oral hygiene and glycemic control on among diabetic patients on medical data (teeth problems), oral hygienic behavior, dietary habits, Dental Neglect scale, and Oral Health-Related Quality of Life among studied diabetic patients, this study used Epi website (Open-Source Statistics for Public Health) *, with the following sample size equation: 1. Considering an α-type I error of 0.05, 2. β type II error of 0.20, 3. a test power of 0.8, 4. m = n1 = size of sample from population 1, 5. and d = 2 as the least significant difference, 6. z1 standard normal deviate for a two-tailed test based on alpha level (relates to the confidence interval level), 7. p percent of unexposed (control) with outcome (improvement in oral hygiene behavior, and dietary habits among the study group of diabetic patients).
20

Inclusion criteria
➢ Patients aged 18 years or older. ➢ Patients who have been diagnosed with Type II diabetes. ➢ Patients who have smartphones running either iOS or Android. ➢ Patients receiving diabetes care in outpatient facilities. ➢ Patients who agree to participate in the study will provide written informed consent.
Exclusion criteria
➢ Patients with uncontrolled diabetes who lack medical follow-up. ➢ Patients with any complications that arise due to diabetes mellitus may lead to Hospitalization ➢ Patients who have severe tooth decay/fractures, defects in the mastication process, and defects in the appearance. ➢ Smoking patients ➢ Patients suffering from hypertension with certain calcium channel blockers could experience enhanced gingival hyperplasia. ➢ Patients who are undergoing any kind of orthodontic treatment ➢ Patients who underwent the periodontal treatment protocol.
Study instruments
Instrument 1: A structured interviewing questionnaire
It was created by the researchers after reviewing the literature4,7–10 and included the following three parts.
Part one: Demographic data
It included questions to assess patients’ age, gender, job, marital status, level of education, and income.
Part two: Medical profile
It included questions to assess the current disease condition and the past medical history of diabetes and oral health problems.
Part three: Oral hygiene behaviors questionnaire
It included questions to assess current oral hygiene behaviors and practices, such as regular tooth brushing, interdental cleaning, water mouth rinsing, duration of brushing, and type of toothpaste, after reviewing the related literature.10,21 It was developed and modified by the researcher to be suitable for Egyptian culture. It included six items with two alternatives (yes/no) to assess oral hygiene behaviors in patients with diabetes. Each correct response was given a score of one, while an incorrect response was given a score of zero. The total score of the questionnaire ranges from 0 to 6.
Instrument II: Oral health values scale (Edwards and Cierra, 2017) 22
It is a 30-item 5-point Likert scale designed to measure the degree to which one demonstrates investment in improving or maintaining oral health. Response options range from “strongly disagree” to “agree strongly.” Scale items that are reverse-scored. Professional Dental Care factor/subscale: Items 4, 8, 11; Appearance and Health factor/subscale: Items 3, 7, 12; Flossing factor/subscale: Items 2, 5, 10; Retaining Natural Teeth factor/subscale: Items 1, 6, 9. The patient’s perception of the importance of oral health and various dental-related situations is assessed. Higher scores on the oral health values indicate lower oral health problems.
Instrument III: Dental Neglect Scale (DNS) (Johnson et al., 2009) 23
The questionnaire included a 6-question Likert-type scale that measures oral hygiene behaviors and attitudes likely to have detrimental consequences for the individual’s oral health. Respondents rate each of the statements on the DNS on a 5-point Likert scale, from 1 (definitely no) to 5 (definitely yes). Lower scores on the DNS indicate a greater oral health condition. The DNS exhibits acceptable internal consistency, α = 0.74, and test-retest reliability, r = 0.81, indicating that the scale is a reliable measure of dental neglect.
Instrument IV: The Oral Health Quality of Life Inventory (OH-QoL) (Bettie et al., 2015) 24
The Oral Health Quality of Life Inventory (OH-QoL) was developed by Bettie et al. (2015) to evaluate the Impact of oral health and functional status on quality of life. This 15-item dental-specific test evaluates an individual’s level of satisfaction with their oral health and functional status, as well as the significance and characteristics of these areas. The purpose of OH-QoL is to assess an individual’s subjective well-being about their oral health and functional status. The higher scores indicate higher levels of oral health quality of life.
Scoring the OH-QoL
OH-QoL items are rated on two dimensions: Importance and Satisfaction. Before scoring, the OH-QoL importance responses are recoded as 0 = not at all important, 1 = somewhat important, and 2 = very important. Satisfaction responses are recoded as -2 = unhappy, -1 = somewhat unhappy, +1 = somewhat happy, and +2 = happy. An OH-QoL score for a given item is the product of importance x satisfaction. The overall OH-QoL score is the mean value of the answered OH-QoL items, thus yielding an almost interval-level measure that ranges from -4 to +4. One OH-QoL item is only asked of denture wearers. No overall OH-QoL score is computed if two or more of the relevant items are assigned missing values.
Instrument V: Physiological measurement of HbA1c level
The capacity to reflect the cumulative glycemic history of the past two to three months, as measured by HbA1c, is a significant indicator of long-term glycemic management. Hemoglobin A1c is a good indicator of chronic hyperglycemia and has a strong correlation with the risk of complications from long-term diabetes. An A1C level of 6.5% or greater indicates diabetes mellitus. Normal level of A1C is up to 5.7% (American Diabetes Association, 2019) 25
Pilot study
Prior to beginning data collection, pilot research was conducted on 10% of patients (n = 8) who met the study’s eligibility requirements to evaluate the study’s clarity, applicability, and feasibility, as well as the time required to complete the instruments. The pilot study’s findings led to the necessary adjustments being made. The full study population did not include the participants in the pilot research.
Validity and reliability of the data collection instrument
The data collection instruments were examined for content validity by a panel of five experts in family and community health nursing, as well as medical-surgical health nursing, and their recommendations were implemented. By administering the same tool to the same participant twice within a two-week period and comparing the findings, the reliability of the tool was tested to determine how closely the questionnaire’s items were related to one another and to assess the comparability of the results. The Cronbach’s α test reached 80% (r = .86) for the Oral Hygienic Behaviors Questionnaire, 80.6% for the Oral Health Values Scale, and 78% for the Dental Neglect Scale (DNS), 81% for the Oral Health Quality of life Inventory (OH-QoL) and 83% for Physiological measurement of HbAIc level was measured. Based on the test-retest questionnaire used in the study, the data collection method was reliable.
Ethical approval
The Faculty of Nursing’s Ethical Committee in Menoufia University approved the conduct of the research with reference number: (961).
Prior to data collection, all participants vided oral agreement, they were informed that there were no hazards to their health, and that data would be kept confidential and anonymous. Ethical considerations included describing the study’s goal, assuring voluntary participation, and allowing participants to quit at any moment.
All data of the patients studied was maintained confidentially and used only for the purpose of the study. Measures were taken to promote transparency, respect for participant rights, and research integrity.
Data collection procedure
The total study period was 6 months, from September 01, 2023, to March 31, 2024, while the follow-up period lasted 12 weeks. The studied sample was selected according to the research inclusion criteria, and oral informed consent was obtained from each patient. A total of 76 type II diabetic patients were assigned to two equal groups, with 38 patients in each. The study (I) and control (II) groups were divided according to the level of their education and Glycated Hemoglobin Level (HbA1c). The use of smartphone apps prevents direct contact and communication between the study group and control group to control the confounding variables in the current study.
The assignment groups to study or control were not announced along with the study period to achieve the single blindness technique.
The researchers assumed to follow the control group by phone calling for management items during the intervention period, including diet, medication regimen, physical activity, and stress management, to maintain adherence to the scheduled routine care.
The patients’ HbA1c level was assessed at the first interview as baseline data and after 3 months for both the study and control groups. Each patient was interviewed individually.
Intervention components
Smartphone applications used in the current study
The applications used were Text2Floss and Healthy Teeth – Tooth Brushing Reminder, which included a timer. Regarding Text2Floss, it sends patient text message reminders encouraging healthy oral habits. As the patient responds to text messages, they can track and view their oral healthcare progress using the My Text2Floss Flossing Report, a valuable tool for improving the health of their teeth and gums between dental visits. He can also receive notifications about important dental-related issues, such as reminders to take premedication prior to a dental appointment and ways to reduce stress. Healthy Teeth – Tooth Brushing Reminder with Timer serves as a daily reminder to brush teeth twice. The application reminded the user through notifications to brush their teeth. In addition, the application features a separate menu with a graphics interchange format (GIF) image to illustrate the correct brushing method. Also, the app notifies users when it is time to change their brush.
Monitoring and follow-up
For three months, the researcher asked the patients to join an instructional WhatsApp group. The study group was divided into two subgroups, each comprising 19 patients, to maximize the effectiveness of the educational group. The subgroups were instructed to pay attention to oral health educational messages and recommended oral health self-care activities that were uploaded to the group. In addition, diabetic control guidelines and nursing guidance encompass a balanced diet, regular physical activity, blood glucose self-monitoring, adherence to medication recommendations, foot care, stress management, and promoting sound sleep quality. Following these guidelines can help achieve an ideal A1c level. The patients made routine trips to the clinic every three months to discuss the results of their HbA1c test with their doctor.
Using a pictorial leaflet, a model demonstration, and a brief film, information, notifications, and instructions regarding all diabetes self-care activities were progressively uploaded to the group every week for three months. WhatsApp includes a function that allows researchers to verify that every patient in the study group has read the material, so they were examined to confirm this. If the patient fails to receive the messages, they will be removed from the research. Techniques for question-and-response and group discussions were employed.
Post-intervention data collection
After three months, the researcher contacted the patients and obtained the completed questionnaire from them over the phone. The most recent HbA1c levels of patients, Oral Health Values, Dental Neglect, and oral health-related quality of life (OHRQoL) were reassessed using the predetermined instruments.
Statistical analysis
Version 22 of the SPSS (Statistical Package for the Social Sciences) statistics package was used to enter and analyze the data. Graphics were created with the Excel software. The standard deviation (SD) and mean (X) values were used to report continuous data (with independent sample t testing to compare group differences) and numbers, frequency, and percentage values for categorical data (with chi-square and Fisher’s exact probability tests to determine intervariable relationships). Pretest-posttest differences were determined using paired-sample t-tests, indicating changes in binary categorical variables following the intervention. The application of these statistical analysis methods affirmed the reliability of cross-comparison results and mitigated the risks of erroneously rejecting null hypotheses, as presented in the following section. After adjustments, a P value of ≤.05 was assumed to indicate statistical significance.
Regarding assessing the HbA1c Levels in this study, the total score of each participant was categorized as “Normal” if he achieved ≤ 5.7, “Insulin resistant” if he achieved (5.8 -6.4), and “Diabetic patient” if he achieved ≥ 6.5.22–25
Results
Socio-demographic characteristics of studied diabetic patients distributed by study and control groups (no = 76).

Number and percent distribution of oral health problems of studied diabetic patients pre intervention (no=76).

Effect of health nursing guidance based smart phone applications of oral hygiene and glycemic control on oral hygienic behaviors of studied diabetic patients pre and post intervention (no=76).
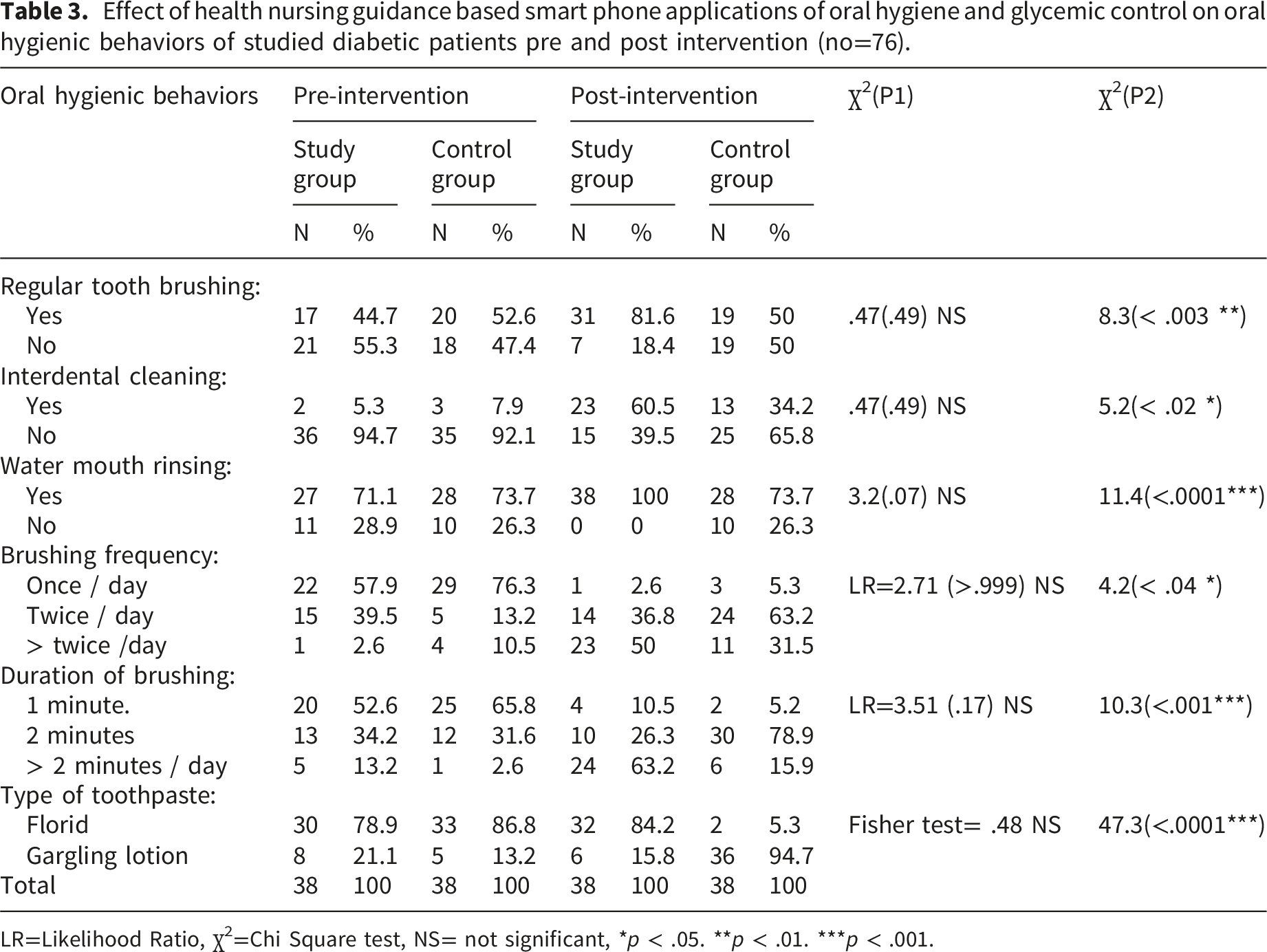
LR=Likelihood Ratio, ꭓ2=Chi Square test, NS= not significant, *p < .05. **p < .01. ***p < .001.
Effect of health nursing guidance based smart phone applications of oral Hygiene and glycemic control on Diabetic outcomes among studied diabetic patients pre and post intervention (no=76).

NB: Diabetic outcomes include Dietary habits, dental neglect scale, Oral Health problems, Oral hygienic behavior and oral health Quality of Life, oral Health value scale and (HbA1C.
SD= Standard deviation, t test = Paired t test, **p < .01***p < .001.
p1=Comparison between study and control groups before intervention. p2= Comparison between study and control groups after intervention.
Effect of health nursing guidance based smart phone applications of oral hygiene and glycemic control on HbA1c of studied diabetic patients pre and post intervention (N=76).
Discussion
One systemic disease that has a significant oral presentation and affects oral health is diabetes mellitus. These days, smartphones are widely employed in all facets of life, including the health sciences. Smartphone apps have become a standard auxiliary tool for oral health education and incentives in dentistry over the past few years. Patient motivation to continue dental care is easier when various software and text messaging services are used. 26
Regarding patients’ demographic characteristics, the results of the current study showed that about two-fifths of study group patients were aged 30 - 39 years, with a mean age of (38.8 ± 11.9), while two-thirds of them were female and married. This result was in the same line with Dakroub et al., (2023) in Lebanon 27 whose study entitled “The socio-demographic and lifestyle characteristics associated with quality of life among diabetic patients in Lebanon: a cross-sectional study” who revealed that the median age of the sample was 35 years ranging from 30-40 years, about half of them were females and nearly two third of them were married. This may be interpreted as the disease usually strikes young adults.
In relation to the level of education, job, and income. Half of the study group held a bachelor’s degree, and approximately two-fifths of them were employed, while the majority reported having a sufficient income. The study is congruent with Kyrou et al. (2020) in Europe, 28 whose study about “Sociodemographic and lifestyle-related risk factors for identifying vulnerable groups for type 2 diabetes: a narrative review with emphasis on data from Europe.” They revealed that three-fifths of them were employed, so two-fifths of them had adequate monthly income and had a university education. This may be interpreted as diabetes mellitus does not interrupt their life process.
Regarding the oral health problems of the studied diabetic patients prior to intervention. The current study revealed that a higher percentage of them complained of effects on taste and smell, healing of mouth wounds, tooth pain, and Gum tissue damage. They represent 97.4%, 50%, 47.4%, and 42.1%, respectively, in the study group, compared to 73.7%, 42.1%, 55.3%, and 26.3%, respectively, in the control group. This result was supported by Alqadi (2023), who reported an association between diabetes and pathologic changes in the oral cavity. 29 Moreover, there was evidence that oral health problems are related to metabolic control and complications of diabetes. 30 Several studies have shown that poor oral wound healing, taste dysfunction, some oral mucosa alterations such as coated and fissured tongue, and recurrent aphthous stomatitis can be associated with diabetes.30–32 These abnormalities are mainly attributed to the endocrine, metabolic, and/or vascular changes occurring with diabetes, alteration of oral microbial flora, and abnormal defense mechanisms.33,34 Additionally, one result aligned with the previous findings conducted by Haghdoost et al. (2023), who reported that following the educational interventions, the mean score for oral health concerns declined in all three groups (P < .001), with the social media group experiencing the most significant decline. 35 These findings suggest that effective dental hygiene practices and diabetic control guidelines can help prevent oral health issues.
Regarding the Impact of health nursing guidance based on smartphone applications for oral hygiene and glycemic control on the oral hygiene behaviors of studied diabetic patients before and after intervention. After the intervention, there was a significant enhancement (with a range of p < .01 to p < .0001) in all oral hygiene behavior items. The study’s findings corroborated those of Haghdoost et al. (2023), who found that the physician-aid group exhibited the most significant behavioral change (P < .001) and increased their frequency of brushing their teeth twice a day or more following the intervention. 35 Following the intervention of Haghdoost et al., (2023), all three groups experienced an increase in the frequency of flossing their teeth at least once a day (P < .01). (The smart application group) showed the most significant improvement in flossing their teeth at least once a day (P < .01). This may be due to that these applications increase dental knowledge and awareness so studied patients might have a motive to practice better oral care regimens. Al-ak’hali et al. 20 found that using a sophisticated smartphone application resulted in a significant difference in oral hygiene behavior scores compared to those who received traditional teaching, which aligns with the current results in the same theme. 26
However, this finding contradicted with of Alasmari et al., (2022), who claimed that periodontal health improved over time regardless of the methods used for oral hygiene instructions, and that smartphone applications for oral health failed to demonstrate any superiority in this regard over the traditional oral health instructions method in the present study as well. 4 This discrepancy in the results may be attributed to the lack of continuity in follow-up and communication.
The current intervention program revealed a probable improvement in the dental neglect score. The mean score improved from 18.8 ± 3.5 to 15.9 ± 4.1 after the intervention (P < .003). These findings were consistent with those of Bhattarai et al. (2020), who reported a mean DNS score of 18.40 and a statistically significant difference (P = .033) between the participants’ ages and the mean DNS score. 36 The study also verified that dental caries and oral hygiene status were strongly correlated with dental neglect, which was found to be common among adult residents of Kathmandu.
Despite the current study revealing a statistically significant difference (p < .003), after a three-month intervention, a slight improvement was noticed in the mean score of HbA1c post-intervention (it decreased from 9.3 ± 1.6 to 6.1 ± 0.4). These results were in line with those of Toda et al. (2019), who demonstrated that oral health instructions improved glycated hemoglobin (HbA1c) levels and significantly lowered the mean HbA1c levels. 37 Also, this result was similar to Jadhav et al. (2016), who reported a significant decrease in” Glycated Hemoglobin Level (HbA1c) after six months in the test group compared to the control group. 38 These results indicate that the use of innovative applications of oral hygiene and diabetic control instructions has a positive effect on decreasing Glycated Hemoglobin Level (HbA1c).
Likewise, this highlighted the possibility that increased dental cleanliness could have a greater impact on glycemic control. These outcomes were also proportionate with those of Haghdoost et al. (2023), who reported that in all three groups, the mean level of the most recent HbA1c decreased following the intervention in comparison to the baseline. 35 However, statistically speaking, this decrease was not significant (P = .83). In all three groups, the rate never dropped below 7%.
The present study revealed a noticeable improvement in all items of diabetic outcomes, as measured by the Dental Neglect Scale, Oral Health problems, Oral Hygiene Behavior, and Oral Health Quality of Life, as well as the Oral Health Value Scale and HbA1c, after the application of Health nursing guidance based on a smartphone intervention. This result aligns with Haghdoost et al. (2023), who reported that diabetic patients did not exhibit an acceptable oral health status, and to some extent, oral problems affected oral health-related quality of life. Smart Applications of Oral Hygiene and Diabetic Control Nursing guidance can improve oral health-related quality of life, encompassing three domains.35 Likewise, this finding aligns with Khalifa et al. (2020), who stated that the results indicated that educational interventions enhance oral health knowledge and improve behavior, resulting in significant improvements in diabetic outcomes for adult patients. 21
The current study extends compelling evidence for the effectiveness of oral health education guidance and interventions in improving oral health outcomes in patients with type II DM. This approach presents a promising strategy for managing diabetes-related oral health issues and improving the overall health and well-being of this population. This outcome aligns with Sowmya & Sangavi (2024), who emphasize that regular oral care significantly benefits diabetic patients, with 61% reporting enhanced oral health and 39% noting no improvement. 39
Limitations of the study
Some challenges with the current study were that, first, the intervention lasted only three months, and the researchers did not extend this period due to concerns about patients’ withdrawal from the study. Therefore, the researchers recommended increasing the duration of the intervention phase to 6 months to maintain validated data and valuable outcomes in future studies. Second, a small sample size was used; this may be due to the limited flow rate in the outpatient clinic at the time of the study’s conduction. Third, sampling biases may be due to the researchers’ focus on a clinical profile of diabetic patients, with neglect of different demographic characteristics. Conducting intervention studies with larger sample sizes would provide more comprehensive and reliable evidence regarding oral health outcomes and glycemic control in individuals with type 2 diabetes mellitus (T2DM).
Conclusion
The role of health nursing guidance based on smartphone Applications can modify health-related outcomes among diabetic patients. The Dental Neglect scale score and the Glycated Hemoglobin Level (HbA1c) decreased in the study group compared to the control group after the intervention, at 3 months. The Oral Health-Related Quality of Life and oral health values scores improved in the study group compared to the control group following the intervention.
Recommendations
➢ Considering the effectiveness of the mHealth instructional approach, it is recommended that the healthcare system utilize it extensively. ➢ Integration with healthcare providers through facilitating communication and data sharing between patients and healthcare providers through the app to enable monitoring and timely intervention. ➢ Dental tests and inspections for people with diabetes should be used in conjunction with assessing health behaviors to consolidate oral health values. ➢ It is essential to educate and counsel diabetic patients and healthcare professionals on the importance of maintaining good dental health. ➢ Develop apps that seamlessly integrate features for oral hygiene management and diabetic control instructions, providing comprehensive support for patients. ➢ Implementing behavioral change techniques that are based on self-monitoring and rewards to promote adherence to oral hygiene and diabetic control instructions.
Footnotes
Acknowledgements
We gratefully acknowledge all the participants at the research location for their invaluable contribution and collaboration in this study.
Ethical considerations
In accordance with the Declaration of Helsinki and principles of ethical research, this study was approved by the Faculty of Nursing’s Ethical Committee in Menoufia University (Ethics code: 961).
Consent to participate
Oral informed consent was obtained from all the subjects before the study. Participants were assured of the confidentiality of their data. They were also informed of their right to withdraw from the study at any time. Informed consent was obtained from all individual participants included in the study.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Guarantor
Dr Nabila and Dr Amal are the guarantors of the work.