
Abstract
Background
Diabetes is a chronic disease affecting many people globally and is a significant health concern. Health services are focusing on managing the rising incidence of diabetes and its complications. A novel mobile health (mHealth) intervention intends to assist diabetics in managing the levels of their blood sugar and improving self-care. The study aimed to evaluate the effect of short message service (SMS) and mobile app interventions on patients’ capacity to improve hemoglobin A1c (HbA1c) levels.
Method
A targeted search was performed in PubMed, MEDLINE, EMBASE, the Cochrane Library, ScienceDirect, and Scopus for randomized controlled trials (RCTs) published from 2014 to 2024 that evaluated the effects of mobile apps and SMS-based self-care interventions on individuals with poorly managed diabetes.
Result
A rigorous review identified nineteen studies for analysis. Fifteen of these studies showed a statistically significant reduction in HbA1c levels in the intervention group, compared to baseline measurements. In contrast, control groups did not exhibit the same level of reduction, resulting in a significant difference between intervention and control groups over time. This suggests that the interventions were effective in lowering HbA1c levels.
Conclusion
Improving glycemic levels in inadequately managed diabetes is crucial. Better blood sugar management enhances patient well-being and lowers healthcare costs, making targeted interventions essential for improved outcomes and healthcare efficiency. When developing support services and educational programs for diabetes self-management, considering value-based care and public health models, it is important for organizations, diabetes educators, legislators, and funders to carefully consider these solutions.
Background
Diabetes mellitus (DM) is a group of metabolic disorders that cause hyperglycemia, which is a common feature of all types of diabetes. This high blood glucose level can lead to a specific kind of microangiopathy1,2 that can result in retinopathy, nephropathy, peripheral neuropathy, and autonomic neuropathy. These conditions can cause various symptoms, including loss of vision, renal failure, foot ulceration, amputations, Charcot's joints, gastrointestinal issues, genitourinary problems, cardiovascular symptoms, and sexual dysfunction.3,4
Diabetes is a prevalent and progressive chronic disease, representing a significant global health concern, especially in low- and middle-income countries. 5 The occurrence of diabetes is steadily increasing, with the World Health Organization (WHO) estimating there were 422 million adults with diabetes worldwide in 2014. The prevalence rate in adults rose from 4.7% in 1980 to 8.5% in 2014, with low- and middle-income nations experiencing the biggest increase in comparison to high-income nations. 6 One and a half million deaths in 2019 were directly related to diabetes, and 48% of these deaths happened in people under 70. 7 If no actions are taken to stop the rise of diabetes, the number of individuals with diabetes is projected to reach at least 629 million by the year 2045. 8
Based on the WHO categorization, there are two main types: T1DM and T2DM. 9 T1DM was formerly referred to as childhood-onset; data from many high-income countries indicate an annual increase of between 3% and 4% in the rate of T1DM in childhood. Despite being common in children, type 1 diabetes can also affect adults, with 84% of individuals living with T1DM being adults. 10 T2DM, formerly called adult-onset or non-insulin-dependent diabetes, makes up 90% to 95% of all cases of diabetes, with the highest proportions in nations with low and moderate incomes. 6
Maintaining proper blood glucose control can help prevent complications from diabetes. Patients with diabetes were found to have a hemoglobin A1c (HbA1c) target of <7% (<53 mmol/mol), which is the commonly advised level for effective control.11,12 If glycemic control is poor (>8%; 64 mmol/mol) or suboptimal (>7%; 53 mmol/mol), more intervention is advised. It is estimated that between 25% and 30% of people with diabetes have HbA1c levels that are higher than 8% (64 mmol/mol), indicating inadequate control.13,14 To attain and sustain this goal of good glycemic control, significant assistance and input are required due to the expensive and incapacitating nature of the complications affecting small and large blood vessels of poorly managed diabetes. 15
Combating the global rise of diabetes is a health service priority. There is substantial proof showing that maintaining acceptable blood sugar levels in individuals with T1DM or T2DM leads to notable decreases in the likelihood of complications occurring. These complications include failure of the renal system, retinopathy caused by diabetes, lower-limb amputation, stroke, and cardiovascular illness.16–18 These issues negatively impact the quality of life for patients, and a significant amount of healthcare expenditures go toward the clinical management of these problems. 19
Interventions focused on supporting the self-management of diabetes have typically been provided through written materials, In-person sessions, or team programs, for instance, “Diabetes Self-Management Education (DSME)” programs. It is designed to meet the seven key practices for self-management behaviors listed by the American Diabetes Association Education: Nutritious meals; Physical activity; controlling, getting medication; resolving problems; minimizing hazards; and coping in a healthy way. 20 For individuals with inadequate DM management, however, assistance may require going outside conventional medical settings to maintain the habits needed to control diabetes in the context of a patient's routine activities.
The implementation of short message services and cell phone applications for DM self-care and assistance has increased since the advent of cell phone technologies, with widespread accessibility and acceptance by all people. 21 Cellular phones are often utilized to create alarms and notifications, showing the ability of cellular healthcare technologies to transcend the pragmatic obstacles of conventional care. Messaging via text is a widely used communication tool globally due to the availability of cell phones. Therefore, short message service (SMS)-based intervention could provide an expandable and efficient means to provide medical data such as adherence to medications, monitoring of blood glucose levels, regular exercise, and a nutritious diet; to enhance healthcare outcomes.22–25
In addition, SMS provides the significant advantage of delivering messages instantly, ensuring that users receive important information without delay and at a very low cost. It could serve as an outstanding and effective tool for offering support in the management of diabetes. This method of communication not only helps in reaching individuals quickly but also keeps them connected to vital resources and assistance, making it an ideal choice for healthcare providers looking to enhance support for those managing this chronic condition. Previous studies have supported the benefits of cell phones for DM self-care.26–28
The study, 29 which had a broader scope, aimed to compare the effectiveness of various digital health interventions: SMS, smartphone applications, and website-based platforms, particularly targeted at adults with Type 2 diabetes, and endeavored to not only evaluate the effectiveness of these interventions but also to assess their reach, uptake, and overall feasibility. The findings showed that both smartphone applications and SMS interventions improved glycemic control.
Objective
The study aimed to evaluate the efficacy of text message (SMS) and cellphone application interventions on the self-management practices of DM patients to improve their elevated HbA1c levels.
Methods
Criteria for selecting articles
The study's inclusion and exclusion criteria considered the following conditions: (i) Type 1/Type 2 DM (T1DM/T2DM) patients, (ii) only research on self-management of T1DM and T2DM that utilized mobile applications or SMS, or coupled with other innovations such as wearable devices (i.e. pedometer). (iii) Follow-up measures are a minimum of 3 months following the initial state. (iv) RCTs, since the study intended to evaluate the efficiency of interventions. 30 (v) It was documented in English. (vi) The research was disqualified if the control groups (CGs) did not receive regular diabetes care or if they used digital technology.
Information sources and design
The review objective and search strategy were guided by the patient, intervention, comparison, and outcomes framework.31,32
The study report followed the principles given in the “Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA)” statement. 33
The following databases were searched: Scopus, ScienceDirect, EMBASE, Cochrane Library, and PubMed on 7 January 2025.
Search strategy
The authors used these keywords to identify relevant published research articles, as shown in Table 1.
Search parameters for selecting articles.

The selection process
The searches were conducted and imported into the EndNote X9 Reference program. A thorough data extraction form was created (LG) and refined (LG and BL). Data extracted from each study included: publication details; study design (purpose, blinding, randomization, and statistical analyses); participant characteristics (condition, inclusion/exclusion criteria, sample size, recruitment, and demographics); comparison details; outcomes (follow-up, primary/secondary outcomes with variability measures, 34 and measurement tool); and conclusions (LG, and BL). TB provided methodological oversight, assisted in resolving discrepancies in data extraction, and contributed to manuscript editing and refinement.
The risk of bias assessment
To assess the possibility of bias in the randomized controlled trial's (RCT’s) results, the RoB 2 tool framework was employed. The tool is structured into five domains: determined by using individual bias items by the guidelines provided in the updated Cochrane bias risk tool for randomized experiments, and classified as “Low risk,” “High risk,” or “Some concerns” (RoB 2). 35
Outcome and evidence
Evidence was tabulated, detailing intervention and comparator treatments, objectives, outcomes, and key study characteristics. The primary outcome was the change in mean HbA1c plasma concentration (with 95% confidence interval) after ≥3 months. Interventions were considered effective if they resulted in either a clinically meaningful (≥0.5% HbA1c decrease) or statistically significant (p < 0.05) difference compared to the CG. Interventions were deemed ineffective if groups showed no clinically or statistically significant difference.
Result
In the initial search of the study, 2929 records were discovered in the databases. After removing 231 duplicates, the topic and abstract of 2698 records were assessed for eligibility. Subsequently, 2607 references were deemed ineligible and excluded. Following this, further analysis will be conducted on the complete texts of the remaining 91 publications. Out of these, 19 articles were deemed eligible for inclusion and are reviewed here. Figure 1 shows the procedure of looking for and choosing using a PRISMA flow diagram.
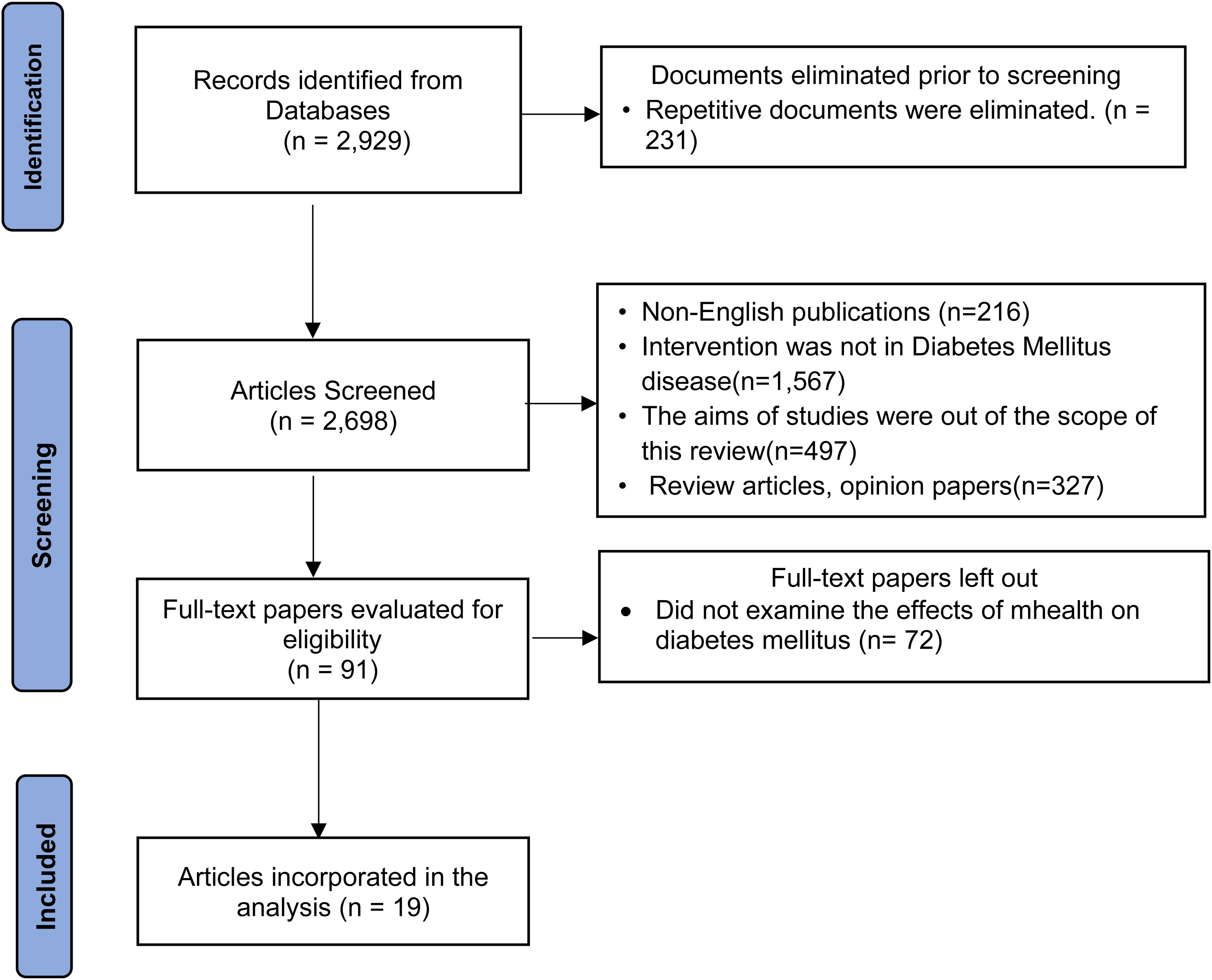
The preferred reporting items for systematic review and meta-analysis (“PRISMA”) diagram showing the selection procedure. 33
Overview of the included research
The study characteristics are detailed in Table 2. Most of the articles (six) were published in 2019, with the other three in 2018, three in 2020, and three in 2024. The remaining four were published in 2014, 2016, 2017, and 2021. As mentioned in Table 2, all studies were RCTs. The diversity of participants in the sample ranged from 30 to 742, providing a comprehensive range of perspectives and insights. One study included individuals with Type 1 diabetes 36 ; two targeted Type 1 and Type 2 diabetes24,37; and the remaining 16 had Type 2. The research was carried out in various populations, including Asian populations,34,38–45 the USA,22,46,47 France, 36 Spain, 48 Australia, 49 New Zealand, 24 the Netherlands, 50 South Africa, 37 and Rwanda. 51 The main result of interest in all studies examined was hypoglycemic (HbA1c) management.
Features of the included studies.

RCT: randomized controlled trial; SMS: short message service; T1D: Type 1 diabetes; T2D: Type 2 diabetes.
The mobile health (mHealth) interventions applied were text messaging (SMS) and mobile applications. Eight studies used text messages (SMS); texting actions provided educational content to enhance individuals’ understanding of the basics of their health status and the need for lifestyle changes such as regular exercise and nutrition; encourage medicine compliance; deliver alerts for constantly tracking the levels of blood sugar and hypertension; and enhance medication adherence.24,36,37,42,43,46,48,49 The rest of the research used smartphone app interventions that require individuals to continually self-care for blood sugar or hypertension levels and track these parameters, together with food consumption, sporting activities, and medicine, permitting medical personnel to deliver knowledge, immediate assistance for medicine adjustment, and advice for lifestyle modifications.22,34,38–41,44,45,47,50,51 All studies compared interventions with standard care.
Evaluation of risk of bias
Figure 2 depicts a summary and graph, indicating the authors’ decisions on every article incorporated in the study for bias risk assessment. Due to inadequate reporting, the existence of bias was ambiguous, making it impossible to determine if any research was without bias. Fourteen papers were at minimal risk of bias resulting from the randomization process.24,36,38–42,44–49,51 Three of the studies did not mention blinding,41,42,50 while four other studies were classified as a significant risk because of the absence of concealment,22,34,37,44 eight studies have been identified as having a high probability of bias due to attrition, 22,24,38,39,45–47,50 with the remaining eight studies34,36,37,40,41,48,49,51 regarded as low-risk, and three studies as some concerns.42–44 In general, the quality of methodology varied significantly among the articles included in the analysis. Out of the total sample, 13 studies (68.4%) were deemed to have a minimal degree of bias, four papers (21%) were identified as having a moderate bias risk, and two studies (10.5%) were believed to have a significant bias risk.
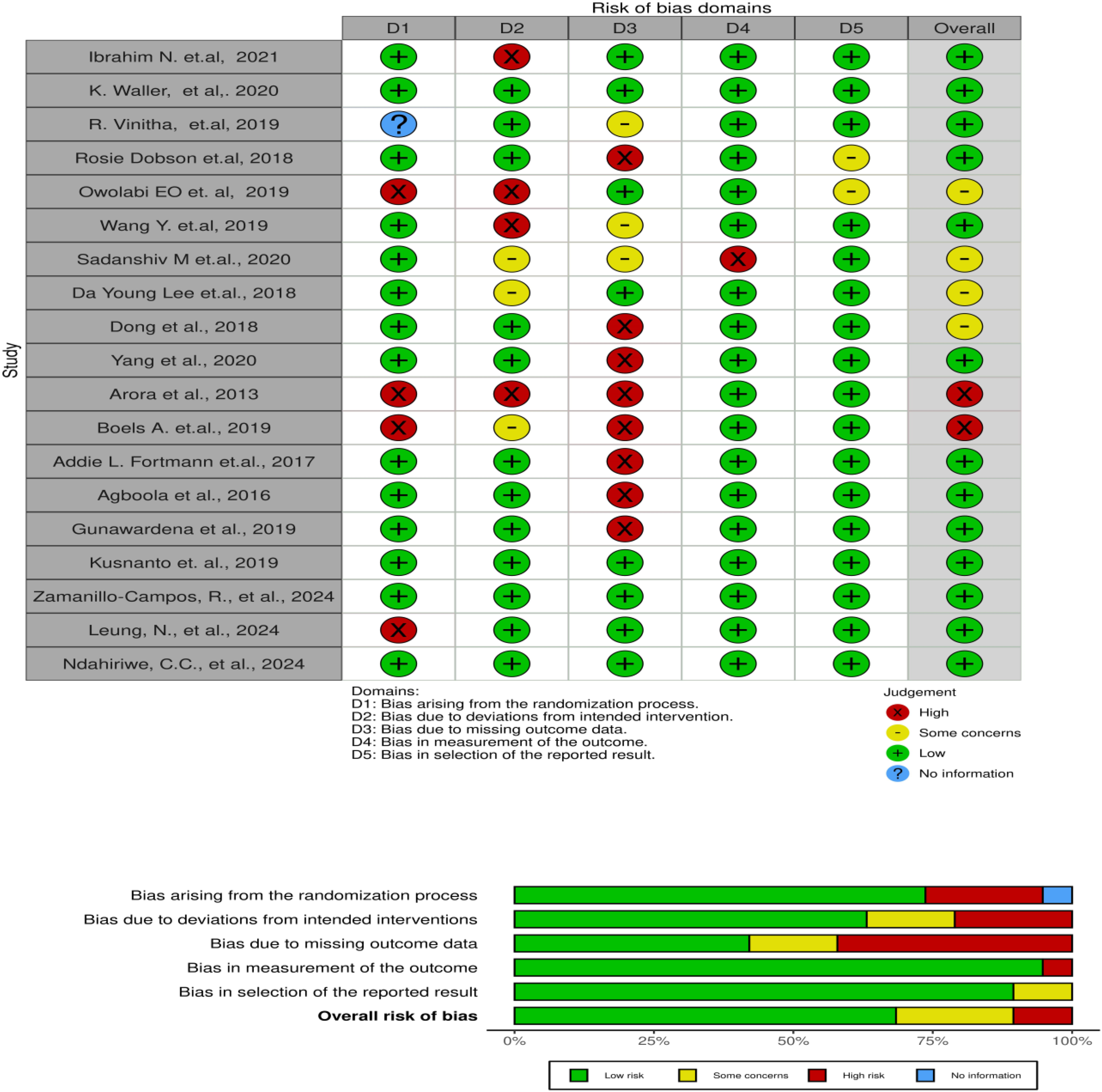
A summary and graph of the risk of bias.
Due to a scarcity of detailed data and inconsistent reporting in the research, the study was unable to perform a sensitivity analysis. The diverse methods and varying quality of the studies also made a reliable sensitivity analysis difficult to conduct.
Effects of mHealth interventions
The intervention group (IG) showed a substantial decrease in HbA1c from the starting point to subsequent monitoring in comparison to the CG, as reported in 15 studies.22,24,36,38–48,51 The other four studies found insignificant differences between the IG and the CG.34,37,49,50
Table 3 provides an outline of the main results from the studies that were selected, with little consistency found in the outcome measures reported. Four studies34,38,41,43 revealed changes in levels of physical activity, with just one indicating a noticeable rise in activity frequency among the IG. 41 Three studies documented alterations in dietary habits, with one study highlighting a significant increase in vegetable intake but not affecting other nutritional outcomes. 49 One study identified no noticeable shift in dietary behavior, 43 while the other found a significant drop in the IG's mean calorie consumption. 38
Key findings from the research.
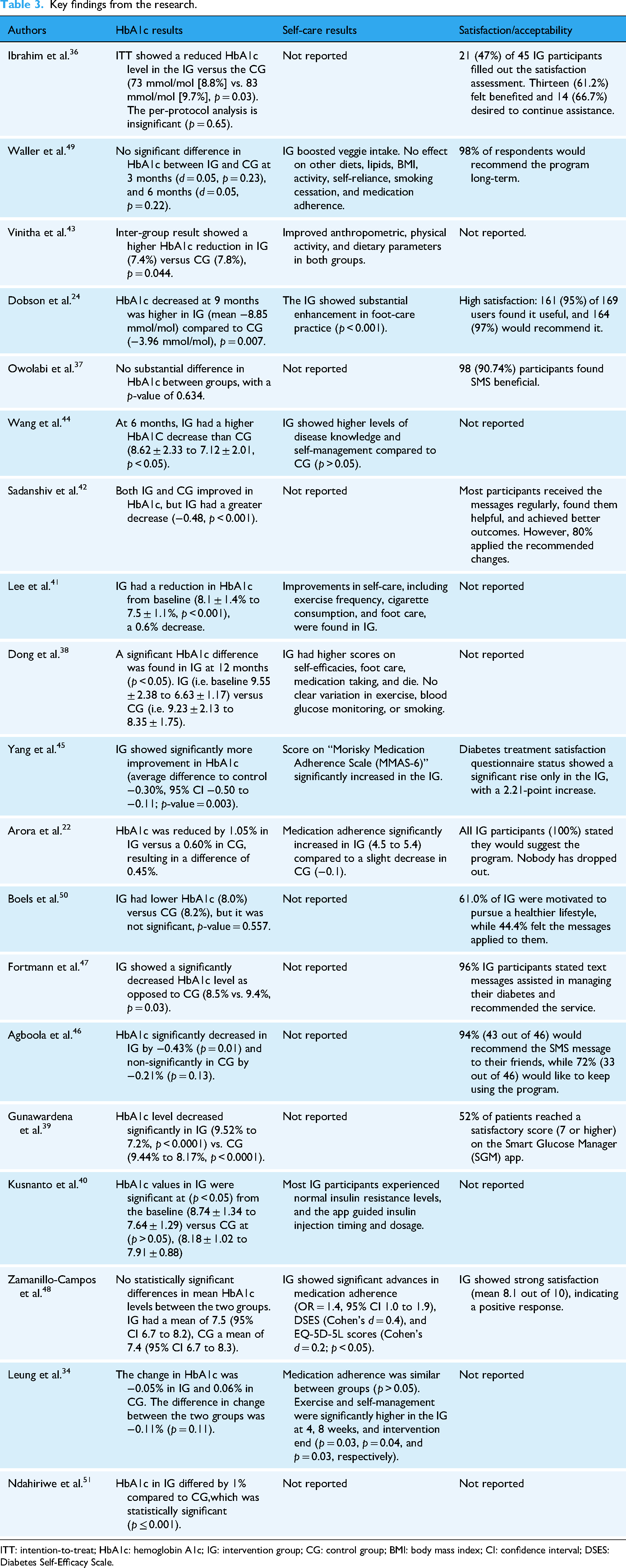
ITT: intention-to-treat; HbA1c: hemoglobin A1c; IG: intervention group; CG: control group; BMI: body mass index; CI: confidence interval; DSES: Diabetes Self-Efficacy Scale.
Three studies38,41,44 examined changes in diabetes-related self-management. Two papers presented improvement in the IG; however, one study found a substantial difference in comparison to the CG. 38 Knowledge of diabetes improved more in the IG as opposed to the CG, as shown in a study. 41 In another study, the intervention arm showed improved blood glucose monitoring, 40 and four of the studies showed significant differences in medication adherence.22,34,45,48 Twelve investigations have consistently shown that the intervention is associated with high levels of satisfaction and acceptability.22,24,36,37,39,42,45–50
Features of successful interventions
The 15 studies resulted in a substantial drop in HbA1c levels from the initial measurement to later assessments, which were all designed differently. Five studies focused on helping individuals memorize their diabetic medications or blood glucose monitoring.34,36,45,47,48 The other 12 provided self-management support,22,24,34,38–44,48,50 and one study 46 offered insulin changes according to individual information collected through a pedometer. Additionally, based on the same patient-specific information acquired by the pedometer, medication and lifestyle advice were also provided. Furthermore, the self-care behaviors focused on also differed—seven studies centered on healthy lifestyle practices and medication adherence,22,24,34,41,43,47,48 whereas the remaining five studies centered on a good diet, exercising, and monitoring.38,40,42,45,50 The successful interventions ranged from 3 to 24 months in duration. One common similarity among the effective interventions was the implementation of mobile devices to deliver automated clinical knowledge via SMS. Despite the varying approaches taken in each of the 15 studies, all saw improvements in HbA1c levels within the IG.
Discussion
The study provided an in-depth assessment of the current mHealth technologies employed for diabetes self-management among individuals with poorly controlled glycemic profiles, as indicated by elevated HbA1c levels. Of the 19 RCTs that met the inclusion criteria, 15 demonstrated a statistically significant reduction in HbA1c within the IG compared to the CG. These findings reinforce the efficacy of mHealth interventions in improving glycemic control and optimizing diabetes outcomes.
Improved glycemic control is widely acknowledged to reduce the risk of both microvascular and macrovascular complications in individuals with diabetes, thus lowering disease burden and mortality rates. 52 The UK Prospective Diabetes Study (UKPDS) notably reported that every 1% reduction in HbA1c was associated with a 21% decrease in diabetes-related deaths, a 14% reduction in myocardial infarctions, and a 37% decrease in microvascular complications. 53 The impact of several diabetes medications on HbA1c reduction is widely understood. 52 Cardiovascular disease is the leading cause of death among patients with diabetes, and one study indicates that diabetics are nearly three times more likely to die from cardiovascular disease. 54 Compared to individuals without diabetes, those with diabetes experience higher death rates following their first myocardial infarction. 55 As per the United Kingdom Prospective Diabetes research, 49% of fatalities in a decade of evaluation were caused by coronary heart disease. 56
The current findings align with the existing literature emphasizing the value of patient self-care behaviors in maintaining glycemic control. Prior studies have demonstrated that following recommended self-care activities for diabetes is crucial for controlling blood sugar levels. Thus, it is possible to deduce that individuals’ active involvement in their care may play an important part in forecasting positive disease results.57,58 It is essential to create new education programs for diabetic patient and evaluate their efficacy to guarantee optimal utilization of healthcare resources. In this respect, cellphone-based self-management learning programs provide the ability to move attention away from the clinic into the patient's daily lives, where attitude and conduct can be modified.59,60
mHealth interventions have rapidly gained popularity in managing chronic diseases, creating opportunities to enhance the self-management abilities of individuals suffering from diabetes.27,61,62 When mobile devices are used for health purposes, they can support various aspects of self-management, including healthy eating habits, physical activity, insulin management, medication adherence, effective problem-solving abilities, positive emotions, and risk-reduction practices.63–65 Previous studies have supported the efficiency of mHealth for diabetic self-management.26–28,66,67
Many scholars have concentrated their efforts on this technology, and numerous studies have been conducted to explore how to enhance treatment effectiveness for individuals with diabetes.68,69 For instance, research conducted in the UK created an innovative assistance system using a distinctive texting platform to provide personalized communication and generic diabetes details. 70 Another study conducted in Korea assessed the influence of the nurses’ use of SMS on elevated levels of HbA1c and patients’ compliance with recommended diabetes therapies. 71 In addition, in the USA, Mulvaney et al. 58 conducted a study to evaluate the efficacy of a customized communication platform based on personally stated diabetes management obstacles, on glycemic levels.
This study found that the mHealth method was deemed satisfactory by a large number of individuals. The acceptance of health information technology (HIT) and mHealth is shaped by various factors, with perceived usefulness and ease of use being key drivers. Individuals are more likely to adopt technologies they see as beneficial and easy to use. Social influences and endorsements from healthcare providers also significantly impact acceptance; patients are more inclined to use HIT and mHealth if trusted healthcare figures support these tools. Additionally, technological literacy and cognitive factors play a role, as those with higher digital skills feel more confident using health applications.
However, barriers exist, especially for older adults. System design and usability issues can hinder engagement, while concerns about privacy and data security deter potential users. Individual preferences for customization in health apps also affect adoption; tailored solutions are more likely to be accepted, enhancing user engagement. Addressing these diverse influences and obstacles is crucial for promoting HIT and mHealth acceptance in healthcare today.72–77
The efficacy of text message interventions and mobile phone apps for the enhancement of HbA1c in DM patients may be explained by various factors. First, because of advancements in technology, contemporary cell phones have a variety of features, such as connecting with wearables or ingestible medical devices78,79 that allow continuous tracking and then enhance outcomes. Second, real-time modes of communication, such as videoconferencing, permit medical professionals to take action more promptly compared to traditional ways. 80 Third, text messages and cellphone apps provide easier, more user-friendly access due to the convenience and portability of cellphones. 29 Fourth, interventions provided at home enhanced accessibility and convenience, likely promoting greater engagement.
Finally, this study is unique in that it is comprehensive and clinically focused, unlike other reviews, such as Moschonis et al., 29 this one looked at secondary outcomes such as diet, physical activity, medication adherence, and diabetes knowledge, giving a more complete picture of the self-care of patients with Types 1 and 2 diabetes. In addition, current research was evaluated, allowing for more recent interventions. Furthermore, the acceptability and satisfaction of the intervention were assessed, which is essential in terms of patients’ usage of and sustained adherence.
Research implications
Further research is needed to evaluate the long-term impact of mHealth interventions on diabetes self-management. Future studies should investigate sustained engagement, long-term adherence, and potential unintended consequences, beyond short-term HbA1c reductions. Exploring artificial intelligence (AI) and machine learning's potential for personalized interventions and improved glycemic control prediction is also critical. Comparative studies assessing the cost-effectiveness of different digital health platforms across diverse populations will help identify optimal interventions.
Practical implications
This study highlights the importance of incorporating mHealth into standard diabetes care. Healthcare providers should use SMS and mobile applications, particularly for individuals with inadequately managed diabetes. To achieve the best results, it is essential to offer training in digital health literacy and ensure accessibility for older adults and underserved populations. Additionally, using telemedicine and interactive mobile coaching can enhance patient engagement and adherence to treatment. Ultimately, successful mHealth interventions need to be user-friendly, customizable, and seamlessly integrated into existing healthcare systems to optimize patient outcomes.
Policy implications
Policymakers should recognize the growing role of mHealth in managing chronic diseases and develop regulatory frameworks that ensure the safe use of digital health technologies. Standardizing data privacy, interoperability, and reimbursement for mHealth can enhance use. Funding initiatives for evidence-based mHealth solutions will ensure equitable access. Collaboration among tech developers, healthcare providers, and patients is essential for improving the effectiveness and sustainability of digital health interventions for diabetes management.
The study limitations
This study did not examine ongoing participation, long-term adherence, and unintended outcomes beyond short-term HbA1c reductions. It also did not explore the use of AI and machine learning to personalize interventions and predict improved glycemic control.
Conclusion
Robust and scalable research methods can revolutionize mHealth research. This may have led to positive changes in DM self-management behavior. These approaches can enable the rigorous evaluation of mobile apps and SMS in a more timely manner, while facilitating the rapid and iterative development of an intervention, keeping pace with the rapidly and continuously evolving mHealth landscape. Enhancing glycemic management in individuals with inadequately controlled diabetes is a difficult task. However, the achievements of these populations are advantageous for the individual's health and for the healthcare system as a whole. Therefore, organizations, diabetes educators, and policymakers must include such approaches in the development of diabetic self-monitoring support and learning services for community health and value-based healthcare systems. mHealth solutions, leveraging evidence-based and tailored behavioral interventions, can improve access to and the effectiveness of diabetes management education and support, especially considering the widespread use of mobile phones.
Footnotes
Abbreviations
Acknowledgements
Not applicable.
Authors contributions
Registration and protocol
Not applicable
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Construction and Practice of Quality Assurance Mechanism for Vocational Undergraduate Nursing Education through Medical Education Collaboration + Hnjg2024-171.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.