
Abstract
Objective
Digital health has recently gained a foothold in monitoring and improving diabetes care. We aim to explore the views of patients, carers and healthcare providers (HCPs) regarding the use of a novel patient-owned wound surveillance application as part of outpatient management of patients with diabetic foot ulcers (DFUs).
Methods
Semi-structured online interviews were conducted with patients, carers and HCPs in wound care for DFUs. The participants were recruited from a primary care polyclinic network and two tertiary hospitals in Singapore, within the same healthcare cluster. Purposive maximum variation sampling was used to select participants with differing attributes to ensure heterogeneity. Common themes relating to the wound imaging app were captured.
Results
A total of 20 patients, 5 carers and 20 HCPs participated in the qualitative study. None of the participants have used a wound imaging app before. Regarding a patient-owned wound surveillance app, all were open and receptive to the system and workflow for use in DFU care. Four major themes emerged from patients and carers: (1) technology, (2) application features and usability, (3) feasibility of using the wound imaging application and (4) logistics of care. Four major themes were identified from HCPs: (1) attitudes towards wound imaging app, (2) preferences regarding functionality, (3) perceived challenges for patients/carers and (4) perceived barriers for HCPs.
Conclusion
Our study highlighted several barriers and facilitators from patients, carers and HCPs regarding the use of a patient-owned wound surveillance app. These findings demonstrate the potential of digital health and areas to improve and tailor a DFU wound app suitable for implementation in the local population.
Introduction
In patients with diabetes, the lifetime risk of developing a diabetic foot ulcer (DFU) is estimated to range from 19% and 34%. 1 Patients with diabetes also have a 15–20 times increased risk of lower extremity amputation and this is usually preceded by a DFU in up to 85% of the time. 2 Previous studies have shown that at least 25% of DFUs do not heal, increasing the risk of amputation.3,4 Following the index DFU, the recurrence of the subsequent ulceration is 40% in the first year and up to 60% in 3 years. 1 DFUs present significant risk factors for lower extremity amputations, leading to increased risk of mortality and costs. 5 In 2017, the mean cost to manage a DFU in Singapore was US$3,368, going up to US$10,468 for a minor amputation and US$30,131 for a major amputation per patient-year. 6
The frequent visits for treatment at healthcare facilities impose substantial burdens to patients with DFU and healthcare systems.5,7 Wound care, being an important aspect of outpatient DFU management, is complex and involves a multidisciplinary team of doctors, nurses, podiatrists, allied health providers, and not forgetting patients and their carers. This process includes (1) wound assessment, (2) documentation and monitoring and (3) intercommunication between different various healthcare providers (HCPs).8,9 There have been several developments of various comprehensive wound assessments and monitoring systems to improve the experience and quality of wound care. Patients with diabetes are educated to take ownership of their foot care and to take preventive measures such as regular foot checks for pre-ulcerative signs and recognise wound progression. 10 Adopting best practice patient education can empower a patient to take care of their own condition and is a cost-effective method to preventing DFUs and offering maintaining ulcer-free foot in remission state.11,12
Technology is increasingly being adopted into diabetes care for example in the implementation of real-time continuous glucose monitoring. 13 These technologies have helped empower patients and improved self-care, 14 resulting in better control of their glycaemic index. 15 Overall, this leads to better patient outcomes and reduced healthcare expenditure.16,17 However, technology has yet to be widely used in DFU care but is slowly gaining traction. 18 Hence, a qualitative approach is timely to provide an in-depth understanding of the participants’ and HCPs’ perspectives in using smart technology. Although there has been some qualitative studies done on patients19,20 with DFUs, these studies recruited their patients from single wound care clinic which might weaken the external validity as the patients with DFUs might have different characteristics and perceptions towards digital health. Thus, we aim to address this limitation by recruiting a wide variety of patients, across various education, employment and ethnicity backgrounds, hence representing the heterogeneity of the Singaporean population to better cater our app development for their ideas, concerns and expectations. Other studies within the literature also included HCPs managing patients with DFUs,21,22 but there were no previous studies that explore the usage of mHealth for DFU from a carers’ perspective. In Singapore, which has an ageing population, many DFU patients are cared for by their family members and/or their domestic helpers.
Therefore, this study aimed to explore concurrently patients, carers and HCPs’ perspectives on a patient-owned wound imaging system for DFU care. This will allow us to explore the perceptions from all stakeholders to develop an effective and seamless application that can integrate into the healthcare system. This study was conducted as the first part of a larger clinical study, seeking to evaluate the
There are four overreaching research questions (RQs) that this study aims to address:
RQ1: What are patients and carers’ preferences regarding features of the app for wound management? RQ2: What are HCPs’ attitudes in using a wound imaging app? RQ3: What are HCPs’ preferences regarding features of the app for wound management? RQ4: What are HCPs perceptions in using a wound imaging app for clinical practice and diverse patients?
Methods
Design, setting and ethics
Semi-structured interviews were conducted via video tele-conferencing between June and October 2021. Interviews were conversational in nature, and items were not asked verbatim or in the order presented in the interview guide (Supplemental A, B and C). Purposive maximum variation sampling was used to select participants with differing attributes such as ethnicity, education and employment and whether they have previously used their phones to take photos of their foot wounds. This provided us with a better representation of the Singapore population and ensured heterogeneity to capture common themes related to the wound imaging app. Participants were recruited from a primary polyclinic network and two tertiary hospitals in Singapore. Ethics approval was obtained from the local institutional ethics board (National Healthcare Group DSRB reference: 2020/01347).
Study participants
There were three categories of participants patients with diabetes, carers of patients with diabetes and HCPs.
Inclusion criteria for patients were: aged 21 years or above, community-dwelling, can speak either English or Mandarin, has diabetes (self-reported by the participants) and affected by DFU for more than 3 months. Exclusion criteria were persons with severe mental illness who lack the capacity to self-care and participants with severe communication difficulties. Inclusion criteria for carers were: they must not be professionally qualified (family member, friends, domestic helpers), 21 years or older, can speak either English or Mandarin (both are commonly used languages in Singapore) and directly involved in the day-to-day care of community dwelling patients with DFU for at least 3 months. HCPs consisted of various representatives from the multidisciplinary management of DFUs. This includes surgeons, primary care physicians, nurses, podiatrists and diabetologists from a primary care polyclinic network and two tertiary hospitals in Singapore.
Data collection
Upon obtaining informed consent, patients and carers were required to complete a brief sociodemographic survey. For patients and carers, an individual interview was arranged. For HCPs, the interviews were conducted through focus group discussion comprising four HCPs per group. Participants were notified that the interview was audio recorded. HCPs were presented with a single video, while patients and their caregivers were shown a separate two-part video, with the purpose of providing them an orientation to the InSight app (eKare Inc, Virginia, USA), as an example of a wound imaging app (Supplemental D).
As per International Organization for Standardization (ISO) 9241-210 definition of human-centred design, our approach to systems design and development aimed ‘to make interactive systems more usable by focusing on the use of the system and applying human factors/ergonomics and usability knowledge and techniques’. 23 Hence, within these qualitative semi-structured interviews were conducted with flexible prompt guides to help facilitate discussions. For interviews with HCPs, they were asked about their demographics (year of experience in wound care and job title), proposed implementation of wound app, perceptions towards challenges for adoption, and factors that will facilitate adoption and preferences regarding features of the app for wound management. For interviews with patients and carers, open-ended questions were asked around topics such as their current usage of mobile apps, their views on the app and any improvements they would like to see that could encourage them to use the app.
In each interview, a notetaker was assigned to observe and give a high-level description of what transpired during the interview, including both participant feedback and any important moments in the discussion. A post-interview memo was written after each interview session as a reflection by the notetaker. The interview notes and post-interview memos were used as references during the data analysis.
Data analysis
To increase the trustworthiness of our study, we have implemented several strategies to improve credibility, transferability and confirmability. Firstly, we transcribed the audio recordings in full verbatim and included time stamps. For interviews conducted in Mandarin, the audio recordings were transcribed in their original language and then translated to English. This approach ensured the accuracy of the data and improved the transferability of the study by providing a clear methodology for analysing the data. Secondly, we conducted a thematic analysis to identify common themes, which enabled us to group the large amount of data obtained from the in-depth interviews into meaningful categories. We generated an initial coding scheme based on key thoughts from the participants, and then sorted the codes based on their relationships to each other. Team members reviewed the transcripts multiple times to achieve a thorough understanding of the interviews and extract the deeper meanings in them. This approach improved the confirmability of the study by demonstrating a systematic and transparent approach to data analysis. Finally, we grouped the emergent categories from the data into meaningful clusters representing the major themes and subthemes of the study. By implementing these strategies, we were able to increase the trustworthiness of our study and provide reliable and valid results.
Results
Patient and carers
A total of 20 patients and five carers were included in this study. The mean age of patients was 61 ± 9, while the carers were younger with a mean age of 45 ± 17. All the carers and 90% of the patients had at least a primary school education. A total of 45% of patients and 40% of carers were employed at the time of the interview. Half of the patients have previously used their phones to take pictures of their foot wounds. The patient and carer demographics are outlined in Table 1.
Sociodemographic characteristics of patients and carers.

Categorical variables are presented as n (%) and continuous variables are presented as mean (standard deviation).
Patients and carers who participated in the study were open and positive to the concept of a patient-owned wound imaging system for DFU care. The participants expressed their perspectives on personal experiences and preferences in relation to application usage. From the participants’ views and experiences (RQ1), four key themes were identified: (1) technology, (2) application features and usability, (3) feasibility of using the wound imaging application and (4) logistics of care. Table 2 summarises the key themes along with their subthemes and specific examples.
Themes with specific examples from patients and carers.

Technology
Technology is a major theme identified in this study and determines the acceptability of introducing a new app to the patients and their carers. In addition, a common subtheme of internet and smart phone accessibility surfaced.
Contrary to popular belief that the elderly are not technologically savvy, most participants had internet access and were using smartphone apps for daily usage with differential needs including online shopping and communication with family and friends. Social media plays a significant part in patients and carers’ daily routines as most of the patients used their smartphones for interaction purposes. For example, different social media usage was discussed, such as Facebook, YouTube, Messenger, Instagram, Twitter, WeChat and Zoom: "Facebook, I have mine, my wife will see what the news is in Singapore."
"I have like this Zoom app, I have a lot of crazy app, Twitter. I have my Signal, I have my Telegram, I have my WeChat, I have my WhatsApp."
A few participants found their smartphones useful for health purposes, but mainly for scheduling their medical appointments: "And then the HealthHub, normally I go for my appointments on this, yeah" "Because why I’m, I’m not very, very good using the phone."
Application features and usability
Another theme that surfaced from the participants’ experiences and preferences is application features and usability. Components of this theme are ease of use and preferred features. The participants expressed that the ease of use was vital. In fact, one of the participants felt very positive about using a wound imaging app. However, she expressed the need to make it simpler for older users, such as step by step prompts on which buttons they should click to perform a certain function: "I’m actually quite impressed with the apps that I,…, about the wound care-thing. Uh, uh, I think it is, it's the simpler it is, the better it is because, like I said, most, most diabetic people with wounds are normally above 50 and above, most of the time."
"More information. Because it takes a long time for the wound to heal. Everybody wants to know how fast can you heal the wound and what other things can help. Which other things… I, I look forward to."
The participants also preferred to have more language options within the app to cater to users whose primary language is not English. In Singapore, it is not uncommon for patients with DFUs to hire foreign domestic helpers as carers. In these cases, English is usually not their first language, and more language options would definitely be beneficial. Hence, it is also important to look into providing language options for carers because as mentioned above, some patients with DFUs, especially those with physical disabilities, require their carers to help them take photos of their wounds.
Feasibility of using the wound imaging application
The theme of feasibility of using the app was gathered during the participants’ discussions. This is further crystallised into subthemes, such as acquiring the habit of taking wound images, acceptance and non-acceptance of the app usage, challenges in taking photos of the wound and assurance about the benefits and usage of the app. Most of the participants do not have the habit of taking pictures of their wounds. It was normally done by the podiatrist at the clinic or hospital during the visit. "So far it's all taken by the, the, the podiatrist, yeah."
"Only the, the doctors and the nurses do the taking of the photo."
This might be a potential barrier in the initial stages and it would be important to reduce the learning curve so that participants would be open to learning and developing the habit of taking images of their wounds. Despite this, when asked if they would be willing to learn how to use the application, most of the participants expressed acceptance and interest in using a wound imaging app that would help them in monitoring and taking care of their wound condition. Most patients agreed to follow up on doctor's instructions on taking photographs of their wound by using an app: "If I’m being told so, by my doctor or the specialist told me to do that, I think I would follow through… my personal, ah, conclusion is that I, would use the experts like doctors you know. Because they would be the best people to tell me how to manage."
Another subtheme uncovered by the study was the challenges in using the wound imaging app to capture images. In order for patients to take a photo of the wound on their foot, they would need to get into an ideal position and be able to visualise the wound relatively clearly. Most patients with visual impairment or other physical disabilities experienced challenges in taking photographs of the wound, especially since the wound is on the sole of foot. Because of these challenges, most patients revealed that they required support from family members, carers or HCPs. One participant explained that nurses and his children were primarily engaged in cleaning and dressing the wound: "My children, uh, my siblings, um, even the nurses, uh, those take care of me, … before the wound nurse we engage, before that, my daughter is the one who do the cleaning for me and dressing up the wound." "And due to their age:" "But very old people, those old-timers, maybe they have problem. Maybe their kids must help"
This view was also upheld by one of the carers of a patient with DFU: "Uh, I think uh, it's very difficult for her to take photos herself because she lost her, uh, right eyesight. […] So she cannot see very clearly. And then, uh, it's very hard for her to take a picture on her own."
This shows that it might be quite difficult for patients, especially the elderly or those with more disabilities, to take photos of their own wounds and might require help from a caretaker in order to take a clear and accurate picture of their wound.
Some patients mentioned that they would be more inclined to use the app if they understood how the app can benefit them. "I, I wouldn’t know [unclear] because I just take a picture and then I just compare. I don’t know how is that going to help me, help me, I don’t understand."
"How, how are you going to help us by taking photo? What other benefits I, I get and so on?"
Other patients needed assurance that they are using the app correctly before committing themselves to do it, possibly because they are afraid that they would jeopardise the clinical information given to HCPs that can in turn lead to poorer management of their DFU.
"If I learn how to, if I know how to use it, yes, I will do it."
Logistics of care
The logistics of care was another theme that was discussed by the participants. The first subtheme in logistics of care is on time saving and flexibility. Patients believed that such an app may allow them to save time normally spent making appointments or visiting the clinics for their dressings. During the COVID-19 pandemic, it may offer flexibility through remote monitoring by sharing the photographs of the wounds with HCPs without necessitating clinic visits: "Even sometimes, like, for, for this pandemic, if I have to stay home, I don’t go, so that at least I can still check on my wound more regularly." "But it will be much more better if you yourself go there and, uh, let the doctor look at it and take photos. I think it will… It, it really will help to see what really is lah… This [remote consultation] is the second, second option lah. If you cannot go then, you can use the Zoom lah or take photos lah."
An interesting finding is that younger patients tend to value the convenience of a wound imaging app, while older patients prefer having in-person interactions with their HCPs.
Healthcare providers
This study enrolled 20 HCPs, of whom six were primary care providers and 14 were tertiary care providers, including five surgeons, three primary care doctors, five nurses, five podiatrists, and two diabetologists (Table 3).
Characteristics of healthcare providers (HCP).
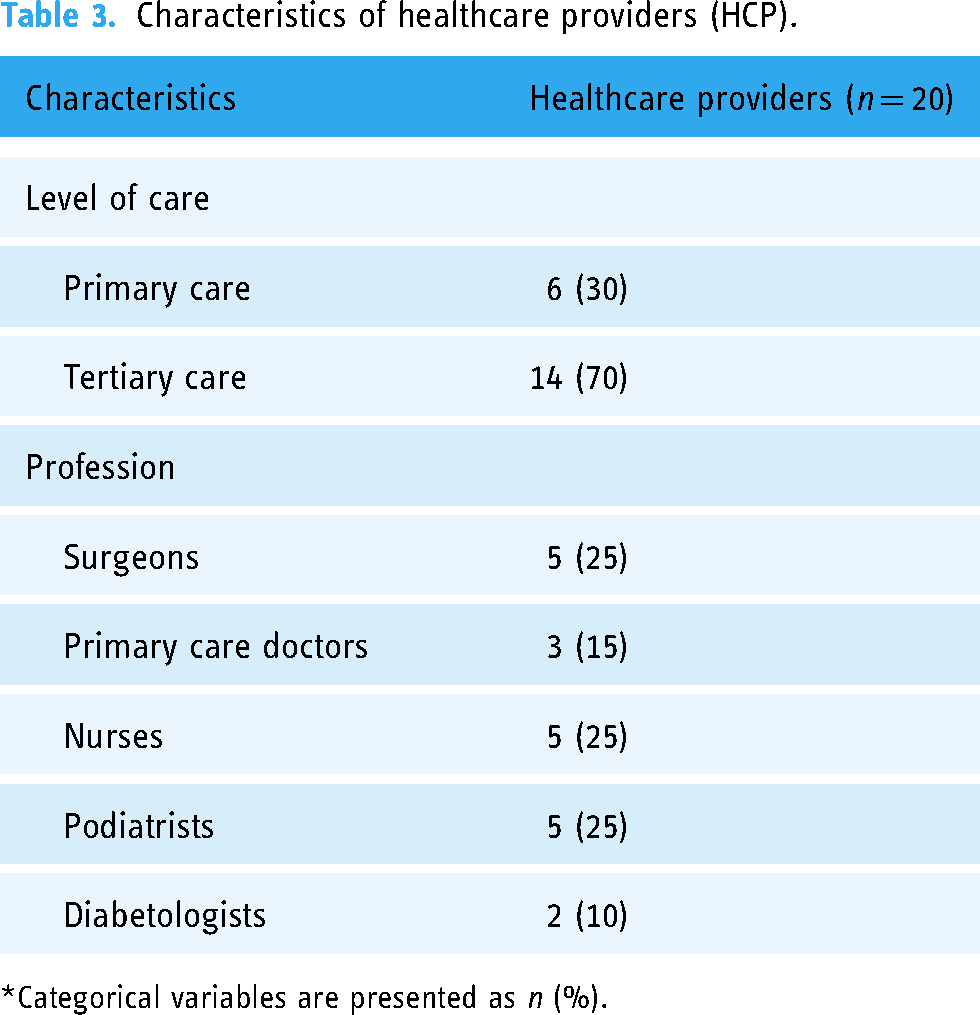
*Categorical variables are presented as n (%).
There were four major themes identified to address our research questions: (1) attitudes towards wound imaging application for RQ2, (2) preferences regarding functionality for RQ3, (3) perceived challenges for patients/carers and (4) perceived barriers for HCPs for RQ4. Table 4 summarises the key themes along with their subthemes and specific examples.
Themes with specific examples from healthcare providers (HCP).

Attitudes towards wound imaging application
The attitudes towards wound imaging applications were discussed, further broken down into the attitudes regarding the sharing of information among HCPs, quality of wound assessment and documentation, remote monitoring and early detection and the use of the application in promoting patients’ compliance. All HCPs were generally supportive of the wound imaging application.
HCPs agreed that wound images enable effective information sharing across various disciplines such as medical, nursing and podiatry. Additionally, it facilitates information sharing smoothly across institutions from primary care to tertiary care. This unfettered information sharing is important as DFU patients often alternate between primary and tertiary institutions for their wound care dressings and reviews. Currently, there is no wound imaging system shared securely within healthcare cluster's electronic medical records, and this will greatly enhance wound assessment and documentation.
"I actually… I think that having patient owning the app actually transcends all boundaries of IT barriers, so they can be from SingHealth cluster, NUH cluster. GPs who doesn’t own anything, they can all view the, the wound progression together with the patient."
"And it helps with our documentation, right, then I think that will help to save time. And if it synchronises well with the current electronic medical record system that we are using, then I think that, that would be very beneficial. And I think the AI, probably, has more standardized way, as compared to different clinicians […]"
"I, I think the, the big advantage is the fact that the wounds are serially documented. In a public healthcare setting, the doctor seeing it may not always be the same person who saw who saw previously. So, it is good to have the reference point, so yeah."
However, there was also some scepticism regarding the validity of the artificial intelligence.
"We must be reassured of the validity of the AI because I think there's quite a few systems out there, and some of them claim that they are able to classify the various structures. But if, if they even.. If they say they could, uh, how do I know that they really could identify the structures correctly."
HCPs felt that the regular and remote monitoring of DFU due to its convenience will enable early detection of wound deterioration. Additionally, it would also help save time for the patients and reduce waiting times in the hospital.
"Ah, actually a lot of the diabetic foot, it will be adequately managed at home if they are young, ah, and with the technology. They’re able to take accurate picture and send for reference or for some care advice. That’ll be great, because you find that they’re all working, and they got no time to actually come to hospital, and each time when they come to hospital, they have to wait a long time."
"Yes, because there are times where the patients cannot come for wound reviews or they have difficulty coming. Such apps would help us, as the other… The other people have mentioned, so early detection, uh, of any complications for the wounds."
Most also agree that proactive wound monitoring will help improve health literacy and promote patient compliance to wound care management as it encourages patients to take greater ownership of their condition.
"Actually, we empower the younger patient, and actually with this available, the photograph, to able to contact the healthcare ASAP. […] So, it would be good, so it would be good to actually have this system, to actually empower the patient to take care of themselves and have the healthcare system to actually support them at home."
Preferences regarding functionality
HCPs have various preferences regarding the functionality and features of the application, including in-app prompts, the AI's ability to identify wound characteristics and compare it with previous wounds, additional information for patients and adjustable app settings in terms of changing the language or increasing the font size. These preferences were mainly related to improving the user experience for the patient as well as the quality of medical information that they can get from the wound image, while not overloading the patient or the healthcare system.
There were also suggestions by HCPs to build prompts in the app to remind the patient-carers on wound care or wound imaging schedules. Additionally, some providers also felt that an SOS ‘return advice’ might be useful for the patient:
"You know they may forget about using it, I don’t know if anyone would be there to like, give them reminders, I think that might be helpful."
"I’m just thinking whether SOS kind of information would be useful, what do you look out for if you do see this, this, this, please approach your doctor, or something. Ya, so at least they know when to escalate, in terms of the deterioration of the wounds. […] Mm, I think if it's used correctly, then I think it would be useful."
On the other hand, there were also concerns that the SOS prompts may cause additional burden on the healthcare system if not implemented properly and unnecessarily triggered.
"It would place unnecessary stress. On the other hand, whoever is receiving the SOS."
"So, if… I mean, really, if there's a case for this SOS button, it's good to, maybe, have some questions prior to that, lah. Like are you experiencing any [unclear] or increasing discharges, and so on, before you press SOS button."
HCPs also felt that visual representations and identification of wound characteristics will inform patient-carers of their wound progress. As the wound is not visualised and examined in-person by the HCP, having the prompt and the ability to upload multiple images would allow a more accurate assessment of the wound, instead of just a single picture and view of the wound.
"Yeah I think sometimes when the, ah, especially if it's only one wound image, um, you don’t really get an accurate representation of what the wound may be like. […] So, I don’t know if like, you could add more pictures to it, like one of it, one of the wound, one of the foot, and then one of the front of the foot, then you may be able to understand a bit more about."
HCPs also opined that it would be beneficial for the application to help record details of the wound. In addition, suggestions were made for the app to have push notifications, upon receipt of wound updates to HCPs; email reports; dashboard; utilization of AI algorithms to highlight deteriorating wounds such as an increase in size, worsening wound characteristics or any reported symptoms such as pain, fever, smell, redness or discharge.
"I think the app itself, right, can, can help in recording the wound details, like the wound description, for example, how many percent granulation, how many percent slough, and identify bone."
Additionally, some HCPs wanted a functionality where they could compare the wounds with previous images to trend the patients’ recovery.
"But in terms of progress, will there be a graph to show, you know, the, the wound size coming down?"
"It will be good if the only measures can be set by the previous wound and the latest wound then you can at least visually compare. Then if the details of the wound can be also side by side, that’ll be very useful."
In terms of accessibility, providers were mainly concerned about whether patients and carers will be able to use the app with reference to language as well as text size. They suggested adding more languages, ability to increase font size as well as audio instructions.
"Because I think the ability to adjust the font size and choose the language, right, in the mother tongue, so it would be quite important."
"Um, but I think the problem is that those people with retinopathy, they probably can’t see very well. Like, the words or the instructions to follow, so maybe if you have, like, audio… Like, you know, an audio aspect to it, it might help lah."
With regard to additional features outside of wound imaging, most HCPs felt that the main aim of the application would be for the patient to document their own wound image.
Some HCPs also proposed that the app incorporate the diabetic and wound care plan, and provide some bite-sized information to help patients manage their diabetes and wound. They felt that providence of diabetic and wound care plans will help educate patients/carers and improve health literacy.
"I think some basic education would be good, but it's more that I think it shouldn’t be a new knowledge kind of thing. It should be for reinforcement because I suppose this group of patient would have seen a healthcare professional before embarking on this app, right? So it should be, like, basic diabetes… Uh, basic wound care… Wound care advice that they just need to follow. […] Um, I think diabetic care plan, it's, uh… It's good to have a brief overview for, for them lah so that they know how, um… You know, that all, all… Like, this… All these matters lah, you know, your blood sugar control."
"I think simple, bite-sized information like what dressing to use, when to change when it's soaked."
On the other hand, some felt that it is important to strike a balance so that it is not too overwhelming for the patient and that the application should focus on its main goal of wound imaging.
"Because if it's too overwhelming, sometimes, they would just decide not to receive any. Ya. So, for diabetic care plan, I mean, maybe not necessary for patient with wounds going on because it might be too much for them."
"I just want to see wound image. What dressing is being put on, and what is the plan for the wound. Because it is a wound app, need to focus the wound app."
Perceived challenges for patients/carers
Most HCPs were concerned with potential perceived challenges for patients/carers. These ranged from physical challenges due to the patients’ physical disabilities, to mindset challenges due to the patients’ hesitance or non-compliance to using the wound imaging app.
With regard to suitability of user, application adoption will require a select group of patients and carers who are willing, possess smartphone/internet access and able to be adequately trained. HCPs felt that this application might not be feasible for patients who have visual impairment or other comorbidities that may result in a poor quality photograph.
"Um, yeah, for the patients that I’m seeing, I think they would find it quite challenging, because they’ve got mobility issues, they can't bend, the eyesight is very poor as well, don’t know if they’ve got that kind of support."
"The patients… The patients who are suitable are those with very stable wounds. They come every one to two months just to ensure… Just for us to ensure that the wound is recovered. Wounds can partially be managed either by podiatrist or by the polyclinic nurses, so these are the subset of patients that are suitable. Those that are not suitable are those whereby the wounds are questionable and those who are pending amputation but patient is, like, deciding."
In terms of acceptability, most HCPs felt that the patients would appreciate the convenience of managing their wound from home:
"I definitely feels that, uh, our patients will see a role in having wound app in… Using wound app in future because we… For, for, for our team, we already have patient taking photo and send it, WhatsApp to us, and ask us for opinion on how to manage the wound […] This is the trend, and it actually minimise patient from coming back to hospital, so nowadays, patients are… They are very independent. They wanted to do their own self-care at home […]"
"And, and, also, on the receiving end for elderly, I’m not sure how receptive they are with regards to the tech itself. Because quite, quite a lot of elderlies, you know, they are still quite lacking in the tech idea."
This might pose as a significant problem because a large majority of the patient group is elderly.
"So, for the patient wise, I would say majority of our patient groups here, I mean, for diabetic, or our supervision, they are pretty old and, and lack of caregiver sometimes. So, I think the accepting level should be quite low in our Polyclinic."
Non-compliance is another important challenge that can hinder the effectiveness of the app. Most HCPs agreed that the app might suit individuals who are more compliant and tech savvy.
"So, those people who are quite engaged in, you know, their wound health status, probably would be useful. And of course, people who are tech savvy […]"
"However, there are a small subset of patients who have very poor compliance, very poor social support, and I would not recommend this for."
Perceived barriers for HCPs
There were several barriers that HCPs felt could limit the effectiveness of the wound imaging app. This included a wide range of factors, including integration with the existing healthcare system and cost to the quality of the wound image and risks of worsening patient outcomes if wound deterioration is missed.
Application compatibility with existing electronic medical records (EMR) system is a major concern, with all the HCPs concerned that more time would be needed to navigate the complex process of integrating the app to hospital's EMRs.
"Compatible or not with your system is another concern. So… And personally, I feel, also, whether it is really time-consuming, and all this thing is another issue for us because due to the patient load and everything."
"Time consumption is definitely an issue because from my understanding of previous platforms, because it's not that compatible, we actually have double work that we actually do some data entry into the app."
With regard to diagnostic accuracy, HCPs felt that the wound image quality, accuracy of wound description, measurements and additional wound-related questionnaires such as pain, fever, smell, redness and discharge will be pertinent. Some HCPs were concerned about how the quality of the camera, angle or lighting might affect the quality of the wound image and consequently the overall accuracy of the analysis.
"I feel that the person taking the, ah, ah, quality of the camera, how easy for the, how easy for the, the patient is the potential family member, can he actually reach and, and take a good shot of the wound. And also, ah, family member lighting may not be optimum and that can translate to poorer picture and affect the analysis."
"Uh, we need to be quite careful with that because I think, especially with diabetic foot ulcer, sometimes it's very… It's not very clear where the wound is, and sometimes without all the cleaning and debridement, you know, taking a photo of it doesn’t tell you much at all what's going on underneath."
Finally, there were also queries about the cost of the wound imaging system, both to the healthcare system and to the patients.
"Then I will also think that costs, whether there will be any cost impact. So, whether it's through organisation or through patients. Now, whether this additional cost of the tool will be transferred to the patients as well."
"And secondly, also, the maintenance of the system, whether or not it will take a lot of cost to maintain."
Discussion
In general, using a novel patient-owned wound imaging system for DFU monitoring is positively received and perceived to be feasible and efficacious in DFU care. Patients and carers were more focused on the benefits of convenience and potential time saved from wound imaging and remote monitoring. HCPs not only agreproed that there are benefits of convenience and reduced waiting times but were also excited about the possibility of sharing information with other HCPs for better continuity of care.
We also elicited several potential barriers that might reduce the adoption or effectiveness of a wound imaging app. Patients and carers were mostly focused on the general usability of the app, including uptake rate amongst the elderly. In our study, the elderly patients with diabetes tend to have more mobility, visual and language barriers. These challenges were also mentioned in previous studies and hence should be taken into account when developing this app.20,24,25 The ease of use was also an important factor found in previous studies to influence the rates of adoption especially among elderly patients.24,26,27 Ease of use can encourage early adoption among the elderly who are not well versed with technology. This can prevent early negative experiences that might deter the usage of the app. 28 These sentiments were also echoed by HCPs. Fortunately, most of these barriers have the potential to be resolved, for example, by adding different languages and creating a more user friendly application.
However, there were several barriers that will require some workarounds. Firstly, HCPs were concerned about the quality of the images and whether sufficient wound assessment can be achieved by visualisation alone without other factors such as temperature or smell. 19 Secondly, in concordance with other studies, 20 we found that some of the older patients preferred in-person interactions with their doctors and preferred face-to-face consultations. This could be because the elderly is not as pressed for time as compared with those who are still in the workforce and thus values in-person interactions with their doctors more. Lastly, some HCPs were concerned about the integration of the wound care app into the healthcare system's electronic medical records for documentation as well as the cost of maintaining the application. Although previous studies done in the Canadian healthcare system has found telemonitoring to be a cost-effective way for the management of DFU, 29 there has yet to be any studies done in the Singapore healthcare system.
Implications of wound imaging system
A shift in research priority from silo-ed hospital treatments to innovative integrated community prevention is critical to address the high DFU burden. The widespread uptake and acceptance of wearable and digital health technologies gives us an opportunity to empower patients in their self-care of DFUs and effectively implement remote monitoring. 30 It is anticipated that the technological apps may help patients with DFU to strengthen their communications with clinicians. 31 A wound app will allow the integration of data information through image capturing, sharing, checking, recording the progress and stimulate best practices of self-care. These attributes were followed by recommendations from associated studies.32–34 The findings of this study provide insights into the facilitators and barriers in the use of a wound imaging app for DFU management. Previous studies have found wound imaging systems to be useful adjuncts in the monitoring of DFUs with most of these systems reporting high accuracy in wound measurement, with some found to be superior to traditional methods of wound assessments. 35
Telemedicine in DFU care has also been well-received and found to be valid, reliable and feasible.36,37 While many of these technologies are still in infancy, the COVID-19 pandemic and current unmet needs to decentralise care for patients with DFU have accelerated the uptake of digital health, smart wearables, telehealth technologies and ‘hospital-at-home’ care delivery model. These technologies can potentially be adopted at scale to improve the remote management of DFUs by triaging those who need to be seen in outpatient or inpatient settings, and supporting acute or subacute care at home. 30 Hence, if future developments can integrate this app with the national electronic medical records system and increase uptake amongst local patients, patients will be empowered to monitor their own wounds but still have expedited clinical management when necessary. This will lead to improved patient outcomes and increased cost-effectiveness for the healthcare system.
Strengths and limitations
There are several strengths of this study. First, this study is based on a diverse sample of participants, including patients and carers from different backgrounds representing the multi-ethnic diversity of patients in the Singapore population. The interview with HCPs also included various perspectives by presenting the views of a multidisciplinary team including surgeons, primary care doctors, nurses and podiatrists, all of which play an important role in the management of DFU. This human-centred approach ensures that the needs and challenges of the various stakeholders involved in the management of DFU are taken into consideration in the development of the wound imaging app. The adoption of this co-design approach has been promoted to ensure that collective knowledge drives the improvement of healthcare.38,39 This would help to prevent potential problems like patients becoming too overburdened by the app and not using it entirely.40,41
However, one limitation of our study is that the participants were asked to provide their views on a patient-owned wound surveillance application that they had not yet had the opportunity to experience and their perceptions were based on the 1-min video of the app orientation as an example of a wound imaging app. Research suggests that behavioural intentions and views of digital technology can change as a result of experience with technology.42,43 Thus, the examination of participants’ actual experience with the app and their views before and after using it would have provided a more in-depth understanding of the app's acceptability and perceived benefits. Future studies could address this limitation by exploring participants’ views following their actual use of the app. Another limitation is that our study was theory-driven, guided by the authors’ clinical and research experience in DFU care. Although previous studies have used theoretical models such as the unified theory of acceptance and use of technology (UTAUT) and/or a mixed design to evaluate patients’ or HCPs’ views of digital technology, the use of such models within the literature for DFU care is limited.
Future directions
As part of the ePOWS study (efficacy of a patient-owned wound surveillance system for DFU care), we will utilise findings from the current study to customise the wound imaging app for use in the local population as a patient-owned wound imaging system for patients discharged from tertiary institutions, after diabetic limb salvage procedures and optimisation of wound care. Future research can also investigate the cost-effectiveness of a nationwide wound imaging app that integrates with the various healthcare clusters in Singapore to improve the continuity of care and ultimately better outcomes for patients.
Conclusion
Our study showed that patients, carers and HCPs are all positive to a patient-owned wound imaging system. These findings will help address concerns and tailor a DFU wound app suitable for implementation in the local population. As part of ePOWS study, we will proceed to clinically evaluate the efficacy of a patient-owned wound imaging system for patients with DFUs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231183544 - Supplemental material for Patients, carers and healthcare providers’ perspectives on a patient-owned surveillance system for diabetic foot ulcer care: A qualitative study
Supplemental material, sj-docx-1-dhj-10.1177_20552076231183544 for Patients, carers and healthcare providers’ perspectives on a patient-owned surveillance system for diabetic foot ulcer care: A qualitative study by Zhiwen Joseph Lo, Bryan Chong, Elaine Tan, Desmond Ooi, Huiling Liew, Wai Han Hoi, Yuan Teng Cho, Kyle Wu, Naren Kumar Surendra, Maleyka Mammadova, Audrey Nah, Victor Goh and Josip Car in DIGITAL HEALTH
Footnotes
Acknowledgements
The study team wish to thank the efforts of the patients with diabetic foot ulcers and their carers for participating in the interviews. The authors also wish to thank the efforts of the healthcare providers who are involved in diabetic foot ulcer care (Dr Hong Qiantai, Dr Liew Huiling, Dr Zhang Li, Dr James Siow Wei Xuan, Ms Lai Peiting, Ms Tan Hui Min, Ms Tiffany Chew Wen Ying, Mr Kenneth Koh Shi’En, Dr Desmond Ooi Guo Shen, Dr Jeremy Hoe Kian Ming, Dr Shaun Chan Wen Yang, Ms Ang Poh Lian, Ms Chelsea Law Chiew Chie, Ms Wong Wan Mun, Dr Elaine Tan Yu Ling, Dr Jonathan Chong Ern-Ji, Dr Loh Yi Bing, Ms Su Jie, Ms Lee Jiayu Samantha and Mr Nicholas Andrew Hulme) for participating in the interviews.
Contributorship
Conceptualization and design: ZJL, BC, ET, DO, HL, WHH, KW and JC. Acquisition of data: ZJL, BC, YTC, NKS, MM, AN and VG. Analysis and interpretation of data: ZJL, BC, YTC, KW, NKS, MM, AN, VG and JC. Supervision: ZJL, ET, DO, HL, WHH, KW and JC. Validation: ZJL, BC, ET, DO, HL, WHH, YTC, KW and JC. Writing – original draft: ZJL and BC. Writing – review & editing: ZJL, BC, ET, DO, HL, WHH, YTC, KW, NKS, MM, AN, VG and JC. All authors approved the final version of the manuscript, including the authorship list and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KW is Chief Medical Officer at eKare Inc. (USA).
Ethical approval
Ethics approval was obtained from the local institutional ethics board (DSRB ref: 2020/01347).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Science, Technology and Research (A*STAR) Skin Research Institute of Singapore Skin Innovation Grant (SIG2002). eKare Inc matched funding to Skin Innovation Grant (eKare had no role in the design, execution, analysis or publication of this study). National Research Medical Council (NMRC) Research Training Fellowship Award (FLWSHP19nov-0015).
Guarantor
ZJL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.