
Abstract
Background
This study aimed to systematically review randomized controlled trials evaluating the effectiveness of web- and app-based health management interventions for patients at high risk of stroke, including those with cardiovascular disease, type 2 diabetes, or obesity. Clinical outcomes (blood pressure and glycated hemoglobin), self-management knowledge, health behaviors, and quality of life were examined.
Methods
Following PRISMA guidelines, we searched PubMed, Web of Science, CINAHL, and the Cochrane Library for randomized controlled trials published between January 2010 and December 2024. Search terms included combinations of “Hypertension,” “Diabetes Mellitus,” “Myocardial Infarction,” “Obesity,” “Mobile Applications,” and “Web-Based Intervention.” Studies that provided sufficient data for quantitative synthesis were included in the meta-analysis. Pooled effect sizes were calculated using RevMan 5.4, and subgroup analyses were conducted based on intervention duration.
Results
Thirty-five studies met the inclusion criteria. Meta-analysis revealed that web- and app-based interventions significantly improved blood pressure, glycated hemoglobin level, and medication adherence among individuals at high risk of stroke. These interventions also enhanced quality of life and increased self-management knowledge and behaviors. Subgroup analyses of web- or app-based educational programs indicated that clinical indicators improved with interventions lasting 3 months, whereas self-management knowledge, behaviors, and depression symptoms showed significant improvements with 6-month interventions.
Conclusion
This study demonstrates that web- and app-based health management interventions yield improvements in clinical, psychological, and behavioral outcomes for patients at high risk of stroke. These findings provide evidence for the development and implementation of tailored digital health interventions for effective stroke prevention and chronic disease management.
Keywords
Introduction
Stroke occurs when a cerebral blood vessel becomes suddenly occluded (ischemic stroke) or ruptures (hemorrhagic stroke), resulting in blood flow interruption and subsequent damage to the brain tissue. Globally, 1 stroke is the second leading cause of death and a major contributor to long-term disability, often requiring temporary or lifelong caregiving support and imposing substantial burdens on patients and their families. 2 In South Korea, the prevalence of stroke continues to rise, with approximately 630,000 individuals living with stroke as of 2022, and this number increases each year. 3 Older adults are disproportionately affected, with individuals in their 60s, 70s, and ≥80 years accounting for 22.6%, 26.3%, and 26.5% of cases, respectively. 4 Given the nation’s rapidly aging population, the burden of stroke is expected to increase in the coming decades.
Stroke can lead to a range of neurological sequelae, including motor paralysis, sensory deficits, aphasia, and dysphagia. 5 Timely emergency treatment is the most critical determinant of prognosis, as it can substantially reduce disability 6 ; however, only 40% of stroke patients in Korea arrived at the emergency department within the “golden window” of 3 hours after symptom onset in 2021. 4 This highlights ongoing challenges in ensuring timely recognition of and response to acute stroke symptoms.
Chronic conditions such as hypertension, diabetes mellitus, obesity, and cardiovascular disease are well-established risk factors for stroke. These underlying conditions contribute to endothelial dysfunction, atherosclerosis, and thrombus formation, impairing cerebral blood flow or directly damaging blood vessels and increasing the likelihood of stroke. Effective prevention requires comprehensive management of these risk factors and encompasses primary prevention—reducing the likelihood of first-ever stroke—and secondary prevention—preventing recurrence and complications after an initial event. Early recognition of warning signs and consistent daily management of key modifiable risk factors, including hypertension, diabetes, and obesity, are essential strategies for lowering stroke incidence. 5
The widespread adoption of the World Wide Web and advances in information and communication technologies since the 1990s have enabled people to access information in real time and communicate with unprecedented ease. 7 These developments have facilitated the rapid expansion of health-related websites and mobile applications, creating an environment in which individuals can monitor and manage their health without in-person clinical visits. Although health promotion in the 1970s and 80s largely focused on one-way information delivery to selected populations, the paradigm shifted toward digitally supported, self-directed health management and personalized health record systems in the 1990s. 8
Several studies have examined web- and app-based health management interventions for individuals with hypertension, diabetes, or obesity and reported improvements in clinical outcomes such as blood pressure, glycated hemoglobin levels, and body weight, as well as enhanced adherence to recommended health behaviors.9–12 Recent systematic reviews and meta-analyses further support these findings. For example, de Souza Ferreira et al. 13 reported significant reductions in glycated hemoglobin levels in a meta-analysis of RCTs; Liu et al. 14 found improvements in glycated hemoglobin and blood pressure in app-based self-management interventions; Mao et al. 15 demonstrated beneficial effects of mobile health interventions on glycated hemoglobin and systolic blood pressure; and Wang et al. 16 reported reductions in glycated hemoglobin levels and body weight in individuals with diabetes or obesity.
Although the focus of disease management differs across conditions, digital interventions—whether delivered via websites or mobile applications—typically encompass dietary counseling, physical activity support, and medication monitoring and education, and have demonstrated varying degrees of effectiveness depending on their specific design. Importantly, intervention duration is a critical determinant of effectiveness. Extremely short interventions may be influenced by temporary Hawthorne effects, in which behavioral changes arise from a heightened awareness of being observed, while the formation of stable health-related habits generally requires at least 2 months of consistent effort. 17 However, most previous systematic reviews have primarily focused on overall intervention effects and have rarely examined how the duration of digital health programs influences different health outcomes. Consequently, evidence remains limited regarding the optimal duration of digital health interventions needed to achieve sustained behavioral change or clinical improvement.
To address these gaps, the present study systematically reviewed RCTs conducted between 2010 and 2024 that evaluated web- or app-based health management interventions for individuals at high risk of stroke, specifically those with cardiovascular disease, type 2 diabetes, or obesity. We synthesized the effects of these interventions on a comprehensive range of outcomes, including clinical indicators such as blood pressure, glycated hemoglobin level, and medication adherence, as well as psychosocial outcomes such as self-management knowledge, health behavior, QoL, depression, and anxiety. In particular, subgroup analyses were conducted according to intervention duration to examine how the length of digital interventions affects different categories of outcomes. These findings aim to provide evidence-based guidance for designing and implementing tailored digital health programs for patients at high risk of stroke.
Methods
The review process followed the methodological guidance outlined in the Cochrane Handbook for Systematic Reviews of Interventions 18 and adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting standards. 19 The protocol for this systematic review and meta-analysis was prospectively registered in PROSPERO (registration number: CRD420251021375).
Search strategy
We systematically searched PubMed, Web of Science, CINAHL, and the Cochrane Library, and additionally performed manual searches using Google Scholar. Eligible studies were limited to peer-reviewed articles published in English between January 1, 2010, and December 31, 2024. The search strategy incorporated combinations of the following keywords and MeSH terms: “Hypertension,” “Diabetes Mellitus,” “Myocardial Infarction,” “Obesity,” “Mobile Applications,” “Web-Based Intervention,” “Randomized Controlled Trial,” and “Controlled Clinical Trial.” All retrieved records were managed using Microsoft Excel.
To ensure accuracy and objectivity, two reviewers independently screened the studies. The selection process was conducted in two stages. In the first stage, titles and abstracts were screened to exclude studies that did not utilize a cluster randomized trial (CRT) or RCT design or that did not target individuals with cardiovascular disease (including hypertension and myocardial infarction), type 2 diabetes, or obesity. Studies that examined telemedicine alone or interventions delivered exclusively via telephone or text messaging were also excluded. In the second stage, the full texts of the studies that passed the initial screening were reviewed, and studies were excluded if they used a single-group design, were published only as conference abstracts, or were written in languages other than English.
Eligibility criteria (PICO-SD)
The inclusion criteria for this review were defined according to the PICO-SD framework: (a) Population: adults at high risk of stroke, including individuals with cardiovascular disease, type 2 diabetes, or obesity. (b) Intervention: studies that implemented a web-based or app-based health management education or intervention program. (c) Comparison: usual care or educational materials delivered through standard non-digital formats (e.g., printed brochures). (d) Outcomes: primary outcomes included blood pressure, glycated hemoglobin (HbA1c), and medication adherence. Secondary outcomes included cholesterol levels, body weight, BMI, QoL, disease-related knowledge and self-management behaviors, and physical activity. (e) Study Design: CRTs or RCTs involving populations at high risk of stroke.
Data extraction
Data extraction was conducted independently by two reviewers using a standardized data extraction form. The following information was extracted from each study: author and publication year, participant characteristics and sample size, intervention group, control group, intervention duration, and reported outcomes. Quantitative data required for the meta-analysis (e.g., means, standard deviations, and sample sizes) were also extracted when available. Information relevant to the risk-of-bias assessment was also extracted. Any discrepancies between the two reviewers were resolved through discussion, and when consensus could not be reached, a third reviewer made the final decision.
Statistical analysis
Meta-analyses were conducted using studies that provided sufficient quantitative data on outcomes (e.g., event counts, means, standard deviations, and sample sizes). For outcomes assessed using different measurement scales—such as disease-related knowledge, self-management behaviors, medication adherence, and depression symptoms—we calculated effect sizes using SMDs. Mean differences (MDs) were used for outcomes measured consistently across studies, including glycated hemoglobin, body weight, and BMI.
Given the expected heterogeneity across studies in terms of participant characteristics, intervention modalities, and study settings, a random-effects model was applied in all analyses18. Statistical heterogeneity was assessed using Higgins’ I2 statistic, with values interpreted as follows: 0%, no heterogeneity; 25%, low heterogeneity; 50%, moderate heterogeneity; 75% high heterogeneity. 18 In addition, subgroup analyses were conducted to examine differences in intervention effectiveness according to the duration of the digital health programs.
Meta-analyses were performed using Review Manager (RevMan), version 5.4. Sensitivity analyses were conducted using a leave-one-out approach to assess whether the pooled effect sizes were disproportionately influenced by any single study, and were performed using R software (version 4.5.1).
Results
A total of 4,578 records related to web- or app-based health management interventions were identified through the database search. After removing 446 duplicates, 4,132 records remained for screening. Based on the predefined inclusion and exclusion criteria, 3,905 studies were excluded during the initial title and abstract screening, and an additional 192 studies were excluded after full-text review. Ultimately, 35 studies met the eligibility criteria and were included in the systematic review. The detailed study selection process is illustrated in the PRISMA flow diagram (Figure 1). PRISMA flowchart of the study selection procedure.
Study characteristics
General characteristics of web- or app-based health management interventions for patients at high risk of stroke.
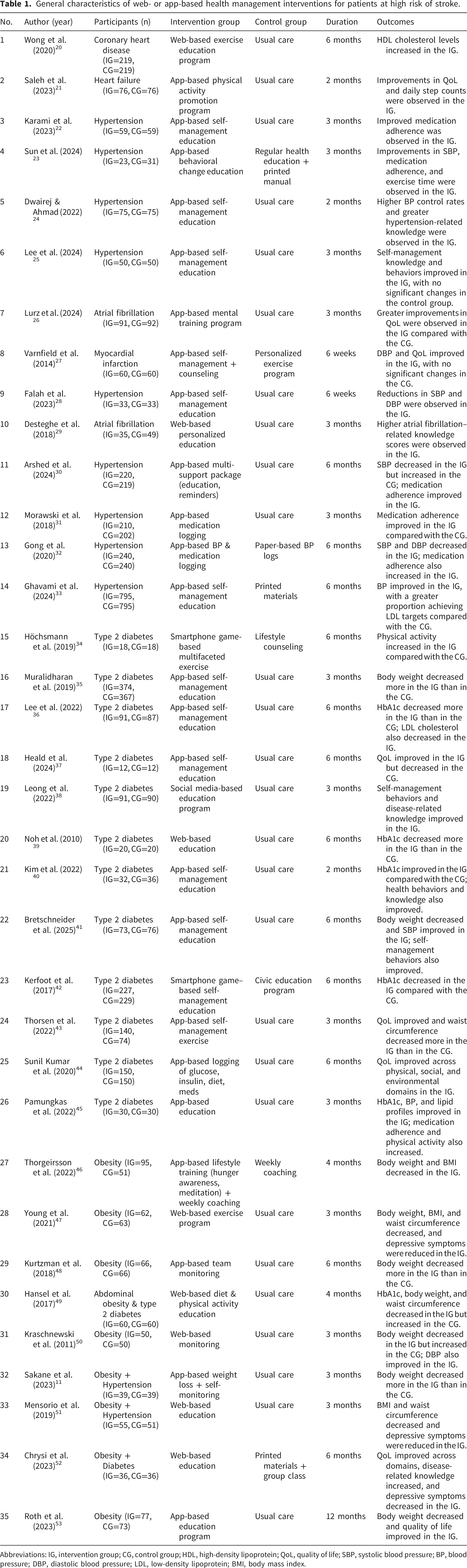
Abbreviations: IG, intervention group; CG, control group; HDL, high-density lipoprotein; QoL, quality of life; SBP, systolic blood pressure; BP, blood pressure; DBP, diastolic blood pressure; LDL, low-density lipoprotein; BMI, body mass index.
Various types of web- or app-based interventions were implemented in the included studies. Educational programs were the most frequently used intervention type (22 studies20,22–25,28–30,33,35–42,45,49,51–53). Other intervention types included physical activity programs (4 studies21,34,43,47), medication logging or monitoring programs (3 studies31,32,44), psychological training or counseling programs (3 studies26,27,46), and weight-monitoring or weight-management programs (3 studies11,48,50).
The duration of interventions varied across the studies, with the most common durations being 3 months (14 studies) and 6 months (13 studies), followed by 2 months (3 studies), 4 months (2 studies), 6 weeks (2 studies), and 12 months (1 study).
Risk of bias
Six studies (17.1%) showed a risk of bias in the randomization process domain due to incomplete randomization of subjects 18, 19, 22, 26, 37, 51. Some concerns is defined as at least one domain having some concerns without a high risk of bias for any domain (Figure 2). Risk of bias.
Meta-analysis results
Primary outcomes (blood pressure, glycated hemoglobin, and medication adherence)
Web- and app-based health management interventions demonstrated significant improvements in blood pressure among individuals at high risk of stroke (systolic blood pressure: SMD = –0.54, 95% CI: –0.82 to –0.26, p < .001; diastolic blood pressure: SMD = –0.39, 95% CI: –0.77 to –0.01, p = .05). The pooled analysis also showed a significant reduction in glycated hemoglobin levels (MD = –0.65, 95% CI: –0.94 to –0.35, p < .001). Heterogeneity was high for blood pressure outcomes (Higgins’ I2 > 70%) and low for glycated hemoglobin (I2 = 32%) (Figure 3). Forest plot of the effects of web- and app-based health management interventions in patients at high risk of stroke.
Additionally, web- and app-based interventions significantly improved medication adherence (SMD = 1.29, 95% CI: 0.55 to 2.03, p < .001), although heterogeneity for this outcome was also high (Higgins’ I2 > 70%).
Secondary outcomes (cholesterol, body weight, BMI, quality of life, disease-related knowledge, and physical activity)
Digital health interventions significantly increased high-density lipoprotein (HDL) cholesterol (SMD = 2.31, 95% CI: 0.71 to 3.91, p < .001), whereas no significant effect was observed for low-density lipoprotein (LDL) cholesterol (MD = –10.05, 95% CI: –27.78 to 7.67, p = .27). Significant improvements were also found in body weight and BMI (body weight: MD = –1.96, 95% CI: –2.79 to –1.14, p < .001; BMI: MD = –1.08, 95% CI: –1.26 to –0.90, p < .001). However, there was no significant effect on WC (SMD = –0.54, 95% CI: –1.32 to 0.25, p = .18). Heterogeneity was high for HDL, LDL, body weight, and WC (Higgins’ I2 > 70%), whereas no heterogeneity was observed for BMI (I2 = 0%) (Figure 3).
Web- and app-based interventions meaningfully increased physical activity levels (SMD = 1.88, 95% CI: 0.99 to 2.78, p < .001) and improved disease-related knowledge (SMD = 0.89, 95% CI: 0.30 to 1.48, p < .01). Self-management behaviors also improved significantly (SMD = 0.27, 95% CI: 0.06 to 0.48, p < .05). Heterogeneity was high for physical activity levels and disease-related knowledge (Higgins’ I2 > 70%) and moderate for disease-related behaviors (I2 = 57%) (Figure 3).
Furthermore, the interventions significantly improved QoL (SMD = 0.99, 95% CI: 0.65 to 1.32, p < .001). In contrast, depression symptoms showed significant improvement in the control group, resulting in no overall intervention effect (SMD = 10.75, 95% CI: 6.20 to 15.30, p < .001). Heterogeneity was high for both QoL and depressive symptoms (Higgins’ I2 > 70%) (Figure 3).
Sensitivity analyses
Overall, sensitivity analyses using a leave-one-out approach indicated that the pooled estimates for systolic blood pressure, glycated hemoglobin, medication adherence, body weight, physical activity, and QoL remained statistically significant and stable across iterations. The pooled estimate for HDL also maintained consistent direction and statistical significance, although only two studies were available. In contrast, the pooled estimates for diastolic blood pressure, BMI, disease-related knowledge, and self-management behaviors showed attenuation of statistical significance in some iterations. The findings for WC, LDL, and depressive symptoms were particularly sensitive to the exclusion of individual studies and should therefore be interpreted with caution.
Subgroup analysis by intervention duration for web- and app-based educational programs
Subgroup analyses were conducted according to the intervention duration for educational programs, which represented the most frequently used type of digital health intervention. Outcomes with insufficient data for comparisons across time frames—specifically WC, BMI, body weight, physical activity, and QoL—were excluded from the subgroup analysis.
Primary Outcomes (Blood Pressure, Glycated Hemoglobin, and Medication Adherence; Figure 4)
When web- or app-based health management interventions were delivered for 3 months, significant improvements were observed in blood pressure among individuals at high risk of stroke (systolic blood pressure: SMD = –0.65, 95% CI: –1.03 to –0.27, p < .001; diastolic blood pressure: SMD = –0.55, 95% CI: –1.07 to –0.03, p = .05). A statistically significant reduction was also found in glycated hemoglobin levels (MD = –1.29, 95% CI: –2.56 to –0.02, p = .05) (Figure 4). Subgroup analysis of intervention duration in web- and app-based education programs.
In addition, both 3-month and 6-month interventions significantly improved medication adherence (3-month: SMD = 1.49, 95% CI: 0.69 to 2.30, p < .001; 6-month: SMD = 1.67, 95% CI: 1.45 to 1.89, p < .001) (Figure 4).
Secondary outcomes (cholesterol, disease-related knowledge, and depression; Figure 4)
Three-month interventions resulted in significant improvements in both LDL and HDL cholesterol levels (LDL: SMD = –20.47, 95% CI: –34.30 to –6.64, p < .01; HDL: SMD = 1.49, 95% CI: 0.91 to 2.06, p < .001) (Figure 4).
However, improving disease-related knowledge (SMD = 1.75, 95% CI: 1.36 to 2.14, p < .001) and self-management behaviors (SMD = 0.28, 95% CI: 0.01 to 0.56, p < .05) required longer interventions. The effects of these outcomes were significant only when programs were delivered for at least 6 months. Furthermore, depression symptoms reduced significantly following 6-month interventions (SMD = –0.53, 95% CI: –1.00 to –0.06, p < .05) (Figure 4).
Discussion
The purpose of this study was to comprehensively examine whether web- and app-based health management interventions improve key clinical indicators among individuals at high risk of stroke. These indicators included blood pressure, glycated hemoglobin, and cholesterol levels. The study also evaluated whether such interventions enhance QoL, disease-related knowledge, and self-management behaviors. As noted earlier, primary prevention plays a critical role in delaying or preventing the onset of stroke by managing modifiable risk factors. In contrast, secondary prevention is essential for reducing recurrence and long-term complications among individuals who have already experienced stroke. In this context, we systematically reviewed RCTs published between January 1, 2010, and December 31, 2024. These trials evaluated digital health interventions targeting this high-risk population. We then conducted a meta-analysis to quantify their pooled effects. Subgroup analyses were also performed to explore the optimal intervention duration required to achieve clinically meaningful improvements.
First, web- and app-based health management interventions were identified as effective non-face-to-face strategies for improving major clinical outcomes. These included blood pressure, glycated hemoglobin, and cholesterol levels. The interventions also strengthened self-management capacities, such as maintaining physical activity and controlling body weight. These findings suggest that digital interventions empower patients to access tailored health information anytime and anywhere. They also enable patients to monitor their health status and initiate behavioral changes more easily.
Our findings are consistent with those of previous meta-analyses. For example, Liu et al. 14 reported significant reductions in glycated hemoglobin levels and blood pressure among patients receiving app-based self-management interventions, along with improvements in fasting blood glucose level and WC. Similarly, multiple systematic reviews have shown that mobile health interventions provide additional benefits beyond standard care. These benefits include greater reductions in glycated hemoglobin levels (approximately 0.3–0.5 percentage points) and additional weight loss (1–2 kg). 16 A notable advantage of web- and app-based platforms is their ability to deliver personalized and multidimensional management. This is achieved through tailored feedback and actionable behavioral guidance derived from patients’ health data. 14 By continuously recording and visualizing key health indicators, such as blood pressure, blood glucose, and medication adherence, patients may gain greater awareness of their risk status and be more motivated to sustain appropriate behaviors.
Furthermore, digital health interventions may serve as an especially valuable alternative for patients living in rural or medically underserved areas or for individuals with limited mobility, by offering high accessibility and continuity of care. Therefore, a single short-term intervention is likely insufficient to enhance self-management capabilities among high-risk individuals with chronic conditions. Instead, long-term engagement, supported by continuous digital services and regular monitoring, is essential. Such sustained approaches are crucial for maintaining and amplifying the long-term effectiveness of digital health interventions.
Second, the findings indicate that the effectiveness of web- and app-based health management interventions varies according to their duration. In the subgroup meta-analysis, short-term interventions of approximately 3 months yielded significant improvements in several clinical indicators. These interventions were particularly effective when delivered as educational programs. Improvements were observed in blood pressure, glycated hemoglobin level, medication adherence, and LDL cholesterol level. In contrast, cognitive and behavioral outcomes, such as disease-related knowledge and self-management behaviors, showed significant improvements only when the interventions were sustained for at least 6 months. This pattern suggests that the pace and extent of improvement differ according to the type of outcome. Physiological outcomes, such as blood pressure and glycemic control, can respond relatively quickly. Therefore, they are amenable to short-term, intensive interventions. However, outcomes that involve habit formation and behavioral change require prolonged and repeated engagement. Such outcomes include self-management skills and lifestyle modification, which typically need sustained participation to achieve meaningful improvement.
This trend is consistent with previous research. Liu et al. 14 noted that although short-term app-based interventions improved several clinical indicators, evidence regarding changes in patients’ knowledge, exercise adherence, and mental health was inconsistent and required further validation. These findings underscore the importance of aligning intervention duration with its primary goals. If the objective is to improve clinical indicators, such as blood pressure, glycemic control, or LDL levels, a short-term intensive intervention may be sufficient, provided that follow-up monitoring or booster education sessions are incorporated to sustain the effect. Conversely, when the aim is to enhance self-management knowledge and behaviors, long-term progressive interventions are needed to provide participants with repeated learning opportunities and adequate time to practice and internalize new habits. Supplementary strategies may also be necessary to support sustained behavior change. For short-term programs, this may include post-intervention follow-up. For long-term programs, motivation-enhancing and feedback mechanisms may be required.
In addition, individuals at high risk of stroke often have multiple comorbid conditions, such as hypertension, diabetes, or obesity. These overlapping conditions necessitate tailoring intervention content to the specific combination of diseases each patient presents. For example, patients with both hypertension and diabetes may require enhanced monitoring of blood pressure and blood glucose, along with more intensive education on medication adherence. In contrast, patients who also present with obesity may benefit from additional dietary counseling and structured exercise guidance for weight management. Therefore, personalized intervention strategies that adjust content and duration based on disease profile, disease severity, health literacy, and individual self-management goals are essential.
Prior literature also highlights the importance of tailoring digital health interventions based on participant characteristics, including customizing message content and optimizing intervention frequency to maximize engagement and outcomes. 16 Furthermore, the effectiveness of such tailored digital interventions is likely to increase when they are integrated into existing health management infrastructure. This infrastructure includes public health centers, hospitals, and community-based care organizations that can provide continuous support and follow-up. From a policy perspective, it is crucial to establish systems that enable long-term access to digital services for high-risk patients with multiple chronic conditions while simultaneously improving access to digital devices and strengthening digital health literacy among vulnerable populations.
Third, the effects of digital health interventions on mental health outcomes, particularly depression symptoms, varied depending on the duration and components of the intervention. Although the overall analysis did not show statistically significant effects of web- or app-based interventions on depression, subgroup analyses revealed meaningful reductions in depression symptoms. These reductions were observed in studies that implemented web-based educational programs lasting at least 6 months. This suggests that short-term information delivery may be insufficient to induce emotional change. In contrast, sustained and structured education and support can deepen patients’ understanding of their condition and enhance their self-regulatory capacity. These processes may ultimately contribute to emotional stability.
This pattern was supported by findings by Chrysi et al. 52 Their RCT demonstrated that a 6-month web-based education program improved participants’ chronic disease-related knowledge and self-management abilities. It also alleviated negative illness perceptions and stigma, resulting in reduced depression symptoms. These results indicate that digital interventions must extend beyond unidirectional information provision. Meaningful improvements in mental health require cognitive shifts and emotional recovery facilitated by education and ongoing support.
Furthermore, certain components of digital interventions—such as personalized messaging and peer interaction—have been shown to strengthen motivation for self-management and provide emotional support, thereby improving psychological outcomes, including depression. 54 Recent studies have emphasized that online support groups and community engagement can positively influence social well-being and promote sustained behavioral change. These findings highlight the importance of integrating interactive features, feedback mechanisms, and psychological reinforcement into digital health programs. 55 Consequently, digital interventions designed for high-risk individuals with chronic conditions should incorporate emotional support features, including peer-to-peer interactions through online communities or social media platforms, to foster encouragement, shared experiences, and enhanced long-term engagement. Such psychosocial design elements may not only promote sustained participation but also maximize improvements in mental health outcomes, including reducing depression symptoms.
Although a growing body of research has examined the short- and long-term effects of web- and app-based health interventions, further evidence is needed to inform more rigorous and broadly applicable prevention strategies. Future studies should consider participant characteristics, psychological and behavioral factors, appropriate intervention targets, and optimal intervention durations when designing digital health programs. In this regard, the present study serves as an important starting point for addressing these gaps.
This study had several limitations. First, considerable heterogeneity existed across the included studies in terms of intervention type (web- or app-based), target condition (cardiovascular disease, diabetes, or obesity), and outcome measures, which warrants caution when interpreting the pooled effect sizes. Second, subgroup analyses were conducted only for educational program interventions, which constituted the most frequently studied intervention type. However, the limited number of available studies prevented subgroup analyses of other outcomes, such as WC, BMI, body weight, physical activity, and QoL. Third, publication bias was not formally assessed because the number of studies included in each meta-analysis was fewer than 10, which limits the reliability of such assessments. Therefore, future research should include a larger body of evidence to enable more comprehensive comparisons across intervention modalities and durations, particularly for secondary and behavioral outcomes.
Conclusion
This study systematically evaluated the effectiveness of web- and app-based health management interventions for individuals at high risk of stroke using evidence published over the past 15 years. The analysis examined multidimensional outcomes. These included clinical indicators such as blood pressure and glycated hemoglobin, as well as psychological and behavioral outcomes including depression symptoms, self-management knowledge, and health-related behaviors. Subgroup meta-analyses of studies employing web- or app-based educational programs further identified the intervention durations that were most effective in improving specific outcomes.
Taken together, these findings provide foundational evidence for the development of digital health interventions. They also inform the practical implementation of programs designed to support the physical, psychological, and social well-being of individuals at high risk of stroke. Well-designed and tailored web- and app-based programs are promising integral components of comprehensive stroke prevention and chronic disease management strategies.
Footnotes
Ethical considerations
This study is a systematic review and meta-analysis based solely on previously published research and did not involve individual patient data; therefore, institutional review board (IRB) approval was not required. To ensure methodological transparency and avoid unnecessary duplication, the review protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD420251021375).
Author contributions
Conceptualization, S.K.K., Y.S.H., and H.S.J.; Methodology, S.K.K. and Y.S.H.; Formal Analysis, S.K.K.; Investigation, S.K.K. and Y.S.H.; Writing—Original Draft Preparation, S.K.K.; Writing—Review & Editing, Y.S.H. and H.S.J.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (RS-2024-00461755).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This study used only publicly available published data. Extracted datasets and analytic codes are available from the corresponding author upon reasonable request.
AI disclosure statement
No artificial intelligence (AI) tools were used in the preparation of this manuscript.