
Abstract
Objective
This study aimed to synthesize and analyze the evidence on the effectiveness of telerehabilitation categorized according to the International Classification of Functioning, Disability, and Health (ICF) outcomes for physical therapy (PT) during the coronavirus disease 2019 (COVID-19) pandemic.
Methods
Studies were identified using the Physiotherapy Evidence Database (PEDro), Scopus, PubMed, EMBASE, and other sources of data. Randomized controlled trials comparing telerehabilitation with the control group (i.e., no treatment/usual care) were included. Standard meta-analysis techniques were applied to assess the effectiveness of telerehabilitation. Outcome measures were categorized according to the domains of the ICF.
Results
Among the 134 studies that met the eligibility criteria, the majority of findings demonstrated significant improvements across all domains of the ICF following telerehabilitation as compared to the control group, regardless of participant groups. Only 9 of 134 studies were included in the meta-analysis. Six studies enrolled individuals with COVID-19 and the remaining three enrolled individuals with knee osteoarthritis (OA) who were unable to access services at the clinic. Compared with the control group, the Borg-Rating-of-Perceived-Exertion scale, as reflected in an impairment domain, was significantly lower in individuals with COVID-19 who received telerehabilitation (3 studies, n = 135; standardized mean difference (SMD) −1.82, 95% CI −2.77 to −0.86). Compared with that in the control group, 30-second sit-to-stand test (3 studies, n = 122; SMD 0.88, 95% CI 0.52–1.25) and 6-minute-walking test (4 studies, n = 221; SMD 0.83, 95% CI 0.42–1.24), as reflected to an activity domain, showed significant improvement in the telerehabilitation group. Conversely, there was no effectiveness of telerehabilitation on an activity domain as measured by the timed up and go test in people with knee OA (3 studies, n = 111; SMD −0.45, 95% CI −1.19 to 0.30).
Conclusion
This study provides evidence supporting the effectiveness of telerehabilitation across all domains of the ICF, with significant improvements observed in the impairment and activity domains for individuals with COVID-19. These improvements are particularly evident in the meta-analysis findings such as perceived exertion, leg strength, and functional capacity.
Introduction
Trends in the utilization of telerehabilitation have shown a significant increase when comparing the period before the pandemic to the coronavirus disease 2019 (COVID-19) pandemic period.1–3 Specifically, the use of video calls has increased more than triple compared to the period before the COVID-19 pandemic. 3 Importantly, the majority of patients who received telerehabilitation reported satisfaction with its effectiveness in delivering care and being evaluated and treated through telerehabilitation. 4 Users suggested that they were positive about the role of telerehabilitation including the convenience and lower cost for service users, the higher dose of therapy possible, and increased access for people in remote areas. 5 According to the COVID-19 outbreak spread throughout the world in December 2019, there was a significant increase in the number of cases and deaths worldwide. 1 To stop this global crisis, social distancing rules were proposed to prevent transmission of the virus, with several countries enforcing community-wide lockdowns. 6 As COVID-19 is associated with a high risk of death or serious complications in older adults and individuals with comorbidities such as cardiovascular disease, diabetes, or respiratory disease, staying at or working from home may be suggested for such individuals. 7 However, some patients such as those with neurological conditions or pain still need routine physical therapy (PT) for management and rehabilitation. Therefore, access to PT clinics and PT hospital services was halted to reduce the risk of viral transmission.8,9 Consequently, telerehabilitation has been suggested as an alternative option for the treatment and monitoring of these individuals during the COVID-19 pandemic. Telerehabilitation has also been used to facilitate respiratory rehabilitation to improve symptoms of dyspnea, relieve anxiety, reduce complications, minimize disability, preserve function, and improve the quality of life among patients with COVID-19 during the acute phase and after discharge. 10
Telerehabilitation uses information and communication technologies to deliver health services, such as therapeutic exercises, education, and mental support, via synchronous online training (i.e., telephone and video conference), or asynchronous approaches (i.e., E-mail and online text messaging such as WhatsApp) to provide rehabilitation services remotely. 11 Although this technology has been used for >30 years, the COVID-19 pandemic has highlighted its utility in different clinical domains, including PT. 12 Individuals with chronic conditions, neurological disorders, musculoskeletal disorders, pain disorders, and disabilities may benefit from telerehabilitation as it enables them to continue their rehabilitation. 4 Furthermore, most patients (≥75%) were satisfied with the effectiveness of telerehabilitation, the feeling of physical safety and privacy facilitated by telerehabilitation, the ability of the provider to pay full attention to the patient, and the ability to provide necessary recommendations and complete assessments without help. 4 A recent systematic review reported that individuals with musculoskeletal disorders were more satisfied with telerehabilitation than face-to-face rehabilitation. 13 Moreover, a recent rapid review study that reviewed the effectiveness of telerehabilitation within PT demonstrated its feasibility during the pandemic. 9 Furthermore, the effectiveness of telerehabilitation in PT was found to be comparable with that of face-to-face rehabilitation and better than that of no rehabilitation. 9
Physical therapy treatments aim to enhance performance in different domains: impairments, activity limitations, and participation restrictions as classified in the components of functioning and disability of the International Classification of Functioning, Disability, and Health (ICF) model.14,15 The ICF model offers a systematic approach that encompasses various aspects of human functioning, incorporating biological, psychological, social, and environmental components. As a result, the ICF model serves as a conceptual foundation for rehabilitation, facilitating a holistic understanding of health and disability within a unified framework. Therefore, a multidisciplinary rehabilitation approach has been developed to enhance the effectiveness of rehabilitation across all levels in alignment with the ICF framework.16,17 Interestingly, recent systematic reviews and meta-analyses have demonstrated the positive effects of telerehabilitation on the activity and participation domains, including improved function in daily activities and quality of life among individuals with neurological 18 and musculoskeletal conditions. 19 Additionally, pain and disability were reduced after receiving telerehabilitation in people with musculoskeletal conditions. 19 However, a recent systematic review and meta-analysis have reported the negative effects of muscle strength and range of motion, as reflected in an impairment domain. 19 To the best of our knowledge, no systematic review and meta-analysis has evaluated the effectiveness of telerehabilitation on each outcome categorized according to the domain of the ICF model during the COVID-19 pandemic. Therefore, this systematic review and meta-analysis aimed to synthesize and analyze the evidence on the effectiveness of telerehabilitation categorized according to the ICF model domains.
Methods
Data sources and search strategy
A literature search was conducted to retrieve relevant articles from the Physiotherapy Evidence Database (PEDro), Scopus, PubMed, and EMBASE databases, and trial registers, journal websites, organizations, reference lists, and other sources, searched from 1 January 2019 to 31 May 2024 to identify studies. The MeSH terms used were as follows: ‘telerehabilitation’ AND (‘activities of daily living’ OR ‘quality of life’ OR ‘The Short Form 36-items Health Survey’ OR ‘SF-36*’ OR ‘muscle strength’ OR ‘strength’ OR ‘grip strength’ OR ‘gait function’ OR ‘walking’ OR ‘balance’ OR ‘fall’ OR ‘TUG*’ OR ‘timed up and go test’ OR ‘6MWT*’ OR ‘30 s sit-to-stands test’ OR ‘30STS*’ OR ‘six-minute walking test’ OR ‘physical activity’ OR ‘range of motion’ OR ‘body composition’ OR ‘upper-limb function’ OR ‘lower limb function’ OR ‘mobility’ OR ‘pain’) (Supplementary Table S1). The protocol for this systematic review was registered in PROSPERO (CRD42021286587) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement recommendations (see Supplementary Table S2, PRISMA checklist). 20
Two independent reviewers (JTha and FK) performed the literature review and selected publications according to the inclusion and exclusion criteria. Disagreements between the two reviewers were resolved by reaching a consensus via discussion with a third reviewer (JTre). The corresponding authors of relevant articles were contacted if important information was not included in the article.
Study selection
The selection criteria were as follows: (i) articles that investigated the feasibility or the effects of telerehabilitation in PT conducted during the COVID-19 pandemic, (ii) articles with a randomized controlled trial (RCT) study design that compared telerehabilitation (the treatment) with no treatment or usual care (which did not include any home-based or hospital-based exercise), and (iii) full reports published in English. Letters, abstracts, books, and conference proceedings were excluded. Nine RCT studies met the criteria for analysis. The primary analysis compared telerehabilitation with no intervention or usual care (control) based on changes from the baseline to the first post-treatment assessment, which, in most cases, was conducted immediately after the intervention. This comparison was chosen as the primary analysis because it represented the main data reported in most trials. To account for the diversity of telerehabilitation interventions across trials, the studies were categorized based on both the type of intervention and the outcomes measured. For trials with three or more treatment arms, two specific assumptions were made to ensure consistency and clarity in the analysis. In addition, studies demonstrating homogeneity in participants and variables were further selected for quantitative analysis.
Data extraction and quality assessment
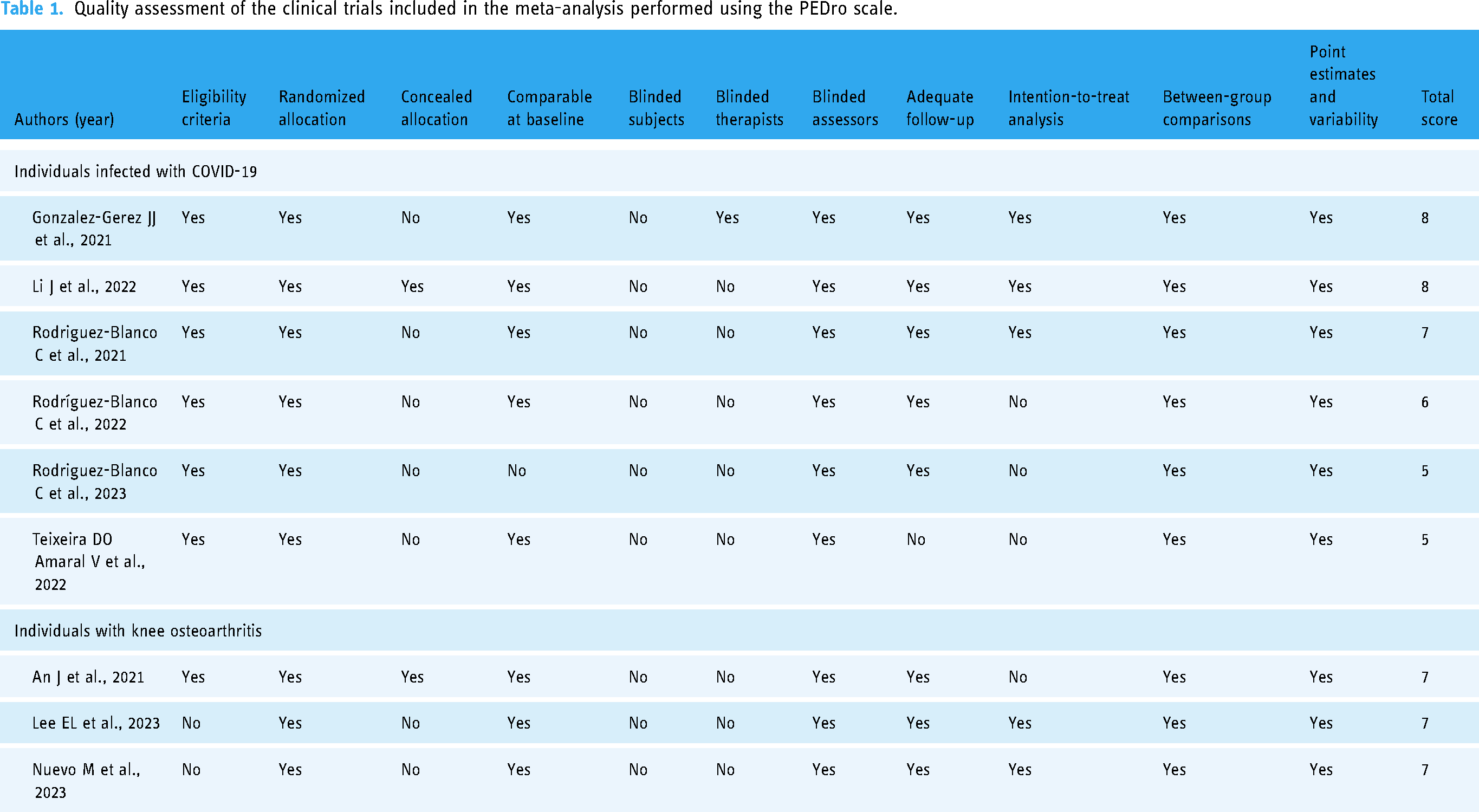
Data from all eligible studies, including the names of the authors, year of study, the aim of the study, study design, sample size, participant characteristics, intervention, outcome measures, and the main findings, were extracted independently by four reviewers (JTha, FK, KA, and KN) using a standardized electronic form. All results were evaluated and assigned to the following domains of the ICF model to analyze the data: impairments, activity limitations, and participation restrictions. Impairments refer to significant deviations or losses in body function or structure, while activities denote the execution of tasks or actions by individuals as defined in the ICF model by the World Health Organization 2001. 15 In addition, the methodological quality of the included articles was independently evaluated by two reviewers (PC and RP) using the PEDro scale. 21 The scale comprises 11 yes/no items, with scores of 0–3, 4–5, 6–8, and 9–10 indicating “poor,” “fair,” “good,” and “excellent” quality, respectively. 22 Disagreements between the reviewers regarding the scores were resolved by reaching a consensus (Table 1 and Supplementary Table S4).
Quality assessment of the clinical trials included in the meta-analysis performed using the PEDro scale.
Quantitative data synthesis
Outcomes based on the ICF domains included the body functions and structures domain (e.g., muscle strength, range of motion, balance, body composition, and pain), the activity domain (e.g., walking, upper limb function, and lower limb function), and the participation domain (e.g., quality of life). Results of each trial were combined using standard meta-analytic methods to estimate the overall effect of telerehabilitation versus no intervention. The Hedges’ g standardized mean difference (SMD) and the standard deviations of outcomes between the control and treatment groups were calculated for the meta-analysis of continuous outcomes. The Hedges’ g SMD reduces bias in studies with small sample sizes. 23 A random-effects model, the restricted maximum likelihood method using user-written commands in STATA/SE version 17.0 (StataCorp, College Station, TX, USA), 180 was used to summarize the data. Q-statistics and p-values were calculated to determine the statistical heterogeneity of outcomes between studies. A large Q-statistic relative to its degrees of freedom (low p-value) indicated heterogeneity in the intervention effects. 17 I2 values of 25% or less were classified as indicating low heterogeneity, 50% as moderate heterogeneity, and 75% or more as high heterogeneity. 24 These values were included in the forest plot. If the review includes more than 10 studies, we intend to evaluate publication bias following the recommendations outlined in Chapter 10 of the Cochrane Handbook. 25 Additionally, if the data were not eligible for inclusion in the meta-analysis (e.g., due to the presence of only a single study or the absence of reported mean differences [MD] and standard deviations [SD] for the outcomes), the effectiveness of telerehabilitation was analyzed qualitatively. This analysis was categorized according to the ICF outcomes relevant to PT.
Results
Search strategy
An electronic search yielded 835 potentially relevant articles published after 2019. After the selection process, 261 full-text articles were evaluated for eligibility, and 123 were excluded (Figure 1). Finally, 134 full-text articles were included for the qualitative synthesis which included individuals with musculoskeletal conditions (n = 38),26–63 cardiopulmonary conditions (n = 44),64–107 neurological conditions (n = 30),108–137 pediatric conditions (n = 6),138–143 and others (n = 16; i.e., individuals with non-communicable diseases and older individuals)144–159 (Supplementary Table S3). Out of the 134 included studies, only nine studies (six studies under cardiopulmonary and three studies under musculoskeletal conditions) were included in the quantitative analysis38,54,61,69,72–75,91 based on the heterogeneity of the participants and variables in the eligible studies (Figure 1 and Supplementary Table S3). In addition to participant homogeneity, the studies included in the meta-analysis employed consistent outcome measures, such as the Borg Rating of Perceived Exertion (RPE) scale,72–74 the 30-second sit-to-stand test (30STST; the number of stands),72,74,91 the 6-minute walking test (6MWT; meters),69,72,74,75 and the timed up and go test (TUGT; seconds)38,54,61 to evaluate the effectiveness of telerehabilitation. However, it should be noted that these assessments overlap in certain studies. As for other conditions that could not be analyzed by the quantitative analysis, the evidence has been shown in Supplementary Table S3).

PRISMA flow diagram of the study. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT: randomized control trial.
Study characteristics
Type of participants and treatment
For the 134 studies included in the qualitative synthesis, participants were categorized into several groups based on their conditions including musculoskeletal conditions (e.g., individuals with knee osteoarthritis (OA),54,56 ankylosing spondylitis, 53 and patellofemoral pain syndrome 55 ); cardiopulmonary conditions (e.g., individuals with coronary artery disease (CAD), 64 chronic cardiac, 65 respiratory, 36 and COVID-19 75 ); neurological conditions (e.g., individuals with multiple sclerosis (MS),108,110 stroke,109,113 and Alzheimer disease (AD)111,131); pediatric conditions (e.g., children with cystic fibrosis 138 ); and other conditions (e.g., older adults at risk for functional decline or falls, 144 individuals with type 2 diabetes (T2D), 145 and women with stress urinary incontinence (SUI)) 147 (Supplementary Table S3). All participants received telerehabilitation, which was compared either to no intervention/ usual care or traditional face-to-face physical therapy at a clinical center.
Additionally, nine eligible RCTs were included in the meta-analysis. They were conducted in Spain (n = 5),38,72–74,91 Korea (n = 2),54,61 China (n = 1), 69 and Brazil (n = 1). 75 Six of these nine studies included individuals with COVID-19 (n = 310),69,72–75,91 whereas the remaining three included individuals with knee osteoarthritis (OA) who were unable to access necessary physical therapy services (pre- and post-operative periods) (n = 111).38,54,61 Those studies were included in the meta-analysis due to the homogeneity of participants and outcome measures.38,54,61,69,72–75,91 A total of 421 participants were enrolled in these studies.38,54,61,69,72–75,91 The participants in the studies that enrolled patients with COVID-19 were trained to perform breathing, aerobic, and resistance exercises through telerehabilitation.69,72–75,91 The treatments were divided into two protocols in the studies that enrolled individuals with knee OA: pre-operative protocol 54 or conventional treatment 61 (such as lower extremity strengthening exercise, mobility, flexibility, and balance) 54 and post-operative protocol (such as lower extremity exercise in each isotonic contraction of a different lower limb muscle: quadriceps, iliopsoas, gluteus medius, gluteus maximus, and hamstring). 38 The participants who received telerehabilitation were compared with those who did not receive any treatment or those who received usual care (Supplementary Table S3).
Type of outcome measures
Various outcome measures were utilized in the 134 studies included in this review, reflecting the diverse nature of the investigations across multiple disease conditions. Therefore, the outcome measures were categorized using the ICF model as detailed in Supplementary Table S3. However, the outcome measures analyzed in the meta-analysis can be classified into two domains of the ICF model: impairment and activity domains. In the impairment domain, the RPE scale (scale) was utilized in the studies.72–74 For the activity domain, the 30STST (number of stands),72,74,91 the 6MWT (meters),69,72,74,75,91 and the TUGT (seconds)38,54,61 were applied in studies.
Quality assessment of the included studies
The quality of the 134 studies was assessed using the PEDro scale (Supplementary Table S4). The quality of the nine studies included in the meta-analysis was judged to be fair–good (Table 1). Most of these studies used randomized methods for allocation38,54,61,69,72–75,91; however, the allocation was concealed in only two studies.54,69 The methodological quality assessment of seven studies was judged to be good based on the achievement of random allocation, comparability at baseline, blinding of the assessors, adequate follow-up, intention-to-treat analysis, and point estimates and variability.38,54,61,69,73,74,91 The methodological quality assessment of two studies was judged to be fair based on the achievement of random allocation, comparability at the baseline, blinding of the assessors, inter-group comparison, and point estimates and variability(Table 1).72,75
Effectiveness of the treatment
Systematic review
The 134 included studies have been synthesized in each condition including musculoskeletal, cardiopulmonary, neurological, pediatric, and other conditions. Most of them were synthesized to investigate the effectiveness of telerehabilitation as compared to no intervention or usual care or traditional face-to-face rehabilitation at center on impairment, functional, and participation domains of the ICF model. First, 35 studies investigated the effectiveness of telerehabilitation compared to no intervention or usual care. These studies addressed musculoskeletal conditions (n = 11),53–63 cardiopulmonary conditions (n = 13),64–76 neurological conditions (n = 5),108–112 pediatric conditions (n = 1), 138 and other conditions (n = 5).144–148 Second, 99 studies evaluated the effectiveness of telerehabilitation compared to traditional face-to-face rehabilitation conducted in a clinical setting. These studies included musculoskeletal conditions (n = 27),26–52 cardiopulmonary conditions (n = 31),77–107 neurological conditions (n = 25),113–137 pediatric conditions (n = 5),139–143 and other conditions (n = 11)149–159 (Supplementary Table S3).
For studies investigating the effectiveness of telerehabilitation compared to no intervention or usual care, a total of 11 studies53–63 focused on musculoskeletal conditions (treatment n = 473, control n = 491) including individuals with knee OA (pre and post-operative), ankylosing spondylitis, patellofemoral pain syndrome, fibromyalgia (FM) syndrome, postoperative low back pain, and elderly patients recovering from postoperative hip fracture patients. The quality of these studies was classified as good (n = 7) and fair (n = 4) as presented in Supplementary Table S3. Most of the evidence showed that telerehabilitation improved outcomes across all domains of the ICF model, regardless of the participants’ group and the quality of study. Interestingly, the study of Hernando-Garijo I and co-workers in 2021, conducted in women with FM, showed no significant improvements in functional (i.e., 6MWT) and participation (i.e., Fibromyalgia Impact Questionnaire (FIQ-R)) domains of the ICF model after immediate 30 sessions of telerehabilitation as compared to no intervention (control group) (shown in Supplementary Table S3). 58 However, the improvement of an impairment domain of the ICF model was washed out when follow-up at 6 months after telerehabilitation. 59 In addition, another study, conducted with individuals with knee OA (post-operative) also showed no improvements across domains of the ICF model after a 2-year follow-up period of telerehabilitation compared to usual care.
For the cardiopulmonary conditions, 13 studies64–76 (treatment n = 794, control n = 718) were included, investigating individuals with patients with coronary artery disease (CAD), chronic cardiac, respiratory, COVID-19, patients with cardiovascular diseases (CVD), elderly patients with chronic heart failure, heart failure (HF) (mild diastolic or severe diastolic dysfunction), and chronic obstructive pulmonary disease (COPD). The quality of these studies was rated as good (n = 9) and fair (n = 4) as shown in Supplementary Table S3. The majority of studies regardless of the participant group demonstrated improvements in various domains of the ICF model following telerehabilitation as compared to no intervention or usual care. In terms of the findings in individuals with COVID-19,69,71–75 they showed improvements across all domains of the ICF model following telerehabilitation as compared to the control group. Additionally, the evidence in people with chronic cardiac, 65 CVD, 66 and chronic HF 67 also showed improvements as well as the participants with COVID-19. In contrast, the telerehabilitation in people with COPD could improve only in impairment and participation domains as compared to the control group, 70 while no improvements in every domain of the ICF model following telerehabilitation were found in individuals with CAD as compared to the control group. 64
Under neurological conditions, five studies108–112 investigated the effects of telerehabilitation as compared to the control group in people with multiple sclerosis (MS) with urinary incontinence (UI), 108 stroke, 109 and Alzheimer's disease (AD) 111 (treatment n = 95, control n = 72). The quality of these studies was rated as good (n = 1) and fair (n = 4) as shown in Supplementary Table S3. All pieces of evidence showed improvements across all domains of the ICF model, regardless of the participant group or the quality of study. However, improvements were not observed consistently across all variables and studies.108,109,111,112 Based on the evidence, individuals with MS with UI showed an improvement in impairment and participation domains of the ICF model following telerehabilitation as compared to the control group. In stroke patients, telerehabilitation could improve the functional and participation domain of the ICF model as represented by 6MWT and Disabilities of the Arm, Shoulder and Hand Questionnaire, respectively. Moreover, the effect of telerehabilitation in people with AD showed the improvement of impairment and functional domain of the ICF model as compared to the control group.
As for pediatric (treatment n = 14, control n = 14), only one study 138 with good quality investigated the effects of telerehabilitation compared to the control group in children with cystic fibrosis. They showed that telerehabilitation could improve the participation domain as presented by major depressive disorder and generalized anxiety disorder. Lastly, five studies were included, investigating other conditions including older adults at risk for functional decline or falls, patients with type 2 diabetes (T2D), women with stress urinary incontinence (SUI), and individuals without COVID-19 (treatment n = 160, control n = 161).144–148 The quality of these studies was rated as good (n = 4) and fair (n = 1) as detailed in Supplementary Table S3. For the findings, most of them showed improvements across all domains of the ICF model following telerehabilitation compared with no intervention or usual care. However, improvements were not observed consistently across all variables and studies.146–148 Based on the evidence, people with older adults at risk for functional decline or falls showed an improvement in the functional domain of the ICF model following telerehabilitation as compared to the control group. Additionally, people with T2D showed that telerehabilitation could improve impairment, functional, and participation domains of the ICF model as compared to the control group. Moreover, telerehabilitation in people without COVID-19 could improve the participation domain of the ICF model as compared to the control group and telerehabilitation could improve the impairment domain in women with SUI as compared to the control group.
Among the studies comparing the effectiveness of telerehabilitation with traditional face-to-face PT care provided in clinical settings, a total of 99 studies were included: musculoskeletal conditions (n = 27),26–52 cardiopulmonary conditions (n = 31),77–107 neurological conditions (n = 25),113–137 pediatric conditions (n = 5),139–143 and other conditions (n = 11).149–159 Specifically, 27 studies focused on musculoskeletal conditions (treatment group: n = 993, control group: n = 957), encompassing individuals with pain (e.g., neck, lower back, shoulder),31,34 hip and knee osteoarthritis (OA, both pre-operative and post-operative),32,37 and specific syndromes (e.g., tennis elbow, 33 hand injuries, 28 plantar fasciitis, 29 chronic whiplash-associated disorders, 45 and rheumatoid arthritis 46 ). The quality of these studies was rated as excellent (n = 1), good (n = 23), and fair (n = 3) as shown in Supplementary Table S3. Most of the evidence showed that telerehabilitation improved outcomes across all domains of the ICF model, regardless of the participant group. However, improvements were not observed consistently across all variables and studies.30,33,35,36 For instance, eight studies26,27,31,37,38,40,44,45 involving individuals with pain, hip and knee OA, or chronic whiplash-associated disorders showed no significant improvement in any ICF domain following telerehabilitation compared to face-to-face PT services. In particular, studies focused on individuals with chronic shoulder pain reported negative outcomes, as evidenced by self-reported pain ratings, with telerehabilitation performing worse than traditional face-to-face PT. 35 Additionally, a study examining individuals post-total knee arthroplasty indicated negative outcomes related to the incidence of reported falls between discharge and 12 weeks post-intervention, with telerehabilitation showing less favorable results compared to traditional face-to-face PT. 27
For the cardiovascular conditions, 31 studies (treatment group: n = 2369, control group: n = 2301) were included, investigating individuals with chronic HF, CVD including angina pectoris and recent myocardial infarction, CAD, atrial fibrillation, idiopathic pulmonary fibrosis (IPF), COPD, COVID-19, and lung cancer.77–107 The quality of these studies was categorized as good (n = 15), fair (n = 15), and poor (n = 1) as presented in Supplementary Table S3. The majority of studies regardless of the participant group demonstrated improvements in various domains of the ICF model following telerehabilitation as compared to the traditional PT face-to-face services. Even though, these improvements were observed in specific variables rather than consistently across all measures.79,81,85,92,93,95,96,98,99,101–103,105 However, eight studies82,89,90,94,97,100,104,106 involving individuals with COPD, COVID-19, HF, and CAD reported no significant improvements in any ICF domain following telerehabilitation. This lack of improvement was observed regardless of the quality of the studies or the ICF domains assessed when compared to traditional PT services.
Under neurological conditions, 25 studies (treatment group: n = 840, control group: n = 797) were included involving individuals with stroke, Parkinson's disease (PD), MS, systemic sclerosis (SSc), mild cognitive impairment (MCI), and AD.113–137 The quality of these studies was categorized as excellent (n = 1), good (n = 16), fair (n = 7), and poor (n = 1) as detailed in Supplementary Table S3. The majority of the included studies showed improvements across various domains of the ICF model following telerehabilitation, in comparison to the traditional face-to-face PT services. However, six studies121,122,124,127,129,130 involving individuals with stroke, PD, and MS reported no significant improvements in any ICF domain after telerehabilitation, regardless of the quality of the studies. These findings indicate that, in some cases, telerehabilitation may not achieve equivalent outcomes to traditional face-to-face PT services for these conditions.
For pediatric conditions, five studies (treatment group: n = 146, control group: n = 143) were included involving individuals with cerebral palsy (CP), spastic paraparesis, organic acidemia, traumatic brain injury and Duchenne muscular dystrophy (DMD). The quality of these studies was categorized as good (n = 3), fair (n = 1), and poor (n = 1) as shown in Supplementary Table S3.139–143 Findings from four of five studies demonstrated improvements across all domains of the ICF model, regardless of participant group following telerehabilitation compared to traditional face-to-face PT services.140–143 However, only one study of poor quality showed no improvement in the Pediatric Quality of Life Inventory (PedsQL) questionnaire score following telerehabilitation for motor learning-based treatment as compared to a face-to-face PT service. 139
Finally, 11 studies (treatment group: n = 297, control group: n = 267) focused on other conditions including healthy adults, older adults, people with obesity, breast cancer, Marfan syndrome (MFS), burn injury, and women with SUI and mixed incontinence (MUI).149–159 The quality of these studies was categorized as good (n = 7), fair (n = 3), and poor (n = 1) as detailed in Supplementary Table S3. Findings revealed that 7 of the 11 studies149–152,154–156 showed improvements across all domains of the ICF model, regardless of the quality of study and participant group after telerehabilitation compared to traditional face-to-face PT services. However, four studies of good quality showed no improvements across any ICF domain.153,157–159 Importantly, one of these studies, conducted with individuals with burn injuries, demonstrated negative results in the range of motion following telerehabilitation compared to a face-to-face PT service provided in a clinical setting. 158
Meta-analysis
In addition to a qualitative synthesis as summarized from 134 studies, nine studies, which had homogeneity of participant and outcome measures as mentioned in the search strategy section, were included for a meta-analysis. A meta-analysis was performed to estimate the pooled effect size of the effectiveness of telerehabilitation on impairments and activities. In the impairment domain, the Borg Rating of Perceived Exertion (RPE) scale (scale) was used to evaluate those effects in individuals with COVID-10.72–74 In the activity domain, the 30-second sit-to-stand test (30STST; number of stands)72,74,91 and 6-minute walking test (6MWT; meters)69,72,74,75 were used in individuals with COVID-19 and the timed up and go test (TUGT; seconds)38,54,61 was used in individuals with knee OA.
Effectiveness of telerehabilitation on the Borg RPE scale
Three studies that enrolled individuals with COVID-19 examined the effect of telerehabilitation using the Borg RPE scale.72–74 The data of 135 participants were pooled (treatment group = 71, control group = 64). The results of the RPE test were significant (p < 0.001). The scale of the treatment group (1.82 scale) was lower than that of the control group (95% confidence interval [CI] −2.77 to −0.86). However, the results exhibited high heterogeneity (Q = 11.56, p < 0.001, I2 = 82.08%) (Figure 2).
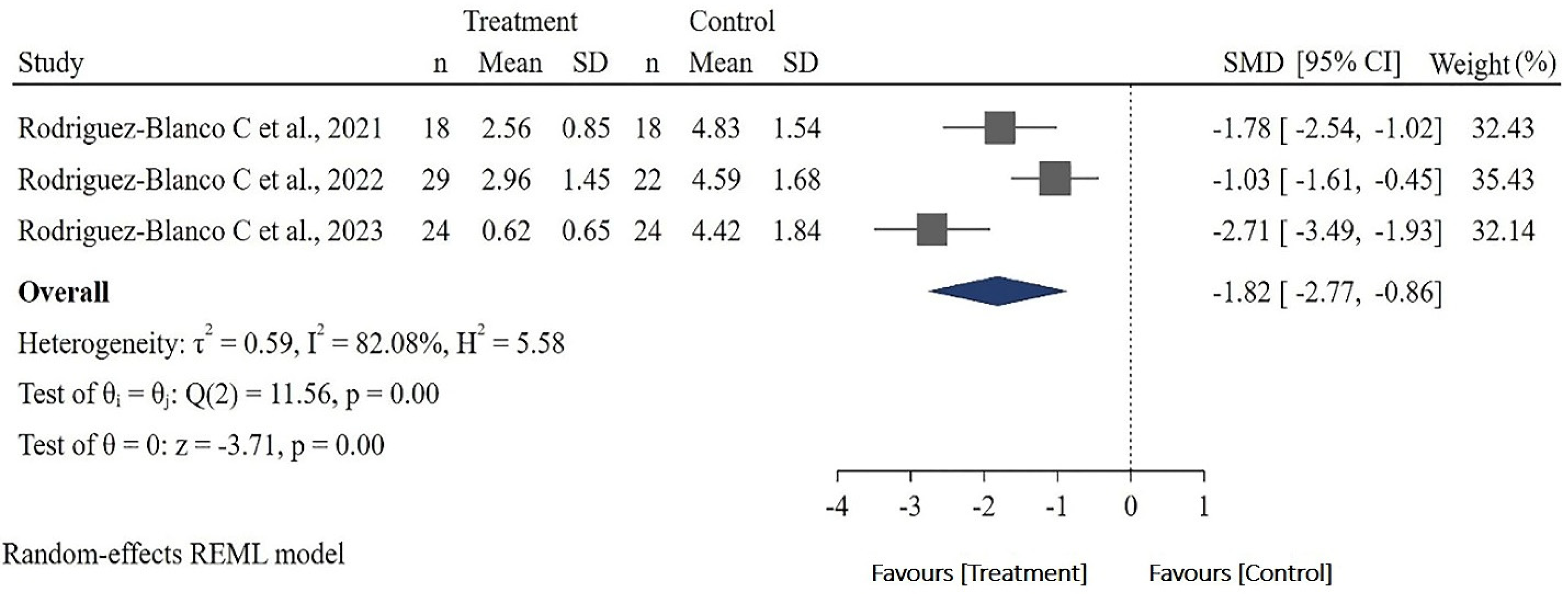
Forest plot of the standardized mean difference for the effect of telerehabilitation on the RPE scale. RPE: rating of perceived exertion; SD: standard deviation; SMD: standardized mean difference; CI: confidence interval.
Effectiveness of telerehabilitation on the 30STST results
Three studies that enrolled individuals with COVID-19 examined the effect of telerehabilitation on the 30STST results.72,74,91 The pooled data of 122 participants (treatment group = , control group = 61) revealed no heterogeneity (Q = 1.39, p = 0.50, I2 = 0.00%). The number of stands performed by the participants in the treatment group during 30STST was significantly greater than that of the participants in the control group (0.88; [95% CI 0.52–1.25], p < 0.001; Figure 3).

Forest plot of the standardized mean difference for the effect of telerehabilitation on the 30STST. 30STST: 30-second sit-to-stand test; SD: standard deviation; SMD: standardized mean difference; CI: confidence interval.
Effectiveness of telerehabilitation on the 6MWT results
Four studies examined the effect of telerehabilitation on the 6MWT results.69,72,74,75 The pooled data of 221 participants (treatment group = 104, control group = 117) revealed moderate heterogeneity (Q = 6.12, p = 0.11, I2 = 50.70%). The 6MWT results of the participants in the treatment group (0.83 m) were significantly greater than those of the participants in the control group (95% CI 0.42–1.24, p < 0.001) (Figure 4).

Forest plot of the standardized mean difference for the effect of telerehabilitation on the 6MWT results. 6MWT: 6-minute walking test; SD: standard deviation; SMD: standardized mean difference; CI: confidence interval.
Effectiveness of telerehabilitation on the TUGT results
Three studies that enrolled individuals with knee OA examined the effect of telerehabilitation on the TUGT results.38,54,61 The pooled data of 111 participants (treatment group = 56, control group = 55) revealed that telerehabilitation had no effect on the TUGT results (pooled SMD 0.45 [95% CI −1.19 to 0.30], p = 0.24). Moderate heterogeneity was observed (Q = 7.32, p = 0.03, I2 = 74.07%) (Figure 5).

Forest plot of the standardized mean difference for the effect of telerehabilitation on the TUGT results. TUGT: timed up and go test; SD: standard deviation; SMD: standardized mean difference; CI: confidence interval.
Discussion
This systematic review and meta-analysis aimed to synthesize and analyze the evidence on the effectiveness of telerehabilitation categorized according to the domains of the ICF model. Individuals with conditions such as musculoskeletal conditions,26–62,102 cardiopulmonary conditions,64–69,71–107 neurological conditions,108–117,119–137,140,160 pediatric,138,139,141–143 and other conditions (non-communicable disease and geriatric individuals)144–159 received telerehabilitation in the present study. The effectiveness of telerehabilitation was compared with that of several control treatments such as not receiving treatment, usual care, and face-to-face rehabilitation. In terms of outcome measures, diverse variables were categorized in each domain of the ICF model; however, the results are controversial. Some variables exhibited positive effects, whereas others exhibited negative effects or comparable effects to the control. Thus, future studies must investigate the homogeneity of the participants and outcome variables.
Based on the studies included in the qualitative synthesis, our findings indicate that telerehabilitation has the potential to enhance outcomes across all domains of the ICF model, regardless of the participant group. These improvements were found to be superior to those achieved through either no intervention or usual care and comparable to, or in some cases exceeding, the outcomes observed with traditional face-to-face physical therapy provided in clinical settings. Among the studies included in our analysis, 35 studies investigated the effectiveness of telerehabilitation compared to no intervention or usual care. These studies encompassed musculoskeletal conditions (n = 11),53–63 cardiopulmonary conditions (n = 13),64–76 neurological conditions (n = 5),108–112 pediatric conditions (n = 1), 138 and other conditions (n = 5).144–148 Additionally, 99 studies assessed the effectiveness of telerehabilitation in comparison to traditional face-to-face rehabilitation provided in a clinical setting. This group included studies on musculoskeletal conditions (n = 27),26–52 cardiopulmonary conditions (n = 31),77–107 neurological conditions (n = 25),113–137 pediatric conditions (n = 5),139–143 and other conditions (n = 11)149–159 In studies focused on musculoskeletal conditions, a diverse group of participants were included in this systematic review. However, the majority of studies were conducted with individuals suffering from hip and knee OA (n = 14),26,27,30,32,38,47,48,51,52,54,56,57,61,102 while others included individuals with pain syndromes such as neck pain or shoulder pain or low back pain.31,34,39–41,43,60 These conditions are leading causes of pain and disability, particularly among older adults. 161 The management of these conditions primarily focuses on relieving symptoms, delaying the need for arthroplasty, and promoting therapeutic exercises, physical activity, and lifestyle changes.162,163 During the COVID-19 pandemic, access to in-person physical therapy was restricted, which led to a significant shift toward telerehabilitation as an alternative approach. The lockdown situation during the pandemic may have exacerbated pain syndromes, as many individuals were confined to their homes, often working remotely and potentially remaining in static positions for prolonged periods. 164 This change in daily routines may have contributed to increased discomfort and pain for many individuals. Additionally, telerehabilitation has been applied in specific syndromes such as women with FM,58,59 ankylosing spondylitis, 53 and rheumatoid arthritis. 46 Compared to no intervention or usual care, telerehabilitation for musculoskeletal conditions showed greater improvement across all domains of the ICF model. However, one study involving individuals with knee OA following surgery showed no improvements across domains of the ICF model after a 2-year follow-up period of telerehabilitation compared to usual care. Even though our systematic review did not synthesize the long-term effects of telerehabilitation, one study extended its investigation into long-term outcomes. However, the findings indicated that improvements did not appear during the follow-up period. This study is consistent with the study of Hernando-Garijo I et al., 2022 that reported no significant improvement in the impairment domain of the ICF model at 6-month follow-up after telerehabilitation. 59 In addition, some evidence involving individuals with pain, hip and knee OA, or chronic whiplash-associated disorders showed no significant improvements in any ICF domain following telerehabilitation compared to face-to-face PT services. These findings suggested that telerehabilitation can be comparable to face-to-face PT services in certain contexts. However, our findings also demonstrated negative results in specific outcomes. For instance, self-reported pain ratings in individuals with chronic shoulder pain and the incidence of reported falls in individuals post-total knee arthroplasty were worse following telerehabilitation compared to a face-to-face PT service. These results highlight the potential limitations of telerehabilitation in addressing the impairment domain of the ICF model, underscoring the need for careful consideration when implementing telerehabilitation for certain conditions.
For cardiopulmonary conditions, our evidence included studies investigating various participant groups, such as individuals with CAD, CVD, COVID-19, and COPD. The majority of the evidence revealed significant improvements across domains of the ICF model, whether compared to no intervention, usual care, or face-to-face PT services in a clinical setting. For example, individuals with CVD demonstrated significant improvements in physical fitness and endothelial function tests, reflecting enhancements in the impairment domain. This finding suggests that telerehabilitation is both feasible and acceptable as a conventional cardiovascular rehabilitation program for people with CVD, particularly when isolation is necessary, as supported by the previous evidence. 165 Additionally, improvements in the functional and participation domains were observed, as measured by increased physical activity levels and enhanced quality of life, respectively. 66 Similarly, individuals with COVID-19 showed significant improvements on the Borg scale,72–74 reflecting progress in the impairment domain, as well as in the 6MWT69,72,74,75,91 and 30STST72,74,91 which are indicative of functional domain improvements. This aligns with findings from a recent systematic review and meta-analysis of patients with COVID-19 who received telerehabilitation. Our results further corroborate the benefits of telerehabilitation in enhancing functional capacity. Moreover, our systematic review extends these conclusions by highlighting significant improvements in quality of life, reinforcing the broader potential of telerehabilitation as a comprehensive approach to rehabilitation for individuals recovering from COVID-19. 10 These findings reinforce the potential of telerehabilitation to deliver comprehensive benefits across the ICF model for individuals with cardiopulmonary conditions.
However, some evidence has shown non-significant improvements in individuals with COVID-19 following telerehabilitation compared to face-to-face physical therapy services in clinical care settings. 82 As a result, both telerehabilitation and face-to-face methods can be recommended based on the specific needs and conditions of each patient. Additionally, our findings indicated non-significant improvements in individuals with COPD at a 12-month follow-up after telerehabilitation compared to traditional physical therapy or usual care.89,90 This is consistent with our findings in individuals with musculoskeletal conditions, particularly regarding the wash-out of long-term effects of telerehabilitation. For neurological conditions, our findings indicate that telerehabilitation can improve outcomes across all domains of the ICF model under various conditions such as stroke, PD, and MS. However, some evidence reported no significant improvements in any ICF domain after telerehabilitation in individuals with these conditions. These findings suggest that, in certain cases, telerehabilitation may not achieve equivalent to traditional face-to-face PT services. This finding is consistent with the previous evidence. 18 In contrast, telerehabilitation has shown superiority over no intervention or usual care out, emphasizing its potential as an effective alternative for individuals unable to access in-person training. For pediatric conditions, few studies have been conducted on the application of telerehabilitation. However, all of these studies showed significant improvements across all domains of the ICF model when comparing telerehabilitation to either no intervention/ usual care or traditional face-to-face PT services. Notably, only two studies specifically showed significant improvements in the participation domain. This could be attributed to the primary objective of these studies, which focused on investigating the effects of telerehabilitation on the participation domain of the ICF model.138,139 Additionally, our findings demonstrate that telerehabilitation could improve across all domains of the ICF model in other conditions such as healthy adults, older adults, people with obesity, breast cancer, MFS, burn injury, and women with SUI and MUI. However, the study investigating individuals with burn injuries showed negative results in an impairment domain of the ICF model as measured by the range of motion test following telerehabilitation compared to a face-to-face PT service provided in a clinical setting. Burns affecting their shoulder and/or hand lead to a higher risk of long-term burn scar contracture with prolonged periods of decreased ROM. Some case requires surgical contracture release years post injury. The 12-week study duration may not have been sufficient to adequately monitor the recovery of full joint range of motion in the affected areas, emphasizing the need for longer-term follow-up. Extended observation is required to determine whether the return to full joint ROM is comparable between home-based telerehabilitation and in-person rehabilitation programs over an extended period post-burn injury. Further research is necessary to investigate whether the observed differences in ROM are attributed to the mode of exercise program delivery or are instead a consequence of the study's limited duration and the inherent complexity of the joints affected by the burn.
In addition to the systematic review, nine of 134 studies were included in the meta-analysis based on the homogeneity of the participant groups and outcome measures.69,72–75,91 This meta-analysis demonstrated that telerehabilitation implemented during the COVID-19 pandemic offered some benefits. This meta-analysis revealed that compared with no treatment and usual care, telerehabilitation had positive effects on the impairment and activity domains of the ICF model. Home- or hospital-based exercises were not performed by the participants in the usual care group. This evidence was obtained from the RCT studies that applied telerehabilitation in individuals infected with COVID-19.69,72–75,91 In contrast, telerehabilitation had no effect on the activity domain of the ICF model in individuals with knee OA.72–74 The findings of the present study differ from those of other systematic reviews and meta-analyses as this study summarized the outcomes categorized according to the domains of the ICF model and included all participants who received telerehabilitation.9,166,167 The ICF framework is used to analyze overall health issues and can be a tool for communication by healthcare professionals to convey the health status of patients. All participants were categorized under each condition and analyzed separately.
Three studies investigated the effect of telerehabilitation on the Borg RPE scale in individuals with COVID-19 in terms of an impairment domain of the ICF model.72–74 The Borg RPE scale is a formal scale used to identify the perception of exertion level. 168 Dyspnea, a subjective perception of exertion level, is a common symptom reported by these individuals. 169 A 14-day (once a day) therapeutic exercise telerehabilitation protocol comprising 10 breathing and strength-based exercises and a 7-day (once a day) protocol comprising 10 non-specific toning exercises of resistance and strength were implemented. The participants received instructions on how to implement these protocols via video conferencing and were motivated by a physical therapist once a week. As for the improvement of the Borg scale, it is possible that the improvements in shortness of breath and fatigue following telerehabilitation were related to a recent respiratory telerehabilitation. 107 This improvement may be attributed to the improvement in respiratory function 74 and strengthening of respiratory muscles, as observed in previous studies. 101 Additionally, the physiological explanation may be attributed to the increase in the capacity of the respiratory muscles, the flexibility of the ribcage, and gas exchange. 169
Telerehabilitation improved the activity domain of the ICF model, as indicated by the 30STST and 6MWT results. This improvement in the 6MWT results may be attributed to the combination of breathing, strengthening, and aerobic exercise.69,75 This approach helps enhance aerobic capacity and endurance. 170 Acute respiratory distress syndrome is a common complication that leads to prolonged treatment in a respiratory intensive care unit (RCU). Bed rest and poor mobility, a consequence of prolonged treatment in the RCU, result in a reduction in physical capacity.170,171 Therefore, pulmonary rehabilitation should be commenced after hospitalization. The findings of the present study are consistent with those of previous systematic reviews and meta-analysis studies that reported an improvement in functional capacity, lower extremity performance or strength, level of dyspnea, and quality of life following telerehabilitation compared with that observed following no treatments.10,167,172 However, other variables such as respiratory capacity (i.e., Forced Expiratory Volume in 1 s (FEV1) and Forced Vital Capacity (FVC)) 173 or Return to Social or Occupational Activities 174 that can reflect the domains of impairment, activity, and participation restrictions more accurately must be included in future studies.
In contrast to individuals with knee OA, the meta-analysis revealed that telerehabilitation had no effect on the activity domain as measured by TUGT. As mentioned in the study by Nuevo et al., 38 this may be attributed to the short follow-up period. The event exhibiting non-effectiveness in quantitative analysis, pre- and post-assessment, revealed an improvement in the TUGT results after remote rehabilitation comprising lower extremity strengthening exercises in individuals with knee OA. 61 The TUGT results can be improved in individuals with advanced knee OA by implementing a pre-operative telerehabilitation program for total knee arthroplasty. 54 Notably, the findings of the present study may be consistent with those of a previous systematic review and meta-analysis study. They showed no improvement in physical function, as measured by the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) physical functional subscale, but the WOMAC pain subscale improved following telerehabilitation as compared to either no treatment or other treatments without telerehabilitation. However, there was a variety of telerehabilitation protocols in the evidence, including physician support, physical therapist support, psychologist support, education, and monitoring of symptoms. 175 Additionally, a previous meta-analysis study showed no effectiveness of telerehabilitation on pain and physical function in individuals with knee OA compared with either no treatment (or usual care) or conventional in-person rehabilitation. 176
This systematic review and meta-analysis have some limitations. First, only a small number of studies were included in the present study as only RCTs published in peer-reviewed journals were eligible for inclusion. Therefore, the results should be interpreted with caution. The second limitation is participant heterogeneity. The potential causes of heterogeneity are the population characteristics (i.e., disease, number of onsets, and severity), intervention protocol (i.e., duration, frequency, length, and intensity), and outcome measures. Discrepancies in the type, intensity, frequency, or duration of interventions across studies may contribute to inconsistent outcomes. Additionally, inconsistent use of measurement tools or varying definitions of outcomes may result in heterogeneity. Nonetheless, a qualitative assessment of the included studies in a systemic review is considered in addition to the findings of this study's heterogeneity test. Based on heterogeneity analysis, the 30SSTS test showed no heterogeneity (I2 = 0), reinforcing the reliability of the pooled findings for this outcome. In contrast, moderate to high heterogeneity was observed in the results of the 6MWT, TUGT, and Borg RPE scale, with I2 values of 50.70%, 74.07%, and 82.08%, respectively. This indicates that caution is warranted when interpreting the pooled results for these measures. The heterogeneity in the 6MWT, TUGT, and Borg RPE scale may be influenced by one or two outlier studies with results that deviate significantly from the majority. Further analyses, such as subgroup analysis or meta-regression, could help identify potential sources of heterogeneity and enhance the validity of the meta-analysis conclusions. Heterogeneity observed in the 6MWT, TUGT, and Borg RPE scale may be attributed to one or two outlier studies whose findings differ significantly from those of the other included studies.
To the best of our knowledge, this is the first systematic review and meta-analysis based on the ICF model of the COVID-19 pandemic. Only the Borg RPE scale, 30SSTS, 6MWT, and TUGT results were included in the present meta-analysis which had a small sample size. These outcome measures do not reflect all domains of the ICF model. Therefore, further studies with larger sample sizes and additional variables in each domain are warranted. Although a positive impact was observed, it was only noted in individuals with COVID-19 owing to the heterogeneity of the participants with various conditions. Consequently, future studies should examine the homogeneity of the participants (Supplementary Table S3).
Based on the ICF model, we did not take into consideration the environmental and personal factors that might be associated with the observed improvements. The use of telerehabilitation is to assess a patient's real-life situation in their natural environment. This includes considering environmental factors that may affect their mobility or functioning, such as the layout of the home or available resources. Telerehabilitation also facilitates engagement with family members and caregivers, providing a more holistic view of the patient's support system. By observing these interactions remotely, healthcare providers can gain better insights into the challenges and needs of both patients and caregivers. However, one limitation of telerehabilitation is the difficulty in physically handling and measuring patients. In traditional healthcare settings, hands-on assessments are often necessary to evaluate physical conditions, which is harder to achieve through telecommunication. To overcome this, there is a need to develop innovations and technologies that can facilitate remote physical measurements, such as wearable devices, motion sensors, or AI-driven tools that can track vital signs and physical movements with precision. To maximize the benefits of telerehabilitation, particularly in the realm of ADL observation, policies need to be implemented that support its wider adoption. 177 For instance, insurance coverage should be expanded to include telerehabilitation services, ensuring that both patients and healthcare providers are financially supported. Governments and healthcare institutions should work towards creating guidelines and frameworks that facilitate the use of telemedicine while maintaining quality care standards. Moreover, investment in research and development of telerehabilitation technologies is crucial to bridge the gap in physical assessments, ensuring that telerehabilitation becomes a comprehensive tool in patient standard care protocols. In future pandemics, telerehabilitation can serve as a scalable and flexible solution to meet the needs of patients while minimizing exposure risks for both patients and healthcare providers. In addition, from the perspective of service users, barriers such as the lack of a stable internet connection, the cost of phones and data packages, and low levels of literacy were identified, particularly in low- and middle-income countries. 5 Consequently, policies should focus on developing technological platforms that are user-friendly and accessible to enhance confidence and acceptance among telehealth users. 178 In addition, policies and healthcare providers should prioritize the promotion and support of digital literacy to facilitate the effective and beneficial use of telerehabilitation. 179
Conclusion
The findings of this systematic review and meta-analysis highlight the effectiveness of telerehabilitation during the COVID-19 pandemic. The majority of the included studies demonstrated significant improvements across all domains of the ICF model following telerehabilitation, compared to either no intervention/usual care or traditional face-to-face PT services provided in clinical settings. These results were observed regardless of the participant group and outcome measures. However, compared to traditional face-to-face PT services, telerehabilitation may not be sufficient to improve the impairment domain of the ICF model as evidenced by the study involving individuals with burn injuries. Additionally, the long-term effects of telerehabilitation remain inconclusive, with some evidence indicating non-significant improvements over extended follow-up periods. In addition to the qualitative synthesis, the meta-analysis provided further evidence supporting the effectiveness of telerehabilitation, particularly for specific conditions. The meta-analysis revealed that compared with no treatment and usual care, telerehabilitation had positive effects on the impairment and activity domains of the ICF model in individuals with COVID-19. The participants in the usual care group did not perform home- or hospital-based exercises. Improvement in the Borg RPE scale in this impairment domain was observed in individuals with COVID-19. Additionally, the 30STST and 6MWT results improved, as reflected by the improvement in the activity domain of the ICF model. Thus, telerehabilitation may be an alternative platform for PT services. However, quantitative assessments using a larger number of studies are required to confirm the findings of the present study. Additional variables reflecting all domains of the ICF model must be investigated in future studies. In addition, the characteristics of participants and interventions must be considered to control the homogeneity and determine the effect of telerehabilitation on other participants.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251325993 - Supplemental material for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-dhj-10.1177_20552076251325993 for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials by Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, Pakaratee Chaiyawat, Kantheera Areerak, Kanjana Niemrungruang and Jarugool Tretriluxana in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251325993 - Supplemental material for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-2-dhj-10.1177_20552076251325993 for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials by Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, Pakaratee Chaiyawat, Kantheera Areerak, Kanjana Niemrungruang and Jarugool Tretriluxana in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251325993 - Supplemental material for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-3-dhj-10.1177_20552076251325993 for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials by Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, Pakaratee Chaiyawat, Kantheera Areerak, Kanjana Niemrungruang and Jarugool Tretriluxana in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251325993 - Supplemental material for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-4-dhj-10.1177_20552076251325993 for Effectiveness of telerehabilitation on the International Classification of Functioning, Disability, and Health framework outcomes during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials by Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, Pakaratee Chaiyawat, Kantheera Areerak, Kanjana Niemrungruang and Jarugool Tretriluxana in DIGITAL HEALTH
Footnotes
Acknowledgements
Financial support from the Physical Therapy Council of Thailand is gratefully acknowledged. Importantly, the authors are also thankful to Assoc. Prof. Sasivimol Rattanasiri, Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Thailand for guidance with a meta-analysis and Professor Jim Richards, Allied Health Research unit, University of Central Lancashire, UK for his invaluable guidance and editing of the first draft of our manuscript. Moreover, we are also thankful to all the researchers who have done research in the field of telerehabilitation for this study.
Contributorship
Conceptualization: Jarugool Tretriluxana, Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, and Pakaratee Chaiyawat. Data curation: Jenjira Thanakamchokchai, Fuengfa Khobkhun, Kanteera Areerak, and Kanjana Niemrungruang. Formal analysis: Jenjira Thanakamchokchai, Ruttana Phetsitong, and Jarugool Tretriluxana. Methodology: Jarugool Tretriluxana, Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, and Pakaratee Chaiyawat. Resources: Jarugool Tretriluxana. Supervision: Jarugool Tretriluxana, and Pakaratee Chaiyawat. Writing—original draft: Jenjira Thanakamchokchai. Writing—review and editing: Jarugool Tretriluxana, Jenjira Thanakamchokchai, Fuengfa Khobkhun, Ruttana Phetsitong, Kanteera Areerak, and Pakaratee Chaiyawat.
Data availability
The data availability has been provided through the supplementary information which can be accessed through the online version of this paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Institutional review board approval was not required as this article was a systematic review of the literature and not original research. However, the protocol for this systematic review was registered in PROSPERO (CRD42021286587).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Physical Therapy Council of Thailand (PTCouncil 1/2564).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.