
Abstract
Objective
Chronic conditions represent a critical threat to the quality of life among older adults, owing to their chronicity and often incurable nature. Meanwhile, many older adults face an eHealth social challenge due to technology anxiety and systemic digital exclusion. Grounded in social cognitive theory and socioemotional selectivity theory, this study examines how online and offline social support aid Chinese older adults with chronic conditions, focusing on the mediating role of health management self-efficacy and the moderating role of online patient-centered communication.
Methods
This study is a national quantitative cross-sectional survey conducted in China from June to October 2023 (n = 4,979), targeting older adults with chronic conditions (n = 721). Mediation and moderation analyses were performed using PROCESS macro for SPSS.
Results
Results showed a significant association between offline social support and healthy lifestyle among Chinese older adults with chronic conditions (β=.135, p <.01), whereas the association between online social support and healthy lifestyle was not significant (β=-.034, p>.05). In addition, health management self-efficacy mediated the association between both online and offline social support and healthy lifestyle (effect=.012, 95%CI [.009,.043]; effect=.032, 95%CI [.023,.042]). Furthermore, a moderating effect of online patient-centered communication was observed in the online social support pathway (β=.160, p<.05).
Conclusions
This study provides empirical evidence on the associations between online and offline social support and healthy lifestyle among Chinese older adults with chronic conditions, with health management self-efficacy as mediator and online patient-centered communication as a moderator. Understanding these relationships can inform interventions designed to enhance health communication, foster social connectedness, and promote well-being among older adults.
Keywords
Introduction
Chronic diseases represent a critical threat to the quality of life among older adults due to their chronicity and incurable nature, 1 necessitating long-term and often lifelong health management. 2 The rapid aging of the global population has led to a higher prevalence of multimorbidity, particularly among community-dwelling older adults, where multiple chronic conditions increasingly coexist. 3 For example, data from the China Health and Retirement Longitudinal Study (CHARLS) indicate that the prevalence of chronic disease comorbidity among Chinese middle-aged and older adults surged from 34.3% in 2015 to 59.9% in 2020. 4 Moreover, national surveys estimate that 81.1% of Chinese older adults have at least one chronic condition, with prevalence peaking at 87.2% among those aged 80-84. 5 This burden of multimorbidity significantly increases treatment complexity and healthcare costs, while also impairing daily functioning. Research has shown that chronic disease and multimorbidity markedly reduce the capacity to perform both basic and instrumental activities of daily living.6,7 In addition, patients with multiple chronic conditions experience a greater treatment burden and reduced health-related quality of life.8,9
In response, health-promoting behaviors, such as balanced nutrition and regular physical activity, are regarded as essential components of chronic disease management. 10 Evidence shows that engaging in physical activity significantly reduces the risks of all-cause and cardiovascular mortality. 11 Moreover, diet intervention such as increasing fruit and vegetable intake and reducing sodium consumption, have been shown to lower the risk of stroke. 12 However, older patients often face challenges in independently maintaining these behaviors. 13 Previous research indicated that among older adults with multiple chronic conditions, limited health knowledge and reduced physical functioning are associated with diminished self-management capacity and poor perceived health status. 13
Within this context, social support, encompassing both offline 14 and online forms, 15 plays a pivotal role in facilitating health-promoting behaviors. Empirical evidence suggests that social support strengthens self-efficacy, thereby contributing to improved health-promoting behaviors in older adults.14,15 For older adults with chronic conditions, offline support offers essential emotional sustenance and practical assistance, 16 whereas online support overcomes spatial and temporal barriers by providing access to a wide range of health information and management tools.16,17 With the rapid growth of digital health in China, older adults are making greater use of online resources and technologies, including wearable devices and mobile health applications.18,19 However, challenges including the digital divide and social isolation limit the effectiveness of these tools, 20 which often fall short of achieving their intended health-promotion goals.20,21 In addition, prior research indicates that as older adults perceive their future time as limited, their social goals shift from seeking information to prioritizing emotional fulfillment and meaningful engagement.22–24 Consequently, they often narrow their social networks, maintaining close ties with family members and long-term friends, which may be sustained through both offline and online communication channels, rather than forming new, less familiar or weakly connected relationships.22–24 In online support contexts, although some assistance is provided by close family members and friends, 25 a substantial proportion of interactions often occur among socially distant or unfamiliar network members through digital platforms.26,27 Compared with support embedded in emotionally close offline relationships, interactions with unfamiliar online users may be less likely to fulfill older adults’ emotionally meaningful goals. 28 Consequently, the shift in social motivation among older population’s may influence digital health adoption and affect the effectiveness of online social support in promoting their health management. 24 These considerations underscore the need to comprehensively examine the relationship between online and offline social support and healthy lifestyle behaviors among older adults with chronic conditions.
Regarding research gaps, the effectiveness of online support for older adults remains a topic of debate.24,29 Some studies suggest that online social support can enhance older adults’ well-being,30,31 while others indicate it may have unintended negative effects, such as increasing anxiety
32
or provoking unnecessary fears.
33
In addition, existing research on older adults rarely adopts a comprehensive perspective on social participation that considers both online and offline social support simultaneously,
24
often focusing on either online or offline participation, or failing to distinguish between the two.24,34 Moreover, intervention research on online patient-centered communication among older adults with chronic conditions in China remains limited.
35
Building on these research gaps and grounded in social cognitive theory and socioemotional selectivity theory, this study examines and compares the associations of online and offline social support with health-promoting behaviors among older adults with chronic conditions, considering the mediating role of health management self-efficacy and the moderating role of online patient-centered communication. The aim is to inform strategies that support the well-being of older adults managing chronic health conditions. Figure 1 displays the conceptual model of moderated mediation based on this thinking. The conceptual model of moderated mediation: Association between online and offline social support and healthy lifestyle among Chinese older adults with chronic conditions, mediated by health management self-efficacy and moderated by online patient-centered communication.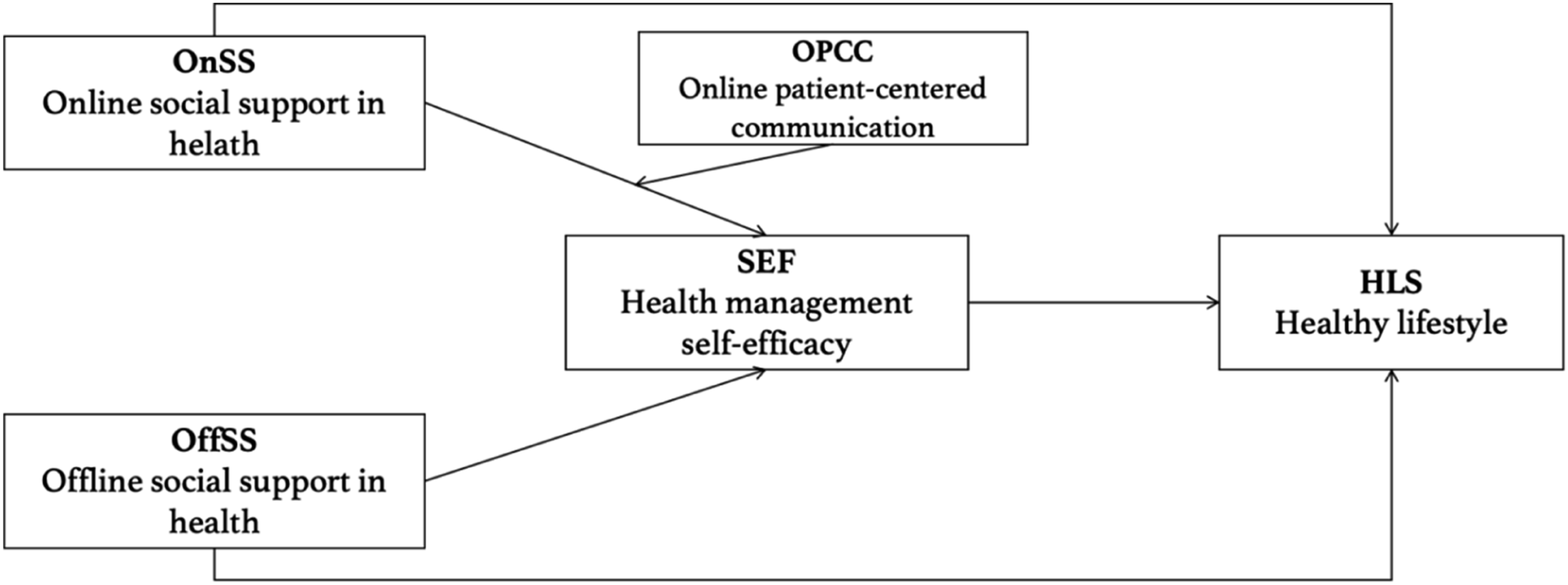
Theoretical framework
Social cognitive theory posits that behavior is shaped by prospective thinking.36,37 In the context of chronic disease self-management, key cognitive determinants include perceptions of health resources, personal goals, and health self-efficacy. 38 According to Bandura’s concept of reciprocal determinism, this study treats health management self-efficacy as an internal personal motivator and social support as an external environmental motivator, 39 acknowledging that external support can strengthen internal self-efficacy and promote health behaviors.40,41
Moreover, this study draws on Socioemotional Selectivity Theory to guide the understanding of perceived external social support among older adults. For older adults living with chronic conditions, the perception of limited lifetime horizons shifts social goals toward emotionally meaningful, present-oriented aims, such as affect regulation and maintaining close relationships, rather than future-oriented objectives like acquiring information or expanding social networks.22,42 Accordingly, older adults tend to narrow their social circles and prioritize emotionally close ties.43,44 For older adults, offline interactions may more consistently provide positive emotional feedback due to their immediacy and relational embeddedness,45–47 whereas a substantial proportion of online social support, particularly loosely structured online communities, tends to emphasize informational or instrumental resources over emotionally meaningful exchanges.48,49 Moreover, interactions in online communities are more likely to involve weak-tie connections, whereas offline support more commonly stems from close family members and friends, reflecting differences in relational closeness across online and offline contexts. 50 This theoretical perspective informs our integrative analysis of online and offline social support and our comparative examination of their respective associations with health-promoting lifestyles.
Formulating hypotheses
Social support, a key concept of this study, is conceptualized as perceived functional support, referring to individuals’ perceptions of the availability of informational, emotional, and instrumental resources provided through social relationships.51,52 Social support is recognized as a motivator that can help individuals progress from the decision-making stage to the action stage. 53 In this study, the “action” of chronic disease management refers to healthy lifestyle behaviors. A healthy lifestyle encompasses patterns of living that promote overall physical and mental well-being while mitigating health risks. 54 Such behaviors include good nutrition, regular physical activity, adequate rest, and stress management. 54 Prior research has demonstrated that actively modifying personal lifestyle can reduce the incidence of chronic diseases and represents a critical component of health management for older adults with chronic conditions. 55
Emerging evidence indicates that online social support can facilitate healthier lifestyles among older adults with chronic conditions.56,57 Previous studies have shown that wearable devices and mHealth applications can increase daily physical activity and improve metabolic outcomes, with interventions targeting older adults demonstrating benefits in step counts, sleep quality, and glycemic control.58,59 Similarly, WeChat-based community programs for middle-aged and older adults with hypertension have enhanced blood pressure management and self-care behaviors, highlighting the value of online peer education and support.
60
In parallel, offline social support from family and close social networks remains a key determinant of lifestyle adherence among older adults with chronic conditions. Instrumental support from family, such as medication reminders, shared meal preparation, and accompaniment to medical appointments, has been consistently linked to better medication adherence
61
and healthier dietary practices.62,63 Moreover, emotional support from spouses and children has been shown to reduce psychological distress,
64
enhance self-efficacy,
65
and foster sustained engagement in physical activity.44,64,65 Accordingly, this study proposed the first and second hypotheses:
Health management self-efficacy is conceptualized as an individual’s confidence in their ability to make decisions and undertake actions that lead to positive health outcomes.
66
This study regards health management self-efficacy as a critical internal factor in the health management of older adults with chronic conditions.
39
In contemporary society, the development of digital health has significantly facilitated healthy aging.
67
Nevertheless, older adults with chronic conditions continue to face substantial barriers, including the digital divide,
68
social isolation,
69
and technology-related anxiety.
70
With this context, social support assumes particular importance.
71
According to social support theory, perceived online and offline support constitutes a form of social capital that older adults can utilize.41,72 Receiving assistance in achieving health goals through such support reinforces their belief in effectively leveraging this capital within a digital context, thereby enhancing confidence in health management and strengthening self-efficacy.16,73 For instance, structured online health communities and remote support groups for older adults with chronic conditions, including type 2 diabetes, arthritis and chronic obstructive pulmonary disease, have been shown to facilitate peer modeling and professional encouragement, thereby enhancing participants’ self-efficacy in chronic disease self-management.
74
In addition, previous studies indicate that the management of older patients with chronic obstructive pulmonary disease (COPD) highlights the role of offline social networks in supporting self-management and enhancing self-efficacy.
75
Therefore, this study posits the third and fourth hypotheses:
The achievement of self-directed change occurs when an individual understands the impact of personal behaviors on well-being, believes in their capacity to influence outcomes through effort and available resources, and is motivated to act accordingly.
39
Previous research indicates that chronic disease self-management improved with enhanced self-efficacy.76,77 Among older adults with chronic conditions, health management self-efficacy is shaped by social capital and support, as recognizing one’s ability to engage in effective self-management through these resources further strengthens self-efficacy,16,78 which in turn can promote healthier lifestyle behaviors.79,80 Consequently, self-efficacy may serve as a mediator between social support and health lifestyle in this population. Thus, this study posits the fifth and sixth hypotheses:
Additionally, regarding social support, previous research suggests that older adults tend to prioritize offline interactions that provide positive emotional feedback over large, complex online networks, which often involve weaker social ties and potential challenges such as misinformation, technology-related anxiety, and challenges in establishing and maintaining meaningful online relationships.22,24,70,81 Building on older adults’ preference for emotionally oriented goals22–24 and the challenges they encounter in online social participation, this study tries to examine the moderating role of online patient-centered communication in shaping the effectiveness of online social support. Within the patient-centered communication approach, the dimension of “effective interpretation and education of health information” enhances the credibility and clarity of information, thereby reducing anxiety stemming from information overload and uncertainty.
82
Furthermore, the emphasis on emotional responsiveness in patient-centered communication is consistent with older adults’ orientation toward emotionally meaningful interactions.83,84 Empirical evidence also suggests that online patient-centered communication can strengthen older adults’ confidence in managing their health.35,85 In addition, prior studies have incorporated patient-centered communication (PCC) as a moderating variable, examining its role in shaping the relationship between online health information use and health outcomes,
86
as well as between minority stress and psychological well-being.
87
Therefore, this paper posits the eighth hypothesis:
Methods
Data sources
This study draws on primary data collected through the Chinese national health survey organized by the corresponding authors’ research team. Research ethics approval for this study was obtained from the first author’s institute, with ethics application reference number SSHRE23-APP013-FSS. This study is a quantitative cross-sectional study implemented with the assistance of Kantar Company between June and October 2023, using quota random sampling method to recruit a total of 4,979 adults from Mainland China. The quotas were set based on age and gender distributions according to the Seventh National Census by the National Bureau of Statistics of China (https://www.stats.gov.cn). Random sampling was then used within each quota cell to reduce sampling bias. Before participation, respondents received an information sheet describing the study’s purpose, the voluntary nature of participation, and the confidentiality of their responses. Written informed consent was obtained from all participants prior to data collection. For the purposes of this study, we focus on a subsample of older adults living with chronic conditions (n = 721).
Sample criterion
This study focuses on older adults with chronic conditions. The first criterion is age. Consistent with the World Health Organization definition and national statistical standards, participants aged 60 years and older were classified as older adults in developing countries. 88 This criterion is widely used in studies on aging 89 and chronic conditions studies. 90 The second criterion aligns with previous studies that include individuals diagnosed with chronic conditions. The presence of chronic conditions was assessed via a self-report checklist of physician-diagnosed diseases. The selection of conditions (including obesity/high blood sugar, hypertension, cardiac problems, chronic lung disease, arthritis) was informed by established comorbidity indices, notably the Elixhauser comorbidity measure, 91 which identifies chronic physical health conditions that are significant drivers of healthcare utilization and outcomes.
Variables and measurements
Healthy lifestyle is an ensemble of behaviors in daily life that help promote health. 54 It is measured using three questions, originated from the well-established Health-Promoting Lifestyle Profile II (HPLP-II).92–94 The first question is about sleep, physical activity and social activity. The respondents were asked whether the following behaviors were consistent with their deed circumstances: (a) “Sleep about eight hours a day”; (b) “A regular routine”; (c) “Be active in fitness”; (d) “Have regular exercise”; I “Participate in enjoyable activity”; (f) “Have suitable relaxation time”. (1= not at all to 5 = fully consistent). The other two questions are about healthy eating: “How many fruits do you eat every day?”; “How many vegetables do you eat every day?” (M =3.70, SD =0.72, Cronbach’s alpha=0.84).
Social support is conceptualized in this study as perceived functional support, referring to individuals’ perceptions of the availability of informational, emotional, and instrumental resources provided through social relationships, both online and offline.52,95 This functional framework is proposed by House 52 and widely adopted in subsequent health research.51,96 The operationalization of online and offline social support are informed by the measurement structure of the Medical Outcomes Study Social Support Survey (MOS-SSS) guided by this framework. 97 For online social support, respondents were asked whether their online health activities make them feel they can: (a) Feel able to find useful health information in online community; (b) When participating in an online community or support group, I feel that I receive practical advice and support from people with similar health concerns; (c) Feel that others in community will provide them with emotional support when they needed. Responses were coded (0=no, 1=yes) to indicate the presence or absence of each type of support, consistent with prior empirical research.98–100 The three items were summed to create an index (range = 0-3), with higher scores indicating greater perceived availability of online social support (M= 1.77, SD= 0.92, Cronbach’s alpha=0.72). Offline social support, defined as support from others offline, was measured using nine items to reflect the informational, emotional, and instrumental construct. The question was “To what extent do you agree with the following statements”: a) I can talk about health issues with my family; b) my family tries to help me in practice; c) I get emotional help and support from my family; d) I can talk about health issues with my friends; e) my friends try to help me in practice; f) I get emotional help and support from my friends; g) I can talk about health issues with a special person; h) there is a special person who tries to help me in practice; i) I get emotional help and support from this special person (1=never to 5=always). (M= 3.84, SD= 0.82, Cronbach’s alpha=0.82).
Health management self-efficacy is defined as a person’s belief in their ability to effectively manage and maintain their health.66,101 In this study, health management is operationalized with five items, drawn from Perceived Health Competence Scale 102 and has been employed in subsequent studies including the Perceived Diabetes Self-management Scale. 103 Respondents were asked to indicate the extent to which the following statements reflected their actual situation: a) I am capable of managing my health conditions when they arise; b) I am skilled at using various aids and tools to make my daily life easier; c) I possess effective skills to help me handle health-related issues; d) I have good strategies for managing health problems; e) I have many effective methods to prevent certain diseases. The answers were measured using a five-point Likert scale (1=strongly disagree to 5=strongly agree). (M=3.74, SD=0.67, Cronbach’s alpha=0.80).
Patient-centered communication is a healthcare approach that focuses on understanding and responding to patients’ needs, preferences, and values, ensuring that patients’ perspectives guide all clinical decisions.104,105 It involves effective information exchange, emotional support, shared decision-making, and fostering a therapeutic relationship that respects the patient as a whole person.104,105 In this study, online patient-centered communication (OPCC) refers to patients’ evaluative perceptions of the quality and effectiveness of physician-patient communication delivered via online channels, rather than to the structural or affordance-based features of the platforms (e.g., synchronicity, modality, or continuity). The measurement of perceived online PCC scale is originated from the three sub-constructs from Epstein and Street’s functional model: exchanging information, responding to emotions, and fostering healing relationships. 106 These sub-constructs have also been applied in the Chinese context in previous studies.107,108 Each construct was assessed with three items. For exchanging information, respondents indicated their level of agreement with the following statements about their experiences communicating with doctors online: a) “My online doctor provided detailed explanations of my health condition”; b) “My online doctor demonstrated a thorough understanding of my health status”; c) “My online doctor’s explanations and recommendations were clear and understandable” (M=1.98, SD=0.62, Cronbach’s α =0.73). For responding to emotions, respondents indicated their agreement with the following statements: d) “My online doctor showed genuine interest in my health”; e) “My online doctor made efforts to reassure and comfort me”; f) “My online doctor was attentive to my feelings” (M=2.05, SD=0.66, Cronbach’s α =0.80). For fostering healing relationships, respondents indicated their agreement with the following statements: g) “My online doctor encouraged me to express concerns and worries”; h) “My online doctor sought my opinions on how to manage my condition”; i) “My online doctor inquired about my views on health” (M=2.03, SD=0.66, Cronbach’s α =0.73). These three core dimensions are consistent with theoretical foundation of Socioemotional Selectivity Theory in this study, which posits that older adults prioritize emotionally meaningful goals, this operationalization emphasizes emotionally meaningful and patient-centered responsiveness in online medical communication contexts.43,109 Responses were recorded on a 5-point Likert scale (1 = Strongly Disagree; 2 = Disagree; 3 = Neutral; 4 = Agree; 5 = Strongly Agree). Higher scores indicated a greater perception of patient-centered communication with online physicians. (M=2.03, SD=0.56, Cronbach’s α =0.85).
Sociodemographic variables were used to reduce the confounding effects, including age (ranging from 60 to 74), education level (1= primary and below to 7= bachelor’s degree or above), birth gender (male and female) and annual household income (1= ¥30,000 to ¥80,000 to 5= ¥1000,000 or above). To better control the potential variables that could influence main variables, related variable psychological distress was included in this study. Previous study indicated that psychological distress is associated with social support 110 and health self-efficacy among chronic disease patients. 111 The psychological distress variable was measured using a 4-item scale derived from the Patient Health Questionnaire-4, 112 a screening tool that assesses core symptoms of depression and anxiety and has been widely used in health research.113,114 Participants were asked to indicate how frequently, over the past two months, they had been troubled by the following issues: (a) having little interest or pleasure in activities, (b) feeling down, depressed, or hopeless, (c) feeling nervous, anxious, or on edge, and (d) being unable to stop or control worrying. (M=1.80, SD=0.63, Cronbach’s α = .80).
Statistical methods
All analyses were conducted using SPSS version 28. First, descriptive analyses were processed to show the characteristics of the main variables. Second, Pearson correlation analysis was used to explore associations among the core variables. Third, before conducting PROCESS macro analysis, a multicollinearity check was conducted for the three key predictors (online and offline social support, and health management self-efficacy) in the regression predicting healthy lifestyle.115,116 Fourth, the proposed mediation was tested using the PROCESS macro (Model 4) in SPSS. 117 To address potential overlap between online and offline social support, each support index was controlled for when estimating the effects of the other in the PROCESS analyses. The PROCESS macro, developed by Andrew Hayes, is an added-on tool for SPSS that supports advanced statistical methods including mediation and moderation analyses. 117 Indirect effects were evaluated using the bias-corrected bootstrap method with 5,000 resamples, and effects were deemed significant when their 95% confidence intervals did not include zero. 118 Additionally, PROCESS model 7 is used to test the moderation effect of online patient-centered communication on the association between online social support and health management self-efficacy among older adults with chronic conditions.
Results
Descriptive data
Descriptive statistics of the independent, dependent, mediating and controlling variables (n = 721; sub-group: older adults with chronic conditions).

SD: standard deviation; M: mean; N/A: not applicable.
Relationships among key variables
Zero-order Pearson correlations (n = 721).

Association among online social support, offline social support, health management self-efficacy and healthy lifestyle
Summary of mediation effects (n = 721).

Note. b is regression unstandardized coefficients B and bp is percentage coefficients

Association between online and offline social support and healthy lifestyle mediated by health management self-efficacy among Chinese older adults with chronic conditions.
The moderation effect of OPCC on the association between online social support and health management self-efficacy among Chinese older adults with chronic conditions.
Discussion
This study examines the direct and indirect associations between online and offline social support and healthy lifestyle among Chinese older adults with chronic conditions, with particular attention to the mediating role of health management self-efficacy. Furthermore, online patient-centered communication is included in the online support pathway as a moderating factor. These findings not only explain how online and offline social support are associated with healthy lifestyle, but also extend the application of social cognitive theory and socioemotional selectivity theory to the context of chronic disease management among Chinese older adults. The following section provides a detailed discussion of the results.
Significant mediation and non-significant direct association in online support pathway
Echoing previous research, this study replicated positive associations between offline social support and healthy lifestyle,61–64,120 as well as between health management self-efficacy and healthy lifestyle among older adults with chronic conditions.77,121,122 In addition, the findings demonstrate the mediating role of health management self-efficacy in the relationship between social support and healthy lifestyle in this population. It is noteworthy that the direct effect of online social support on a healthy lifestyle was not significant; however, health management self-efficacy significantly mediated this association. Importantly, this finding should not be interpreted as evidence that online social support is inherently ineffective or emotionally superficial for older adults. Rather, it suggests that the effectiveness of online social support operates through more indirect and conditional pathways. In this study, online social support was measured as the perceived ability to obtain useful health information, participate in peer communities, and receive emotional support when needed. These elements reflect informational, instrumental, and emotional availability rather than direct behavioral guidance. As such, they may not immediately translate into routine behaviors such as regular exercise or sleep. Instead, they are more likely to strengthen individuals’ confidence in managing health conditions, using appropriate tools, and applying effective strategies, which are core dimensions of health management self-efficacy. For instance, perceiving access to useful information may enhance confidence in handling symptoms or making dietary decisions, 123 while interaction with people with similar health concerns may provide social modeling 124 and emotional reassurance might reduce uncertainty. 125 Through these processes, online social support operates as a cognitive and motivational resource that enhances perceived competence in health management. For older adults with chronic conditions, access to such support alone is insufficient. What proves essential is their perceived self-efficacy, sense of empowerment and the emotional significance they attach to these experiences. 14 When older adults recognize their capacity to effectively use online social support, their confidence in managing chronic conditions increases, which is associated with greater engagement in health-promoting behaviors.16,78
These results align with Socioemotional Selectivity Theory (SST), which emphasizes that older adults’ social preferences are guided by goal orientations rather than by communication media itself.22–24 As perceived future time becomes limited, older adults increasingly prioritize emotionally meaningful, present-oriented goals over future-oriented goals such as information accumulation or network expansion.22,23,81 Within this framework, online and offline social support should be understood as differing in their dominant functional emphases rather than representing mutually exclusive or homogeneous categories. While offline interactions may more consistently facilitate emotionally meaningful exchanges due to their immediacy and relational embeddedness, 126 emotionally close and meaningful support can also be delivered through online channels, particularly when interactions involve close family members or long-standing social ties (e.g., intergenerational communication via WeChat). 127 Therefore, the absence of a direct effect does not diminish the potential value of online social support; instead, it underscores the importance of psychological mechanisms, including health management self-efficacy, that enable older adults to translate online support into concrete health behaviors.
Positive moderation effect of online patient-centered communication
Although the direct effect was not significant, the positive indirect associations between online social support and healthy lifestyle through health management self-efficacy highlights the potential benefits of online support. Furthermore, this study identified a positive moderating role of online patient-centered communication within the online support pathway. This finding aligns with Socioemotional Selectivity Theory, which posits that when lifetime horizons are perceived as limited, older adults increasingly prioritize emotionally meaningful goals.22,23 In the context of online physician-patient communication, patient-centered communication delivered by online doctors is more likely to meet older patients’ needs to feel understood, reassured, and emotionally supported. 128 In addition, the moderating effect of OPCC in this study highlights the value of authoritative, patient-centered communication in shaping how community-based online support is interpreted and utilized. Although online social support from communities members often provides experiential advice and emotional encouragement, the medical appropriateness and individual applicability of such information may be uncertain. 129 When OPCC is of high quality, online doctors can respond to patients’ concerns, clarify misunderstandings, and offer structured and personalized guidance.130,131 This process enables patients to integrate online community-based information with professional medical advice, thereby enhancing their confidence in managing their health. Additionally, this interpretation is further supported by prior research using HINTS data, which demonstrated that online patient-centered communication was positively associated with higher self-efficacy among patients with chronic conditions. 132 Therefore, these findings suggest that the perceived quality of patient-centered physician communication through online channels may strengthen the positive association between online social support and health management self-efficacy among Chinese older adults with chronic conditions, thereby contributing to better overall health and well-being.
Practical implication
In terms of practical implications, firstly, this study underscores the importance of both online and offline social support for older adults with chronic conditions. Family members, friends, and online communities should engage in timely communication with patients about their health issues and give them information support, as well as participate in their daily routine of health management to give them emotional support such as a sense of companionship and reassurance. Secondly, the findings indicate a significant indirect association between online social support derived from online communities and a healthy lifestyle via health management self-efficacy, whereas the direct association was not significant. This finding suggests that simply providing online support may be insufficient, and its benefits rely on enabling older adults to effectively use the support, which builds their self-efficacy and internal motivation for managing their conditions. Accordingly, the design and implementation of health interventions should prioritize empowering patients through the creation of a supportive environment. For example, to enhance older adults’ perceived ability to obtain useful health information, communities should provide curated and clearly organized content, such as pinned evidence-based posts, simplified symptom-management guides, and searchable Q&A sections addressing common concerns (e.g., medication use, diet, exercise). 48 Short instructional videos demonstrating home-based practices may further translate information into actionable skills, strengthening users’ confidence in applying effective strategies. 133 To leverage peer interaction, communities can incorporate structured experience-sharing threads or highlight members’ coping strategies to facilitate social modeling. Such visibility of practical success may reinforce beliefs in older adults’ own ability to manage chronic conditions. 134 Thirdly, this study highlights the moderating role of online patient-centered communication, suggesting that online support from community may be most effective when complemented by structured physician involvement that embodies patient-centered communication. For example, in a physician-driven social media group for older adults with chronic conditions, physicians could periodically review common questions, provide clear and accessible explanations, and clarify misunderstandings arising from experiential advice shared by community members. 135 Beyond clarification, physicians can encourage patients to articulate concerns and reflect on how recommended strategies fit their daily lives. In this way, online patient-centered communication strengthens older adults’ confidence in symptom management, practical tool use, and prevention. In addition, given the large number of older adults in China who regularly watch short dramas on the Douyin platform (Chinese TikTok), health education by healthcare professions on chronic disease management could be integrated into short-video storytelling. In practice, it is vital not only to provide support, but it is also crucial to consider how to facilitate the effective use of this support. Achieving this requires disseminating health knowledge, strengthening oversight of online health information, and improving patients’ health literacy, but most importantly, carefully addressing the genuine needs and concerns of older adults through appropriate responses in medical practice.
Limitations and future research
This study has several limitations. Firstly, the cross-sectional design of the study restricts the ability to establish causal relationships to gain a more accurate understanding of the causal links among social support, health management self-efficacy and healthy lifestyle, experimental research and panel research are essential. Secondly, for the measurement of variables, although both online and offline social support were operationalized based on functional support dimensions, the measurement of offline support is necessarily more concrete due to the identifiable nature of offline relationships (e.g., family and friends), whereas online support reflects more diffuse and community-based interactions. Future research could benefit from more parallel measurement instruments across online and offline contexts. In addition, further exploration through in-depth interviews is proposed, focusing on specific aspects of information and emotional support within online and offline social support for a more nuanced and comprehensive investigation. Thirdly, the operationalization of online patient-centered communication in this study captures patients’ perceived communication quality delivered via online channels, but does not assess the structural or affordance-related characteristics of online interaction (e.g., synchronicity, platform modality, continuity of communication, or engagement patterns). Future research could incorporate measures of online interaction affordances to better distinguish between communication quality and platform-based interaction processes. Fourthly, the sample size was determined by feasibility considerations and data availability rather than a formal a priori power calculation. Nevertheless, the final sample of older adults with chronic condition (N = 721) exceeds the sizes typically required for regression-based mediation analyses. Future studies should incorporate formal power analyses at the design stage to improve methodological planning and transparency. Finally, this study regards health management self-efficacy as a significant mediator in the relationship between social support and healthy lifestyle among older adults with chronic conditions, potentially overlooking other pertinent intervening variables. Future research should strive to bridge this research gap by investigating factors such as socioeconomic, family relationships, healthy lifestyle cognitive beliefs and social exclusion.
Conclusion
Drawing on social cognitive theory and socioemotional selectivity theory, this study provides empirical evidence regarding the relationships between online and offline social support and healthy lifestyle among Chinese older adults with chronic conditions. Our findings indicate offline social support is positively associated with healthy lifestyle, whereas online support shows no statistically significant association. Health management self-efficacy significantly mediated the associations of both online and offline social support with healthy lifestyle. Furthermore, online patient-centered communication significantly moderated the association between online social support and health management self-efficacy. Recognizing these relationships can inform the design of interventions aimed at strengthening health communication, fostering social connectedness, and promoting overall well-being in older populations.
Supplemental material
Supplemental material - Factors associated with healthy lifestyles in Chinese older adults with chronic conditions: A comparison of online and offline social support, mediated by health management self-efficacy and moderated by online patient-centered communication
Supplemental material for Factors associated with healthy lifestyles in Chinese older adults with chronic conditions: A comparison of online and offline social support, mediated by health management self-efficacy and moderated by online patient-centered communication by Qingqing Xie, YingXia Zhu and Xinshu Zhao in Digital Health.
Footnotes
Ethical considerations
Research ethics approval for this study was obtained from the Institutional Review Board of the University of Macau, with application reference number SSHRE23-APP013-FSS. Before the survey, each participant was provided with a participant information sheet that explained the purpose of the study, the voluntary nature of participation, and the confidentiality of their responses.
Consent to participate
An informed consent sheet was obtained from all participants before their involvement in the study.
Author contributions
The author contributions for this manuscript are as follows: Qingqing Xie conceptualized the model and wrote the original draft of the manuscript. YingXia Zhu contributed to method. Xinshu Zhao served as the guarantor for the research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by grants of University of Macau, including CRG2021-00002-ICI, ICI-RTO-0010-2021, Xinshu Zhao PI; Macau Higher Education Fund, HSS-UMAC-2020-02, Xinshu Zhao PI.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available from the corresponding author upon reasonable request.
Use of artificial intelligence
During the preparation of this manuscript, the authors used the AI tool ChatGPT (OpenAI) to assist with improving the clarity and readability of the language. No substantive content, results, or conclusions were generated by AI, and the authors take full responsibility for all content.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.