
Abstract
Background
The exponential growth of artificial intelligence (AI) in healthcare has raised critical ethical concerns.
Aims
To systematically identify research hotspots and trends of AI ethics in the medical field and provide evidence-based insights for future research.
Methods
A bibliometric analysis was conducted on publications from the Web of Science Core Collection (WOSCC) and China National Knowledge Infrastructure (CNKI) up to August 24, 2025. Visualisation tools were used to map the publication trend, as well as author, country, institution, journal, and keyword distributions. Keyword co-occurrence networks, clustering and burst analysis were employed to identify research hotspots and evolving trends. The results are reported following the BIBLIO checklist.
Results
A total of 1034 publications (291 from CNKI, 743 from WOSCC) were included. Key journals were Chinese Medical Ethics (CNKI) and Journal of Medical Ethics (WOSCC). China (n = 291) and the USA (n = 174) were the top publishing countries in CNKI and WOSCC, respectively. Leading institutional output came from developed countries (e.g., Harvard University, University of London, University of Toronto). Four research hotspots were identified: 1) ethical issues in different application scenarios of AI techniques in clinical practice, 2) AI ethical concerns and considerations in medical academia, 3) ethical challenges in AI-driven medical education, and 4) ethical governance, supervision, and review in healthcare. Keyword burst analysis indicated an increasing attention on balancing AI development with ethical governance, promoting research on complex intelligent tools embedded with ethical principles.
Conclusion
Attention to this topic has grown steadily over the past eight years. Research trends reflect a shift from fragmentation to the integration of technology and ethics in medicine. Future research should further refine the operational definitions of ethical principles across diverse application scenarios to guide stakeholders in effectively integrating technology and ethics.
Introduction
The rapid advancement of artificial intelligence (AI) is driving a profound transformation in healthcare. AI technology has permeated various critical domains, including disease prediction, screening, diagnosis, treatment, and surveillance, medical imaging analysis, predictive analytics and risk assessment, clinical decision support, robot-related research, virtual and remote assistance, mental health support, medical education, training and consultation.1–5 These applications enhance diagnostic accuracy, improve work efficiency, and ultimately lead to better patient outcomes. 1 However, this proliferation has also raised pressing ethical concerns, including challenges to the integrity of informed consent, 6 data security and privacy risks, algorithmic bias and opacity, rigid regulatory frameworks, insufficient rigour in ethical review processes, gaps in governance, and the issues of patient acceptance and trust in AI solutions, all of which demand immediate and thoughtful resolution.7,8
These pressing challenges have garnered significant academic attention. Scholars have conducted bibliometric analyses on this topic from diverse perspectives, covering health big data privacy protection, 9 ethical issue categorisation in AI-driven healthcare, 10 AI advancement in health and medicine,11,12 AI trends in critical care medicine 13 and AI-enabled medical education.14,15 Overall, from a macroscopic perspective, the focus of these studies is relatively dispersed, hindering a comprehensive grasp of this field. Furthermore, most studies tend to describe research hotspots from a static perspective, with no trend analysis of hot keywords. Additionally, most review papers exhibit language bias due to their reliance on monolingual sources.16–18 This often overlooks valuable research published in other languages (e.g., Chinese), creating a gap in the literature.
Therefore, this study aims to address the aforementioned research gaps by incorporating publications from both English and Chinese academic databases. This approach leverages the complementary nature of these sources to mitigate language bias and provide a more comprehensive and systematic overview of dynamic global research hotspots and evolving trends. The findings are expected to offer valuable insights for future research, standardisation, and policy formulation. This will help safeguard patient rights and public interests, ensuring that medical AI technology contributes to the well-being of human society.
Materials and methods
Search strategy
The China National Knowledge Infrastructure (CNKI) and Web of Science Core Collection (WOSCC) databases were systematically searched from database inception to August 24, 2025. The search strategy was developed through discussions among the authors (JLL and BLL), based on a review of similar literature and expert opinions (QSZ) in the field of evidence-based medicine. Search terms encompassed “AI”, “artificial intelligence”, “medic”, “medics”, “medical”, “medicine”, “ethic”, and “ethics”. Considering that the “ethic” and “medic” have multiple lexical variants, truncation symbols were incorporated in our search query (WOSCC). The detailed search strategies are provided in Supplementary File 1.
Eligibility criteria
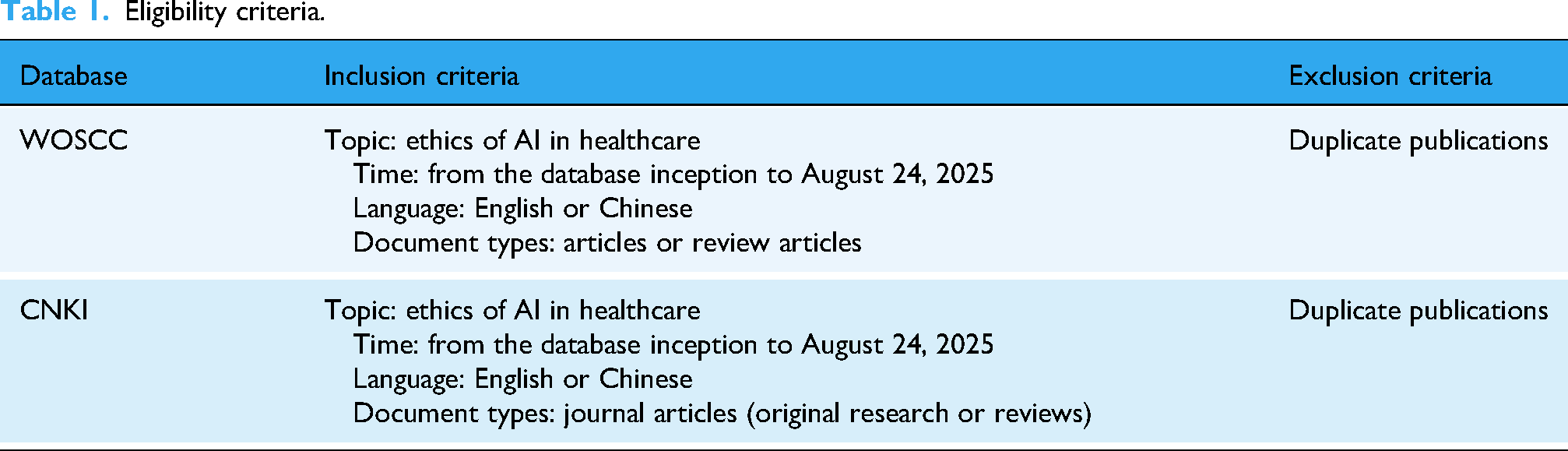
Two authors (JLL and BLL) established the selection criteria through deliberation. We aimed to include studies on the ethics of AI in clinical settings. The detailed eligibility criteria are presented in Table 1.
Eligibility criteria.
Study screening and selection
Two researchers (JLL and BLL) independently performed the initial search, yielding 1403 records from WOSCC and 448 records from CNKI. Following the eligibility criteria, a total of 1537 records (364 from CNKI, 1173 from WOSCC) were imported into EndNote 20.0 for screening. After removing duplicates, further screening was conducted by JLL and BLL, who comprehensively reviewed titles, abstracts, and keywords. Discrepancies were resolved through consensus discussions within the research team to confirm thematic relevance (JLL, BLL, and YJQ). This multistage selection process resulted in 291 Chinese and 743 English publications (1034 total) for subsequent analysis. The entire process of study searching and selection is shown in Figure 1. Related records are shown in Supplementary File 2.

Studies screening and selection flow diagram.
Data extraction and import
The titles, abstracts, authors, keywords, and other metadata of eligible publications were extracted and exported. Chinese publications were formatted in RefWorks, while English publications were in RIS format. Both datasets were saved as “download_.txt” files and imported into CiteSpace 6.4.R1 software for analysis. WOSCC data were directly compatible with the software, whereas CNKI data required format conversion to ensure interoperability. Given the language difference in data format and structure between WOSCC and CNKI, separate data import and analysis were conducted for each database.
Data analysis
Data analysis included descriptive analysis and visual analysis. Data were initially collated and summarised in Microsoft Excel for descriptive analysis, which included the annual trends in publication output and the distribution of the number of journal publications. Author, country, institution, and keyword (co-occurrence, clustering, and burst) visualisation analyses were primarily performed using CiteSpace software. A 1-year time slice was adopted, with the time spans set as 1999–2025 for WOSCC and 2017–2025 for CNKI. Term extraction sources included title, abstract, author keywords (DE), and keywords plus (ID). Nodes were sequentially selected as author, institution, country, and keyword for corresponding analysis. The g-index threshold was set to k = 25, while all other parameters were configured as default values. Detailed software configurations can be found in Supplementary File 3.
Results
Distribution of publication time and journals
Annual publication trends
Publications in this field have demonstrated a gradual upward trend overall. The earliest record in CNKI dates back to 2017, focusing on AI applications in biomedicine and strategies for addressing legal and ethical challenges. 19 In contrast, the earliest record in WOSCC dates back to 1999, with initial studies concentrating on the ethical implications of electronic health records. 20 Following these early publications, both databases experienced a prolonged period of low output. Sustained growth began around 2017, with a more pronounced increase after 2018. In comparison, the growth within CNKI has been more gradual. Given that data for 2025 are incomplete (cutoff date: 24 August 2025), we tentatively identify 2025 as the peak year for Chinese publications (Figure 2).

Annual trends in publication output.
Ranking of the number of journal publications
Journals with the highest publication output in this field are presented in Table 2. For CNKI publications, Chinese Medical Ethics leads with 38 articles, followed by Medicine and Philosophy. For WOSCC publications, the Journal of Medical Ethics has the highest output (37 articles), followed by the Journal of Medical Internet Research.
Key journals and publication counts.

Publication volume of country/institution
In WOSCC, the top five countries by publication count were the USA (174 articles), Germany (62 articles), China (55 articles), the UK (50 articles), and Australia (40 articles). Since all publications in CNKI (291) were from China, a cross-database deduplication was performed. The results confirm that China and the US are the top publishing countries in CNKI and WOSCC, respectively. Research on the ethical issues of AI in the medical field was initiated earlier in developed countries. However, the substantial publication volume from China indicates a growing focus on this topic among major developing economies.
Further analysis of institutional publication output shows that Harvard University (USA) and University College London (UK) rank first and second, with 25 and 24 articles published, respectively, followed by the University of Toronto (Canada) in third place with 22 articles. Notably, although China leads globally in total publications, no Chinese institution ranks among the top global publishers. Within China, the most prolific institution is the School of Humanities and Social Sciences at Peking Union Medical College, with four articles (Table 3).
Ranking of the number of publications.

Node type: institution.
Research team and author analysis
In the WOSCC database, prominent research teams include those led by Buyx (Technical University of Munich, Germany) and Savulescu (National University of Singapore, Singapore), each with seven publications. Buyx's team focuses on embedding ethics into the development of AI in medicine, whereas Savulescu's team focuses on ethical considerations pertaining to AI applications in medical settings.
In CNKI, the leading research team is headed by Fei Xu from the University of Science and Technology of China, having published four articles to date. Their research primarily addresses gaps in the soundness, maturity, supervision, and governance of ethical norms, as well as innovations in embedding ethical values, formulating ethical practice guidelines, and improving review mechanisms. A co-authorship analysis indicates that Xin Huang and Tianwei Yuan, who rank among the most productive, have collaborated on ethical issues in medical safety, life sciences, biology, ecological safety, and other domains in the context of emerging medical technologies (including AI, gene editing, 3D printing, and biotechnology).
Frequency of hot keywords
Analysis of WOSCC data shows that the top five most frequent keywords are “AI”, “medical ethics”, “machine learning”, “medical informatics”, and “general & internal medicine”. Analysis of CNKI data reveals the top keywords to be “AI”, “medical ethics”, “ethics”, “ethical review”, and “ethical issues”. These findings indicate that scholars pay substantial attention to ethical issues of AI in clinical application (WOSCC) and the construction of ethical governance, review, and regulatory frameworks (CNKI). Detailed keyword co-occurrence patterns are presented in Figure 3(a) and (b), respectively.

Co-occurrence of hot keywords (a) co-occurrence of hot keywords in CNKI, Node = 153, Link = 297; and (b) co-occurrence of hot keywords in WOSCC, Node = 392, Link = 1557. Node type: keyword, Link: connection of keywords.
Keyword co-occurrence analysis
Keyword co-occurrence analysis was performed on the 291 CNKI and 743 WOSCC publications, resulting in networks of 153 nodes and 297 connections for CNKI, and 392 nodes and 1557 links for WOSCC. In these networks, nodes represent keywords and links represent co-occurrence relationships. Key metrics include “frequency” (the occurrence count of a keyword), “betweenness centrality” (the positional importance of a node in the network), and “year” (the year the keyword first appeared). 21 Key nodes were selected based on high frequency and a betweenness centrality value of ≥0.1. Notably, some nodes in the CNKI network had betweenness centrality values exceeding 1. As defined by Chen, 22 betweenness centrality measures the proportion of all shortest paths in a network that pass through a given node. Following verification, we applied max normalisation for normalisation (Table 4). The detailed raw and normalised values are shown in Supplementary File 4.
Statistics of keywords with high centrality rankings.

Node type: keyword. Normalisation formula: Xnormalised = (x − xmin)/(xmax − xmin), X∈[0, 1].
For WOSCC studies, key research hotspots include: 1) Ethical challenges associated with the application of core AI technologies (e.g., machine learning, big data, deep learning, large language models) in healthcare settings; 2) AI applications within specific healthcare subfields; 3) Core research focuses and challenges (e.g., informed consent, social issues, health data); 4) Ethical dimensions of AI integration in medical education.
For CNKI studies, key research hotspots centre on: 1) Ethical issues, dilemmas, and risks of AI applications in healthcare; 2) Ethical review frameworks, monitoring, and governance for intelligent healthcare systems; 3) Ethical issues in talent cultivation, medical humanities, and medical education; 4) AI-driven transformations in physician-patient relationships and principles of justice, dignity, and fairness in medicine.
In summary, there is a global focus on the ethical challenges of AI in clinical practice and medical education. We further reviewed articles associated with key nodes (from CNKI and WOSCC) and highly cited papers identified through reference analysis in WOSCC (Supplementary File 5). A core topic common to both databases is AI-driven academic issues in medicine. Methodologically, studies in the CNKI database primarily employed literature analysis or descriptive reviews to discuss the construction of ethical review and governance. In contrast, studies in the WOSCC database employed a wider variety of research methodologies to explore a broader range of topics (Table 5).
Diverse methodologies in WOSCC.

Keyword cluster analysis
Keyword co-occurrence networks can be further analysed through clustering to identify distinct research themes. Based on network structure and clustering validity, CiteSpace generates Modularity Q and Mean Silhouette S values, which are key metrics for evaluating cluster quality. Generally, Q > 0.3 indicates a significant community structure. S = 0.7 signifies high clustering reliability, and values S > 0.5 are generally considered reasonable. 41 This study yielded nine Chinese clusters (Q = 0.5502, S = 0.8943) and eight English clusters (Q = 0.4583, S = 0.7222), both of which demonstrate significant network community structures and high clustering reliability. Detailed information is presented in Table 6. The clustering results reveal that global research attention focuses on several core themes: “Clinical Applications of AI Technologies”, “AI in Medical Education”, “AI in Biological Heredity”, “Ethical Principles and Issues”, and “Turing Test” globally.
Cluster analysis of keywords.

Choose keyword sources to label clusters. CNKI: ① Timespan: 2017–2025 (Slice Length = 1); ② Selection Criteria: g-index (k = 25), LRF = 3.0, L/N = 10, LBY = 5, e = 1.0; ③ Network: N = 153, E = 297 (Density = 0.0255); ④ Largest 1 CCs: 123 (80%); ⑤ Nodes Labelled: 1.0%; ⑥ Pruning: None; ⑦ Modularity Q = 0.5502; ⑧ Weighted Mean Silhouette S = 0.8943; ⑨ Harmonic Mean (Q, S) = 0.6813. WOSCC: ① Timespan: 1999–2025 (Slice Length = 1); ② Selection Criteria: g-index (k = 25), LRF = 3.0, L/N = 10, LBY = 5, e = 1.0; ③ Network: N = 392, E = 1557 (Density = 0.0203); ④ Largest 1 CCs: 376 (95%); ⑤ Nodes Labeled: 1.0%; ⑥ Pruning: None; ⑦ Modularity Q = 0.4583; ⑧ Weighted Mean Silhouette S = 0.7222; ⑨ Harmonic Mean (Q, S) = 0.5607.
Analysis of keyword burstiness
Keyword burst detection identifies emerging research hotspots and reveals thematic evolution over time. The results show a dynamic, phase-based evolution of research focuses. With a burst threshold set at 0.21, 14 high-burst keywords were identified in CNKI. The evolution of its research themes can be divided into four periods: 1) Hot keywords included “medical devices”, “medical safety”, “ethical challenge”, and “doctor-patient relationship”, indicating that ethical challenges caused by medical devices, particularly those straining doctor-patient relationships, became a core research focus starting in 2019. 2) By 2020, “big data”, “ethical design”, and “ethics” gained prominence, reflecting how the rise of big data drew scholarly attention to ethical design. 3) Since 2021, with the emergence of intelligent medicine and smart medicine, research has focused primarily on technology ethics and ethical principles. 4) From 2022 to the present, ethical dilemmas and practical applications of AI in healthcare have continued to attract significant attention (Figure 4(a)).
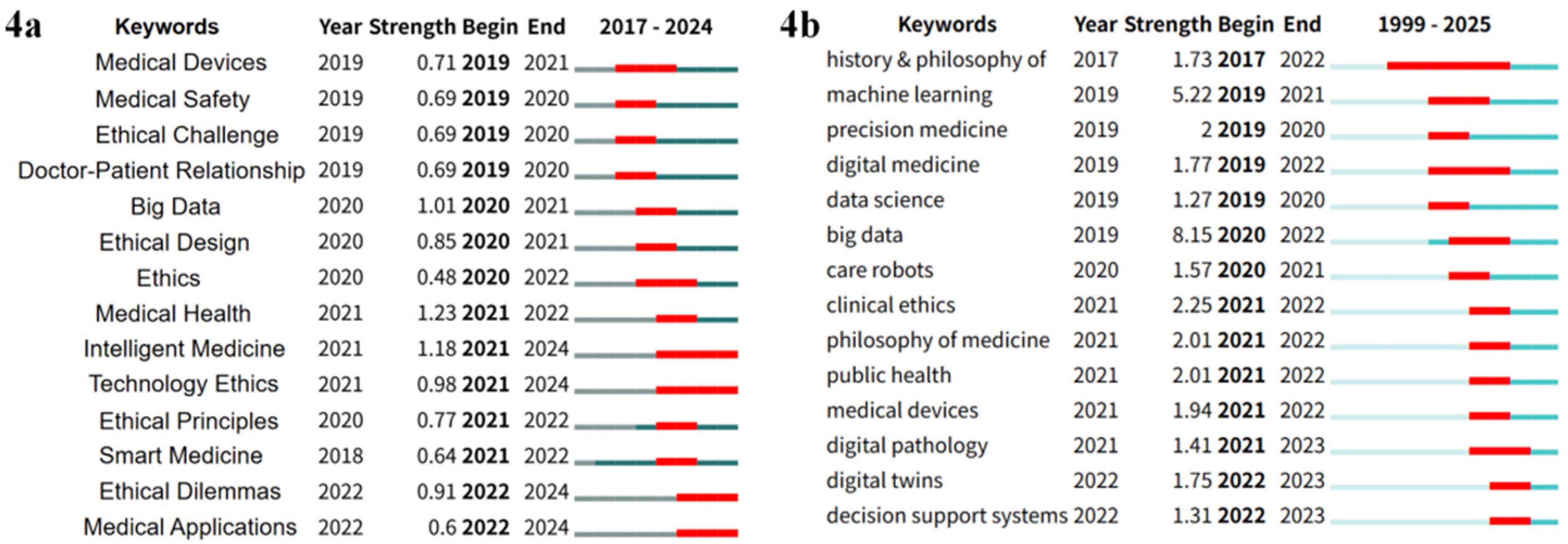
Keyword burst analysis (a) keyword burst analysis in CNKI, threshold at 0.21; (b) keyword burst analysis in WOSCC, threshold at 0.37.
For WOSCC studies, a burst threshold of 0.37 identified 14 high-burst keywords. The thematic evolution unfolded in three phases: 1) From 2017 to 2020, “history & philosophy of medicine”, “machine learning”, “precision medicine”, “digital medicine”, “data science”, “big data”, and “care robots” served as hot keywords. As the theoretical foundation of AI was deeply explored, scholars increasingly focused on data-driven medicine. The emergence of precision medicine, digital medicine, and care robots signalled trends toward personalisation, remote care, and automation in medicine. 2) From 2021 onward, attention shifted to the clinical application of AI-driven devices and the associated ethical issues. 3) By 2022, “digital twins” and “decision support systems” signalled a deepening of research into AI technologies within virtual and complex intelligent systems (Figure 4(b)).
Discussion
Ethical issues have emerged as global hotspots in the medical application of AI. This study found that research hotspots in this area encompass education, clinical practice, and academia. Research trends are shifting from identifying and governing ethical issues to designing and optimising complex AI tools embedded with ethical principles.
Descriptive analysis identifies commonalities and disparities among studies from different databases across temporal, journal, national/institutional, and authorial dimensions. Regarding publication time, 2017 marks a pivotal year in this research field. In 2016, the news that Google's deep learning-based AI AlphaGo's victory over South Korean 9th Dan Go champion Lee Sedol caused a sensation in both fields of AI and Go, which marked a significant milestone in the development of AI. 42 The following year, top international journals successively published articles related to medical AI.43,44 Since then, ethical issues pertaining to medical AI have received widespread and sustained scholarly attention. 45
Analysis of national and institutional contributions reveals distinct publication patterns. The USA and Canada are the most productive countries in terms of overall output in the WOSCC database. A significant volume of literature is also published in Chinese and indexed in the CNKI database. Additionally, the research landscape in this field is characterised by a wide distribution of contributing teams and institutions, which is common in rapidly evolving interdisciplinary areas. While this demonstrates broad interest, it also suggests that the field may still be in a phase of growing consolidation. Encouraging sustained collaboration both within and across national research communities could be instrumental in fostering deeper integration and advancing the field collectively.
To map the research landscape, we further reviewed and inductively categorised the highly cited papers and key articles associated with these keywords into four main perspectives: 1) ethical issues in different application scenarios of AI technique in clinical practice, 2) AI ethical concerns and considerations in medical academia, 3) ethical challenges of AI in medical education, 4) a macroscopic perspective discussing ethical governance, regulation and review. To further understand these research hotspots, an ethical framework could be helpful. 10
The technology is applied across clinical specialities, including ophthalmology, 46 imaging, 47 neurology, 48 gastroenterology, 49 paediatrics, 50 and mental health, 51 supporting tasks from image analysis to diagnostic consultation. When deploying the technology across these fields, we must carefully consider the associated ethical challenges, encompassing issues of algorithmic transparency, 52 justice and fairness, patient consent, 53 privacy, and responsibility. 54 These can be categorised into three ethical dimensions: epistemic, normative, and traceability ethics. 10 Epistemic concerns centre on the need for explainability and accuracy. Although explainability promotes trust and perceived fairness, 55 opaque decision-making remains commonplace in clinical practice, and diagnostic accuracy may take precedence over interpretability in certain contexts. 56 Normative ethics underscore the necessity of strengthened regulation, particularly regarding fairness, as biases can originate from data, algorithm design, and clinical interactions. 57 Beyond improvements in data management and clinician-patient education, addressing these requires algorithmic auditing and a redefinition of fairness in technology and clinical settings. 58 Simultaneously, privacy protection requires dynamic strategies, such as technologically enabled recurrent informed consent, clear data withdrawal rights, and evolving data protection, anonymisation, and regulation. 59 Within traceability ethics, a key challenge resides in determining ultimate accountability, 60 which in healthcare often remains permissible only when the technology serves a strictly auxiliary and supplementary role. 50 These ethical domains are deeply interrelated and cannot be resolved in isolation. Ultimately, navigating them may require a careful balance to achieve clinical and ethical acceptance.
The use of AI in medical academia has likewise raised significant ethical concerns and considerations.61,62 These relate largely to research misconduct, including issues within funded projects, 63 academic writing and publication practices. 64 Key problems involve information inaccuracy and fabrication, touching on epistemic and traceability ethics.10,65 Furthermore, while AI has the potential to bridge language barriers in global research, it also risks widening inequalities if primarily leveraged by high-income countries and privileged researchers (normative ethics). 66 In response, scholars have conducted extensive studies covering attitude surveys, strategic proposals, publishing guidelines, 61 critical discussions, 65 and ethical reflections. 67 Addressing these issues will require strengthening education and guidance for researchers, advancing detection technologies for AI-generated content, and coordinating international regulatory efforts. 68
Turning to medical education, ethical challenges posed by AI include privacy and data security, overreliance on technology, a tendency toward utilitarian teaching, and potential impacts on doctor–patient relationships.51,69 These issues largely fall within epistemic and normative ethical domains. 10 Current research exhibits notable regional divergence. Studies indexed in CNKI predominantly review the current state of AI adoption in medical schools, analysing associated ethical challenges and responses, with a focus on leveraging AI to foster professional competencies and ethical literacy. 69 In contrast, literature in WOSCC demonstrates broader thematic diversity, including the development of scales to assess readiness for medical AI, 70 debates on the necessity of AI ethics education, 71 the formulation of application guidelines, 72 and the exploration of innovative teaching methods. 73 This divergence highlights the need for developing countries to assess the global significance of AI ethics education, integrate it with the realities of their medical education landscape, and develop teaching approaches and systems tailored to national needs. Furthermore, greater attention should be directed toward understanding the needs and acceptance of AI ethics education among medical faculty and students, as such insights are essential for guiding curricular reform and implementing effective strategies.
From a macro governance perspective, the growing complexity of ethical challenges underscores the need for robust oversight frameworks to ensure the safe, effective, and equitable application of AI. Research indexed in CNKI primarily adopts a review-based approach, identifying core governance elements: privacy protection, algorithmic transparency and justice, clear accountability, and the enhancement of public trust. 74 Corresponding recommendations emphasise strengthening legal and regulatory systems, expanding educational initiatives, and cultivating professional expertise.74–77 Similar themes are also explored in WOSCC literature.78,79 Some studies further underscore persistent implementation gaps. Although practical guidelines exist for specialised fields,80,81 a significant chasm remains between ethical principles and their operationalisation, largely attributable to the lack of a clear, actionable definition of these principles. 82 Establishing clear operational definitions is crucial to mitigate the risks of unintentional misunderstandings of the term, as well as intentional misuse/ethics washing. However, we may caution that over-technicalising the definitions of ethical principles may conflict with the interpretive, relational, and normative dimensions of medicine, which cannot be codified. 83
Strengths and limitations
This study employs bibliometric analysis to identify research trends and emerging topics in AI ethics within the medical field. Given the broad coverage of research domains and wide adoption in previous bibliometric studies, we selected the WOSCC database. To mitigate language bias and capture research from China, we also included the CNKI database, a comprehensive and authoritative resource in the region. Analysing these databases separately allowed for comparative insights into content similarities and differences. Furthermore, visualisations of research trends were generated to facilitate a clear and efficient understanding of the landscape and to highlight potential future research directions.
However, notwithstanding its systematic approach, this study has several limitations that should be acknowledged. Primarily, our reliance on only two databases may give rise to selection bias, as this omits relevant studies indexed in other databases (e.g., PubMed). Secondly, this study adopts a macro perspective to map the research landscape, and a more granular analysis of research hotspots within specific subareas was precluded. Thirdly, we delimit publication types to research papers, excluding editorials, commentaries, viewpoints, etc., which may reduce the comprehensiveness of the results. Additionally, as a bibliometric study, this work does not assess the quality of the included literature. Consequently, our analysis depends on assessments of content relevance, a process inherently influenced by the researcher's expertise and judgement, which may limit the objectivity and replicability of the results. Future research could address these limitations by expanding database coverage, incorporating diverse publication types, and integrating more objective indicators or automated tools to enhance analytical rigour and reproducibility.
Conclusion
Academic attention to AI ethics in the medical field has risen markedly since 2017, encompassing diverse research perspectives and methodological approaches, gradually forming a systematic, multidimensional research system. Although stable journals and influential, productive countries have been established, team/country collaboration remains to be further strengthened. The shift in research trends reflects an evolution from fragmentation to integration of technology and ethics in medicine. Future research should further refine the operational definitions of ethical principles across diverse medical AI application scenarios, thereby guiding researchers to design medical AI systems with in-depth integration of technology and ethics, and also providing a clear foundation for educators to design and implement relevant courses and training, as well as for policymakers to formulate enforceable ethical norms and regulatory standards.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261431438 - Supplemental material for Research hotspots and trends of artificial intelligence ethics in medicine: A bibliometric analysis from 1999 to 2025
Supplemental material, sj-docx-1-dhj-10.1177_20552076261431438 for Research hotspots and trends of artificial intelligence ethics in medicine: A bibliometric analysis from 1999 to 2025 by Jialu Li, Jun Li, Yunjing Qiu, Shiquan He, Zhenxiang Zhang, Peng Wang, Hui Zhang and Beilei Lin in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261431438 - Supplemental material for Research hotspots and trends of artificial intelligence ethics in medicine: A bibliometric analysis from 1999 to 2025
Supplemental material, sj-docx-2-dhj-10.1177_20552076261431438 for Research hotspots and trends of artificial intelligence ethics in medicine: A bibliometric analysis from 1999 to 2025 by Jialu Li, Jun Li, Yunjing Qiu, Shiquan He, Zhenxiang Zhang, Peng Wang, Hui Zhang and Beilei Lin in DIGITAL HEALTH
Footnotes
List of abbreviations
Acknowledgements
We would like to thank all team members for their indispensable assistance in conducting this research.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Authors’ contributions
Jialu LI: Conceptualization, Methodology, Formal analysis, Writing - Original Draft, Visualization; Jun LI: Writing - Review & Editing; Yunjing Qiu: Writing - Review & Editing; Shiquan HE: Visualization; Zhenxiang Zhang: Supervision, Writing - Review & Editing; Peng Wang: Supervision, Funding acquisition; Hui Zhang: Writing - Review & Editing; Beilei LIN: Conceptualization, Writing - Review & Editing, Supervision, Funding acquisition. All authors have approved the submitted version and are accountable for the contributions and integrity of the paper.
Funding
This work was supported by the scholarships from the Postdoctoral Research Foundation of China [2023M743197], Foundation of Henan Educational Committee [25A320027], and National Natural Science Foundation of China [72104221, 72274180].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available on reasonable request from the corresponding author.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.