
Abstract
Background
Chronic cor pulmonale (CCP) represents a considerable health burden globally, especially in community settings where resources for management are frequently constrained.
Objective
This study aims to establish an internet-based integrated healthcare and prevention self-management intervention model for community-dwelling patients with CCP (pulmonary heart disease) and to evaluate its effectiveness in improving disease management and health outcomes.
Methods
Patients diagnosed with CCP within a community setting were enrolled. According to the management strategies they actually received, they were categorized into an intervention group and a control group. The intervention group received an internet-based integrated healthcare and prevention self-management intervention, while the control group received conventional management. The duration of the intervention was six months. Changes in the dyspnea index, oxygen saturation, quality of life scores, and readmission rates were measured before and after the intervention. Statistical analysis was conducted using SPSS version 21.0.
Results
Compared to the control group, the intervention group exhibited significant improvements in the dyspnea index, oxygen saturation, and quality of life scores (P < 0.05), as well as a significant reduction in readmission rates (P < 0.05).
Conclusion
The internet-based integrated healthcare and prevention self-management intervention model demonstrated significant effectiveness in enhancing self-management capacity and overall health status among community-dwelling patients with CCP.
Keywords
Introduction
Chronic cor pulmonale (CCP) is a widespread long-term condition that results from prolonged pulmonary disorders or complications with the pulmonary vasculature, which lead to pulmonary arterial hypertension and subsequently cause right ventricular dysfunction. 1 Key pathological mechanisms include chronic hypoxemia and pulmonary vasculature remodeling, both of which adversely impact cardiopulmonary function and can trigger extensive multi-organ damage. 2 Given the high levels of disability and mortality, CCP poses a significant public health issue, imposing considerable financial and caregiving burdens on patients’ families and healthcare systems. 3 The global occurrence of CCP is increasing, especially against the backdrop of an aging population and deteriorating air quality, leading to a persistent rise in its prevalence and associated health challenges. 4 Frequently reported symptoms in patients encompass dyspnea, chronic cough, and fatigue, which significantly diminish their quality of life. In the advanced stages of the disease, right heart failure and acute exacerbations become critical factors contributing to elevated rates of hospitalization and mortality. 5
In community settings, patients with CCP frequently face difficulties in self-management, primarily due to a limited understanding of their condition, ineffective symptom tracking, and poor adherence to healthy lifestyle choices. 6 Infrequent interactions between healthcare providers and patients further complicate the implementation of individualized treatment strategies, resulting in suboptimal disease management. 7 Additionally, limited community healthcare resources obstruct the delivery of effective ongoing management for CCP. 8 These interconnected challenges highlight the pressing need for the development of more efficient and accessible community-based management models.
The integrated framework for healthcare and prevention signifies a progressive method for managing health, intertwining clinical treatments with public health efforts to develop a unified service structure for prevention, treatment, and rehabilitation.9,10 Recently, the rise of Digital Health Interventions has significantly bolstered the application of this model through advanced technology.11–15 Prior research has produced compelling evidence advocating for their effectiveness in managing chronic respiratory and cardiac diseases, which possess similar pathophysiological features to CCP. For example, systematic reviews and meta-analyses pertaining to telehealth for individuals with chronic obstructive pulmonary disease (COPD) have repeatedly shown a decline in hospital readmissions along with enhancements in quality of life.16,17 In a similar vein, randomized controlled trials focused on heart failure management have indicated that remote monitoring and structured telephone support can improve self-care practices and reduce mortality rates. 18 These investigations affirm the overall efficacy of digital strategies in managing chronic diseases. Nonetheless, there remains a noticeable gap in existing literature. A majority of past studies have concentrated on interventions that utilize a single modality (such as only telemonitoring or solely education) or have been performed in stringently controlled hospital environments. Very few have thoroughly assessed a comprehensive, multi-faceted digital intervention that fully realizes the integrated healthcare and prevention model. Additionally, the particular requirements of the community-dwelling CCP population, who frequently contend with distinct accessibility and resource limitations, have not been adequately addressed. Our approach distinguishes itself from earlier research by integrating real-time monitoring, personalized rehabilitation, ongoing education, and proactive physician–patient engagement into a singular, cohesive digital platform designed for this at-risk demographic.
This research was conducted to assess the effectiveness of a novel integrated self-management intervention model targeted at community-dwelling patients suffering from CCP. The main goal was to evaluate how the intervention influenced patients’ functional status, which was determined by the variation in the Modified Medical Research Council (mMRC) dyspnea score from the initial assessment to the six-month mark. Additionally, the study aimed to investigate the intervention's effects on physiological measures (including changes in blood oxygen saturation, SpO₂), patient-reported quality of life (evaluated through changes in SF-36 scores), and healthcare use patterns (specifically, the hospital readmission rates over six months).
Materials and methods
Study design and participants
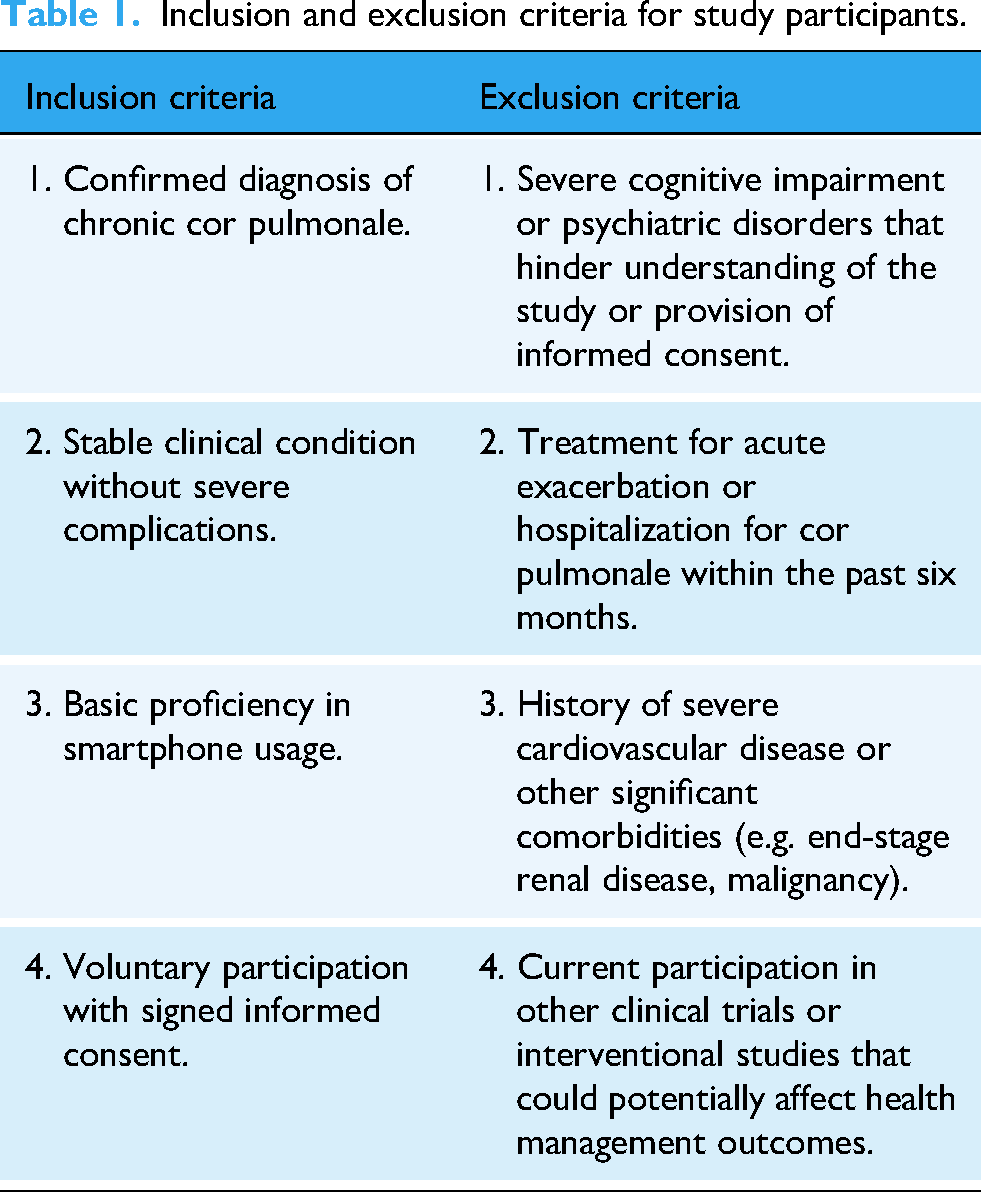
This study was conducted as a prospective observational study, enrolling patients diagnosed with CCP from three community health service centers: Panhuang, Yanlong, and Bufeng. The reporting was conducted in accordance with the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). The eligibility criteria for participant enrollment are detailed in Table 1. Ultimately, a total of 100 eligible patients were included in the study. This research received approval from the Medical Ethics Committee of Yancheng Third People's Hospital (Ethics Approval: LS-2024-031), and all participants provided signed informed consent.
Inclusion and exclusion criteria for study participants.
Participant grouping
A total of 100 patients who met the inclusion criteria were enrolled in this study. Based on the treatment they received, the patients were divided into an intervention group (n = 50) and a control group (n = 50). The grouping was not conducted through randomization; rather, it was an observational classification based on the interventions administered in clinical practice. To minimize selection bias, the baseline characteristics of both groups were compared to assess their comparability. Group allocation was recorded by the researchers at the time of patient enrollment. The personnel responsible for data collection and outcome assessment were blinded to the group allocation and clinical decision-making during the study, thereby reducing the potential for information bias and observer bias.
Interventions
The intervention period spanned six months.
Platform development and content validation
The intervention platform was developed by a multidisciplinary team consisting of clinical specialists in respiratory medicine, cardiovascular medicine, and general practice, as well as public health professionals, community nurses, and software engineers. Prior to the study, a rigorous content validation process was undertaken. A panel of seven experts, including specialists in respiratory medicine, cardiovascular medicine, general practice, nursing, and public health, reviewed the intervention modules. The panel assessed the rationale behind physiological data collection, the clinical acceptability of alert thresholds, and the accuracy and readability of health education materials. Based on the expert feedback, the alert rules, educational content, and follow-up forms were refined to ensure clinical safety and feasibility.
The platform was deployed as a WeChat Mini Program, featuring distinct interfaces for patients and healthcare providers. Its core functions included the following components: First, Data Collection, which involved SpO₂, heart rate, and respiratory rate collected via Bluetooth-enabled pulse oximeters or manual entry. Second, Risk Warning, where automated alerts were triggered based on pre-set thresholds, such as SpO₂ levels lower than 90% or consecutive abnormal readings, which were then communicated to the medical end. Third, Personalized Planning, which generated rehabilitation exercises, dietary recommendations, and medication reminders based on patient risk stratification. Fourth, Health Education, providing curated articles and videos accompanied by stage-based quizzes. Data security was ensured through encrypted transmission and strict access controls to comply with local data privacy regulations.
Control group
Individuals in the control cohort were provided with standard community-based care, which was uniformly structured to encompass the subsequent elements: Monthly Health Education Gatherings: These sessions, lasting around 30 min and led by community nurses, were conducted in groups. The topics included vital information pertaining to CCP, such as typical symptoms, medication usage principles, and identification of warning signs for exacerbations. Regular educational assistance during follow-up appointments: At the monthly in-person follow-ups with community physicians or nurses, patients were given consistent verbal reinforcement concerning their treatment strategies, daily care practices, and preventive actions.
Intervention group
Patients in the intervention group received a digitally enabled self-management intervention delivered via a dedicated mobile application, the “Community CCP Management Platform.” This proprietary application, developed in collaboration with the local community health information system, was installed on the patients’ personal smartphones. The intervention was supervised by a dedicated team of community physicians and nurses from the participating health centers. The model comprised the following components:
The digital health platform and connected devices: The core of the intervention was the mobile app, which served as the central hub for all data and communication. Each patient was provided with a Bluetooth-enabled fingertip pulse oximeter (Model: YX301, Yuwell Medical Equipment, Jiangsu, China) to self-monitor their blood oxygen saturation (SpO₂) and heart rate. Patients were instructed to take measurements twice daily (morning and evening). The data were automatically transmitted via Bluetooth from the oximeter to the mobile app and subsequently uploaded to a secure, cloud-based server integrated with the community health information system.
Supervision and real-time monitoring: The community healthcare team, which included physicians and nurses, had access to a web-based dashboard to monitor all patient data in real time. The system was programmed to generate automated alerts to the team if a patient's SpO₂ dropped below 90% or their heart rate exceeded 120 b/min on two consecutive readings. Upon receiving an alert, a designated nurse would contact the patient by phone within 24 h to assess their condition and, if necessary, arrange a consultation with a physician.
Personalized rehabilitation and education: Based on baseline assessments and ongoing data, the healthcare team developed personalized rehabilitation plans tailored for each patient, which were delivered through the application. These plans incorporated instructional videos for respiratory exercises, such as pursed-lip breathing, customized dietary recommendations, and specific daily activity goals. Furthermore, the application contained a comprehensive library of educational resources, including articles and short videos, focusing on COPD management, medication adherence, and lifestyle modifications.
Proactive physician–patient interaction: The platform featured a secure messaging function that enabled patients to send non-urgent inquiries to the healthcare team and receive responses within 48 h. Additionally, physicians performed a monthly review of each patient's health data trends, providing personalized feedback and adjustments to their treatment or rehabilitation plans through the application or scheduled phone calls.
Measurements
All outcome data were collected at baseline (pre-intervention) and during the 6-month follow-up visit. Data for the mMRC (Table 2) dyspnea scale and the SF-36 were gathered by trained research nurses, who were not involved in the delivery of the intervention, through face-to-face interviews to ensure data quality and consistency. In the intervention group, SpO₂ data were collected via a digital platform, whereas in the control group, measurements were taken by the nurse during the visits. Readmission data were obtained from hospital records. The primary outcome measure was the functional status assessed using the mMRC dyspnea scale. Secondary outcomes included SpO₂, quality of life as measured by the SF-36, and rates of hospital readmission. The specific domains, measurements, collection methods, and expected impacts are detailed in Table 3. The complete versions of the mMRC and SF-36 questionnaires utilized in this study are available in the Supplemental Materials.
Modified Medical Research Council (mMRC) dyspnea scale.
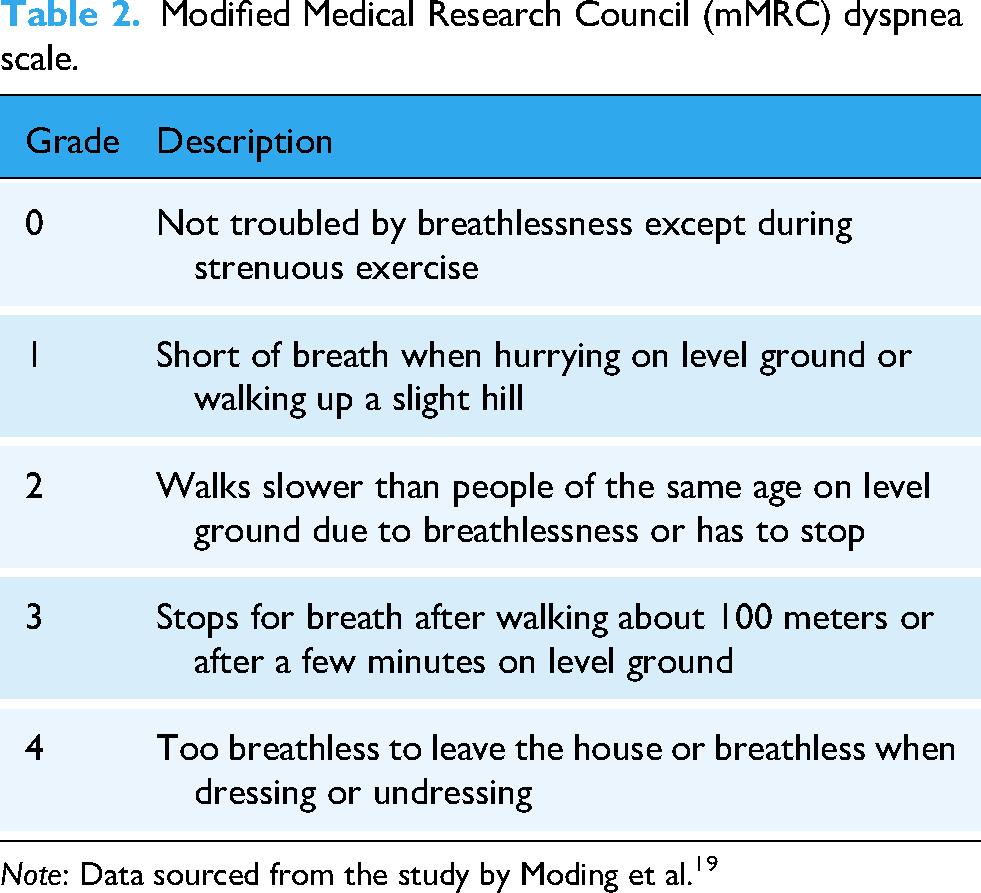
Note: Data sourced from the study by Moding et al. 19
Summary of outcome measurements.

Statistical analysis
All data were analyzed using SPSS version 21.0 statistical software. Data normality was assessed using the Shapiro–Wilk test. Quantitative data are presented as mean ± standard deviation (Mean ± SD). Differences between the intervention and control groups were analyzed using independent samples t-tests, while changes from baseline to post-intervention within each group were evaluated using paired samples t-tests. Categorical data were evaluated using chi-square tests. The significance level was established at α = 0.05, with a P-value of less than 0.05 indicating statistical significance. P-values that are below 0.05 were deemed to be statistically significant. Values are reported as highly significant when P < 0.001.
Results
Comparison of baseline data between two groups of patients
There were no statistically significant differences (P > 0.05) in baseline characteristics such as age, gender, disease duration, and baseline mMRC scores between the intervention group and the control group, indicating comparability (Table 4).
Comparison of baseline characteristics between the two groups (n = 50).

Comparison of changes in indicators before and after intervention
Regarding the Dyspnea Index, the post-intervention mMRC score in the intervention group decreased significantly from 2.8 ± 0.4 to 1.5 ± 0.3 (P < 0.001), indicating a greater improvement compared to the control group, which decreased from 2.7 ± 0.5 to 2.4 ± 0.4. In terms of Blood Oxygen Saturation, the intervention group exhibited a significant increase from 89.5 ± 2.1% to 93.2 ± 1.8% (P < 0.001), whereas the control group showed no significant change. With respect to Quality of Life, the SF-36 score in the intervention group improved from 55 ± 8 to 70 ± 7 (P < 0.001), which was significantly higher than the control group's post-intervention score of 58 ± 6. Lastly, the Readmission Rate in the intervention group was 12% (6/50), significantly lower than the 30% (15/50) observed in the control group (P = 0.0495) (Table 5, Figure 1).

Comparison of outcome indicators before and after intervention. (A) mMRC dyspnea score; (B) blood oxygen saturation (SpO2) level; (C) SF-36 quality of life score; (D) 6-month readmission rate. Data are presented as mean ± SD. Error bars represent standard deviations.
Comparison of outcome indicators before and after intervention in the two groups.

Discussion
The findings of this prospective observational study indicate that the implementation of our digitally enabled integrated self-management intervention model is associated with significant improvements in key health outcomes for community-dwelling patients with CCP. The following discussion explores the potential mechanisms through which the intervention achieved these effects for each specific outcome.
The significant reduction in dyspnea symptoms, as measured by the mMRC scale, and the concurrent improvement in SpO₂ are likely attributable to the personalized rehabilitation and real-time monitoring components of our intervention. The digital platform delivered tailored respiratory exercises, such as pursed-lip breathing, which are known to enhance breathing efficiency and reduce the work of breathing. 22 Continuous SpO₂ monitoring provided patients with immediate biofeedback, potentially reinforcing their adherence to these exercises and other lifestyle modifications, such as home oxygen therapy. This aligns with studies on COPD patients, where tele-rehabilitation has been shown to improve functional exercise capacity and respiratory symptoms. 23
The substantial improvement in quality of life, as reflected by the SF-36 scores, is likely a multifactorial outcome. Firstly, the alleviation of physical symptoms like dyspnea directly contributes to improved physical functioning and vitality scores. Secondly, the educational and interactive features of the intervention likely enhanced patients’ self-efficacy. By gaining a better understanding of their condition and maintaining direct communication with their healthcare team, patients may have felt more confident and less anxious in managing their disease, which positively impacted the mental health domains of the SF-36 scale.24,25
Most notably, the significant reduction in the six-month hospital readmission rate underscores the critical role of the platform's early warning function and enhanced physician–patient interaction. The automated alert system, triggered by drops in SpO₂, enabled the healthcare team to proactively intervene before a patient's condition severely deteriorated. This proactive approach facilitated timely adjustments in medication or treatment strategies within the community setting, thereby preventing exacerbations that would otherwise necessitate hospitalization. This finding aligns with robust evidence from systematic reviews in both COPD and heart failure, which have concluded that telemonitoring interventions can effectively reduce hospital readmissions.
Despite the positive effects of this intervention, certain limitations persist that warrant further research and refinement. The intervention period in this study was relatively brief; although improvements were observed, the long-term effects remain unclear. Future research should extend the intervention duration and conduct long-term follow-ups. Additionally, the sample size of this study was relatively small, which may introduce bias in the statistical results. Therefore, future studies should aim to increase the sample size to enhance the reliability and generalizability of the findings. Finally, although this study demonstrated the effectiveness of the intervention, its cost-effectiveness has not been thoroughly evaluated. Future research should focus on the cost-effectiveness ratio of the intervention model to provide a theoretical basis for its widespread implementation.
Study limitations
This study has several limitations that warrant acknowledgment. The sample size was determined based on the number of eligible patients available in the participating community health centers during the study period, rather than through an a priori power analysis. This approach may limit the statistical power of the study to detect smaller differences between groups. First, the 6-month duration of the intervention, although adequate for observing short-term effects, may prove insufficient for assessing the long-term sustainability of the observed improvements. Given the observational nature of the study design, the grouping was determined based on clinical practice rather than randomization. While baseline characteristics were compared, unmeasured confounding factors may still influence the observed associations, thereby preventing definitive causal conclusions. Second, the study was conducted at a single center with a relatively small sample size, potentially limiting the generalizability of our findings to other populations and healthcare settings. Third, while key patient-reported outcomes were collected by trained nurses, the physiological data (SpO₂) in the intervention group relied on patient self-measurement. Although automated data transmission minimized reporting errors, the potential for inconsistent or incorrect device usage introduces a risk of measurement bias. Fourth, the inclusion criterion mandating basic smartphone proficiency may have introduced a selection bias, potentially excluding older or less technologically literate patients, who are often the most vulnerable. This limitation restricts the generalizability of our findings to the broader population of CCP. Finally, this study did not include a formal cost-effectiveness analysis. The development and maintenance of the digital platform, along with the provision of connected medical devices and the time commitment from healthcare personnel, require significant resources. While our intervention demonstrated a significant reduction in hospital readmissions, suggesting potential cost savings, a comprehensive economic evaluation is necessary to formally assess whether these savings offset the costs of the intervention. Future research should prioritize conducting a thorough cost-effectiveness analysis to determine the economic viability of this model and provide a stronger basis for its widespread implementation.
Conclusion
The digitally enabled integrated self-management intervention model demonstrated significant therapeutic effects for community-dwelling patients with CCP. These improvements are likely attributable to the model's key multi-component features, which synergistically enhanced patient engagement and clinical oversight. Specifically, real-time physiological monitoring, combined with an early warning system, facilitated proactive interventions that prevented acute exacerbations and reduced readmissions. Furthermore, personalized education and rehabilitation guidance empowered patients, thereby improving their self-efficacy, which likely contributed to the observed enhancements in functional status and quality of life. The proactive communication between physicians and patients fostered a continuous care relationship, ensuring that management plans remained aligned with patients’ evolving needs. While acknowledging the study's limitations, this model represents a promising, effective, and accessible strategy for improving health outcomes in this vulnerable population. Future research should focus on long-term effects and cost-effectiveness to support its widespread implementation.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261428191 - Supplemental material for Establishment and effectiveness of a community self-management intervention model for patients with chronic pulmonary heart disease: A prospective observational study
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261428191 for Establishment and effectiveness of a community self-management intervention model for patients with chronic pulmonary heart disease: A prospective observational study by Sheng Cheng, Jianxin Zhou, Weisong Zhang, Xia Li, Li Qin, Jiuyan Ding, Shanshan Pang, Jing Zhou and Wenchun Song in DIGITAL HEALTH
Footnotes
Ethical statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author contributions
S.C., J.Z., and W.Z. contributed to the conception and design of the study. X.L., L.Q., and J.D. were responsible for data collection and the supervision of interventions. S.P. and J.Z. conducted the statistical analysis and interpreted the results. S.C. and W.S. drafted the manuscript. All authors critically reviewed the manuscript and approved the final version for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: 2024 Provincial Traditional Chinese Medicine Science and Technology Development Program—General Project (MS2024104); 2023 Yancheng Science and Technology Bureau Key R&D Program—Social Development Guidance Project (YCBE202346); Special Scientific Research Fund for Clinical Medicine of Nantong University (2024JZ001).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.