
Abstract
Introduction
Diabetic foot self-management intervention programs have been proven to positively influence individuals’ behaviors in preventing diabetic foot ulcers. Using digital technologies to deliver programs can facilitate compliance with diabetes self-management programs. However, few studies have focused on the effects of such digital programs on improving the self-efficacy and behaviors of older adults with type 2 diabetes in the community.
Aim
To evaluate the effects of a digital foot self-management program on self-efficacy, self-care behavior, and Hemoglobin A1c levels.
Design
A single-blinded, randomized controlled trial was conducted.
Methods
The intervention program comprised a 4-week digital foot care program with one face-to-face education session, phone calls once weekly, and LINE messages (social media) three times per research nurse and a follow-up of three months. Patients in the control group received routine care.
Results
A total of 100 participants (n = 50 in the control and n = 50 in the intervention groups) completed the study with a mean age of 67.55 (SD = 11.17). The results showed significant improvements in self-efficacy (F = 2187.24, p < 0.01) and self-care behavior (F = 614.71, p < 0.01) in foot care between the groups. The Hemoglobin A1c levels showed a 0.41% reduction over time in the experimental group (t = −3.759; p < 0.01), whereas the control group showed a 0.06% reduction (t = −0.797, p > 0.05).
Conclusion
The newly developed digital foot self-management program was effective in community-dwelling older adult patients with type 2 diabetes.
Introduction
The number of individuals with type 2 diabetes continues to grow and is estimated to reach 700 million by 2045 globally. 1 The National Health Administration statistics in Taiwan report that 1.76 million people with type 2 diabetes account for 12.3% of the total population in Taiwan. Annually, over 90% of patients with diabetic foot had an infection. 2 The patients often require recurrining hospital visits, or some patients need to be hospitalized for serious infection over 40 days (Interquartile range: 15–99). 3 Diabetic foot is the most common, expensive, serious, and preventable complication.4,5 The risk of a person with diabetes having foot ulcers over the years is 19%–34%, which can be responsible for 85% of causes of lower limb amputations. 6
Evidence shows diabetic foot ulcers significantly increase medical costs, reduce quality of life, and increase the risk of premature death. 6 A higher proportion of patients with diabetic foot ulcers were men, older adults with a low education level, and low income. The prevalence of diabetic foot ulcers was 0.5%–0.8% and showed stable growth year on year in Taiwan. 7 Approximately 40% of older people with diabetic foot ulcers experience a recurrence within 1 year of ulcer healing, 60% within 3 years of ulcer healing, and 65% within 5 years linked to the complex wound problem of diabetic foot ulcers. 8 However, at least 70% of amputations caused by diabetic foot ulcers are reported to be preventable by enhancing patient's confidentice in their own self-care behaviors. 9 Foot care behavior involves feet inspection (such as assessing skin color, temperature, presence of calls), washing and drying, care of toenails, appropriate footwear, and basic wound management.7,10
Self-efficacy is a critical construct in Bandura's Social Cognitive Theory. 11 Self-management programs guided by the self-efficacy model have shown positive improvements in better managing the health outcomes of patients with chronic diseases, such as cardiac and diabetes. 12 Studies have also shown that providing foot care education based on self-efficacy design to people with diabetes improves foot care behavior.13,14 Moreover, diabetes self-management via emerging innovative applications motivates individuals to engage in healthy lifestyle activities to reduce complications. Mobile devices and applications have provided benefits to health professionals by supporting clinicians’ clinical decision-making and improving the health outcomes of people with diabetes. 15
Multiple digital applications are available for older people with diabetes to more sufficiently self-manage their condition.16,17 Digital defines in this study including using mobile devices for accessing calls, videos via application, e-books, which have shown the effect of increasing patients’ willingness to improve their behaviors in managing their everyday conditions. 18 Patients felt more comfortable and motivated to engage in foot care activities as well as interacting with the research nurse through the application. Despite the many applications available to healthcare providers and patients, evidence evaluating digital foot care interventions specifically designed for older people with diabetic feet is limited. 19 In addition, lack of theory-based teaching materials targeting in-home patient self-care, we addressed the gap by assisting patients to improve their knowledge and skills. Digital self-care videos and games highlighting the different levels of prevention care were designed so that in-home patients can experience and understand while living with diabetes.
Aim
This study aimed to develop and evaluate the effectiveness of a digital foot self-management educational program for older adults with type 2 diabetes on self-efficacy, behavior, and hemoglobin A1c (HbA1C) outcomes.
Methods
Study design
A two-armed, single-anonymized, randomized controlled trial was conducted to evaluate the effect of a digital foot self-management program. A total of 100 participants were randomly allocated to either the experimental group (n = 50) or the control group (n = 50). A computerized random number generated by an independent statistician was used to allocate each potential participant to the control or experimental group in a one-to-one ratio. Participants in the experimental group received a digital foot self-management program and routine care. The control group participants received routine care in the diabetes clinic, including routine checkups every three months, and foot care education. Technical support was provided by a research nurse, who liaised with the application developer if necessary. The outcomes were self-efficacy, self-care behaviors during foot care, and HbA1C levels.
Participants and recruitment
After obtaining ethical approval and agreement from the community authorities to participate in the study, eligible participants were recruited from five communities in southern Taiwan, and were intermediated by community coordinator. Participants were approached if they met the following inclusion criteria: Diagnosis of type 2 diabetes, age over 65 years, ability to use a mobile device (e.g., smartphone, tablets), and ability to read and comprehend Chinese. Participants were excluded if they could not perform the recommended physical activities, had cognitive impairment, or could not read Chinese (Figure 1).

CONSORT flow diagram of the trial.
Sample size calculation
The sample size calculation was based on the primary outcome of self-efficacy for over 80% of power using G-power 3.1.9.2 to set F verification by repeated measured analysis of variance, α=0.05, and the moderate effect size was 0.25, power was 0.80, and 20% attrition rate. Data were collected by a research assistant, and an intervention program was delivered by a research nurse.
Intervention
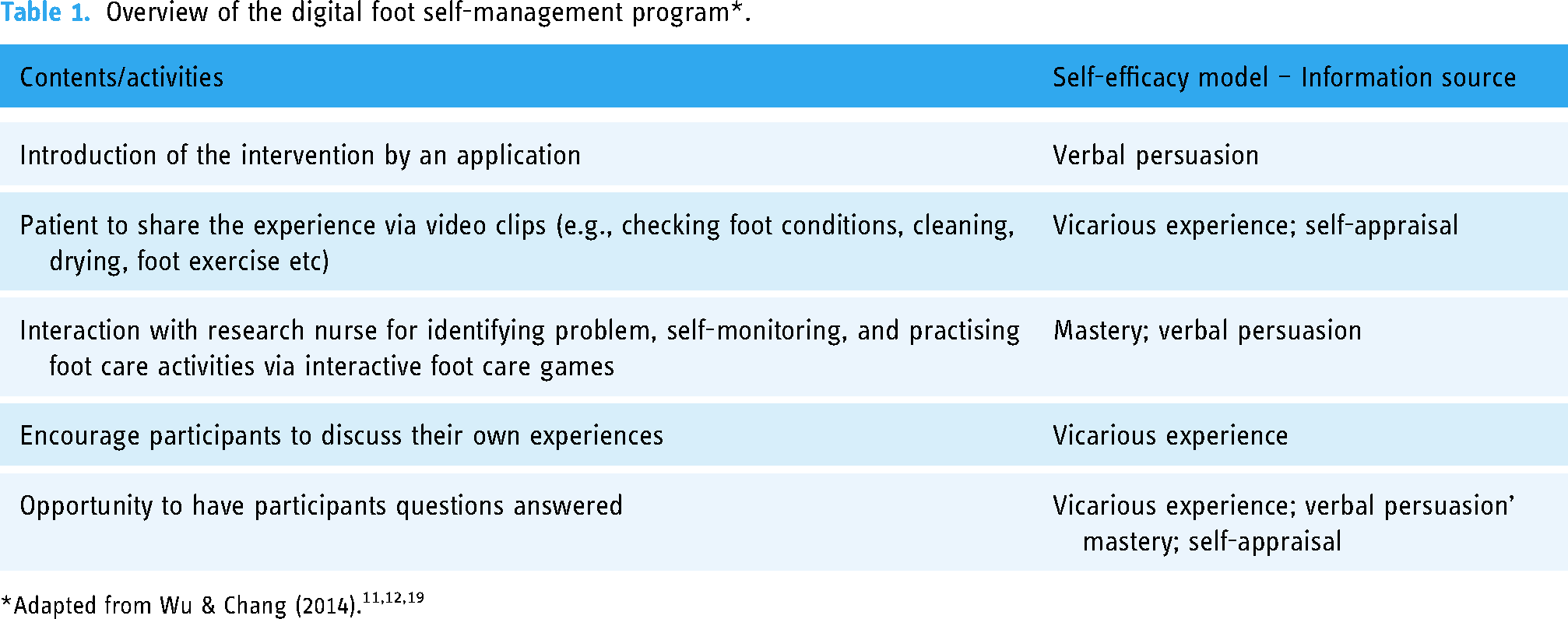
A digital foot self-management program guided by Bandura's self-efficacy model 20 for older people with type diabetes was developed, comprising 4-week sessions and a follow-up of 3 months. The self-efficacy information sources of mastery, vicarious experience, verbal persuasion, and physiological feedback were applied to the program.11,12 See Table 1. For example, a peer-supporting video, a quiz game, and a feedback system were used to encourage participants to resolve self-identified programs. The contents were adapted from the diabetes foot care guidelines of The Diabetes Association of Taiwan, 21 including checking foot conditions and cleaning, assessing for corns and calluses, foot exercise, diet-related foot care, foot care logs, and culture-involved foot care at home. If corns and calluses are identified, patients are asked to see their own doctor for appropriate management. Week 1 of the intervention consisted of a one-hour face-to-face session, introducing key topics and navigating the application functionalities, including an opportunity to discuss and practice activities with the research nurse. During weeks 2–4, participants received weekly follow-up phone calls and three messages through the application feedback system. A research nurse provided an application feedback system for up to 3 months. For the second and third months, participants were encouraged to use the digital platform to monitor their compliance with the program from home. Participants were informed that technical phone support was available during the trial. Benchmarks from digital information literacy on “knowing, accessing, managing information, sharing information” 22 (p,7) were used to assess the participant's digital literacy levels via feedback from engaging in the learning activities.
Overview of the digital foot self-management program*.
Outcome measures
Self-efficacy was assessed using the Chinese version of the Foot Care Self-Efficacy Scale. 23 This scale contains 16 items measuring an individual's foot care management efficacy, and was scored using a five-point Likert scale: “completely disagree,” “slightly disagree,” “no opinion,” “slightly agree,” and “completely agree,” with a minimum of 16 and a maximum score of 80. The Cronbach's alpha was 0.82 in this study. The scale was used at baseline (T1) and at four weeks (T2) for the control and experimental groups.
Self-care behaviors were assessed using the Diabetic Foot Self-Care Behavior Scale. 20 The scale consists of seven questions divided into two parts consisting of the number of days, and the frequency of foot care activities. On a 5-point Likert scale (never, days a week = 1 point; rarely, 1–2 days a week = 2 points; sometimes, 3–4 days a week = 3 points; often, 5–6 days a week = 4 points; 7 days a week = 5 points). A scale of 7–35 indicates good foot self-care behavior. The Cronbach's alpha was 0.92 in this study. The scale was used at T1 and T2 for the control and experimental groups.
Glycemic control was determined based on HbA1C at baseline and 3 months. Data were obtained from the participants’ medical records.
Data collection
Data collection commenced after informed consent in paper format, was obtained. Data were collected online through web-connected portals so that trained community nurses could provide individualized foot care and consultation after receiving ethics approval. Demographic data were collected at baseline. Other outcome measures were collected at baseline and 3 months, such as questionnaires and HbA1C in both groups.
Data analysis
This study was analyzed and calculated using SPSS Windows software version 22.0. Baseline demographic profiles were examined for similarities between the experimental and control groups. Between- and within-group comparisons were performed to examine self-efficacy and self-care behaviors. The Johnson–Neyman technique was conducted to the HbA1C if time and group interaction effects were identified. A statistical of .05 was regarded as a statistical significance.
Ethical considerations
Ethical approval was obtained from the university hospital. The study was approved by the Ethics Committee (Anonymized for review). Personal information and questionnaire content were anonymous, confidentiality and privacy were maintained for online data collection, and only members of the research team had access to the participants’ app feedback information and physical online data through the principal investigator of this study. These are presented as numbers where necessary. The participants had the right to decide whether to participate or withdraw from the study.
Results
Sample characteristics
A total of 100 patients participated in this study. The mean age was 67.55 years (SD = 11.18). The majority were female participants (51%), married (67%), and had completed junior high school (39%). Over 80% were unemployed and had no active foot ulcers (93%). The mean HbA1c was 7.53 (SD = .71). There were no significant differences in the demographics and outcomes at baseline between the experimental and control groups, indicating similarities between the participants in both groups (Table 2).
Demographic profile in baseline (n = 100).

CG, control group; EG, experimental group; HbA1C: hemoglobin A1c.
Self-efficacy in diabetic foot care
One-way analysis of variance (ANOVA) showed significant improvements in self -efficacy between intervention and control groups (F = 2187.247, p < 0.00) indicating that participants who have received digital foot self-management program, have a substantial difference in self-efficacy compared to the control group. Within groups, there was a significant difference between baseline and 4-week intervention in the experimental group (24.96 ± 2.276 vs. 76.56 ± 1.656; t = 137.706, p < 0.001), but it was significant in the control group (25.02 ± 2.910 vs. 56.0 ± 2.597; t = 65.352, p < .001). See Table 3.
Effects of foot care self-efficacy and behavior from baseline to 4 weeks in the two groups (n = 100).

Diabetic foot care behavior
ANOVA showed significant improvements in diabetes foot care behavior between intervention and control groups (F = 2.99, p = 0.087) indicating that participants who have received digital foot self-management program, have a substantial difference in self-efficacy compared to the control group. Within groups, there were significant differences between baseline and 4-week intervention in the experimental group (8.08 ± 1.140 vs. 32.36 ± 1.453; t = 100.122, p < .001) and also significant in the control group (7.80 ± 1.088 vs. 22.00 ± 2.548; t = 33.895, p < .001). See Table 3.
Glycemic control
Glycated hemoglobin (HbA1C) levels were measured at baseline and 3 months. The mean HbA1C levels in the experimental group reported a 0.41% reduction (7.49 ± 0.80 to 7.08 ± 0.41) (t = −3.759; p < 0.001) over time. The control group showed no significant HbA1C level increase of 0.06% from baseline to 3 months, respectively (7.56 ± 0.68 to 7.50 ± 0.54) (t = −0.797, p = 0.429). In comparison, the independent t-test for the experimental and control groups at 3 months showed a significant difference (t = −4.35, p < 0.001). However, because the interaction between the group and baseline HbA1c was significant (F = 11.575; p < 0.05), the Johnson–Neyman technique, rather than independent samples one-way ANCOVA was used to explore the intervention effect on HbA1C. The results showed digital foot self-management program significantly improved HbA1C among participants, with baseline values greater than 6.99%. The improvements were more significant in the experimental group than in the control group (Figure 2).

The Johnson–Neyman statistical analysis of HbA1cC, baseline data in each group and the cut points of significant differences between the two groups.
Discussion
Our newly developed digital foot self-management program positively affected the outcomes of self-efficacy, self-care behavior, and HbA1C levels. There are few digital foot care programs in the studies developed for community-based diabetic foot care in older adults, one of which is Dincer and Bahçecik. 24 Dincer and Bahçecik developed a mobile application on foot care for patients and a population management system for a hardware device that synchronizes patients’ footcare animation-supported health literacy from their mobile devices. Their mobile device incorporated aspects of care and was used for educational purposes. Our findings support using digital platforms as an intervention delivery model to reduce health professionals’ direct contact time and allow them more time to attend to others’ needs. The findings comprise literature that used the digital platform to promote patients’ awareness, and increase their self-efficacy and behavior to care for their own feet, reducing nursing manpower and medical costs. 18 We acknowledge there are other applications for the self-management of the diabetic foot in terms of exercises and pressure sensing. 24 Our theory-based intervention via a digital platform was specifically designed for older people with diabetic foot ulcers in the 40% community.
Patient health literacy and age remained crucial components of optimizing the effect of digital foot care.22,25 Motivating engagement and changing foot care behavior in older people with lower health literacy can present challenges for health professionals. Previous studies have shown that patients with improved self-efficacy would feel more confident about managing their diabetic foot care. 26 Our study used a digital foot self-management program with self-help games designed for a detailed analysis with a Chinese cultural design platform to help participants understand their own situation and care. One of the critical contributions to our intervention program was evidence-based self-care activities, such as checking feet daily, walking barefoot, checking the water temperature before bathing, and self-rubbing for foot woods. 10 Our results highlight the importance of considering the environment in which people live. With the high humidity weather in the summer in Taiwan, some individuals often walk barefoot at home, which puts them at risk of foot ulcers.
Barriers and facilitators in using digital applications in healthcare have been investigated. Facilitators include the use of digital health programs by health professionals, specific group, or geographic locations could potentially enable the utilizations. However, infrastructure, training, time, environment factors could influence the uptake of digital interventions. 27 Environmental factors highlight the challenges of managing foot ulcers, which can be affected by wound healing and patient foot care behaviors.27,28 Anecdotally, our participants were initially less or not interested in foot care. Nonetheless, after receiving the intervention program, they said, “It is not as difficult as I thought it would be.” “I can do it again.”
Strengths and limitations
This study's major strength was the program's context, which used the self-efficacy model to guide the digital design of older people with diabetes in the community. However, this study had some limitations. This study was focused on the Taiwanese population's specific environment and culture for diabetic foot care, it may be appropriate to generalize to other population. Furthermore, although significant improvements in glycemic controls have been found in our study, it is unknown as whether how long these older people with diabetic foot care would continue to be embedding in their everyday activities. We also acknowledge that the limitation of not being able to record individual's interaction time with the application and its association with the outcome.
Future research
The implications for community diabetic foot care include incorporating a digital foot self-management program into existing diabetes education. A longitudinal study is recommended to address these limitations. Future research on a holistic approach that seeks and incorporating feedback from all stakeholders (patients, health professionals, community members, administrators) is also recommended. Future study on the dose-effect of the digital intervention program is suggested.
Conclusion
Our study was the first randomized controlled trial of a digital foot self-management program for older people with type 2 diabetes living in a community in Taiwan. The results highlighted the benefits of a theoretical model for facilitating people's self-management of their conditions at home.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial registry number
NCT05272670
Contributorship
Study design was done by S-MC and C-JW. Data analysis was done by S-MC and C-JW. Manuscript drafts were done by S-MC and C-JW. Appraisal and editing of all revisions equally were done by S-MC and C-JW. Final approval was done by S-MC and C-JW.
Ethical approvals
The study was approved by the Antai Medical care Corporation Antai Tian-Sheng Memorial Hospital Ethics Committee (No.20-084-B).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Fooyin University in Taiwan (grant no. FYU1300-109-02). The funder did not play any role in the conduction or publication of the study. The authors would like to thank Shu-Hsien Lee for her assistance on data collection.