
Abstract
Objective
Self-management support services can improve patients’ self-management ability. This study summarized the best evidence on a self-management support scheme for patients with inflammatory bowel disease based on a mobile health system to accurately describe the current status of the field and provide recommendations for healthcare workers.
Methods
Two researchers retrieved studies from computer decision support systems, guideline websites, official association websites, and databases from the establishment of the database until October 2023. The quality of the included studies was independently evaluated by two authors using the Appraisal of Guidelines for Research and Evaluation Instrument II and the 2016 version of the corresponding evaluation standards of the Australian Joanna Briggs Institute Evidence-based Health Care Center. The classification of evidence and recommendation level adopted the 2014 version of the Australian Joanna Briggs Institute evidence pregrading and recommending level system.
Results
Fifteen studies were included, comprising one guideline, two expert consensuses, four systematic reviews, four quasi-experimental studies, and four qualitative studies. The overall quality of the included studies was moderate to high. Thirty-six pieces of best evidence were compiled for seven elements, namely, mobile health system type and functional support; mobile health system application preparation; health information recording, uploading, and presentation; zoning management of diseases and early warning of the active period; support related to health education; healthcare support team formation and services; and virtual communities.
Conclusions
Our study evaluated the quality of the included studies and summarized a self-management support scheme for patients with inflammatory bowel disease based on a mobile health system. The main scheme was divided into 7 parts and 36 items, which can be used as a reference for healthcare workers so that they can provide more comprehensive and scientific self-management support services for patients with inflammatory bowel disease through mobile health systems.
Keywords
Introduction
Inflammatory bowel disease (IBD) refers to a group of chronic, nonspecific intestinal inflammatory diseases of unknown cause, including ulcerative colitis (UC) and Crohn's disease (CD). Abdominal pain, diarrhoea, mucus, mucopurulent bloody stool, etc., are the primary symptoms. 1
Recently, the prevalence of IBD has increased worldwide. The prevalence of IBD is more than 0.3% in many nations, including those in North America, Oceania, and Europe. The highest incidence is found in Europe, where 322 persons out of every 100,000 are affected annually. 2 China has the greatest incidence rate in Asia, with 35 cases per 100,000 people annually. 3 It is predicted that 1.5 million people in China will have IBD by 2025. 4 IBD is a chronic disease characterized by repeated attacks. There is still a lack of effective diagnostic and treatment methods for this disease, which seriously affects patients’ physical and mental health and quality of life. 5
Self–management refers to an individual's ability to manage the symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with a chronic condition. 6 Effective self-management involves monitoring one's condition and enacting the cognitive, behavioral, and emotional responses necessary to maintain a satisfactory quality of life. 6 In recent years, experts have recommended improving the self-management capacity of patients with IBD as a means of preventing disease recurrence. This approach can effectively reduce disease activity and improve patients’ quality of life. 7 Unfortunately, the current self-management status of IBD patients is not promising and is mainly plagued by problems such as lack of disease knowledge, poor medication compliance, insufficient disease monitoring, and obstructed doctor‒patient communication.8,9 There is an urgent need to obtain self-management support from professionals. 10 Self-management support, defined as the systematic provision of education and supportive interventions by healthcare professionals, aims to enhance patients’ skills and confidence in managing their health conditions. This encompasses regular assessment of progress and challenges, collaborative goal setting, and problem-solving support. 11 Despite healthcare workers’ efforts to provide self-management support within their clinical practice, the current model often lacks continuity and systematic implementation due to factors such as demanding clinic schedules and the rising prevalence of IBD. 12 In recent years, with the emergence of information technology and 5G networks, mobile health systems have been developed, creating a new method for healthcare workers to provide self-management support and demonstrating better availability and acceptability among patients and healthcare workers. 13 Self-management support based on mobile health systems facilitates the health management of IBD patients while reducing medical utilization and outpatient pressure, which is highly important for improving patients’ self-management and quality of life.14,15
Research has been undertaken to explore how mobile health systems can be used to provide self-management support to patients.16–18 Although related interventions have been reported in the literature, the evidence available is rather dispersed, and there is no unified and clear self-management support scheme specifically tailored for patients with IBD, which makes it difficult to provide systematic, personalized self-management support for these patients. Therefore, we conducted a systematic review of studies investigating self-management support for IBD patients delivered through mobile health systems. The purpose of our study was to summarize the best evidence after evaluating the quality of the studies, hoping to make a case for healthcare workers to carry out self-management support through mobile health systems to improve patients’ self-management abilities.
Methods
This study adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines. 19 The review protocol was registered with PROSPERO (ID: CRD42024519521) and is publicly available. No modifications were made to the protocol during the review process.
Search strategy
A systematic literature search was independently conducted by two researchers for articles published up to October 2023 across guideline networks, professional society networks, and databases. Data sources: (i) The guideline networks searched were as follows: BMJ Best Practice, UpToDate, Joanna Briggs Institute (JBI) Library, Scottish Intercollegiate Guidelines Network (SIGN), National Institute for Health and Care Excellence (NICE) website, Guidelines International Network (GIN), National Guideline Clearinghouse (NCC), Registered Nurses Association of Ontario (RNAO), Yi Maitong, and MedSci. (ii) The professional society websites searched were as follows: World Gastroenterology Organisation (WGO), International Organization for the Study of IBD (IOIBD), American College of Gastroenterology (ACG), American Gastroenterological Association (AGA), British Society of Gastroenterology (BSG), European Crohn's and Colitis Organisation (ECCO), IBD Society of Taiwan, Chinese Society of Gastroenterology, Chinese Medical Association, and Chinese Nursing Association. (iii) The databases searched were as follows: PubMed, Cochrane Library, Web of Science, Embase, China National Knowledge Infrastructure (CNKI), Wanfang, and China Biology Medicine disc (CBM).
Guidelines and consensus documents were obtained from guideline network, professional society website, and database searches using the terms ‘Inflammatory bowel disease/Crohn's disease/ulcerative colitis’ AND ‘self management support/self care support’.
A systematic search of the databases was conducted. ‘Inflammatory bowel disease/Crohn's disease/ulcerative colitis’ AND ‘self management support/self care support/self management’ AND ‘telemedicine/mobile health/mHealth/Telehealth/eHealth/mobile application/app/smartphone/short message service/We Chat/QQ’ were used as search terms. Supplementary Material 1 provides the complete search strategy used for each database.
Inclusion and exclusion criteria for the studies
To be eligible for inclusion in this study, the articles had to meet the following inclusion criteria: (i) study subjects were IBD patients who were ≥18 years; (ii) Study contents include self-management support for IBD patients delivered through mobile health systems; (iii) The types of literature included guidelines, evidence summaries, expert consensus, systematic reviews, clinical decisions, best practices, and empirical research closely related to the topic; (iv) for revised or updated guidelines, only the latest edition was included; and (v) the language of publications was limited to Chinese or English.
Articles were excluded from the study if they met any of the following exclusion criteria: (i) direct translations, or repeated inclusions of foreign guidelines or expert consensuses, such as guideline interpretations; (ii) literature with incomplete information or inaccessible full text, including research proposals, drafts, reports, or abstracts; and/or; (iii) studies that did not pass the quality assessment.
Selection process
The literature review process was initiated in October 2023 (updated in December 2023). Our aim was to enhance sensitivity by integrating studies in the initial screening, even if the content that was directly relevant to our inquiry was not included in the abstract. During the screening of the searched records, two authors (CR and QC) independently evaluated the qualifying titles and abstracts. In cases of disagreement, a third reviewer (YZ) was consulted for resolution. After the titles and abstracts were examined by two researchers, the potentially eligible records were consolidated. During the title and abstract screening phase, the complete texts of the articles were acquired. Each text was then independently reviewed by two reviewers (CR and QC), and in case of any disagreement, a third reviewer (YZ) was consulted. After collectively reviewing all the studies, those deemed suitable for inclusion were selected.
Quality evaluation
The quality evaluation criteria, according to the type of study, were as follows: (i) The Appraisal of Guidelines for Research and Evaluation Instrument II (AGREE II) was used to evaluate the quality of the guidelines. The evaluation tool consists of 6 fields, 23 items, and 2 overall evaluation items. Each item is scored from 1 to 7 points: 1 is strongly disagree, and 7 is strongly agree. The final score in each field is calculated using standardized percentages. Scores in all fields >60% are grade A; scores in 3 or more fields between 30% and 60% are grade B; scores in 3 or more fields <30% are grade C. 20 (ii) The quality evaluation tool developed by the JBI Evidence-Based Health Care Center in 2016 was used to evaluate the quality of expert consensus, systematic reviews, quasi-experimental studies, and qualitative researches. 21 Two researchers (CR and MZ) with training in evidence-based nursing independently assessed the quality of the literature; in cases of disagreement, a third, highly trained researcher (YZ) was consulted before a decision was made.
Summary and grading of evidence
Relevant evidence on self-management support schemes for patients with IBD based on mobile health systems was independently collated and extracted by two researchers (CR and QC) trained in evidence-based nursing and checked by a third researcher (YZ) trained in evidence-based nursing. Evidence that was consistent or complementary was incorporated. When the content of the evidence from different sources conflicted, the inclusion principle followed in this study was evidence-based evidence, high-quality evidence, and the latest published authoritative literature first. The 2014 version of the Australian JBI evidence pregrading and recommending level system 22 was used to determine the evidence grade, which was divided into levels 1–5 according to the types of studies included in this study, with 1 as the highest level and 5 as the lowest.
Results
Literature review results and general information on the included studies
Initial database searches yielded 2072 studies. After removing 285 duplicates using EndNote, 1787 studies remained. Two researchers (CR and QC) independently reviewed the titles and abstracts of each study. After excluding studies without full-text availability, 206 articles remained. Following full-text review, 191 articles were excluded for not meeting the inclusion criteria. This resulted in 15 articles included in the final analysis: one guideline, 23 two expert consensuses,24,25 four systematic reviews,12,26–28 four quasi-experimental studies,29–32 and four qualitative researches.33–36 The PRISMA flow diagram in Figure 1 depicts the study selection process. Table 1 depicts the basic characteristics of the included studies.
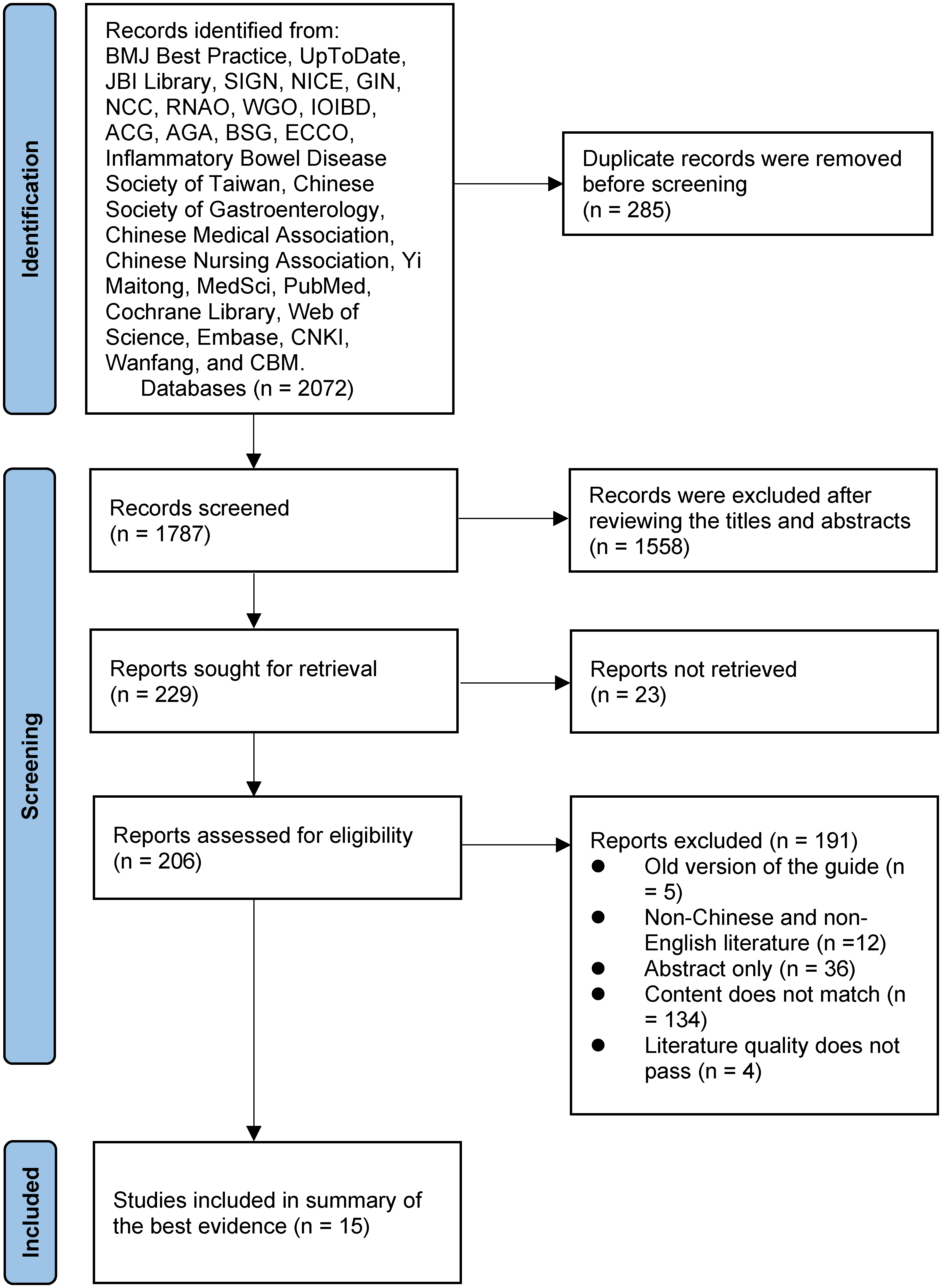
PRISMA flow diagram of the study selection process.
Basic characteristics of the included studies.

Quality evaluation results of the included studies
The methodological quality of the included guideline, expert consensuses, quasi-experimental studies, and qualitative research was assessed using the JBI Critical Appraisal tools (2016). Detailed results are presented in Supplementary Material 1. Recommendation levels for the guideline are shown in Table 2. All included studies were of medium to high quality and were approved for inclusion after discussion by the study team (CR, MZ, and YZ). Four systematic reviews12,26–28 were included in this study. For the study of Conly et al., 12 item 6, “Was critical appraisal conducted by two or more reviewers independently?” was evaluated as “no”, and the other items were all evaluated as “yes”. For the study of Davis et al., 26 item 9, “Was the likelihood of publication bias assessed?” was evaluated as “unclear”, and the other items were all evaluated as “yes”. For the study of Gordon et al. 27 and Pang et al., 28 all items were evaluated as “yes”. Overall, the quality of the studies was high, and was deemed suitable for inclusion in the present study.
Quality evaluation of the guideline.

Evidence aggregation and generation
By summarizing the evidence on self-management support schemes for patients with IBD based on mobile health systems, 36 pieces of best evidence were summarized from 7 aspects, including mobile health system type and functional support; mobile health system application preparation; health information recording, uploading, and presentation; zoning management of diseases and early warning of the active period; support related to health education; healthcare support team formation and services; and virtual communities, as shown in Table 3.
Summary of the best evidence on self-management support schemes for patients with IBD based on mobile health systems.

Discussion
Mobile health systems have received increasing attention as a new means of disease self-management for IBD patients and have shown good usability and acceptability among patients. 13 With the progress of related research, the problem of poor usability by patients has gradually been revealed.17,18,37 This may be related to the fact that most mobile health systems are used infrequently by patients, and the lack of collaborative participation of healthcare workers leads to unsatisfactory use results. 38 Therefore, there is an urgent need for healthcare professionals to provide patients with self-management support. We are committed to integrating relevant self-management support strategies to support patients in using mobile health for disease self-management to improve patient compliance and protect patient health. This information has been encompassed in numerous recommendations, guidelines, etc., in various databases. In our study, the primary focus of healthcare workers delivering self-management support to patients via mobile health systems was categorized into seven main aspects: mobile health system type and functional support; mobile health system application preparation; health information recording, uploading, and presentation; zoning management of diseases and early warning of the active period; support related to health education; healthcare support team formation and services; and virtual communities. However, some of the included studies did not cover all aspects. Consequently, it becomes imperative to synthesize and present all favourable evidence while also ensuring regular updates and supplementation of evidence to expedite the dissemination of advanced research findings to clinical settings.
Evidence 1–4 summarized the types of mobile health systems that provide self-management support for IBD patients and the functions they should have. Mobile health systems include telephone services, social media, remote management systems, mobile health applications, etc.39,40 However, given that remote management systems and mobile health applications are portable, intelligent and fully functional to meet the diverse needs of patients, remote management systems and mobile health applications are recommended as self-management platforms. Mobile health system applications can be divided for patient use and medical use, facilitating better patient management through the system. The medical end provides functions for interaction, automatic tracking of visits, remote monitoring and management, health interventions, and other functions. The patient end has access to services such as doctor-patient interactions, health counselling, self-management support, health data upload, examination report acquisition, and information support.26,28 Considering the particularity of IBD, patients need to undergo regular clinical reviews to monitor the illness, but patients often forget their appointments, which leads to worsening of the disease. 31 Therefore, it is necessary to add a reminder function to the mobile health system. With the rapid development of information technology, 13 big data processing functions have been gradually applied to mobile health systems; these systems can combine, split, and match the content of self-management support for different IBD patients’ needs and provide patients with precise and personalized support, thus facilitating patient self-management from passive acceptance to active participation and enhancing patient self-management enthusiasm.
Evidence 5–7 summarized the preparations of IBD patients before they use the mobile health system. Since mobile health systems are new for users and require an acceptance process, user training is required before patients can formally use them. The training content includes an introduction to the basic disease knowledge of IBD and guidance on the use of the mobile health system; the training formats can include pre-recorded video courses or offline training sessions. It is recommended to keep the training sessions concise and focused, ideally between thirty to forty-five minutes.30,32 After patients master their usage, they can be guided to enter personal information and medical history and at the same time create personal files in the mobile health system to facilitate the storage and management of patient health information.26,30
Evidence 8–17 summarized the health information content that IBD patients need to record in the mobile health system, as well as the uploading and presentation of related content in the system, thus laying a good foundation for the development of self-management support. Health information recording is a prerequisite for healthcare workers to provide self-management support for patients. Complete and accurate health information records are very important for healthcare workers to manage patients online. There is substantial evidence supporting the inclusion of various components in recording patient information. These components encompass self-assessment questionnaires, medication administration records, diet diaries, symptom documentation, test results, medical visits, and body mass index measurements.25,27,32,35,36 By incorporating these elements into patient records, healthcare workers can gain a comprehensive understanding of the dynamic changes in a patient's condition, enabling more accurate evaluation. Malnutrition stands out as a significant clinical manifestation among patients with IBD, contributing to increased mortality rates. Effective nutrition management plays a crucial role in reducing nutritional risks and addressing malnutrition in IBD patients. However, due to a lack of nutrition knowledge among many patients, optimal nutrition management is often not achieved. 41 Consequently, it becomes imperative to provide specialized nutritional support to patients. Nevertheless, the limited number of clinical IBD healthcare workers and the demanding workload of outpatient services make it challenging to deliver comprehensive offline nutritional support. 42 Fortunately, the continuous advancement of information technology has given rise to mobile health systems, facilitating online nutrition support. Healthcare workers can now offer patients professional nutrition knowledge and dietary guidance through online platforms, thereby enhancing patients’ ability to manage their nutrition effectively. This study also focuses on nutrition support, which involves providing health education materials related to diet and nutrition, supplying nutrition status assessment questionnaires, offering a body mass index recording module, and furnishing a diet diary recording module. By reviewing and documenting these aspects, patients can expand their knowledge base on diet and nutrition, promptly monitor their nutritional status, and identify dietary contraindications, thus enabling better disease management. Additionally, Coşkun et al. 42 propose the provision of telenutrition consultations for patients with mild disease or those in remission. This approach caters to individual patient needs, reduces medical costs, and holds significant value. Since electronic medical records and imaging systems across medical institutions have not been established at this stage, information sharing and in-depth integration among medical institutions cannot be realized; therefore, medication use records, examination data records, and medical consultation records are mainly recorded manually or uploaded as photos, thus increasing the input time of patients, which may lead to a decrease in the accuracy of patient input data and patient compliance with mobile health systems. This limits the further development of mobile health. In the future, we should strive to achieve information sharing among medical institutions and reduce the input burden of patients’ health information to increase patients’ willingness to continue to use mobile health systems. Patient data should be uploaded in encrypted form and stored in the mobile health system to protect patient privacy.26–28 However, the “2017 Cost of Data Breach Study: Global Overview” released by the IBM Security and Ponemon Institute showed that the average cost of global health data disclosure is 380 dollars, 43 and the current mobile health systems on the market have not implemented this very well. This has led to some users’ concerns about the disclosure of personal privacy information when using mobile health systems, and when users do not trust privacy protection measures, they may choose to refuse to disclose personal information. Therefore, when developing a mobile health system in the future, we should fully consider the setting of information technology for protecting patients’ privacy and reducing security risks in the process of patient use. When health information is presented, healthcare workers hope that the mobile health system can present the patient's health data in a clear and intuitive form (such as in the form of a chart). With this, they can clearly understand the disease performance and health status of patients in the shortest possible time and improve work efficiency.27,30,34–36
Evidence 18–20 summarized the mobile health system's zoning management and early warning of activity for IBD patients. Zonal management of disease refers to judging the severity of a patient's disease according to disease indicators and dividing it into three zones: red, yellow, and green. The red zone indicates that the patient is in a severe disease state, the yellow zone indicates that the patient is in a mild-to-moderate active disease state, and the green zone indicates that the patient is in remission.23,26,29 Dividing patients according to their disease severity will help healthcare workers better manage patients. On the one hand, healthcare workers can identify the patient's current disease status as quickly as possible through partitioning. On the other hand, they can provide self-management support services suitable for the patient's current disease state according to the patient's partition. At present, the disease indicators included in the partitions and the partitioning standards of related disease indicators have not yet reached a unified standard. Several studies have used the disease activity index as the only criterion for partitioning,37,44 and other studies have used the disease activity index and faecal calprotectin concentration as common partitioning criteria. 45 Moreover, considering the particularity of the IBD population, the criteria for determining the value of disease indicators can be appropriately relaxed compared to those of the general population. Therefore, it is suggested that healthcare team members jointly determine the disease indicators to be included in the zone and establish zoning standards for different disease indicators and thresholds for generating alarms according to the severity of the disease. 29 When the disease index reaches the predefined warning value set by the healthcare team, the system automatically generates an alarm and sends an alarm reminder to the patient via email, prompting the patient to seek medical treatment as soon as possible and providing updates on the condition, thereby improving clinical outcomes and quality of life.26,27,30,36 In this process, the patient's ability to identify potential health risks can also be gradually improved. 46
Evidence 21–28 summarized the content, sources, presentation forms, and expressions of health education materials that IBD patients can access in mobile health systems. Good self-management behaviour in patients is based on understanding the disease and receiving guidance. Mastering disease-related knowledge is at the core of self-management. By providing support related to health education for IBD patients, we can improve their knowledge, skills, self-efficacy, etc., thereby improving their self-management abilities and delaying disease progression. 47 In the process of disease management, IBD patients often experience self-management and decision-making problems due to a lack of disease-related knowledge or confusion from complex and contradictory information. Therefore, once IBD patients are diagnosed, they should be provided with support related to health education immediately to help them establish good self-management behaviours.34,44 Research shows 48 that IBD patients want to obtain diversified, personalized, and specific health education materials, and mobile health systems have this advantage. By adding a knowledge database module to the mobile health system, educational topics can be presented in the form of mind maps to provide patients with systematic and comprehensive health education materials.27,31,36 Through the presentation of mind maps, patients can quickly find what they are interested in among numerous materials. Before compiling health education materials, patients’ needs for health knowledge can be investigated through questionnaires, and the healthcare team can determine the educational content and educational themes based on the patients’ needs.12,24,30,32,34,36 This ensures that the health education materials developed are what patients need. The content of health education materials should come from the latest authoritative research results, be reviewed by professional doctors, and be presented to patients in a form that is illustrative and easy to understand.25,32,34,36 In addition, many patients express the desire to obtain the most cutting-edge health information about the disease in real time. Therefore, the latest developments in drugs and treatments can be provided to patients through mobile health systems, and reminders can be sent to patients so that they can receive timely information updates. 48 When patients read health education materials, they can provide feedback on those with poor legibility to the healthcare support team, and healthcare workers can modify the content of the materials with poor legibility,27,31,35 thereby improving the readability of the health education materials.
Evidence 29–35 summarized the composition and specific service content of healthcare teams that provide self-management support services for IBD patients. Self-management support via mobile health systems was effective at reducing patients’ disease activity and improving patients’ quality of life, but the loss to follow-up rate was high during the study.17,30,44,45 There are many reasons why patients are unwilling to continue to use mobile health systems to manage diseases. One of the main reasons is the lack of continuous and effective supervision, support, and communication by medical teams in the process of using the mobile health system to manage diseases. 36 Therefore, it is necessary to establish a professional medical team. With the participation of a medical team, patients’ willingness to continue to use the mobile health system can improve. However, the composition of medical team members is still controversial. Some studies suggest that team members should come from multiple disciplines,12,35 while others believe that team members can include only healthcare workers from gastroenterology departments.24,31–33 Considering that the self-management support services provided by medical team members are mainly for home-based IBD patients in remission, multidisciplinary teams mainly target IBD patients with complex disease conditions; therefore, this summary of the best evidence suggests the establishment of a healthcare team, including an IBD specialist, gastroenterologist, IBD specialist nurse, colostomy specialist nurse, and digestive department nurse, to provide self-management support for patients. Through the establishment of a healthcare support team, we can provide services for patients through health monitoring, remote consultation, online follow-up, etc., reward patients with high enthusiasm for self-management, and solve difficulties for patients with low enthusiasm. When applying the relevant evidence in clinical practice, full play should be given to the subjective initiative of nurses, a nurse-led team model should be established, and personalized self-management support services should be provided for IBD patients through doctor and nurse cooperation.
Evidence 36 summarized the ways in which patients with IBD receive peer support in mobile health systems. Mobile health systems can be used as a medium to create virtual communities where patients can share experiences, discuss treatments, find fellow patients with similar disease characteristics or experiences, obtain support from fellow patients, learn from each other, and inspire each other. 36 Interpatient communication and experience sharing can be promoted through peer support to improve self-efficacy. Notably, interpatient communication needs to be correctly guided, and through online communication, patients’ subjective initiative can be effectively stimulated, positive communication between patients can be encouraged, and each patient's awareness of self-management can be promoted.
Current evidence provides a clear understanding of the functional modules and content of healthcare workers support offered by mobile health systems for IBD patients. However, the integration of artificial intelligence (AI), a rapidly evolving technology, remains limited in this domain. 49 It is suggested that AI technology could be incorporated into the development of mobile health systems in the future. User portrait could be made based on each patient's medical history, disease status, medication administrated, etc. and specific disease knowledge could be pushed to specific users by recommendation algorithm to realize personalized self-management support services so as to improve the user experience of the mobile health systems. 50
Strengths and limitations
The strengths of our study are as follows. First, to ensure that our research was scientific and rigorous, we strictly adhered to the evidence summary formation method advised by evidence-based nursing, retrieved pertinent evidence in a systematic manner using the “6S” evidence model, and summarized the evidence according to the inclusion and exclusion criteria and quality evaluation. Second, the current study focused on different interventions to provide self-management support to IBD patients via mobile health systems and systematically synthesized high-quality evidence on this topic, the results of which should be of interest to IBD medical teams.
However, our study has several limitations. First, the evidence we summarized included only published studies in Chinese and English, and studies in other languages should be included to form a better summary of the evidence. Second, although we attempted to conduct the literature search as exhaustively as possible, some studies may still have been missed, and there may still be a risk of publication bias. Readers are therefore advised to critically select the best available evidence. Moreover, the best evidence summary will continue to change over time and should be updated by researchers. Third, although the evidence summarized in this study provides a reference for healthcare workers to provide patients with self-management support through mobile health systems, there is no unified standard for the specific division of labour, frequency, or duration of support. Therefore, it is necessary to improve the scheme in the future based on the needs of patients and healthcare workers.
Conclusions
This study summarized the best evidence on self-management support schemes for IBD patients based on mobile health systems, including seven aspects and thirty-six best evidence items, providing a theoretical basis and practical guidance for healthcare workers to use mobile health systems to support patient self-management. However, since this study included only Chinese and English language studies, there may be cultural differences in the support schemes used, and some obstacles may arise during operation. Therefore, further clinical transformation is needed before the plan can be put into practice. In the process of follow-up, specific clinical situations should be evaluated, the opinions of patients and healthcare workers should be accepted and included to support the patients, and support schemes should be improved to obtain personalized and operable self-management support schemes, whose feasibility and effectiveness should be further verified.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241261906 - Supplemental material for Summary of the best evidence on self-management support schemes for patients with inflammatory bowel disease based on mobile health systems
Supplemental material, sj-docx-1-dhj-10.1177_20552076241261906 for Summary of the best evidence on self-management support schemes for patients with inflammatory bowel disease based on mobile health systems by Chenfei Ren, Yunxian Zhou, Qian Cai and Mi Zhou in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241261906 - Supplemental material for Summary of the best evidence on self-management support schemes for patients with inflammatory bowel disease based on mobile health systems
Supplemental material, sj-docx-2-dhj-10.1177_20552076241261906 for Summary of the best evidence on self-management support schemes for patients with inflammatory bowel disease based on mobile health systems by Chenfei Ren, Yunxian Zhou, Qian Cai and Mi Zhou in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the experts who generously contributed their time to provide guidance for this article.
Contributorship
CR and YZ conceived this study. CR and QC completed the literature search, literature screening, data extraction and data integration. CR, MZ and YZ evaluated the quality of the studies. CR wrote the first draft of the manuscript. YZ and QC critically revised the manuscript for important intellectual content. All authors reviewed the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Public Welfare Science and Technology Research Program Project of Jinhua City (grant number 2021-4-244).
Guarantor
YZ.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.