
Abstract
Objective
We conducted usability sessions with publicly insured pregnant individuals living with type 2 diabetes (T2D) and unmet social needs, and their care team members to assess: (1) interface usability, (2) user experience, and (3) clinical workflow integration facets of a high-fidelity prototype of our multi-component digital solution to refine user specifications for the randomized controlled trial (RCT).
Methods
Five patients and eight care team members from a tertiary Diabetes in Pregnancy Program participated between March and July 2023. Data collection included think-aloud sessions, empathy mapping, and semi-structured discussions guided by the double diamond framework. Transcripts were coded by four researchers, with saturation assessed across participants. Personas were created grounded in Social Cognitive Theory. Usability feedback was synthesized using affinity diagramming and IBM prioritization matrices. We conducted a reference-based validation study in which care members addressed persona-driven scenarios; proficiency, efficiency, and concordance with expert recommendations were calculated to identify areas for refinement.
Results
We identified 21 desired mHealth and six dashboard topics. The top three mHealth topic frequencies were personalized prompts (85%), learning card content (62%), and glucose tracking (62%). The top three dashboard topics were prioritized clinical and social needs pathways (63%), social needs risk levels (50%), and glucose tracking (50%). Three personas emerged: (1) “hands off,” (2) “overwhelmed but trying,” and (3) “engaged.” In the validation study, concordance varied: goal setting showed 100% concordance, while social needs referrals had the highest discordance (60%). Average proficiency and efficiency scores across scenarios were 40% and 37%, respectively, with the lowest agreement for “engaged” persona scenarios.
Conclusion
Patients and care team members identified highly valued and implementation-challenging features using our prototypes. The personas highlighted distinct engagement needs, and validation results underscored variability in concordance for social needs management. These findings inform pre-RCT refinements of the digital solution.
Introduction
The frequency of pregestational type 2 diabetes (T2D) has more than doubled over the past 2 decades in the United States, and is one of the most frequent chronic comorbid conditions in pregnancy, affecting nearly one in three pregnant individuals. 1 Nearly one in two individuals with T2D will experience an adverse pregnancy outcome (APO), including preterm birth, large for gestational age, congenital abnormalities, preeclampsia, and stillbirth. 2 The risk of APOs is increased with inadequate glycemic control. Achieving glycemic control requires an integrated, multi-component approach broadly defined as “diabetes management” or “diabetes self-management,” including behavioral changes, such as diet, physical activity, and self-monitoring, pharmacotherapy, engagement with the care team or prenatal and diabetes care providers, and increasingly the use of technology (continuous glucose monitors, CGM). 2 Engaging in diabetes self-management can be challenging and difficult for individuals who experience a high burden of unmet social needs.2–4 For pregnant individuals, unmet social needs (e.g., lack of transportation, nutrition, and food insecurity) can exacerbate the ability to effectively manage T2D, putting individuals at higher risk for APOs. 5
Despite the importance of comprehensive management, current maternity care models are often misaligned with patient preferences. 6 Pervasive technologies, such as mobile health (mHealth) apps and Internet of Things devices, offer new opportunities to support diabetes management in pregnancy. 7 Surveys indicate that nearly 75% of pregnant individuals have downloaded at least one mHealth app, with most using them weekly,8,9 and over 90% of women of reproductive age, including those on Medicaid, own smartphones. 10 Pregnant individuals report willingness to use digital tools for health management,11,12 suggesting high feasibility for mHealth approaches in this population.
Mobile applications have been created to either improve diabetes management or promote positive pregnancy health behaviors.13,14 In addition, mHealth apps have been created to support social needs screening and connect individuals to community resources.15,16 Despite these independently designed applications, there is a lack of applications that address the combination of T2D management, pregnancy, and social needs. Most applications are only patient-facing and do not provide data to help the care team review and manage care for patients.
Provider-facing dashboards offer a complementary solution by integrating patient-reported and clinical data, delivering real-time alerts on glycemic control and psychosocial issues, 17 supporting team-based provider coaching, 18 and enabling behavior change strategies.19,20 In non-pregnant populations, such approaches have improved glycemic control 21 and adherence to evidence-based diabetes care. 17 Together, a bi-directional platform that combines a patient-facing mHealth app with a provider-facing dashboard could provide a comprehensive, tailored, and sustainable intervention to address both the clinical and social needs of publicly insured pregnant individuals living with T2D.
As part of a larger trial aiming to improve pregnancy outcomes and glycemic control for publicly insured pregnant individuals living with T2D and unmet social needs, we developed a personalized digital solution that integrates a patient mHealth app, CGM, care team dashboard, coaching, and access to a community health worker (CHW). This multi-component intervention aimed to provide patients and their care team with resources for better clinical management and support patients with unmet social needs.5,22 Participants in our previous work provided specific expectations for digital tool features and content that formed the basis of our initial prototype.5,22
The current analysis builds on our exploratory study, where we interviewed 30 patients and 14 care team members to gain insights about patient and care team perspectives on digital solutions in obstetric care. 23 We found that both patients and care team members were interested in using patient-facing digital solutions to report patient-generated data (PGD). 23 These findings formed the basis of the ACHIEVE intervention. 22 Our team first developed low-fidelity prototypes and evaluated them with seven patients and seven care team members using a mixed-methods approach. Based on the validated NASA Task Load Index survey, participants rated both the mHealth application and care team dashboard in the 20th percentile of the national distribution without pre-testing training, suggesting that user interfaces were clear and straightforward. 24 Albeit, we documented feedback for required improvements to a high-fidelity prototype.
Our study consists of three objectives. We conducted usability sessions with patients and providers to assess: (1) the interface usability, (2) user experience, and (3) clinical workflow integration facets of our digital solution (a high-fidelity mHealth and dashboard application) to ascertain a refined set of user specifications for the primary study's randomized controlled trial (RCT). Interface usability refers to how participants interact with the prototypes. User experience consists of evaluating participants’ thoughts, feelings, and actions while using the prototypes to further examine their motivations. Clinical workflow integration focuses on the participants’ behaviors when engaging with the prototypes to develop an optimal workflow. Our approach for developing the ACHIEVE RCT intervention is grounded in an evidence-based framework for creating inclusive and personalized mHealth solutions. 5
Methods
Study setting and sample
Patients
Our research team recruited individuals from the Diabetes in Pregnancy Program within the division of Maternal Fetal Medicine at our AMC. Inclusion criteria included patients who were pregnant, diagnosed with T2D, covered by Medicaid insurance, and able to speak English. We excluded patients who were not 18 years of age or older. A convenience sample was identified and eligible patients were recruited and consented to by a study team member. Each patient received a $30 gift card at the end of the study as an incentive for participation.
Providers
Criteria for provider inclusion required physicians, nurses, diabetes nurse educators, and nurse assistants to be involved in the care of pregnant patients with diabetes. Providers were recruited from the Diabetes in Pregnancy Program. A convenience sample was identified and consented to by a study team member. Each non-physician provider received a $30 gift card as an incentive for participation.
The study was conducted between March and July 2023. This work was approved by the Institutional Review Board of The Ohio State University (IRB2022H0399). Patients and providers provided verbal consent to participate in this study.
Data collection and analysis
We first developed a research-informed patient proto-persona that reflected a potential user of the ACHIEVE mHealth application. The persona was grounded in (1) prior qualitative user experience sessions conducted as part of this study, (2) clinical experience of the multidisciplinary research team, and (3) formative discussions with care team members who routinely care for pregnant individuals with T2D and unmet social needs. The persona created was a pregnant individual with T2D who experienced unmet social needs, such as housing insecurity, lack of transportation, inadequate healthcare access, and need for health education. This persona used a smartphone for social media and sought health information using resources such as WebMD. We confirmed with care team members that the patient persona accurately reflected the types of patients they managed. Providing participants with patient personas allows participants to immerse themselves in the feedback process and provide clarity with assumptions about the intent of application design (see example mHealth application flow for patient persona in Figure S1). The persona was subsequently operationalized through multiple realistic patient scenarios (and confirmed by the clinical members of the research team) derived from themes observed in user experience sessions, which were then presented to participants to elicit appropriate clinical and social needs–related responses. These scenarios also informed downstream design decisions and care pathway mapping to support better clinical workflow integration.
We conducted interviews with patients and care team members to gather user specifications for our digital solution, guided by the double diamond framework, focusing on interface usability, user experience, and clinical workflow integration. At the beginning of each interview, participants were shown a video introducing the patient persona. Interviews were roughly 60 min and were conducted either virtually or in person in the clinic. Zoom was used to audio-record and transcribe the interviews verbatim. A research team member reviewed the transcripts for accuracy. Three team members conducted interviews and three team members performed the analysis for this study. This study was conducted and reported in accordance with the COREQ guidelines, 25 which are summarized in a supplementary table (Table S1). We conducted semi-structured interviews and group interviews with patients and care team members, with both deductive and inductive analysis. Interviews were facilitated by NF, CS, and YW, who had training in mixed-methods, qualitative, and user experience research; two physician scientists (JJJ and KKV) contributed clinical expertise. KKV has a physician–patient relationship with some of the patients. Interviewers were diverse in gender and age and disclosed the scientific purpose of the study to participants.
Participants were recruited by research staff from clinic lists provided by a clinical lead. A convenience sampling approach was used, maximizing diversity by race/ethnicity. In total, five patients and eight care team members participated, while 33 individuals were approached; non-participation was primarily due to time constraints, caregiving responsibilities, or health reasons. Interviews were conducted via Zoom or telephone, typically lasting for 60 min. Audio recordings and field notes were collected, and data saturation was monitored throughout. Four researchers coded transcripts using Microsoft Word, developing a coding tree both deductively and inductively. The research team met after each interview to discuss emerging themes, and saturation was determined by the consistency of general themes across participants, while also capturing in-depth usability and user experience insights on specific components of the prototypes. All of the guides used in the study were pilot tested with two patients and two care team members. The guides (see Appendix) were also refined from prior studies on similar topics. We present exemplary quotes in the results section. Member checking involved care team members providing additional insights during the workflow integration sessions on the feedback gathered from the usability and user experience sessions.
High-fidelity prototypes
During interviews, we focused on how participants felt about the digital solution using a high-fidelity Figma prototype that illustrated how patient-generated data (PGD) can be used to manage their health. The ACHIEVE mHealth prototype (Figure 1) featured goals on the homepage, a CGM tab that displayed recent blood glucose and insulin values, learning cards on clinical and social needs, and a journal for tracking important events. The care team dashboard prototype (Figure 2) showed hemoglobin A1c levels and CGM time-in-range percentages for the past seven days. Top social needs and a seven-day activity summary were also featured on the dashboard. We investigated how the prototypes may be used to manage pregnant individuals living with T2D.
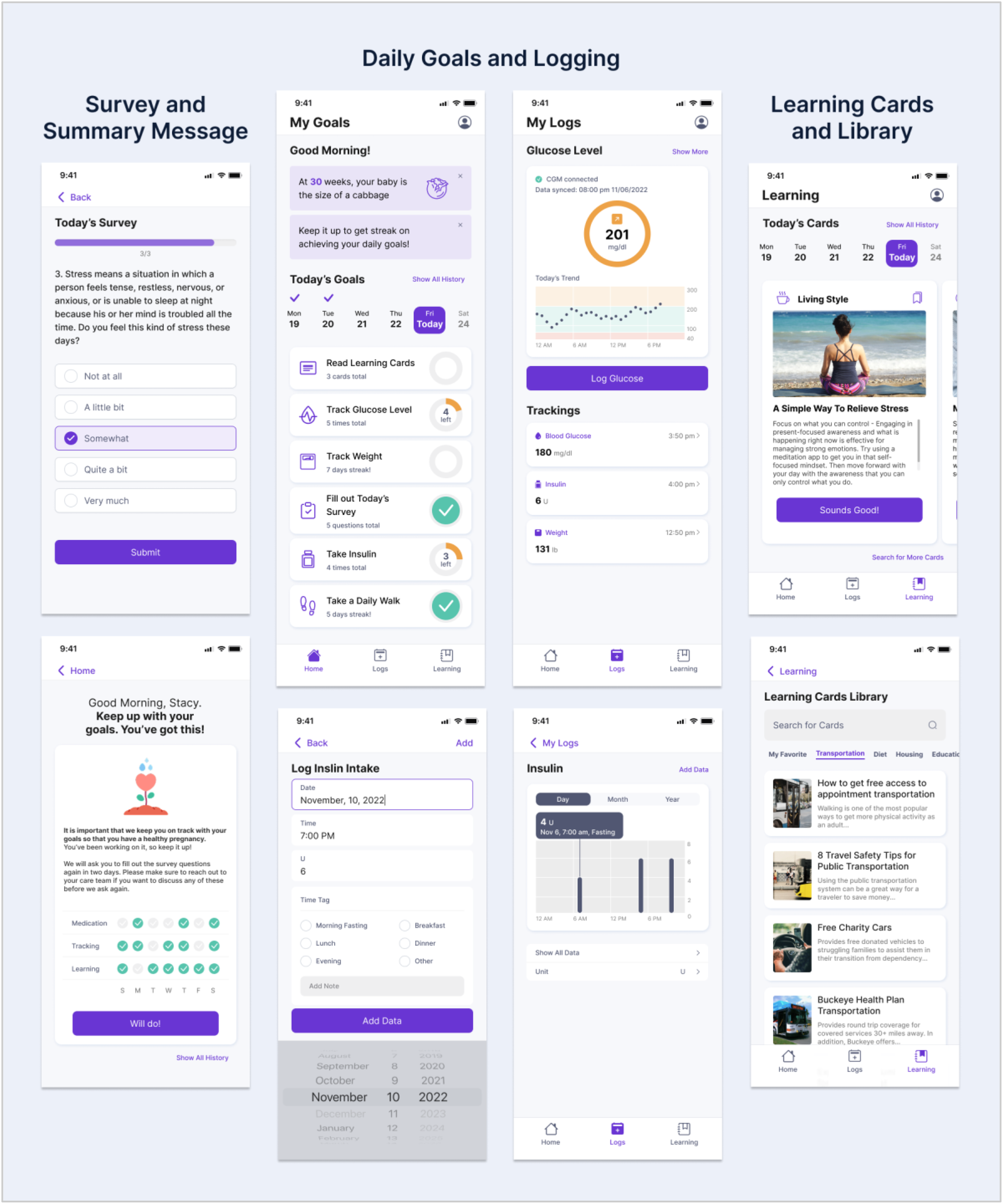
Key features of the high-fidelity mobile health prototype.

Key features of the high-fidelity care team dashboard prototype.
Interface usability
We asked participants during the think-aloud sessions about their perspectives on the appearance and functionality of the prototypes including features, content, and aesthetics. Participants were given the prototype and asked to click around the prototype while sharing their impressions and recommendations. We performed affinity diagramming to analyze participant feedback and group features based on participant perspectives (patients and care team) on the mHealth application and dashboard (care team). Two iterations of clustering were performed to refine the grouping of features. The first iteration focused on building topics and the second iteration identified multiple features associated with themes under each topic. We also categorized user input into positive and negative groups for specific features of the dashboard and mHealth applications on Miro boards. We calculated the frequency of feature preferences. We then developed IBM prioritization matrices for each component of our digital solution to evaluate feature importance and feasibility. In this matrix, the y-axis displays the value of specific features to end-users and the X-axis demonstrates the feasibility to develop and implement features for the research team. An example of an IBM prioritization matrix from our study is displayed in Figure 3.

Sample IBM prioritization Matrix illustrating value and feasibility tradeoffs for the patient mobile health application based on participant feedback.
User experience
We used empathy maps to gather deeper insights into end-user needs and motivation during our interview sessions. Participants completed the empathy maps based on the patient persona presented in a video at the beginning of the usability interview. We documented specific experiences participants believed the patient persona would have while using the prototype. An example of a completed empathy map from a patient participant is shown in Figure. 4. We used feedback from our interviews and our study's conceptual framework, Social Cognitive Theory (SCT), to abductively develop three patient personas. 26 Our intervention was developed to address key SCT constructs, such as an individual's self-efficacy, knowledge and beliefs, and skills to better manage T2D, pregnancy, and social needs. In interviews, we discussed initial impressions of the persona developed by the research team. Table 4 summarizes three personas derived from the proto-persona and deductively refined based on participant feedback mapped to SCT constructs.
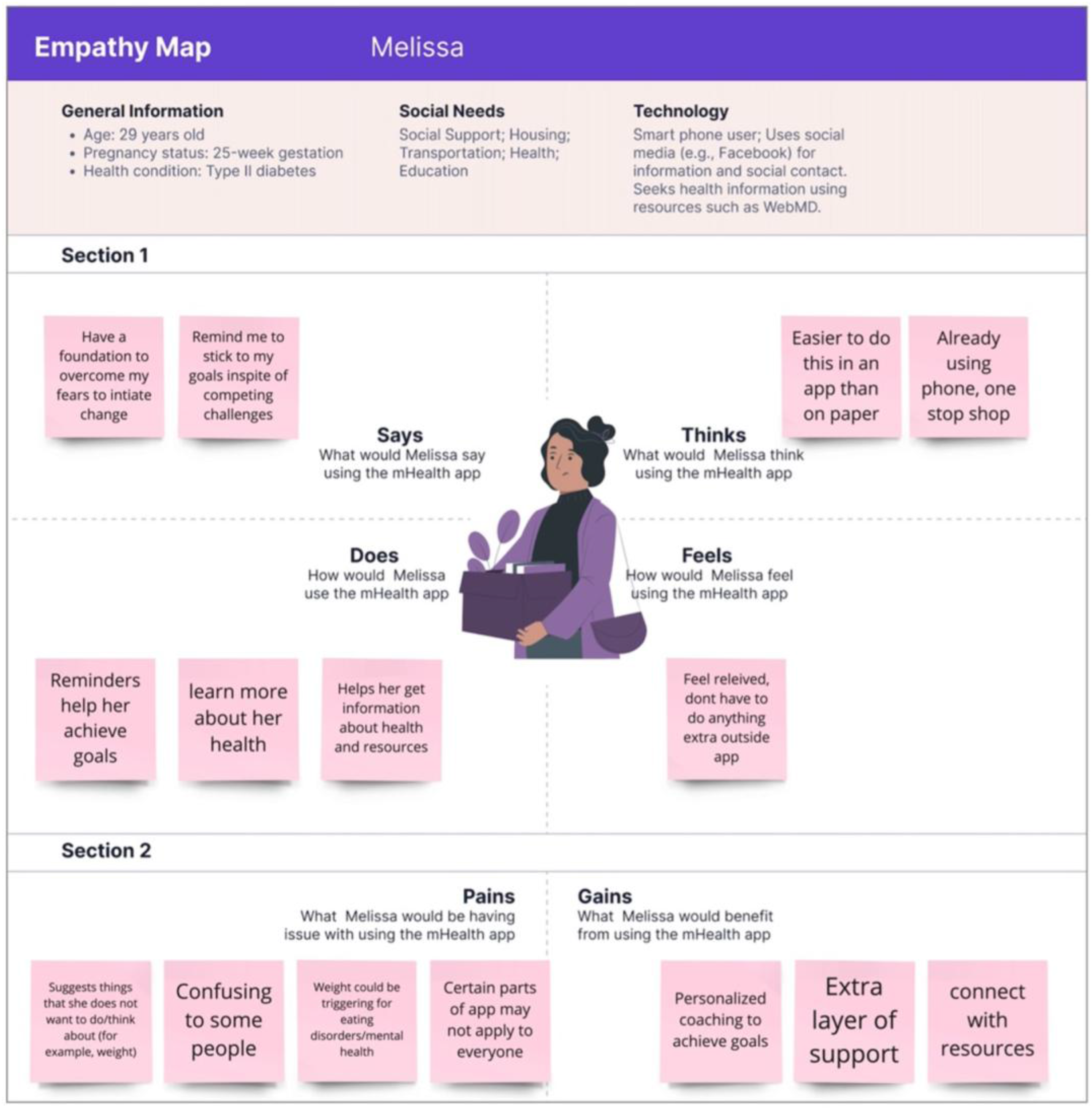
An example of an empathy map for a persona who is 25-weeks pregnant with type 2 diabetes and struggles with social needs (e.g., limited social support and transportation insecurity). This persona uses a smartphone and seeks health information online.
Clinical workflow integration
We conducted a reference-based validation study to identify areas of prototype refinement before embedding the applications in the clinical workflow. The goal of this approach was to evaluate how well care team members’ responses aligned with a reference based on expert guidance when addressing realistic patient scenarios developed from our user-centered personas. By embedding both clinical needs (e.g., referrals, medication adherence, care-based goal setting) and social needs (e.g., diet recommendations, access to transportation or food, journaling) into the scenarios, we aimed to examine concordance across role types, assess proficiency in selecting responses consistent with expert recommendations, and evaluate efficiency in choosing responses with precision and parsimony. This design enabled us to identify where prototypes effectively supported patient needs, where care team approaches diverged from reference practices, and which areas required additional refinement for intervention design, specific work tasks and workflow integration, and training.
We created five realistic patient scenarios based on the new personas derived from our proto-persona and refined after our user experience sessions, and asked care team members what clinical and social need responses would be appropriate for each scenario. Examples of clinical responses were referral to set up doctor's appointment, medication adherence questions, and care-based goal setting. Examples of social needs responses were diet recommendations, sharing a list of neighborhoods resources (e.g., transportation, food pantry, paying bills), and journaling about social needs. An example of a patient scenario is a 36-year-old, “hands off” pregnant patient with T2D, who struggled to manage elevated blood glucose levels despite being recommended to use a CGM. She lacks confidence in managing her health, does not track her diet or insulin, and is unsure why her hemoglobin A1c levels are high. She shares a car with her partner and normally takes the bus to work and her doctor's appointments. She cannot take time off from work easily and tries to schedule doctor appointments during her lunch breaks.
Scenarios were used during the reference-based validation study to examine how well the prototypes addressed each persona's different needs (see Appendix for sample scenarios and response choices). We assessed concordance to learn how care team members can best support different patient types. We also sorted responses based on concordance. This sorting helped identify areas that required more attention in preparation for intervention design, training, and implementation. We calculated proficiency and efficiency scores. Proficiency enabled us to ascertain whether selected responses are aligned with best practices. Low proficiency scores suggested that sub-optimal responses were selected vis-à-vis an established set of responses developed by the research investigators and expert guidance. Efficiency gave us insight into whether responses were chosen in a simple and deliberate manner, with low efficiency scores indicating that participants selected more responses than what was established as necessary for a scenario.
We calculated the interquartile range (IQR) of the deviation from the mean of responses for each scenario across the roles. The smaller the IQR, the higher the concordance across roles. Our established guideline for the reference-based validation study was developed based on the input of a health equity expert and an expert on perinatal health disparities, both of whom were physicians. Subject matter guidance about the responses to these specific scenarios was critical to assess how the care team utilized the intervention from a workflow perspective. If both guides identified the same clinical or social needs response for a scenario, we assigned a score of 1; if they differed, we assigned a score of 0. Next, we compared insights from three diabetes nurse educators with the guides. If the guides and participants identified the same response, then we recorded this as 1; if they differed (e.g., 1 and 0), we recorded it as −1. If both guides and participants did not select a response, then we recorded it as 0. We calculated the algebraic sums of these scores and evaluated proficiency and efficiency, calculating the average proficiency and efficiency across the five scenarios. We calculated proficiency by dividing the algebraic sum of the participant's score by the algebraic sum of the guides’ score. We calculated efficiency by dividing the algebraic sum of the participants’ scores by the total number of responses the participant identified for each scenario. 27 We calculated the algebraic sums of the three participants for each scenario and sorted the clinical and social needs responses from least to most concordant. We also determined which scenarios were the least proficient and efficient.
Results
Participant characteristics
We recruited five patients and eight care team members. Details on patients and care team members are presented in Tables 1 and 2. The average age for our patient sample was 30 years old. For patients, 40% were Non-Hispanic (NH) Black, 20% were NH white, 20% were Hispanic, and 20% were more than one race or ethnicity. The average gestational age was 27 weeks (SD: 8). For care team members, 87% were female and 13% were male. Care team member interviews were completed with three physicians, two diabetes nurse educators, two social workers, and one dietitian.
Characteristics of patient sample (n = 5).
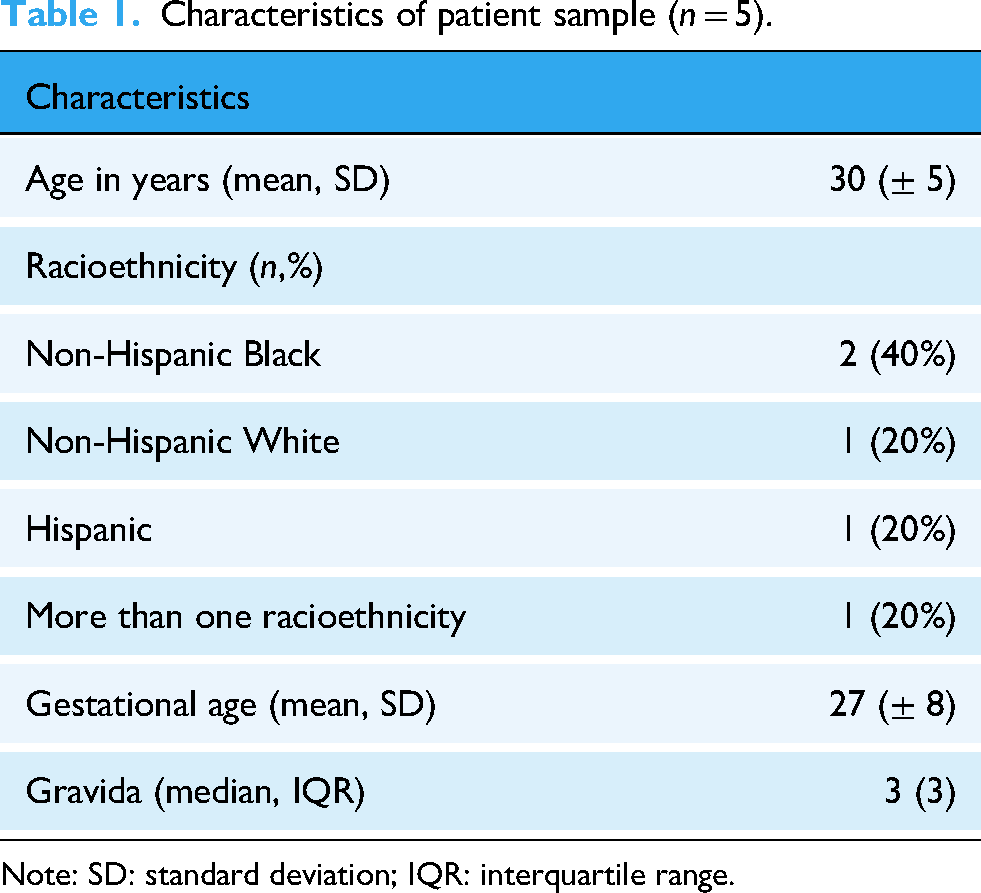
Note: SD: standard deviation; IQR: interquartile range.
Characteristics of care team sample (n = 8).

Interface usability
Affinity diagramming and user feedback
During our usability testing, specific topics emerged after participants engaged with the prototypes. These general topics were documented and participants provided additional insights for each topic. We discuss the general topics below and specific insights from the frequently mentioned topics. Specific topics, sub-features, and the frequency of mentions are listed in Table 3.
Highest frequency topics discussed of desired features (n = 5 patients; n = 8 care team).

We identified twenty-one topics of features for the mHealth application prototype: training on how to use the app, survey questions, compliance, encouragement, privacy, weight tracking, journal feature, connection with CGM, communication, availability in other languages, accessibility, personalization, adding pictures/visuals, shared account for family members, learning cards content, tracking meals and carbohydrates, showing trends, glucose tracking, pregnancy-related information (for baby and mother), personalized prompts, and one-stop-shop functionality. The top three topic frequencies were 85% (11/13) for personalized prompts, 62% (8/13) for learning card content, and 62% (8/13) for tracking and sharing glucose data.
Both patients and care team members valued personalized prompts as essential for managing the complex demands of diabetes during pregnancy. A patient described struggling with medication timing: Sometimes it's 2 hours later when I have to take it [the medication] again, I said, I'm gonna have to set myself a reminder. (Patient 4)
Another patient highlighted the overwhelming nature of managing diabetes during pregnancy while balancing other responsibilities.
Patient 12: I have 2 kids at home, and I'm pregnant, and I work a full time job…I'm not always going to remember. Hey, you need to check your blood sugar… Hey, you need to eat something or hey, you need to take your insulin.
This same patient emphasized the importance of reminders that consider both maternal and fetal health.
Patient 12: To be able to set reminders…that are for you and baby, not just yourself, but the baby that's growing…too much exercise can lead to damage…not enough can [lead to] having higher blood sugars gaining too much weight while you're pregnant, which also has a factor on your baby.
Patients also valued reminders for healthy behaviors, with one patient noting: “I love like chocolate or candy, and maybe something that remind me, avoiding those things… [set reminders for] like walk…maybe drink water” (Patient 2). Walk reminders were particularly valued for prompting physical activity as a glucose management strategy. A patient appreciated the visibility of activity prompts: “I like that view. You can see like your weight, and like the remember to take it 20 min walk today like…it's reminding you that you have to do so” (Patient 2). A patient drew parallels to existing wearable technology: “I see there's like the take a daily walk, which, when I do wear my apple watch, you know, it reminds me to stand up if I've been sitting for a long time, so that's always helpful” (Patient 4).
From the care team's perspective, a nutritionist recognized the clinical value of activity reminders.
Care team member 5: It's like a good reminder for some healthy habits like maybe something that like taking a daily walk is something that I encourage all of my patients to do. But sometimes, you know, they don't have that reminder. It's difficult to get it done.
A patient articulated the clinical rationale: Walking is very important, especially when you're diabetic, any kind of exercise physically is important while you're pregnant, and you're diabetic…because it could also help keep control of how high your blood sugars go. (Patient 12)
Learning cards featuring educational content and social needs resources were valued by both patients and providers for addressing knowledge gaps and access barriers. A patient emphasized the critical need for centralized resource information: “To have all these kind of resources on here is a good idea…because not a lot of women look into getting help because they don't know where to go” (Patient 12). This patient identified specific types of assistance that would be helpful, including “housing…help with like bills, or if they need to help with food, clothing for their children…and themselves.”
Another patient recognized the comprehensive support the learning cards could provide.
Patient 3: I think it's a good thing, because…you can help her [Melissa, the persona] with…a lot of things like getting house assistance, transportation, if she needs it.
Even patients who did not personally need social resources recognized their value for others, with one patient stating: “I feel like I won't use it…but for somebody else, I think it's good” (Patient 2), while expressing interest in nutrition-related learning cards.
From the care team's perspective, providers valued the ability to customize and deploy relevant educational content to patients. A social worker appreciated having control over which resources to share.
Care team member 14: After a patient disclosing what the need is…being able to say, okay, well, we have the specific pathway that we can…make sure that's shared on your app.
A physician noted that tracking which learning cards patients engaged with could facilitate important clinical conversations.
Care team member 11: You know education, Card X number of times and stuff. Then that would prompt the question of hey, you know, are you having some troubles getting here?
Patients emphasized the value of sharing glucose data with their care team to demonstrate adherence and facilitate more productive clinical conversations. A patient highlighted how integrated tracking could help prove compliance to providers and insurers.
Patient 1: The app is going to track sugar and also track when patients taking insulin…doctors will be able to see the patient…submit that to the insurance and see, hey, this person is committed. Their body is just not functioning the way they needed to, and they need that extra help.
Another patient contrasted the app with traditional paper logs: Instead of being complained at all the time about not having your readings, or having your paper to show your readings, you have the app that will show that your log and everything right on what they want to see or what they need to see. (Patient 12)
Both patients and care team members recognized that shared data could transform care interactions and support sustained behavior change. A patient stated the app would “help you with how to manage my sugars” (Patient 3) and enable different discussions with providers. A patient valued how longitudinal data could motivate continued adherence.
Patient 4: It becomes a part of your appointments like, well…I saw that, you know you took all your medicine and…comparing to your test…Look at the results you're getting…that's good motivation to see, like consistency, will get you the results.
Patients also appreciated the convenience of an integrated platform, with one patient noting: “It's nice to see everything on the same place…I don't have space on my phone” (Patient 2). A nutritionist emphasized the clinical utility of integrating food with glucose data.
Care team member 5: having it tied to each data point is definitely the most helpful clinically…I like the proportion of target like coloring like how it kind of tells you immediately like how they're doing.
We identified six topics of features for the dashboard application: clinical history, food tracking, blood glucose tracking, pathways for patients, care team communication, and social needs and dashboard activities. Dashboard activities involved viewing a patient's recent activity or having the ability to review breakdowns of patient survey responses. The top three topic frequencies were 63% (5/8) for clinical and social needs pathways for patients, 50% (4/8) for social needs and dashboard activities, and 50% (4/8) for blood glucose tracking.
Care team members had varied perspectives on clinical and social needs pathways depending on their role and workflow needs. Social workers valued the ability to control which resource pathways to deploy.
Care team member 14: I think that's really helpful, especially after a patient disclosing what the need is, and then being able to say, okay, well, we have the specific pathway that we can…make sure that's shared on your app, so that the provider or social worker, whatever could make sure that they have that particular resource available to view.
Physicians expressed that educational pathways might be less relevant to their specific workflow compared to other team members. A physician stated a preference for activity summaries over pathways on the main dashboard view: “Maybe I don't need the pathways for the patient on that front page. I like the 7 Day activity (Care team member 13).” Another physician explained the division of labor in diabetes education.
Care team member 11: They [diabetic educators] often are the ones who do all of those education sessions…they actually talk to them about like…carbohydrate counting what's that mean? What are good foods, what are bad foods like. That's not what we, as the providers do, [monitoring educational pathways] might be a little bit better suited for them [diabetic educators] than perhaps us [providers].
However, this physician emphasized the value of the dashboard for identifying barriers and making referrals: If there's somebody who's struggling to get to appointments, and I see that they're here [on the dashboard] with transportation, I'm probably gonna have social work see them to see what we can do to kind of help break down that barrier.
Care team members emphasized the clinical value of color-coded social needs risk levels for rapid triage and interdisciplinary coordination. A nutritionist explained how visual prioritization could facilitate cross-disciplinary referrals.
Care team member 5: Prioritize, because that might, you know, obviously like, lead to a referral from another discipline…something that's going to signify to them. Oh, look, that's red over there. I should pay attention to that. That's what it's about food. Yeah, I should get [the nutritionist involved].
A social worker reinforced the need for visual flags given providers’ time constraints.
Care team member 14: They unfortunately don't dig in to our notes or things. So having something that like could be a flag when they're already, you know, busy doing another thing to be like, oh, maybe we should get you know someone else involved.
Care team members prioritized longitudinal trends, detailed adherence data, and identification of patterns. A physician mentioned the importance of accessing granular data.
Care team member 13: “When I look at a paper sheet, I can see that over the last 28 [days]…she's done all of them or half of them,” and emphasized incorporating CGM metrics: “the CGMs have their own graphic of time below range time in range time above range…that's sort of what has become the standard for looking at people's glucose control, time below range, time in range time above range, and the standard deviation and the coefficient of variation.”
The dashboard's value extended beyond in-person visits, with physicians highlighting remote monitoring: “A lot of our diabetes management now consists of reviewing the patients glucose control data, blood pressure data in weeks they don't come to the clinic, and then getting giving them feedback…that would be very helpful (Care team members 9 and 13).” A diabetes educator valued capturing patient insights alongside metrics: “We always ask patients…if they have any thoughts or insights to this weekly review…if they feel like they need more insulin, less insulin. Have they had any problems…with lows in the middle of the night (Care team member 4).” Providers emphasized visual design for safety, with one physician requesting: “Something that is above 140 or above 90, I think, should be somehow highlighted in red…I want to make sure no one's missing that (Care team member 9).”
Feature Evaluation and Prioritization
Creating clusters of identified features allowed us to prioritize user feedback on the digital solution to determine end-user value and feasibility for the research team. Some of the frequently mentioned and valued features were feasible for the research team to execute. An example of these features for the mHealth prototype was creating a place to log activities (e.g., meals) to match with blood glucose events, which was mentioned by 31% (4/13) of respondents (see Figure 5). A social worker valued the ability to quickly identify timing-specific patterns.

Changes made to the mobile health application event tracking based on usability feedback.
Care team member 14: “Being able to go in and say, oh, look! This patient Amelia [a persona] is doing really well like her sugars are always in range. But then, looking at Melissa [a persona] here…she's having a lot of trouble in the evenings like that would be beneficial just to have a little snapshot of like medically, whether they are on track, whether they are adhering to things.”
This social worker also explained the diagnostic utility of integrating food with glucose data: “To be able to print an entire log and say, oh, look! Every time you had issues, this is what you were eating, or here's the similarities we're seeing…it gives you a better picture of what was going on.”
Another example was displaying blood glucose trends, which was mentioned by 31% (4/13) of respondents. The ability to visualize glucose trends over time was valued both for patient self-management and provider review. A patient explained that the tracking would help “Keep better track…even if you have to take your shots…you'll be able to tell you exactly how high or how little or how in between you were (Patient 12).” A patient recounted how her doctor used printed graphs to identify patterns: “We'll see that today. You go, you know, off the deep end. So what can we do to change that one day (Patient 4).”
From the care team's perspective, a physician valued longitudinal data for clinical decision-making.
Care team member 11: What I would look at is the hemoglobin A1c trend. Have we made a difference since the beginning, and how bad was it when we started, and I like the proportion at target the 7 Day glucose summary thing. That is what is going to make a difference.
Users highly valued the ability to set reminders or goals by themselves on the application and 38% (5/13) of respondents mentioned displaying images or illustrations to show the size of the baby each week of gestation. Both features were considered feasible for the research team to implement. Approximately 46% (6/13) of respondents also requested weekly, personalized information about pregnancy for individuals with T2D, which is unique, as most applications only do this for pregnancy. The research team adopted American Diabetes Association (ADA) guidelines to create this feature. 28 It was also feasible to expand the learning cards’ content to provide comprehensive coverage across multiple domains: clinical care management, nutritional guidance, social needs resources, lifestyle factors (including weight management, mental health, and exercise), and CGM utilization tutorials. This expansion directly addressed the feedback from patient participants who requested content on social needs, as illustrated in our feature evaluation (Figure S2).
There were a number of features considered highly valued by users, but difficult to implement. Approximately 38% (5/13) of respondents mentioned features that encourage patients to use the mHealth application and 15% (2/13) of respondents mentioned communicating with the care team via messages or video call. These features were more difficult for the research team to implement within our AMC ecosystem due to security restrictions and challenges with integration within the electronic health record. Other highly valued features that were not as feasible for the research team to deploy were allowing users to define their mealtimes based on personal routines which was mentioned by 15% (2/13) of respondents. Approximately 38% (5/13) valued information about diet and nutrition related to T2D and pregnancy which was difficult for the research team to deploy.
Care team members highly valued color-coded social risk levels on the dashboard and the ability to review breakdowns of survey responses. These features were considered moderately feasible for the research team. A physician underscored how the dashboard could surface unmet needs that patients might not volunteer.
Care team member 11: Seeing it does bring it to your attention…Sometimes people only answer the questions they are asked, and if you don't know to ask the question, you will never get that answer.
Beyond visual alerts, care team members emphasized the need for detailed survey breakdowns to inform clinical action. A social worker noted this point.
Care team member 15: Going back to just like in the details, regardless of how you do the summary, at least in those details being able to know…what were the answers to this question so that we could kind of draw out and weed out what is the actual issue to address with the patient.
A nutritionist reinforced the importance of making social needs visible to all providers: “If those top social needs don't also kind of pop out, I don't know that a provider like a … physician or someone will really delve into that (Care team member 5).”
Incorporating live updates on patient food intake on the dashboard was considered difficult for the research team to execute. Social workers and dietitians wanted to keep social needs on the dashboard for physicians to review, which was moderately feasible for the research team to implement. Users valued displaying information about the types and number of units of insulin, which was considered difficult for the research team to deploy. Care team members also wanted to know which learning cards were deployed and their descriptions so the care team could have a conversation with the patient and reinforce the information sent by the system.
User experience
During the second part of our session, we focused on the facilitators and barriers the patient persona introduced in the video may encounter while using our proposed mHealth application. A care team member noted that patients would like the convenience of the mHealth application as it manages social needs, T2D, and pregnancy. Care team members highlighted that the digital solution would empower patients, providing an extra layer of support. Care team members raised concerns about ensuring patients have a smartphone with internet to access the mHealth application. Additionally, they were concerned about patients not engaging with the mHealth application. They feared that patients may need motivation to complete tasks or health goals in the mHealth application. These insights were confirmed during interviews with patient participants, who mentioned that features to encourage engagement would be helpful for using the mHealth application. Patient participants saw the importance of goals and shared that the digital solution was easy to navigate. Some noted that the mHealth application's checklist features encouraged patients to discuss their T2D management with their care team. Patient participants noted that notifications, if not too often, would be helpful for the mHealth application. The resources available on the learning cards were considered useful, particularly for patients who need social needs assistance.
Our built personas were based on the feedback from patients and care team participants about the proto-persona presented during our sessions. The refined personas represent different types of patients: (1) the “hands off” patient, (2) the “overwhelmed but trying” patient, and (3) the “engaged” patient. Each persona reflects different levels of the SCT constructs: knowledge and beliefs; skills; and self-efficacy, and important considerations with how a patient may engage with specific components of the applications. Briefly, the “hands off” patient has basic skills for managing T2D and pregnancy. They may face obstacles that lower their confidence and struggle to make connections between diabetes and their overall health. The “overwhelmed but trying” patient shows signs of confidence and may encounter some challenges. They strive to do what is best for the baby, but cannot make clear connections between T2D and their overall health. Despite being overwhelmed, they try to have a positive attitude and be engaged. The “engaged” patient is confident and can manage obstacles. They understand the importance of managing their T2D and overall health. They have a positive attitude and are motivated to adopt healthy behaviors. These personas were used to personalize content for different types of users and tailor features within the mHealth application prototype. We identified exemplary quotes that represent each persona in Table 4. We also provide implications for use of the applications by each persona, as well as salient features from the applications to augment each persona's engagement with the applications to enhance their self-efficacy, knowledge and beliefs, and skills associated with their T2D and pregnancy.
ACHIEVE patient personas developed based on social cognitive theory.

Clinical workflow integration
We developed clinical and social needs responses for the reference-based validation study using the features identified during affinity diagramming. We found differences in how participants and guides used the prototypes based on the validation study. Participants were more concerned about comprehensiveness, as they selected a wide range of relevant responses for each scenario. In three out of five scenarios, at least two participants selected more responses than the guides. This also suggests that the guides were more concerned with efficiency. There were also differences between the participants with regard to responses selected (mean range between 12 and 17, out of a possible 18 responses, selected across all scenarios).
We assessed the variability in the number of responses selected across different roles by calculating the IQR of the deviation from the mean for each scenario. We first compared responses between the guides and the participants, and then computed the IQR among the three participants. We found similarities between both analyses. Care team members had higher concordance for the scenario based on a “hands off” patient and the lowest concordance for an “engaged” patient scenario. Scenario 5 (“engaged” patient) had the widest IQR of 6.5, which indicates the most discordance across guides and participants. Scenario 4 (“overwhelmed but trying” patient) had the second largest IQR of 2.5 across guides and participants. Scenario 1 (“hands off” patient) had the smallest IQR of 1.5, comparing guides and participants. We also computed the IQR among the three participants. The largest IQRs were for Scenario 5 (“engaged” patient) and Scenario 3 (“engaged” patient), respectively, indicating the most discordance among the three participants. The smallest IQR was for Scenario 1 (“hands off” patient), indicating the highest concordance among the three participants.
We found varying levels of concordance by response type between the guides and participants. Across all five scenarios, goal setting was the only response with 100% concordance between the guides and the participants. The response with the second highest concordance (87%) across all five scenarios was referral to set up an appointment with a diabetes nurse educator. The response with the highest discordance (60%) was referral to the Supplemental Nutrition Program for women, infants, and children (WIC) across all five scenarios. The response with the second-highest discordance (53%) was connecting patients with a CHW to discuss social needs. Responses focused on social needs such as sharing a list of neighborhood resources (e.g., transportation, food pantry, paying bills) and journaling social needs had low concordance (27% or lower).
Table 5 provides the average proficiency and efficiency percentages and respective standard deviations for the three diabetes nurse educators in each patient scenario. The participants had lower proficiency and efficiency in Scenarios 3 (“engaged” patient) and 5 (“engaged” patient). This suggests that there is variation in our proposed use for patients who manage their T2D with fewer obstacles. The participants were the most proficient and efficient in Scenarios 1 (“hands off” patient) and 2 (“overwhelmed but trying” patient). This indicates less variation in our proposed use among guides and participants for patients facing challenges managing their T2D and overall health. We also calculated the average proficiency and efficiency percentages across the five patient scenarios. The average proficiency score was 40%, and the average efficiency score was 37%.
Average proficiency and efficiency scores and standard deviations of three diabetes nurse educators for each scenario.

Note: Scores of diabetes nurse educators were compared to two physician guides. Proficiency allowed us to determine if selected responses were consistent with the guides. Efficiency provided insight into whether necessary responses were deliberately selected. Proficiency was calculated by dividing the algebraic sum of the participant's score by the algebraic sum of the guides. Efficiency was measured by dividing the algebraic sum of the participant's score by the total number of selected responses by the participant for each patient scenario. Mean (SD) reported in each cell.
Discussion
We described the development of the ACHEIVE multi-component digital intervention to address clinical and social needs among publicly insured pregnant individuals living with T2D and unmet social needs. The most desirable features for our proposed patient mHealth application involved the ability for patients to share CGM-based glucose information with their care team, allowing users to set reminders and goals, and providing access to social needs resources through an integrated and single electronic platform. For the care team dashboard, features requested by participants were risk levels for social needs, the ability to see patient survey responses, and the ability to view type and weekly short and long insulin doses. The research team leveraged participant input to create three patient personas: “hands off,” “overwhelmed but trying,” and “engaged.” These personas were used to create patient scenarios to assess how well the content and features of the ACHIEVE digital intervention would address the needs of many patient types. Care team members selected clinical and social needs recommendations for different scenarios, and we found that participants and guides behaved differently, with participants selecting more responses while guides were more selective. Findings from this activity indicated a need to further refine our intervention and role expectations to improve end-user proficiency and efficiency when using the digital solution. Moreover, we also discovered that managing unmet social needs was challenging within the context of clinical workflow integration based on our reference-based validation study.
Our findings have implications for the existing evidence base on the use of digital tools in diabetes care and managing social needs. Patel and colleagues tested a randomized controlled intervention to address unmet social needs among adults with diabetes and found no statistically significant improvements in clinical outcomes; the researchers underscored the importance of intervention design to ensure impact on health outcomes. 29 In pregnancy-specific contexts, Leblalta and colleagues demonstrated through a systematic review and meta-analysis that digital health interventions for gestational diabetes improved glycemic control and self-management behaviors, particularly when they included personalized feedback and provider communication—features echoed in ACHIEVE. 30 Similarly, Kirkwood and colleagues highlighted in a qualitative study that pregnant individuals with gestational diabetes prioritized integrated tools combining clinical monitoring, resource navigation, and educational support, and that design should account for varied levels of user engagement—consistent with ACHIEVE's persona-based approach. Taken together, these studies suggest that user-centered digital interventions such as ACHIEVE are well-positioned for rigorous evaluation, particularly in understudied populations such as pregnant individuals with type 2 diabetes. 31
Most of the features recommended by patients and providers were incorporated, but not all due to feasibility and value to the user, including the ability to connect to other patients or to receive social support. It is important to consider both the needs of patients and care team members and the capabilities of the designers when developing mHealth applications.32,33 Because key stakeholders may have different interests, considering the different users and technical possibilities is necessary to produce the most acceptable final product. 34 The patient recommendations that were not incorporated were not consistently rated the highest value features, and were either deemed “unwise” or “big bets” in our prioritization matrix. Future iterations of the intervention could add more features once the main priorities are incorporated. The differences in proficiency and efficiency identified in our workflow integration evaluation indicated the need for an intervention manual and training to close the gap between care team members and their use of the intervention across various scenarios.
Prior research regarding telehealth devices has indicated a lack of user-centered design and non-intuitive use, highlighting the importance of early development of digital solutions with end-user feedback. 35 There may be a disconnect between end-user desires and what developers can do, and digital solutions that do not incorporate end-user input may only focus on the feasibility and simplicity of features.35,36 The end-users in our study are pregnant individuals with T2D, and IT developers may not have successfully related to the context in which their work will be used. Designing without user and task analyses in this study would risk producing a product that ignores accessibility requirements and user-preferred features. 37 The concept of dominant logic, defined as ‘a mindset or a worldview or conceptualization of the business and the administrative tools to accomplish goals and make decisions in that business is often used in economics and technology settings to describe how businesses perform. 38 In technology development, differences in dominant logic between developers, those marketing a product, and end-users may lead to differences in the design process. 39 For example, IT teams might focus on technical novelty and feasibility factors that may result in misalignment between prototypes and user expectations. Developers need to focus on the desires and preferences of the customers to better prioritize features based on their context. 40 Our study provides a means through which this delicate balance may be achieved to solve a complex healthcare problem. We also utilized a User-Centered Advisory panel that was composed of members from multiple stakeholder groups to help reconcile tensions that arose during our study activities.
Over 90% of individuals in the USA use smartphones, and over 95% of those under 50 years old. 41 We have previously demonstrated that this statistic is similar for Medicaid-insured pregnant individuals with unmet social needs. 10 There are thousands of mHealth applications that are tailored to specific health conditions and purport to improve health and self-management behaviors. 42 Pregnancy apps have been shown to improve weight management, knowledge about pregnancy, adherence to prenatal care, and gestational diabetes control.14,43–45 Despite these benefits, many pregnant individuals report using multiple applications because of different desirable features on each application and few applications are comprehensive enough for all of their concerns.43,46,47 In the current study, patients reported similar barriers to using only one application, and many only used pregnancy applications that did not address social needs or diabetes. This mHealth application was developed to help this specific population with their complex self-management needs by providing a wide range of functions recommended by patients with similar needs to the intended end-users. This evidence-based approach signifies an opportunity for patients to be better informed about their care needs and have personalized discussions with their care team members. 5
Limitations
Our research should be interpreted in the context of some limitations. Participants were recruited from the same clinic, and their opinions may not be generalizable to other clinical settings. Albeit our institution engages with a wide range of patients from diverse backgrounds as a tertiary care academic medical center, who experience complex health and social needs. Our prototype mHealth and dashboard applications did not have all of the proposed features incorporated at the time of the interviews, so participants were not responding to the final multi-component intervention currently being tested in an RCT. We did not have the ability to collect feedback about the mHealth application and dashboard use over time and continued engagement. We plan to continue to measure the usability and acceptability of our multi-component digital solution as it is adopted in the ongoing ACHIEVE RCT. We also recognize that additional workflow integration challenges may arise during the RCT and this may form the basis of a subsequent study that will lay the foundation for a knowledge base for effective implementation of digital solutions across diverse community settings.
Conclusion
We conducted usability sessions on a high-fidelity prototype of a multi-component digital solution that supports pregnant individuals with T2D, poor glycemic control, and unmet social needs with potential participants and healthcare providers. During these sessions, we assessed interface usability, user experience, and clinical workflow integration of our prototypes through think-aloud sessions, empathy map activities, affinity diagramming, IBM prioritization matrices, and a reference-based validation study. We also developed patient personas for our digital solution. The prototypes received positive feedback for the current features and additional desirable features were recommended and prioritized based on value to patients and technical constraints. Our future work will address the sustainability of these components and features.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261423982 - Supplemental material for Usability, user experience, and workflow readiness of a digital health solution for publicly insured pregnant individuals living with type 2 diabetes
Supplemental material, sj-docx-1-dhj-10.1177_20552076261423982 for Usability, user experience, and workflow readiness of a digital health solution for publicly insured pregnant individuals living with type 2 diabetes by Naleef Fareed, Christine Swoboda, Yiting Wang, Joshua J Joseph and Kartik K Venkatesh in DIGITAL HEALTH
Footnotes
Ethical approval
This work was approved by the Institutional Review Board of the Ohio State University (IRB2022H0399). Patients and providers provided verbal consent to participate in this study. The IRB granted a waiver of written documentation of consent because the study posed minimal risk to participants, involved no procedures for which written consent is normally required outside of the research context, and collecting signed consent forms would have created unnecessary participant burden and potential privacy concerns.
Contributorship
NF conceived the study. CS, YW, JJJ, KKV, and NF contributed to the writing of the manuscript. KKV and NF were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Department of Biomedical Informatics, The Ohio State University, and the Agency for Healthcare Research and Quality (R01HS028822).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
NF
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.