
Abstract
Background
A tailored and integrated technology solution (patient mHealth application and provider dashboard) can provide a 360° view of Medicaid-enrolled patients with type 2 diabetes (T2D) during pregnancy that could improve health outcomes and address health inequities.
Objectives
To develop a set of user specifications for the mHealth and dashboard applications, develop prototypes based on user needs, and collect initial impressions of the prototypes to subsequently develop refined tools that are ready for deployment.
Methods
Study activities followed a double-diamond framework with a participatory design mindset. Activities were divided into two phases focused on a qualitative inquiry about participant needs and values (phase 1) and design, development, and usability testing of low and high-fidelity prototypes (phase 2).
Results
We identified themes that exemplified pregnancy experience among Medicaid-enrolled individuals with T2D. Patients (n = 7) and providers (n = 7) expressed a core set of expectations for the mHealth and dashboard applications. Participants provided feedback to improve the mHealth and dashboard. For both applications, participants reported scores for the NASA Task load Survey (TLX) that were in the 20th percentile of national TLX scores.
Conclusions
Digital health tools have the ability to transform health care among Medicaid-enrolled patients with T2D during pregnancy, with the goal of managing their blood glucose levels, which is a precursor to experiencing a successful pregnancy and birth. Distilling patient and provider needs and preferences—then using them, along with prior studies and theory, to develop applications—holds great potential in tackling complicated health care issues.
Introduction
Type 2 diabetes (T2D) affects nearly 100,000 pregnant individuals in the United States every year.1,2 The prevalence of T2D is expected to double in the next decade, putting a greater number of mothers and infants at risk for diabetes-related complications in pregnancy. 3 In parallel, the prevalence of T2D has doubled among pregnant individuals of low socioeconomic status (SES). 4 Over 50% of pregnant individuals with T2D are enrolled in Medicaid and are of low SES.5,6
Diabetes management in pregnancy requires strict glycemic control, which necessitates lifestyle adjustments, glucose monitoring, and pharmacotherapy over a relatively short duration of time. 7 Suboptimal glycemic control results in adverse maternal and fetal outcomes, including preeclampsia, birth trauma, severe maternal morbidity, NICU admission, neonatal hypoglycemia, fetal growth abnormalities, and stillbirth. 8 Clinical care alone is not sufficient and social determinants of health (SDoH) can have a significant influence on health outcomes. 9 SDoH are conditions in which people are born, grow, live, work, and age, and they include factors such as insurance status and SES, which is consistently a strong predictor for diabetes onset and progression.9,10 SDoH impact the ability of Medicaid-enrolled pregnant individuals with T2D to achieve glycemic control, including lack of reliable transportation to attend visits, access to healthy diet and exercise resources, and convenient methods to log self-monitored glucose values and adjust insulin dosing.11–18 Limited education and income may further exacerbate barriers to care for Medicaid-enrolled individuals with T2D who are unable to engage in activities that achieve glycemic control. 19 When social needs are not met, T2D management may become increasingly difficult.4,20–22 This is concerning because recent data regardless of diabetes status have documented higher rates of adverse pregnancy-related outcomes among individuals on Medicaid compared to those with commercial insurance.11,23 These findings highlight the need for interventions that are tailored to Medicaid-enrolled pregnant individuals with chronic comorbid conditions, including T2D.
Evidence suggests that current models of maternity care are inconsistent with patient preferences regarding diabetes management and interaction with their care providers. 24 Pervasive technology such as mHealth and Internet of Things wearables present several opportunities for fostering pregnancy care management. 25 Nearly 75% of pregnant individuals reported downloading at least one mHealth app, and a majority of them indicated that they are likely to use them once per week.26,27 Over 90% of women of reproductive age are smartphone users, including those on Medicaid. 28 Existing research indicates the willingness of pregnant individuals to use digital tools for health management.29,30
Stand-alone mHealth applications have demonstrated benefits for diabetes management among non-pregnant individuals, but the potential of mHealth among pregnant individuals has yet to be fully realized. 21 A recent study comparing performances of pregnancy-related diabetes management mHealth apps indicated that existing apps perform well in areas of education and information, but only a few provided comprehensive evidence-based educational content, tracking tools, and the ability to integrate meaningfully with electronic health record systems. 21 Applications that are comprehensive, personalized, and integrated within care team workflows are likely to be more effective, 21 increase patient uptake, 31 sustain patient and provider behavior change over time, 32 and demonstrate long-term sustainability. 31 Existing diabetes-related mHealth apps also fail to capture SDoH and address specific patient needs. Current prenatal and diabetes care delivery for Medicaid-enrolled pregnant individuals is fragmented. 11 Furthermore, the current health system lacks a multi-faceted intervention that incorporates tools at both patient and provider end to facilitate patient-provider communication and provide a 360° view of patients’ pregnancy experience.
Provider-facing, bi-directional dashboards can provide comprehensive diabetes information to care teams, including timely clinical alerts about glycemic control, psychosocial issues, and treatment plans 33 ; facilitate team-based provider coaching and feedback 34 including recognizing patient beliefs, values, and readiness for change; and help with behavioral modification.35,36 Outside of pregnancy such an approach has improved glycemic control 37 and adherence to evidence-based diabetes care. 33 Based on the existing evidence, our study team was motivated to explore a platform that capitalizes on the integration of a mHealth app and dashboard technology to provide a comprehensive, tailored, and team-based solution that addresses clinical management and social needs among Medicaid-enrolled pregnant individuals with T2D.
Our objective is to describe a formative study that developed an integrated patient-based mHealth and provider dashboard application system for management among Medicaid-enrolled pregnant individuals with T2D. Our goals were to: (1) develop a set of user specifications for the mHealth and dashboard applications; (2) develop prototypes based on user needs; and (3) collect initial impressions of the prototypes to subsequently develop refined tools that are ready for deployment.
Methods
The double-diamond framework
Our study activities followed the “double diamond” framework, a user-centered approach widely used in information technology development. Figure 1 shows the roadmap of our design framework starting with a diagnosis phase followed by four sequential double-diamond phases: discover, define, develop, and deliver. 38 Our study utilizes the double diamond process to (a) define problems faced by Medicaid-enrolled individuals and their providers for effective diabetes management during pregnancy, (b) develop prototypes of our mHealth and dashboard applications, and (c) elicit reactions from users with regards to usability and acceptance.

ACHIEVE pilot study activities through the lens of a double diamond framework and participatory mindset.
The shape of the double diamond figure signifies the process of collecting divergent insights during discovery and subsequently translating these insights into concepts by convergence and definition. 39 This conceptual framework has been successfully used for complex health care problems.40,41 For example, Asbjørnsen et al. designed an eHealth intervention that aimed to support behavior change for long-term weight loss maintenance in the general population. 39 We complemented our double diamond framework thought process with a participatory design mindset and included system requirements generated by end users to ensure that expectations for the final product were met. 42 The section that follows describes each of the double diamond phases as they pertain to our study.
Diagnose
As a first step, three members of our research team (EB, AL, and GO) conducted a scoping review of the literature for key problems and existing gaps related to diabetes management in pregnant individuals. Our research focused on two domains: health disparities due to clinical and non-clinical factors and technology use. Both areas focused on populations that are at risk, minority, and public health insurance. We examined various sources, including peer-reviewed articles and registered clinical trials, for scientific evidence. Significant findings were reported on our study Miro board for reference and discussed as a team, which included gaining input from our clinician investigator (KV) for validation from a health care provider perspective.
Phase I
Discover (formative interviews)
The problems identified in the diagnosis phase were further studied in our target population by means of a pilot study. Our team conducted individual interviews to identify current structural and process barriers, as well as practices associated with the management of diabetes among Medicaid-enrolled patients. We conducted separate interviews with patients and their providers at our Division of Maternal Fetal Medicine (MFM). Interviews examined three areas of interest: (a) current workflows for standard of perinatal and postpartum care; (b) current workflows and processes for collection of SDoH-related information and (c) participants’ needs in regard to the design an mHealth application (for patients) or dashboard (for providers) for diabetes management during pregnancy. All study activities were approved by our Institutional Review Board.
Study sample
Patient Recruitment. Patients were recruited from the Diabetes in Pregnancy Program within the division of Maternal Fetal Medicine. Inclusion criteria included patients who were pregnant, had T2D, were covered by Medicaid insurance and were able to speak English. We excluded patients who were not 18 years of age or older. A convenience sample was identified and eligible patients were recruited and consented to by a study team member. Each patient received a $50 gift card at the end of the study (after completing both phases) as an incentive for participation.
Provider recruitment. Criteria for provider inclusion required physicians, nurses, diabetes nurse educators, and nurse assistants to be involved in the care of pregnant patients with diabetes. Providers were recruited from the Diabetes in Pregnancy program. A convenience sample was identified and consented to by a study team member. Each non-physician provider received a $50 gift card at the end of both study phases as an incentive for participation.
Semi-structured Interviews. Patient and provider interviews lasted 60 minutes, were audio recorded, and were transcribed verbatim. Our research team conducted the interviews using semi-structured guides to explore patient and provider experiences. These guides were developed by the research design team, pilot-tested on two patients and two providers, and refined based on the provided feedback. The patient interview guide included four key sections: patient background (including gestational age, challenges, and changes since pregnancy), management of pregestational diabetes (experiences and challenges following healthcare recommendations), information on SDoH (whether access to resources was discussed with providers and how they were addressed), and desired features and content in an mHealth application for diabetes management during pregnancy. Similarly, the provider interview guides included four sections: provider background (care team roles, typical experiences providing care for expecting women), treatment of pregestational diabetes (usual care, characteristics of patients, and challenges providing care), information on SDoH (what information is collected, how they are addressed), and desired features and content in a dashboard for diabetes management during pregnancy. The interviews were conducted via the online platform Zoom or the telephone. Primary interviewers were female in their early to mid-30s and secondary interviewers included two males between ages 30 and 40. All interviewers were English speaking; however, factors such as cultural differences and prior experiences with pregnancy may have brought bias to the work. The research team discussed after every interview whether new or interesting themes emerged, and there was a consensus that was achieved to signify the theoretical sufficiency of our themes. Details of our study following the COREQ guidelines 43 are provided in the supplementary table (Table S1).
Define (Data analysis). This phase consisted of thematically organizing patient and provider interviews by means of open coding. Interviews were analyzed inductively to categorize our findings and reveal emergent themes. 44 Three team members (EB, YW, and NF) reviewed at least 20% of each transcript, and two members (PS and NF) reviewed the entire transcripts independently to identify emergent themes. These two members met frequently to ensure consistency of coding and agreement about definitions of new codes as they emerged during the coding process, consistent with the grounded theory approach. 45 A third researcher team member (RS) independently reviewed the thematic codes and reconciled any differences. Information from our literature review and thematic analyses, in consort with the fundamental constructs of social cognitive theory (SCT),46,47 was used to develop elements that formed high-level specifications for the mHealth and dashboard prototypes. Microsoft Word was used to analyze quotes and STATA 17SE was used to analyze all quantitative data for the study.
Phase II
Develop (prototype design and development). We designed numerous low-fidelity prototypes in the form of paper and pencil sketches to visually explore features based on the key themes identified from the phase I interviews. Many components, features, and interactions represented in the low-fidelity prototypes were then used to inspire the creation of high-fidelity clickable prototypes in Figma for the mHealth and dashboard applications. The features were designed to be user-centered, engaging, and driven by the SCT approach to motivate specific behavioral activities among patients to lower their Hemoglobin A1c (A1c) through effective management of blood glucose and social needs during pregnancy. We concurrently developed an initial infrastructure architecture to demonstrate the integration of the applications via a digital platform with a defined ecosystem within which patients and their providers would engage with the system and communicate with each other.
Deliver (usability assessment). In the final phase of our pilot study, we used the high-fidelity clickable prototypes developed in Figma of the mHealth and dashboard based on the feedback provided by study participants and our user experience design team. Key features present in the initial low-fidelity prototypes, though not intended to be comprehensive, represented a core set of functions that would promote behavioral modifications as guided by the principles of SCT. Following the approach undertaken by Yardley et al., our research team met multiple times over the course of several weeks to plan, prioritize, and highlight prototype features that were crucial. 48
We conducted the Phase II interviews with the corresponding prototypes to obtain feedback from the users who participated in our Phase I interviews. We conducted usability testing and think-aloud sessions with patients and providers. The aim of these interviews was to systematically collect feedback about the prototypes using a deductive approach based on our prior work on decision support tools where we categorized identified themes into one of three categories: (1) function, issues that are related to meaningful and intuitive navigation of an application; (2) content, problems with information provided in an application that complicates or leads to misinterpretation of information; and (3) aesthetics, concerns that impede an application from having a minimalist design that effectively communicates information.49,50
Usability (UX) and think-aloud. At the time of the interview, each participant was asked to perform a predetermined set of tasks with no time limit. Participants were requested to complete tasks (e.g. inputting blood glucose values for a specific time of day, setting up a new appointment, and reviewing a goals card). Participant actions and spoken-aloud thoughts during the usability session were recorded for further analysis. Participants were asked to share their experiences with the application and usability of the product. Our team documented challenges to the use of prototypes and completion of prespecified tasks as a list of recommendations by function, category, or aesthetic.
Cognitive workload survey (WLS). Upon the completion of the usability assessment, participants were asked to respond to questions assessing mental, physical, and temporal demands; frustration levels; overall performance; and effort required to complete the usability assessment in the WLS made available through Qualtrics. The questions in the WLS survey involved the items from the validated NASA Task Load Survey (TLX). 51
Feedback from the survey and interviews will be used to develop the final version of the mHealth and dashboard applications.
Results
Patient characteristics
We recruited seven patients and seven providers in our study. All patients and providers completed Phase I, and three patients (42%) and four providers (57%) completed Phase II.
The primary reasons for loss to follow-up were because of time commitments, lack of childcare for an interview, and health reasons for patients (a majority of these patients were past their first trimester of pregnancy), and time commitments were also a challenge for providers given the challenges of factors such as the COVID-19 pandemic.
Characteristics of our study samples are provided in Tables 1 and 2. Most of the patients identified as non-Hispanic Black, had two previous pregnancies (gravida), and had a mean age of 29. Among our provider sample, we recruited four physicians and three registered nurses.
Characteristics of patient sample (n = 7).

Characteristics of provider sample (n = 7).

Diagnosis phase
Problem. Pregnant individuals on public insurance with T2D are 50–80% more likely to have elevated A1c levels and experience adverse birth outcomes, which result from dysglycemia early in pregnancy, compared to their counterparts with private insurance.11,52 Over 40% of U.S. pregnant individuals receive prenatal care through public insurance. 53 While early and sustained prenatal care improves maternal and neonatal outcomes for T2D,54,55 pregnant individuals on public insurance encounter numerous barriers that preclude appropriate and timely prenatal care.14,56 Based on the Determinants of Health Model, clinical care alone for this population is not sufficient, and SDoH influences health outcomes. 16 Social needs such as food security, adequate housing, a safe environment, and access to medications and health care, influence health outcomes and glycemic control. 16 When social needs are not met, T2D management, including achieving glycemic control, becomes increasingly difficult.9,20
Intervention. Our team proposed an intervention to address social needs among Medicaid-enrolled individuals with poorly controlled T2D during pregnancy. Pregnant individuals are interested in engaging in alternative prenatal care models 57 that can mitigate health and social disparities. 56 In addition, a linked provider dashboard can facilitate better decision-making and regular contact between patients and providers, and improve patient outcomes. 58 The value of mHealth apps for health-based interventions in diabetes outside of pregnancy has been demonstrated.37,59 Mobile health apps result in lower A1c levels, improved healthcare utilization, better patient-reported outcomes (PROs),60–63 and improved post-intervention engagement and diabetes outcomes. 64 Due to the underlying health inequities and the willingness of our study pregnant population to adopt digital health technology, our team proposed to use mHealth and provider dashboard applications to mitigate existing disparities. 29 In this study, we provide the rationale and process used to develop our initial prototypes.
Phase I
Discover. When asked about their pregnancy experiences, patients indicated common thoughts about a constant feeling of tiredness, adherence to a new regimen, preparation for the pregnancy, and the need for resources. Their pregnancy journeys included several lifestyle modifications, barriers, and experiences, and these experiences were captured by our interviews.
Managing exhaustion. When describing their pregnancy experiences, patients frequently reported feelings of constant exhaustion, especially those with older children or employed. Patient 2 shared: “So, we're always staying active, just because young ones keep you busy, but once I come home, I always feel so exhausted, and I try to like sometimes force myself to go for a walk.”
Adherence to a new regimen. Patients reported having to be more aware of their health status and willing to adapt to new health regimens, including greater reporting of blood glucose levels, food intake, and physical activities. However, these added measures were perceived as demanding: Patient 1 noted: I’m taking my medicine better. Before I really wasn't taking my insulin like that, and now I’m really taking it, taking it better, checking my sugars way more like they asked me to. It's really tedious, oh my gosh, it's so tedious.
Preparing for pregnancy. Patients reported the need to prepare for their pregnancy and the importance of having support that would be critical to maternal and infant care, especially during the early stages of infant life, as well as financial security. Patient 5 highlighted: “I feel like I'm more aware of things, like I’m gonna have to take care of somebody else and making sure I’ve got time, money and resources to do that.” They also mentioned: I try to plan ahead more than I did. I was, before you called, I was sitting down and writing out a budget, which I've never really had to do before. Just to make sure that I would have enough.
Resources to manage SDoH. Many patients mentioned that during their visits, their social needs were not actively discussed in detail. Some mothers requested to be enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Patient 3, for instance, mentioned about WIC that their providers “normally had the pamphlets and stuff for all that.” The patient indicated the importance of these resources because of the frequency of interacting with WIC, “well, a lot because I get WIC monthly so I’m constantly checking everything.” Patient 1 recognized the additional barriers faced by individuals with diabetes to access affordable health care resources: “I know a lot of people that don’t have health care that can’t afford to take in their diabetic stuff.” Access to resources was also qualified by the type of resources and the importance of closing the loop. For example, Patient 5 indicated regarding her mental health that providers gave her a “brochure or something” and “They called me, but they haven’t called me back for the appointment,” and “I looked at it wasn’t helpful.”
Patient-reported needs and preferences in an mHealth application. Patients expressed a core set of expectations for an mHealth application that involved features to offer electronically captured and management of information, access to support systems, use of diabetes technology, and help through problem-solving and personalized recommendations.
Electronic capture and management of information. Our results indicated the emerging need to include an electronic feature to capture blood glucose levels. Existing processes included recording blood glucose levels in the form of paper logs and sending them to the providers by email or by fax, which was perceived as being cumbersome. Patient 4 shared: something that can keep track of my, my sugar records. That would be nice, instead of having to write everything down and then send it on through email. It would be awesome just to have it on the app. That would definitely be a plus.
In addition to capturing FSBG values, patients expressed the need to include a feature that captured details about their dietary intake and out-of-range values with means for providing open-ended responses. For example, Patient 4 mentioned: it'd be nice to have like a schedule of like your, when you're supposed to check your sugars and then being able to write down what your sugar was that day and then even going to the extent of what did you eat and explain why your sugar is that low or that high. I think that would be awesome.
Support system. Patients suggested the need to include a feature that allows them to communicate with other individuals for support and learning from their experience. Patient 4 said: What they eat [support group] is a good one because I get bored with the same old food so it'd be nice to know what other people are eating that's been able to maintain their sugar. What they do, as far as exercise to where they don't overdo it, but I know walking is a good one, but that would actually be something nice to know what other people is doing to maintain their weight and everything during, especially having diabetes during pregnancy.
Diabetes technology. The availability of innovative technology for diabetes management has been rapidly increasing. Patients expressed interest in the use of such technologies, especially continuous glucose monitoring (CGM) devices. Patient 4 expressed interest in using CGM: I do think one idea would be awesome would be having a monitor, which I know they have them out there, but for pregnant women … that is actually you're able to check it like it's inserted in you. I forget what it's called, but I know they have some on that out there, but it’d be awesome if they can actually get one approved for pregnant women, to make it so much easier on them. The scanner that I use is on my phone. I don’t have to have like an additional piece of equipment…I downloaded the app and just scan my arm from there, I don’t have to, you don’t have an extra piece of equipment, so it just makes it easier for them to get the numbers from directly from the app.
Problem-solving and personalized recommendation. Pregnancy is a unique experience for every patient and requires guidance that accounts for specific challenges faced by a pregnant individual. Patients reported the need for direction on how to actively plan activities and meals that aligned with effective blood glucose management. Patient 1 mentioned: Maybe like suggestions for different things like they want me to eat three meals and three snacks and there is no way I can keep all that down half the time, so maybe like suggestions or like what could be a snack and things like that and meal suggestions cause you don’t want me eating carbs and go easy on the sugar.
Provider-reported needs and preferences in a dashboard application. Providers indicated a general set of expectations for a dashboard application including features such as dynamic and actionable data, tools to capture unmet social needs, and enhanced patient–provider communication.
Data that is dynamic and actionable. Most physicians expressed the need for electronic and standardized means to capture blood glucose data. Typically, providers receive blood glucose values through email and paper logs brought to a clinical encounter. Provider 2 acknowledged the value of having a more comprehensive story about their patient at their fingertips: “Estimated fetal weight, the gestational age of the patient, the dosing of the insulin or metformin they’re on, if I could have all that information, I could do a lot of this work within the app.” Another provider, Provider 3, noted the importance of a user-friendly application: Right, um, obviously there, there are a lot of systems now available for displaying, for instance, blood glucose levels to providers. I’ll start there, and I’ll say that in my opinion, most of them do not represent user friendly displays. And an incredible amount of data is collected in some of these systems. Yet it's not user friendly to the practitioner, especially in pregnancy, where decisions are made week to week, if not even more frequently with regard to changes in insulin dosage.
Tools to capture unmet social needs. Providers expressed that there was no standard procedure to capture unmet social needs information. Provider 3 noted: You know where there are, is some, albeit skeletal social work support and what have you, but I'm not sure that that's uniform with them …. I think that when that becomes very apparent is when an individual woman indicates that you know, resources are an issue for her in terms of doing glucose testing in terms of obtaining medication including insulin and then that comes to a head pretty quickly, and then we have to do some problem solving. Often patients are the best, I mean, they know if they’re exposed to smoke or if they have access to healthy food or you know what kind of safe neighborhood or lack thereof, they live in, or if they're able to get exercise and whatnot. So rather than having the providers sit there and ask these questions and put the data in I wonder at some level if this can be data that the patient themselves directly enters via an app and then that populated in the dashboard and then the provider is simply reviewing that data or embellishing it or correcting it in the sense that you know they’re not entering it all, and the patient has done the hard work, because the patient knows that stuff best and then the provider is simply reviewing that data, but that it gets entered in a systematic way that you can see it.
Provider 4 indicated the value of an application that can recommend resources to patients: In our clinic and McCampbell we have one or two social workers and we're seeing hundreds of patients. You know, every day we're seeing enormous numbers of patients. In our diabetes clinic on Tuesday we have you know 25 to 35 prenatal visits for our patients with diabetes … the real challenge is, is access to our social workers and that the app may be able to provide a more accessible resource for our patients if they can look at the app and say where can I get healthy food, where can I obtain my medical supplies, how do I arrange transportation to the clinic. Having a way to stay in direct communication, making it as easy as possible for the patient in terms of communicating with the team accessing information about her diabetes management, glucose control, diet would really, I think, be helpful. The more the patient understands the challenges, the better partnership can be established.
Define. Upon review of the transcripts, our team identified problems and possibilities faced by our patient population. Three study members operationalized important concepts onto the Miro board following pre-defined color codes (i.e. orange—keywords, yellow—general summaries/insights, blue—ideas for prototyping, pink—barriers, azure—manual processes, and violet—analysis/decisions) (see appendix figures S1–S4). The study members worked collaboratively to manually sort notes into clusters of similar functional areas (e.g. communication, glucose management). This was conducted for both the patient mHealth and provider dashboard applications. Study team members further synthesized information into high-level user specification maps (Figure 2) to translate the user requirements into an actionable development plan, highlighting the essential functions and their subthemes for each application. This process also facilitated forming the structure of how the mHealth and dashboard applications would achieve information exchange.
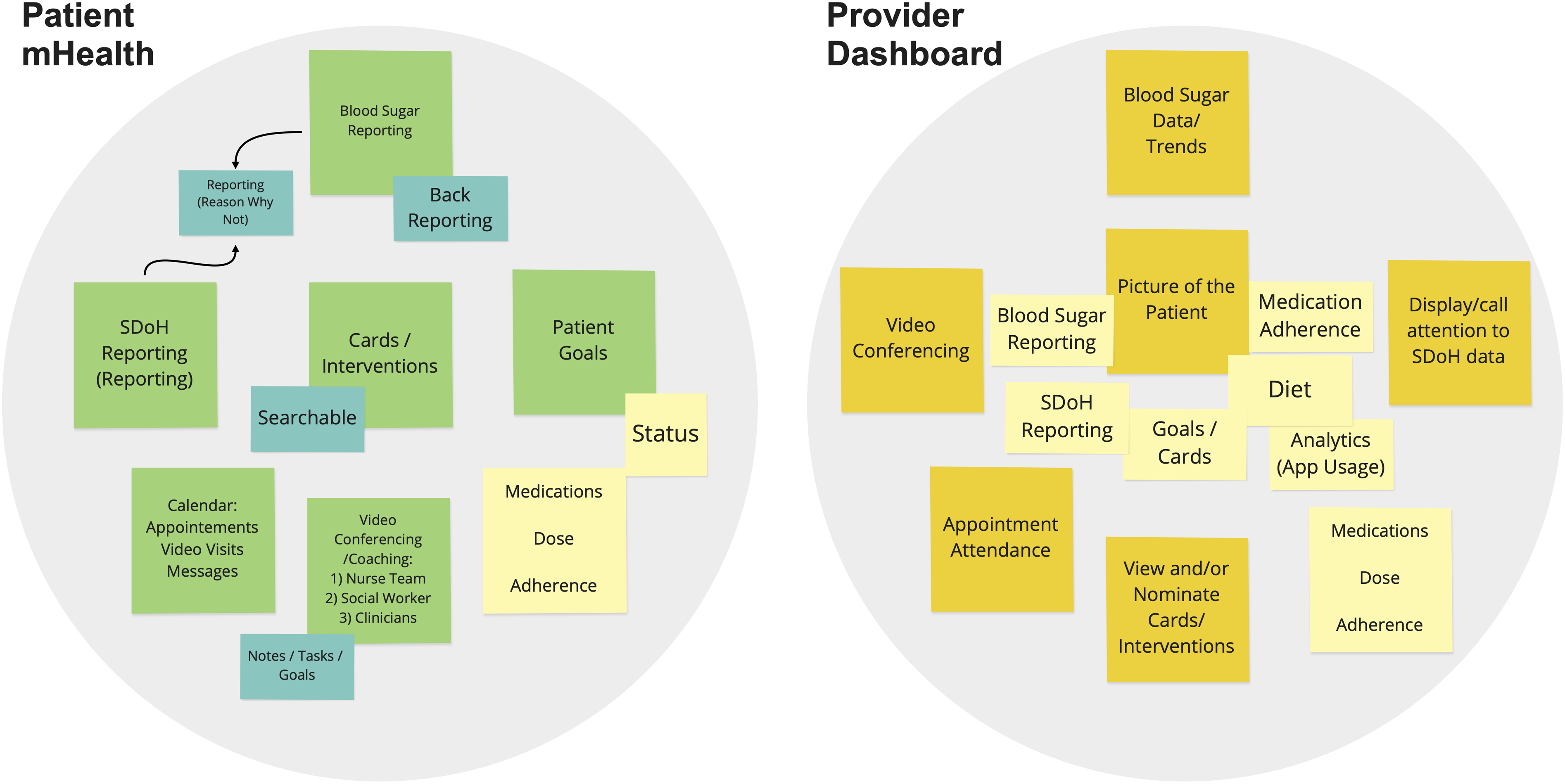
Initial user specifications for mhealth and dashboard applications.
The mHealth app is centered on the reporting and management of blood glucose values and social needs. Customized patient goals and care pathway cards (clinical and social needs-oriented activities that would help patients achieve their specific goals) were included as primary features, along with other essential elements such as a calendar, video conferencing with the provider team, and medication information. The dashboard focused on showing the trend of a patient's glycemic control, social needs information, and other critical vitals (e.g. gestational age, other medications) that would present a 360° view of the patient. Providers would also use the dashboard to monitor patient activity, actively communicate with them, and tailor their care pathways based on the feedback gathered about a patient from the system.
Phase II
Develop. We continued further analysis of the interview data using swim lane diagrams. A swim lane diagram represents how different roles perform their tasks, take on their responsibilities, and interact with others along a timeline, which generates a holistic view of the system to help identify gaps and discover intervention opportunities. We used the diagram to map out the current clinical workflow based on the journey of a Medicaid-enrolled patient with T2D during pregnancy (Figure 3) and developed an improved clinical workflow with the engagement of the applications (Figure 4).

Swim lane of “as-is” clinical workflow (figured scaled to illustrate complexity of the system).

Swim lane of “to-be” clinical workflow with ACHIEVE tools.
In the “as-is” clinical workflow (Figure 3), five roles (1-Pregnant T2D Patients, 2-OB/GYN or MFM provider, 3-Diabetes Nurse Educator, 4-Physician, and 5-Community Health Worker) are presented in lanes with distinguished colors, followed with the actions taken from a patient's perinatal period through their post-partum period. The arrows and lines indicate the flow of interaction. We used color-coded notes to capture findings in the workflow, which include issues/barriers, possible features, questions, analysis/decision points, and follow-up questions. During this activity, a variety of gaps were revealed. Major gaps included: (1) the patient's adherence to their goals, care plan, and medication regimen; (2) the communication and information exchange between the patient and the provider, also among members of the care team; and (3) the need to address barriers to social needs occurring throughout pregnancy.
Based on the study results from Phase I and our additional analyses, our design team designed high-fidelity prototypes for the mHealth app and dashboard. With features reflecting patient- and provider-generated requirements with the goal of achieving relevance through a useable, useful, and desirable product. 65 Figure 5 displays the mHealth application prototype with five pages that cover critical domains identified for the application. Figure 6 displays the provider dashboard prototype with patient page displayed. Both prototypes were used for our usability testing.

Mhealth application prototype. The app contains a to-do list for the patient providing an overview of their tasks for the day as well as the ability to report outcomes, track their glucose levels, manage and learn about their care pathways, and track their goal achievements over time.

Dashboard application prototype. The dashboard presents patient profiles, scheduling information, and options to communicate with the patient or provider; tracks the patient's A1c, proportion of time in the target range for glucose level, goal achievement, and social needs; and offers notification messages about the patient's health status and care pathway selections for the patient given their specific patient-reported outcome responses.
Deliver. We conducted usability assessments of the mHealth and dashboard applications with patient and provider participants, respectively. We synthesized and categorized feedback from participants and their actions into the content, function, and aesthetics domains based on the application tested (Tables 3 and 4).
Patient feedback and recommendations for the mHealth prototype.

Provider feedback and recommendations for the dashboard prototype

Unweighted patient and provider TLX scores.

Task load survey. Workload measurements such as the TLX provides a general sense of how tasks related to the use of a tool are experienced. Overall TLX unweighted scores reported were 33 for both the mHealth and dashboard application, which translated to the 20th percentile of a national review of studies that used the TLX across multiple technologies (overall mean score = 42 and health care median score = 45). For the mHealth application, this score was driven primarily by relatively low temporal and frustration scores; albeit, patients expressed some concerns about the performance demands (possibly due to the lack of initial training to input data). The TLX score for the dashboard was driven primarily by low physical and temporal scores, with equally moderate concerns raised about mental and performance demands. Reweighted scores for both TLX measures indicated improvements, with a higher difference for the dashboard. The reweighted measure reallocated a total weighting of 15 points across four of the five domains (mental = 4; performance = 3; effort = 2; frustration = 3; physical = 0) as recommended by Hertzum et al. based on the study of similar technologies reported in the literature (Table 4). 66
Discussion
Stand-alone mHealth applications for diabetes management in pregnant individuals exist, but only few are comprehensive and integrated, and none are tailored to meet the needs of those on Medicaid. 21 We leveraged findings from existing studies to design an integrated approach for Medicaid-enrolled individuals with T2D during pregnancy that provides a comprehensive, tailored, and team-based solution addressing clinical management and social needs using themes identified through prior research, behavioral theory, and our qualitative work. Our intervention brings together multiple technologies in an integrative framework to gain a 360° view of a T2D patient's pregnancy experience more effectively and be responsive to that information regarding clinical, social, and supportive care.
Principal findings
We identified three themes that exemplified the pregnancy experience among Medicaid-enrolled individuals with T2D: managing exhaustion, adherence to a new regimen, and preparing for pregnancy. Exhaustion and fatigue are among the commonly reported feelings of pregnancy that may exacerbate a chronic comorbid condition, such as diabetes. 67 During pregnancy with diabetes, specific lifestyle adjustments are recommended over a short period of time. 7 Individuals with T2D who were previously on oral pharmacotherapy or diet-based therapy now generally require insulin to achieve glucose control using strict parameters, including upwards of 4 daily FSBG,68,69 and patients are challenged to learn to regulate both the quantity and quality of carbohydrate consumption while simultaneously adopting new medication use and exercise behaviors. The strict medication and dietary requirements and increased home-based activities such as glucose monitoring and reporting escalate the burden of disease management contributing to pregnancy fatigue. Moreover, multiparous women taking care of older children may face additional barriers that compound this preexisting exhaustion.
Diabetes in pregnancy requires economic and social stability. T2D management in pregnancy is expensive, with more than $7000 in excess pregnancy-related costs and individuals often report financial planning as part of diabetes management strategy. 70 Likewise, social support is equally important for good quality of life during pregnancy and requires planning in the earlier stages. The associated disease novelty, especially among nulliparous women living with T2D, and dynamic physiological and clinical changes require preparation for upcoming lifestyle demands.71,72
Participants expressed needs and preferences in a mHealth application that were represented by five themes: electronically captured and management of information, access to support systems, use of diabetes technology, help through problem solving, and personalized recommendations. The most desired feature in an mHealth application, by both patients and providers, was the ability to electronically capture blood glucose data. Pregnant individuals with diabetes often find it cumbersome to manually record, save, and communicate their glucose values with their care team providers. An electronic platform with the ability to capture and communicate blood glucose values in a meaningful manner emerged as a desired feature by both patients and providers. As opposed to manual data entry, an mHealth application provides patients with the opportunities to experience streamlined and routinized data collection that requires less effort on their part. For example, use of a CGM device that syncs with a mHealth application with a user friendly interface may promote long-term use of the application and device. 73
User needs and preferences for T2D management during pregnancy. The interrelated themes we identified from patients and providers revealed specific end-user specifications that aligned with the theoretical underpinnings of SCT. SCT posited that successful performance of a behavior depends on an individual's behavioral capability as well as cognitive and environmental influences on behavior via three domains: (1) skills; (2) knowledge and beliefs; and (3) self-efficacy. 46 The themes identified from our qualitative work highlight the importance of these three domains specific to individuals with T2D during pregnancy. Individuals require educational information that clearly explains how behaviors and specific clinical and social needs pathways will help them achieve the primary outcome of glycemic control (knowledge and beliefs). Patients need skills and coaching to engage with the diabetes care team, which can be accomplished by collecting and synthesizing detailed information about the pregnant individual from the mHealth app to the provider dashboard to better communicate with the diabetes care team (skills). Team-based coaching based on CGM output, personalized information, and care pathways may help the pregnant individual learn more about T2D in pregnancy and better adhere to their T2D care regimen. Closing the loop (e.g. having a community health worker document the individual's successful securing of healthy food through a community food pantry) could ensure that an individual's new skills yield meaningful outcomes and enhance their confidence (self-efficacy).
Design requirements and refinements needed to meet end-user preferences and needs. Our research team recognized the importance of leveraging technology that is highly relevant to our study population and their providers. We utilized applications that did not require high costs to maintain in the long-term and were evidenced-based. Albeit, in our exploration of the evidence base for mHealth and provider dashboard applications tailored to similar populations, we quickly recognized the challenges faced in prior implementations of each application. 21 Specifically, these previous approaches to improving care for Medicaid-enrolled patients with diabetes have been siloed and fragmented. 11 We, therefore, identified an intervention that would-be systems-oriented and addressed the pitfalls associated with the use of each application by itself. We focused more on the gestalt effect of these applications and their ability to collectively transform health care by providing a comprehensive, 360° view of the patient using information that was dynamic and closed the loop between the provider and the patient (e.g. the provider will be aware that a patient completed an assigned care pathway).
Our analysis of the “as-is” and the “to-be” workflows identified major gaps critical to an ideal workflow: (1) patient adherence to their goals, care plan, and medication regiment; (2) the communication and information exchange between the patient and the provider, as well as among members of the care team; and (3) the need to address barriers to social needs occurring throughout the pregnancy. Our applications considered not just the clinical and psycho-social requirements for the patient, but also these realities in our clinical setting. We pursued a deeper understanding of the requirements of applications by testing them with patients and providers, and although initial impressions were highly positive (e.g. TLX scores for both applications were in the 20th percentile of national TLX scores across all devices), we obtained notable feedback that will be used to improve the content, function, and aesthetics of our applications before a full deployment. Our high scores on the TLX surveys for both our prototypes should also be highlighted because participants did not receive any pre-training to use the applications. This suggests the intuitiveness of our prototypes, especially the interfaces. The implications for such design performance may include reductions in cost and effort associated with training and greater engagement from individuals with lower technology literacy.
Implications and recommendations for future design and practice. A key consideration when it comes to the use of digital health tools is the reversal of newly established behaviors.74,75 Whether our approach—which is supported by prior studies, our own mixed-methods findings, and theory—results in long-term behavioral modifications is not demonstrable in this paper and requires further inquiry. A critical component of such an inquiry would involve gauging the cost-benefit ratio that individuals mentally construct in determining their desire to balance the use of our applications to manage blood glucose levels during their pregnancy. Relatedly, the timing of our intervention is another area of consideration, especially given our focus on pregnancy. Extending the use of our application before pregnancy (in preparation for pregnancy) and postpartum use (especially during the interconception period) could have implications for the successful management of blood glucose beyond the perinatal period.
Strengths and limitations
An important limitation of our study is that it is not tied to the evaluation of health outcomes. It reflects realistic perspectives of patients and providers whose behaviors and interactions could have an impact on health outcomes. Our study is also focused on a specific population during pregnancy and does not capture their views before and/or after pregnancy. Our study involves perspectives of patients and providers who are highly committed and engaged in the use of our applications, which may influence study findings. 76 Nonetheless, our team was able to gather both positive and negative impressions of the final prototypes. More work is required to obtain generalizable perspectives beyond our sample. The data we collected, albeit from small samples, was rich and the insights on our prototypes were detailed. A consensus about the sufficiency of themes emerged among the team based on our interview data for our small, in-depth study. Our approach to developing applications using a double-diamond framework with a participatory design mindset is generalizable and is already utilized in multiple domains beyond healthcare including government, finance, and insurance not to mention general consumer markets.
Conclusions
Digital health tools such as mHealth and dashboard applications have the ability to transform health care among Medicaid-enrolled patients with T2D during pregnancy, with the goal of managing their blood glucose levels, which is a precursor to experiencing a successful pregnancy and birth. Distilling patient and provider needs and preferences—then using them, along with prior studies and theory, to develop applications—holds great potential in tackling complicated health care issues. Engaging individuals such as those from our study population presented a unique set of challenges, and it was apparent to our team that system relevance throughout pregnancy was a critical success factor for our end users relative to all others, regardless of efficacy. The methods described in our study can be used as a template for future design considerations specific to the development of digital health interventions, including those focused on understudied populations.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221144181 - Supplemental material for Developing and testing an integrated patient mHealth and provider dashboard application system for type 2 diabetes management among Medicaid-enrolled pregnant individuals based on a user-centered approach: Mixed-methods study
Supplemental material, sj-docx-1-dhj-10.1177_20552076221144181 for Developing and testing an integrated patient mHealth and provider dashboard application system for type 2 diabetes management among Medicaid-enrolled pregnant individuals based on a user-centered approach: Mixed-methods study by Naleef Fareed, Christine Swoboda, Priti Singh, Emma Boettcher, Yiting Wang, Kartik Venkatesh and Robert Strouse in Digital Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This work was approved by the Institutional Review Board of The Ohio State University. Patients and providers provided consent to participate in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Department of Biomedical Informatics, The Ohio State University, Agency for Healthcare Research and Quality (grant number R01HS028822).
Guarantor
NF.
Contributorship
NF conceived the study. NF, CS, PS, EB, YW, RS, and KV contributed to the writing of the manuscript. NF, PS, EB, YW, and RS were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Peer review
The authors have chosen the individuals who reviewed this manuscript to remain anonymous.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.