
Abstract
Objective
The successful transition of a digital platform from a research institution to a government system in under-resourced environments necessitates effective cooperation among various stakeholders and a strong sense of responsibility from both the Malawi Ministry of Health (MoH) and all users. The article aims to describe the implementation and lessons learned in transitioning a maternal surveillance digital platform (MATSurvey) from a research-based to a government-owned system in Malawi.
Methods
The transition process involved active participation of the MoH leadership and close cooperation with healthcare workers and partners. The process comprised six stages, including stakeholder engagement, user feedback, system design, obtaining stakeholder input on the design, system development and testing, piloting and full implementation. The process emphasised stakeholder engagement, with technical teams from the MoH and Malawi Liverpool Wellcome Programme incorporating feedback during development.
Results
The successful transition of the MATSurvey platform from the Malawi Liverpool Wellcome Programme to the Digital Health Information System 2 tracker required strong leadership from the MoH, active engagement of partners and stakeholders, and a gradual, inclusive process. Challenges such as reliance on donor funding and delays in government support were notable, while ensuring clear data governance policies, system scalability, effective communication, and comprehensive training contributed to a smoother transition and successful adoption.
Conclusion
Transitioning of a digital health platform such as the MATSurvey platform requires strong leadership and supervision to ensure adoption, acceptance and ownership. The active involvement of MoH, partners and stakeholders accelerated transitioning of the platform despite challenges in funding, which ultimately resulted in delaying the process.
Introduction
The integration of digital healthcare into national systems has been acknowledged as a pathway to attaining sustainable development goals (SDGs) by enhancing access to, quality and affordability of healthcare services. 1 The global health strategy on digital health 2020–2025 aligns with the SDG of communication technology development and global interconnectedness, which has the potential to improve human lives, increase knowledge, and close the digital health gap. 2 Governments worldwide are prioritising high-quality digital services in healthcare, where implementation requires many stakeholders, with the government playing a central role. 3 One notable domain for digitalisation focuses on maternal and newborn health, specifically in the context of remote obstetric monitoring, where the objective is to tackle the challenges faced and reduce mortality rates.1,2 Government support enables the digital health platforms to scale up operations, reaching a larger population and ensuring the sustainability of the initiative over time for improving health outcomes.4,5 This is effective, however, if integrated into a functional local system that ensures sustainability with technical assistance and support from stakeholders.4,6,7
Malawi has the goal of moving towards universal health coverage (UHC) with digital health at the centre of achieving this goal. 8 Improved digital health service delivery requires not only the development of an appropriate platform, but also a change in the mindset of users to make the most of the technologies. 5 The maternal and newborn health surveillance platform (MATSurvey), a digital system created in Malawi for real-time data collection on the impact of emerging diseases on maternal and newborn health outcomes, near-miss incidents, maternal deaths, and quality of care indicators, 9 can prove highly efficient when implemented correctly within the government structure. The platform, which was developed by Malawi Liverpool Wellcome Programme (MLW) and Malawi Ministry of Health (MoH) during the period of the COVID-19 pandemic to capture real-time data, was adapted from a paper-based system. It has been used by the MoH and stakeholders for reporting maternal and newborn health indicators, including research. The MATSurvey platform adheres to a government-established framework for data collection, with safe motherhood coordinators (selected health care workers at district and central hospitals responsible for ensuring the health of women and their newborns is improved) serving as the primary data collectors. Reports are transmitted from the district level to the national level in real time. Nevertheless, while the government fully owns the data, the digital, real-time platform received wholistic support from MLW, hence the decision to have its technical aspects and functionalities transitioned into the government system for sustainability. The platform is composed of five data collection forms built on Open Data Kit (ODK), such as the enrolment forms (maternal death, near-miss and COVID-19 reporting forms); weekly facility outcome form; maternal death audit form; Near-miss audit form; and COVID-19 and near-miss daily follow-up forms. MLW initially managed system analytics and dashboard visualisation using the paid Zoho Analytics platform, which offered advanced functionality but raised concerns regarding long-term sustainability within government systems that prioritise low-cost, locally managed outputs.
To ensure long-term sustainability, stakeholders involved in maternal and newborn health within the MoH reached a consensus to incorporate the MATSurvey digital health platform into the reporting and supervision frameworks of Maternal and Perinatal Death Surveillance and Response (MPDSR) within the government structure, additionally transitioning it into the District Health Information Software 2 (DHIS2) tracker. The DHIS2, widely adopted in low and middle-income countries (LMICs), including Malawi, serves as a platform for health information analysis and reporting aggregated data. 9 It has features that enable immediate dissemination of disease outbreaks, improvement of data collection tools and facilitation of interoperability. 10 The DHIS2 tracker is an extension of the DHIS2, enabling the collection of disaggregated data such as daily case follow-ups.10,11 Although anticipation was that the resulting DHIS2 dashboards would differ in appearance and offer fewer advanced features than the Zoho version, this represented a deliberate trade-off between technical functionality and long-term operational sustainability by MoH. Evidence highlights the significance of incorporating various expertise, partnerships, and advocacy over transitioning donor-funded initiatives into governance frameworks to ensure long-term sustainability.5,7 Nevertheless, it is essential to acknowledge the obstacles associated with donor dependency during both the transition and post-transition periods. 7
This implementation and lessons paper outlines transitioning of the MATSurvey platform to the Malawi MoH system, DHIS2 tracker. The article discusses the six collaborative steps among stakeholders, highlighting successes, obstacles and insights gained concerning the technical aspects and functionalities of the platform in Malawi. This knowledge is valuable for streamlining the transition of similar programs from research institutions to government platforms in low-resource settings.
Methods
Methodological framework
An implementation and learning process approach was used, focusing on the real-world deployment of the digital health platform with ongoing monitoring and adaptation. Lessons learned were documented to identify operational challenges and inform research gaps related to transitioning platforms from research institutions to government management.
Design and population
The transition process, an implementation and learning process approach, involved moving a national digital health platform used for collecting maternal and newborn health data from the research institution to the government system and did not recruit any participants. The process began with the initial planning involving collaborations between MLW and MoH directorates such as the Reproductive Health Directorate (RHD), Quality Management Directorate (QMD), Digital Health Department (DHD) and the Central Monitoring and Evaluation Division (CMED). Table 1 describes institutional positions and roles of the MoH directorates and units that were involved in the transition of the MATSurvey platform. The directorates and departments were prioritised in the process due to their crucial roles in monitoring and improving maternal and newborn health outcomes, as well as ensuring the government's digital health system meets current data management requirements. The transitioning of the platform from a donor-funded research institution to the government-recommended DHIS2 tracker aimed to secure the sustainability and accountability of real-time maternal and newborn health data by the MoH's RHD and QMD.
Ministry of Health units involved in the transition of the maternal and newborn health surveillance platform (MATSurvey), including institutional positions and roles.

Timeline and implementation site
The transition process began on 15 November 2021 and was completed on 31 March 2025. This transition took place in Malawi, where MLW served as the research institution responsible for the design and hosting of the Matsurvey platform, and the MoH served as the lead authority and recipient of the platform.
Selection of management and technical teams for the transition process
To ensure smooth transitioning of the platform from MLW data management and systems to MoH systems, technicalities and functionalities of the platform were discussed with stakeholders who included RHD, QMD, DHD, CMED, health care workers, zone managers, academic representation as well as maternal and newborn health main partners to the MoH such as United Nations Fund for Population (UNFPA), World Health Organisation (WHO), Deutsche Gesellschaft Für Internationale Zusammenarbeit (GIZ), MOMENTUM 1 and 2, Newborn Essential Solutions and Technologies (NEST 360) and Africa Medical and Research Foundation (AMREF). The MATSurvey technical and functional aspects requiring transitioning and strengthening are outlined in Figure 1.

MATSurvey technicalities and functionalities for transitioning into the DHIS2 tracker and strengthening within the MoH system.
Technical considerations for platform transition
The DHIS2 tracker was the preferred platform to accommodate disaggregated data from the MATSurvey platform. The MATSurvey platform operated through an ODK Collect, a data collection tool capable of gathering data even without a network connection, and a paying analysis platform referred to as ZOHO analytics.
The MATSurvey technical considerations primarily focused on the functionalities governing data collection, analysis, and presentation. The design of data collection forms was tailored to align with ODK Collect, ensuring smooth data flow for analysis and presentation. Built-in mechanisms for ensuring data accuracy and quality, including integration of skip patterns, were added as applicable. Various dashboards, including trends in maternal mortality ratio, case characteristics, and newborn health outcomes, were developed based on consensus within the group, with access granted to authorised individuals by RHD. Data collection was carried out using tablets, which MLW data managers and coordinators could remotely access for error correction and system upgrades. The functional aspects centred on the system's operation, encompassing data collection and supervision, feedback mechanisms, follow-up procedures, registration, and ongoing training and support for healthcare workers and supervisors regarding system navigation. It was decided that MoH, led by RHD and QMD, would assume the roles previously held by MLW while CMED and DHD would oversee data management and security, including server maintenance. Stakeholders would actively participate in the transition process to ensure a favourable outcome.
The transition steps
To ensure the long-term viability of the MATSurvey platform within the operational framework of the healthcare system in Malawi, the MoH and MLW designed and agreed on six steps for the transition of the platform's technical aspects and functionalities into the DHIS2 tracker. Supplemental Table S1 describes the transition steps indicators that were derived, which inform the outcomes of the transition process.
Figure 2 illustrates the steps taken for the transition process of the platform into the DHIS2 tracker.

Steps undertaken for the transition of the MATSurvey from the MLW system to the DHIS2 tracker.
Step 1: Stakeholder engagement: Familiarisation with the system to determine the transition process
For sustainability and ownership of the platform, a high-level team from the MoH proposed the establishment of a steering committee comprising members from various departments, such as the MoH directorates, including RHD, QMD, DHD, and CMED and research institutions such as the KUHeS Obstetrics and Gynecology Department (KUHeS OB-GYN), and MLW (Table 2). The committee would examine the necessity of transitioning the platform to the DHIS2 tracker, particularly due to its collection of sensitive real-time maternal and newborn health data owned by the MoH. This data could be accessed and visualised at any moment, highlighting the importance for the MoH to safeguard and effectively manage it for informed decision-making across district, zone, and national levels. Additionally, attention would be given to MLW's status as a research institution, with projects having limited lifespans that could impact the utilisation and administration of data after the project phase concludes. Additional meetings would be arranged involving technical teams from district hospitals to the national level to achieve a deeper grasp of the platform's technical aspects and features that required transition. The DHD system developers were to be provided with data collection forms definitions and the platform's system design specifications to enable designing and development of the tracker. Documentation of the platform's functional components was going to be shared with the MoH leadership to guarantee its long-term viability. The MoH would coordinate all meetings, lead issue resolution, and ensure stakeholder alignment through regular virtual and stakeholder meetings.
Composition of the steering committee and technical team from the Ministry of Health.

Step 2: Feedback from users of the MATSurvey platform
A meeting was organised, supported by MLW, where a total of 70 RHD, QMD, CMED, DHD, and safe motherhood and quality improvement coordinators, zone coordinators, and managers extensively deliberated on the data collection forms employed in the platform. Figure 3 describes the data collection forms used for the MATSurvey platform.

The maternal and newborn health surveillance platform (MATSurvey) data collection forms.
Suggestions were made to enhance the system, improve user-friendliness, and ensure sustainability. The team examined the forms and recommended adjustments to the weekly facility, enrolment, COVID-19 daily and near-miss daily follow-up, maternal death audit, and near-miss case audit forms, which compose the MATSurvey platform. The newly developed neonatal audit form by the MoH was reviewed during discussions, with proposed modifications, before its integration into the MATSurvey platform within the DHIS2 tracker. All agreed recommendations (Table 3) were incorporated into the platform.
MATSurvey data collecting forms feedback from stakeholders.

MATSurvey: maternal and newborn health surveillance platform; DHIS2: District Health Information Software 2.
Step 3: System designing
The MoH's CMED and DHD data management teams, including those of MLW and Momentum 1, transformed the data collection forms into a format compatible with the DHIS2 tracker (Supplemental Figure S1). The current system was structured into three segments: functions, MATSurvey processes, and analytics. This segmented approach was used to ensure that all the elements of the current system are seamlessly integrated into the DHIS2 tracker. The function segment focused on the primary purposes and tasks that the system is designed to perform. Process segments detailed the step-by-step actions, algorithms, and workflows that drove the system's operations. The analytics segment dealt with the interpretation and utilisation of the data collected or processed by the system. The team devised the data flow and integration of forms within this system framework. Factors such as performance, scalability, security, reliability, and user-friendliness, based on the technical details and functionalities provided, were put into consideration during the designing (Supplemental Figure S1). The design incorporated connections between forms within the system, with the dashboard serving as an outcome display. It depicted the enrolment of eligible women on the platform, with data analysis and representation on the dashboard. The design specified the recipients of notifications regarding any maternal death enrolments, while authorised stakeholders were granted access to download the desired dashboard.
Step 4: Stakeholder feedback on the system design
The MoH engaged with stakeholders, including partners and the technical teams from district hospitals and zone-level management (Supplemental Table S2). Groups of five to seven members from different institutions were formulated with four key aspects of discussion: data quality and management, data usage, capacity building and responsibilities, and materials and resources. They discussed the system's functions and technical aspects and addressed system-related challenges and potential solutions. Input from stakeholders regarding the system design led to the development of strategies to oversee the system and ensure its long-term viability. This meeting highlighted recommendations and processes over the transition phase to ensure the effectiveness of the platform and sustainability (Figure 4).
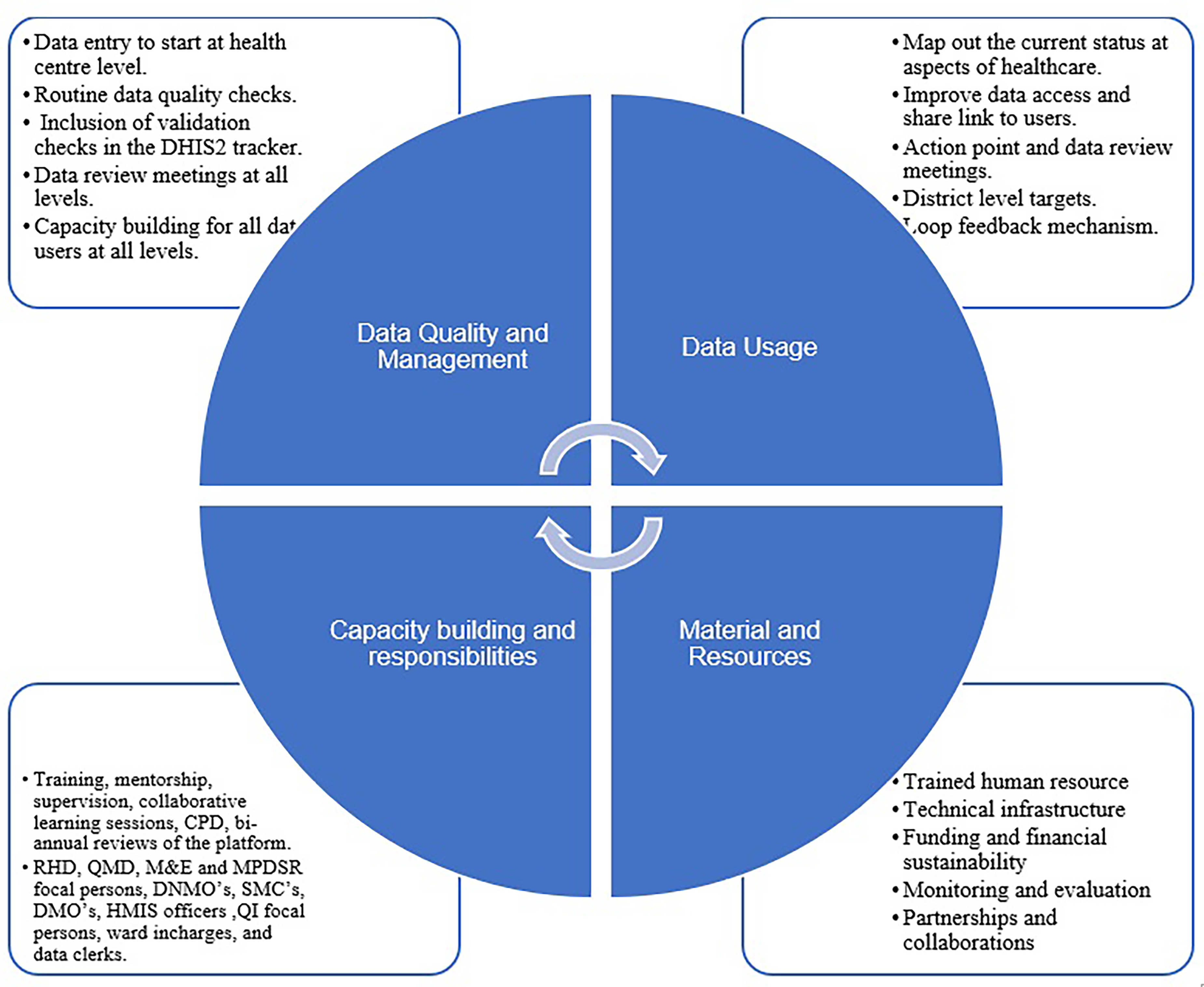
Stakeholders' recommendations on the maternal and newborn health surveillance platform’s (MATSurvey) design and sustainability.
Step 5: System development and testing
The phase allowed for the integration of the Matsurvey system into the DHIS2 tracker while taking stakeholder feedback into account. Matsurvey adopted the moniker MPDSR platform in the DHIS2 tracker, incorporating all technological features. With technical expertise, data elements were created and imported into the tracker with the inclusion of in-built patterns to allow users to navigate the platform. The development was conducted by DHD, CMED, and MLW experienced technical teams (Table 4). Sub-groups were created to work on the data collection forms: (a) weekly aggregate form, (b) enrolment form, (c) daily follow-up, (d) near miss audit, (e) death audit, and (f) facility audit form. All teams had the responsibility of creating import files in Excel for the data elements associated with their specific forms. This task included defining and organising the data elements, maintaining data consistency. The import files were prepared, based on the existing data collection forms, but in line with the DHIS2 tracker data element standards, while ensuring a seamless integration of the data elements into the DHIS2 tracker. Special consideration was given to mapping data elements to their respective categories and datasets, aiming to guarantee data integrity and accuracy within the system.
System development technical team.

DHIS2: District Health Information Software 2.
System configuration and user manual development
The objectives for system configuration and user manual development were to review the DHIS2 tracker system parameters and create an end-user handbook for the DHIS2 tracker application. The configuration phase included reviewing the requirements of the system, identifying data items, mapping the workflow and improving the process, as well as practical configuration and testing exercises. The configuration's overarching objective was to maximise the system's efficacy and efficiency.
A perinatal death audit (PDA) form was to be incorporated as one of the data collection forms to match with MPDSR data elements in the DHIS2 tracker system. A project strategy and timeframe for numerous additional configuration-related action items were developed to address them in order. A task force made up of Momentum 1 technical staff, MLW data manager, and digital health personnel was established to work on all areas that were suggested for change and provide input weekly until the tasks were completed. Senior staff from Momentum 1 and representatives from KUHeS and RHD served as the task force's supervisors. The list of participants along with their roles and duties towards the transition of the MATSurvey platform to the DHIS2 tracker is highlighted in Supplemental Table S3.
System testing
A follow-up testing of the system was implemented. With recommendations from RHD, QMD, and KUHeS selected partners and stakeholders, such as MLW, members of the academia, and health care workers (Table 5) were tasked to test the platform's usability in the DHIS2 tracker. The criteria for selecting the system testers included familiarity with the MATSurvey platform, data entry experience in the platform, data utilisation and analysis from the platform, and feedback and communication abilities of the users. A set of instructions on how to navigate the platform was sent along with the links to activate access to the DHIS2 tracker. A checklist of what to be checked and provide feedback for was sent to individual testers, and a deadline for submitting feedback was indicated. The focus of the system testing was to guarantee user-friendliness, data accuracy, comprehensible system processes, and suitable data presentation. The phase highlighted navigation of the data collection forms, data element flows, notification requirements and dashboard reflection.
MATSurvey platform system testers.
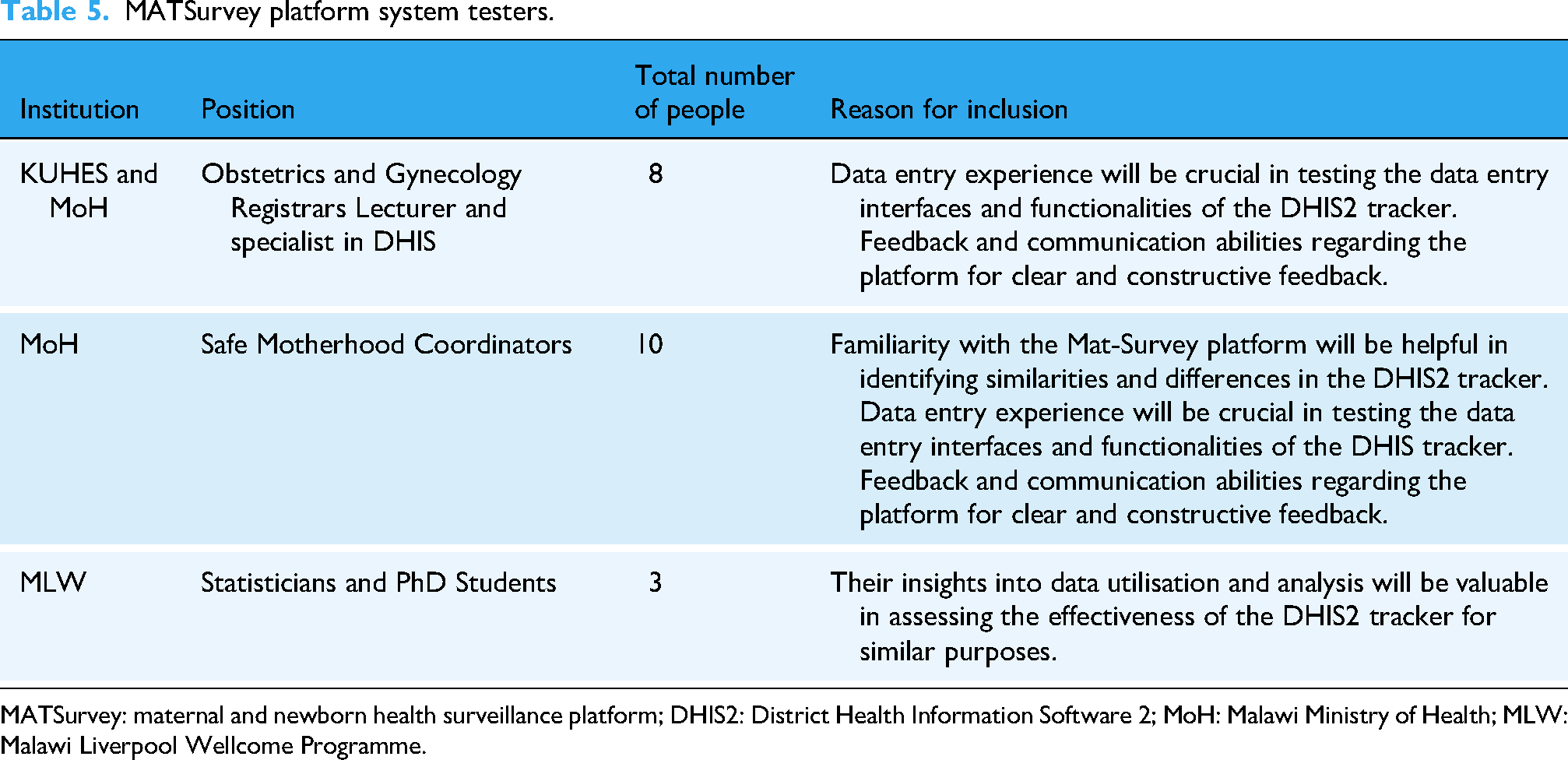
MATSurvey: maternal and newborn health surveillance platform; DHIS2: District Health Information Software 2; MoH: Malawi Ministry of Health; MLW: Malawi Liverpool Wellcome Programme.
The checklist helped reduce confusion and misinterpretation during this phase because testers knew exactly what to look for and what kind of input was expected. Additionally, it made sure that every part of the system was thoroughly tested, guaranteeing that no important features or functionalities were missed. Furthermore, by ensuring consistency in the input, the checklists helped to minimise unpredictability and subjective interpretations. Most significantly, by concentrating on particulars, it expedited the testing procedure and saved time and resources. The checklist also assisted in locating flaws and potential development areas, resulting in a digital health information system of higher calibre.
Indicator and dashboard configuration sessions for small and sick neonate (SSN) and MPDSR
This phase involved stakeholders working in diverse groups to configure indicators for both MPDSR and SSN as main components of the DHIS2 tracker. The process conducted, which included seven steps, has been described in Supplemental Figure S2.
Step 6: MPDSR platform in the DHIS2 tracker piloting, refinement of the system and training
This phase included a random selection of two facilities for piloting the system. The selected facilities included Dowa and Mzimba district hospitals from the central and northern regions. The district hospitals, which provide secondary-level care to the local population, offer a range of medical services which include maternal and child health care. Like many district hospitals in Malawi, the selected district hospitals serve to address the health needs of the surrounding communities; however, facing challenges such as limited resources and high patient demand. The technical team and leadership from MoH, comprising of District Medical Officers (DMO), District Nursing Officers (DNO), SMC's, RHD, QMD, DHD, CMED, Momentum 1, and NEST360 and stakeholders were involved in the piloting of the platform. The exercise involved gathering insights from both the existing MATSurvey platform and the MATSurvey platform within the DHIS2 tracker. A 3-month pilot phase for implementing the MATSurvey platform at district hospitals (from January to March 2025) was set to enable further adjustments and improvements. After this phase, the platform would be rolled out to the rest of the districts. Refresher training over the platform was scheduled for Safe Motherhood Coordinators and HMIS officers from all districts in Malawi to ensure the platform's sustainability.
Results
Stakeholder engagement
A national multi-sectoral steering committee was formally established by the MoH. The committee formally approved the migration of the MATSurvey platform from the MLW environment to the national DHIS2 tracker to strengthen government ownership, data security, and long-term sustainability. A total of 70 national stakeholders participated in structured consultations on the MATSurvey platform, reflecting full (100%) representation across relevant technical, clinical, and management cadres. Stakeholder engagement was sustained across all phases of system transition. Stakeholder feedback directly informed revisions to system architecture, data collection forms, dashboards, and workflows.
System design and configuration outcomes
All core system design documents were completed, including finalised system architecture, workflow diagrams, and data integration pathways. The redesigned system was structured into three integrated components: system functions, technical processes, and analytics, ensuring compatibility with the DHIS2 tracker environment. System configuration was completed across seven core data collection modules. All required data elements, indicators, and metadata were standardised and imported in accordance with the DHIS2 tracker requirements. Configuration validation confirmed no critical functional gaps prior to piloting.
System testing outcomes
All planned system test domains were executed, including data entry, workflow navigation, notification functionality, security validation, and dashboard performance. Testing identified data accuracy discrepancies primarily related to form configuration errors, as well as challenges with complex indicator configuration and limited search functionality. Performance and scalability assessments demonstrated that the system could support multiple concurrent users with short response times, although minor bottlenecks were observed in data aggregation and report generation. Data security and privacy testing confirmed compliance with DHIS2 standards, access controls, and encryption requirements. All critical configuration-related errors identified during system testing were corrected prior to pilot implementation, and system refinements were incorporated to improve usability and data integrity. Figure 5 illustrates some of the feedback from the system testers.

Feedback from system testers demonstrating accuracy, user experience, data security and privacy, and performance and scalability.
Indicator and dashboard configuration
The workshop resulted in the successful configuration of SSN and MPDSR indicators within the DHIS2 tracker system. Stakeholders completed indicator mapping, validation, and dashboard development following a structured seven-step configuration process. The resulting dashboards supported real-time visualisation of enrolment, audits, and outcome trends.
Piloting outcomes
The MPDSR platform was piloted in two district hospitals representing 100% of the targeted pilot sites. The pilot confirmed the functional integration of modules within the DHIS2 tracker. During piloting, a skip-pattern configuration error was identified and successfully corrected. Dashboard and real-time notification configuration were deferred for post-pilot refinement following MoH guidance. The pilot demonstrated the operational feasibility of the platform at the district level and informed final refinements prior to national rollout.
Refinement and system improvement
All major issues identified during testing and piloting were formally resolved prior to scale-up. Version updates and configuration adjustments were applied across all system modules, ensuring consistency, reliability, and improved user experience.
Training and national readiness
National refresher training was conducted for Safe Motherhood Coordinators and HMIS Officers from all districts in Malawi, achieving full national district representation. Post-training assessments confirmed that participants achieved functional competency for routine system use, supporting the platform's readiness for long-term sustainability.
Discussion
Given that governments are playing a central role in advancing high-quality digital health services which requires the involvement of many stakeholders, 3 it is evident especially in low-resource settings that successful transition of digital health platforms depend on continued donor support, strong technical guidance from the MoH, active stakeholder engagement, and robust leadership3,12 from both the MoH and the institutions from which the digital health platforms are being transitioned. Partner involvement from organisations, as well as healthcare professionals and all pertinent departments of the MoH, ensured active engagement and the integration of practical ideas for sustaining the platform both during and after the transition phase in Malawi. Nevertheless, stakeholders’ engagement throughout the transition phases provided support, comprehension of system functionalities and technical aspects, and integration of feedback to create a user-friendly platform accessible to all. Their involvement also facilitated cost-sharing across the transition stages, guaranteeing the platform's successful transition as anticipated. The joint endeavour aimed to secure complete ownership of the platform by the MoH while ensuring its sustainability. 13
Despite the successful execution of every step of the transition process, the platform's transition took more time than expected. Delay stemmed from challenges encountered by the MoH in obtaining funding for the process, with unavailable budgets for the transition process, a common finding with other studies, 13 compounded by various priorities from different departments within the MoH that were involved in the process. Transitioning digital health platforms into the local government systems requires the allocation of financial and human resources to ensure that the digital platform receives the necessary support to operate efficiently and effectively.7,14 Prioritisation of limited resources for essential health care activities in low-resource settings has proven challenging.15–17 In Malawi, underfunding is a major obstacle in health governance. 18 Underfunding leads to the government's continued reliance on donor support, even for maintaining platforms like the MATSurvey platform, which are crucial for improving healthcare outcomes. A study conducted in eastern Uganda, examining the impact of HIV services following the transition from donor support to local systems, revealed that many services experienced a reduction in implementation unless they continued to receive donor support. 19 This illustrates the significant role donor aid plays in sustaining programs in LMICs where governments rely heavily on external support for resources. The MoH coordinated donor funds for transitioning of the MATSurvey platform with constant communication with MLW.
Studies in low-income countries highlight how interventions have failed or lacked emphasis and sustainability without stakeholder perspectives.20,21 This is significant as it underscores the influence stakeholders have in decision-making regarding healthcare interventions, as well as the sustainability of these interventions in LMICs. A study conducted in Mozambique emphasised the critical role of stakeholder engagement during the early stages of transitioning a donor-funded intervention, noting that its absence leads to challenges throughout the process. 22 Another study highlighted that the involvement of various stakeholders with common interests is crucial for successfully transitioning digital health programs, despite the challenges that may arise. 16 Early and continuous engagement of stakeholders from the outset of the transition phase, as has been asserted for previously, 23 facilitated their support and involvement, even when delays occurred due to competing stakeholder priorities.
The emphasis of transitioning the MATSurvey platform to the government structures was consistently placed on elucidating the steps involved with a clear focus on both the process and its long-term outcomes (Supplemental Figure S3). The MATSurvey transition process outlined the post-transition phase, specifying how the government would assume full ownership of the platform and detailing the implementation process. Operating within a government framework can equally enhance public trust and confidence in the digital health platform, as it demonstrates accountability, transparency, and reliability in the delivery of healthcare services.
The numerous sensitisation, planning and progress workshops held with stakeholders at national as well as technical levels cement what has been previously asserted that workshops conducted at various stages of the transition process are essential for fostering sustainability and ensuring local structures take ownership of the platforms. 24 The stakeholders emphasised the necessity for the platform to be widely accessible to interested parties. However, concerns over the sensitivity of the data and the need for maximum security were raised. The recommendation was to have RHD responsible for authorising access to the platform. Advancements in digital health platforms have introduced new security and privacy risks to patients’ health data, making the protection of confidentiality, integrity, and availability (CIA) essential to safeguard sensitive information in the healthcare sector. 25 The RHD supported by the QMD guaranteed appropriate integration of the digital health platform into the national healthcare infrastructure, enabling improved coordination and information exchange across different levels of care, as demonstrated by other studies showing its effectiveness. 26
Due to insufficient funds to support healthcare activities, governments primarily rely on cost-effective methods for managing services. 18 The migration from the proprietary Zoho Analytics platform to the free DHIS2 visualisation capabilities was a necessary step to promote fiscal sustainability. While this shift resulted in noticeable differences in dashboard appearance and functionality, it did not hinder the ability of key MoH stakeholders, including RHD and QMD, to interpret data or make informed decisions. Although the DHIS2 tracker dashboards offered more limited visualisation features compared with Zoho Analytics, the minimal functionality provided was sufficient to support routine decision-making processes. This outcome highlights a critical balance in implementation strategy, achieving cost-effective and sustainable system operation while maintaining adequate utility for high-level decision-making. The experience underscores that, in resource-constrained contexts, strategic compromises in advanced technical features can be acceptable if core functionality for decision support is preserved.
Ensuring the continuity of data collection and utilisation throughout the transition phase was crucial. Both the MoH and MLW made certain that data collection within the platforms persisted, and system functionalities remained intact. Other studies have indicated challenges in transitioning digital health platforms in countries where health systems are poor, leading to failure of sustaining such platforms. 27 For instance, challenges in managing multiple systems and a lack of resources, including personnel, equipment, and internet access, were identified as key concerns during and after the transition period in China and Uganda, despite subsequent successes. 16 Numerous consultation meetings with stakeholders regarding the adoption of digital platforms in existing systems appear to be a critical factor in the successful implementation of most digital platforms 24 ; without such consultations, the adoption process would most likely be challenging. Despite the MATSurvey platform being built within existing government systems, healthcare workers, including safe motherhood coordinators and the entire maternal and newborn health supervision structure, needed to maintain their morale to prevent disruptions to the system flow. Through collaboration of key stakeholders from the MoH and supporting partners, the long-term viability of platforms like the MATSurvey can be ensured.5,28 MoH took a centre role in leading, resolving issues and coordinating the transition process, making it achievable. Overall, transitioning a digital health platform into a government system can lead to a more comprehensive, inclusive, and sustainable healthcare ecosystem if implemented correctly.2,5,8,14,26,28 The experience in Malawi demonstrates that effective transition of digital health platforms in low-resource settings depends on active government leadership, sustained stakeholder engagement, and the commitment of healthcare workers. Ensuring these factors in low-income contexts, along with collaborative approaches, may enhance the success and sustainability of such interventions.
Strengths
The MoH took the lead in coordinating the transition process and establishing sustainable strategies. The active involvement of stakeholders and their partnership with the MoH resulted in shared responsibilities during the transition phase, and the integration of the system received widespread acknowledgements from all users. The MoH diligently followed the process, presenting process steps at national forums to keep authorities informed of the progress. The government ensured documentation and action points of all requirements post-transition to have the system sustained. Here's a clear paraphrase of your sentence. Given that CMED and DHD within the MoH structure are the primary implementers and managers of digital health systems and health data, QMD and RHD would oversee the execution of action points and the technical management of the system, similar to the DHIS2 framework.
Limitations
One of the key limitations of this transition process was the absence of dedicated government resource allocation for the transition process, which emerged as the single most critical factor contributing to the prolonged implementation delays. This constraint informs the broader systemic governance challenges identified, as reliance on fragmented and externally driven funding limited timely decision-making, continuity of activities, and institutional accountability. Another limitation of this work was that it was an implementation and learning process rather than a formal research study. Nevertheless, the insights generated through this process offer valuable guidance for digital health systems research and informing policy. While the data transformation and alignment between the ODK-based MATSurvey system and the DHIS2 tracker standards have been implemented, comprehensive technical documentation demonstrating implementation fidelity is still under preparation and, therefore, not fully presented in this manuscript. Despite that the plan for maintaining system technicalities and functions was devised, there was limited consensus between RHD and QMD on the way forward. Anticipated post-transition challenges included a lack of supervision and support, data inaccuracy, and failure to maintain tablets and their functionality after donor funding ceased. Staff turnover without adequate training on platform usage posed a risk to sustainability.
Conclusion
The migration of digital health platforms like the MATSurvey platform demands more than just robust leadership and partnerships; it necessitates clearly defined goals that attract stakeholder interest, along with a mindset shift in low-resource settings. The involvement of MoH leadership and stakeholders at each stage of the transition process can facilitate a seamless transition, overcoming challenges in system utilisation. The success of transitioning the MATSurvey platform was guaranteed by engaging all stakeholders and technical teams from the initial phase through the entire process. This process demonstrated that the successful migration and institutionalisation of digital health platforms depend on more than technical readiness and system design alone. While active leadership, coordinated governance, and comprehensive stakeholder engagement are essential enabling factors, the transition process clearly shows that long-term operational viability ultimately hinges on a deliberate shift toward sustained domestic financial commitment. Continued reliance on short-term, externally driven funding cycles poses a significant risk to system continuity, scalability, and national ownership. The findings, therefore, determine the need for ministries of health to embed digital health platforms within routine national budgeting and financing frameworks. This provides a clear and actionable policy lesson for resource-constrained settings, without autonomous domestic financing, even well-designed and successfully migrated digital health systems remain vulnerable to disruption and failure. Ministries of Health should align costs for hardware, software, maintenance, and human resources with existing government financial cycles. Additionally, platforms should be accompanied by evidence of effectiveness and cost-efficiency, supported by monitoring and evaluation data, to justify recurrent funding and facilitate informed decision-making for scale-up and long-term implementation.
Supplemental Material
sj-odt-1-dhj-10.1177_20552076261422087 - Supplemental material for Transitioning of the maternal and newborn health surveillance online digital health (MATSurvey) platform from a research institution to the government DHIS2 tracker
Supplemental material, sj-odt-1-dhj-10.1177_20552076261422087 for Transitioning of the maternal and newborn health surveillance online digital health (MATSurvey) platform from a research institution to the government DHIS2 tracker by Laura Munthali, Lumbani Makhaza, Annie Kuyere, Chifundo Ndamala, Mtisunge Gondwe, Blessings Kamanga, Samson Mphamba, Bertha Maseko, Chifundo Kondoni, Luis Gadama, Thokozani Namale Ganiza, Alfred Muyaya, Malangizo Mbewe, Rosemary Bilesi, David Lissauer and Linda Alinane Nyondo-Mipando in DIGITAL HEALTH
Footnotes
Acknowledgements
Sincere gratitude to the Ministry of Health RHD, QMD, and DHD departments, as well as the district and central hospitals, and the MLW team for their invaluable participation and commitment in reviewing and engaging with all activities involved in the MATSurvey transition process. A special thanks to the following individuals, who were actively involved in the process: Jonathan Phiri, Alinafe Mbewe, Juliana Kanyengambeta, Rajab Billy, Alie Chibwe, Bertha Kayuni, Olivetta Soko, Innocent Wowa, Haroon Twalibu, Lizzie Kadango, Owen Musopole, Gladys Gadama, Vincent Maso, Francis Kalonga, Eteaner Phiri, Daisy Simeza, Grace Panchi, Nyuma Manda, Jane Dzoole, Lucy Chigwenembe, Ruth Mwale, Bongani Chikwapulo, Gift Kwamdera, Selina Chikuyu, Elias Kantepa, Wisdom Chiomba, Isaac Kasalu, Alie Ndelemani, Matthias Joshua, and Fanny Kachale. Your collective efforts and dedication have been instrumental in ensuring the success of this transition process.
Ethical approval
Approval for the transition process was sought from the College of Medicine Ethics Committee (COMREC) (reference ID: P.11/20/3186) and the leadership of the Ministry of Health (RHD and QMD) of Malawi. The Malawi Ministry of Health supported the MATSurvey transition process. No human subjects were recruited for the transition process, no data was accessed for the process, and no authors had access to information that could in any way identify individuals during the transition process. Due to the nature of the transition of the MATSurvey digital health platform from a research institution to the Malawi government system, no informed consent was required. The MOH of Malawi took leadership of the process and involved recognised government stakeholders and partners in maternal and newborn health for a smooth transition. During the process, no written or verbal consent was acquired as there were no participants recruited.
Authors contribution
LMu, LMa, BM, CN, AM, SM, DL, LNM, BK, RB, MM, TG, AN, LG, and MG collaborated in the design of the transition process of the MATSurvey platform, including implementation and review of the process. LMu, LMa, MM, RB, BM, MG, CK, AN, AK, DL, and LNM also played a crucial role in the administration of the transition process. LMu played a leading role in writing and conducting literature searches. LMu, LMa, AN, and CN were responsible for the review of the manuscript prior to senior review by LNM and DL. All authors contributed towards the final version of the manuscript. LNM and DL served as the principal investigators of the project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MATSurvey was funded by the Bill & Melinda Gates Foundation (INV-004839). This research was also funded by the National Institute for Health and Social Care Research (NIHR300808 Stopping mothers dying of sepsis and NIHR134781 Improving the quality of maternal healthcare in Africa) using UK international development funding from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK government.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Due to the nature of this work, no data was used. However, if MATSurvey data is to be accessed, permission should be sourced from the Malawi Ministry of Health, who are the custodian of the data.
Trial registration
The MATSurvey transition process was undertaken under the College of Medicine Research Ethics Committee (COMREC) approval, number p.11/20/3186 and the Malawi Ministry of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.