
Abstract
Background
The process of stakeholder engagement in the implementation of a digital health platform is vital, especially in low-resourced countries like Cameroon, where the digital health ecosystem is still emerging. Stakeholder engagement can make meaningful contributions to a project allowing for increased project visibility and reach, uptake, acceptability, and sustainability. However, collaboration among stakeholders during stakeholder engagement cannot be implied. This article focuses solely on intersectoral collaboration amongst stakeholders in the implementation of the BornFyne-PNMS digital health platform in Cameroon.
Method
The study took on a participatory action research approach using stakeholder discussions, feedback from participants, questions, and suggestions to inform the progress and continuous implementation. This also included follow-up discussions with stakeholders from various sectors. The intersectoral meetings took into consideration a wider perspective on the implementation process and the launch of universal health coverage in Cameroon.
Results
A total of five stakeholder meetings were held during the implementation phase, and a total of 174 stakeholders were engaged. As a follow-up, a total of 19 letters were prepared by the Department of Family Health and addressed to strategic departments including international partners to introduce the BornFyne project. Findings are centered on six major themes that emerged from the coded data and they are as follows: (1) aligned goals and objectives; (2) enhanced health care delivery; (3) data quality and availability; (4) accessibility issues; (5) intersectoral collaboration for universal health coverage; and (6) equity aspects.
Conclusion
This article underscores the relevance of engaging a diverse group of stakeholders as a strength in intersectoral collaboration and partnership in implementing digital health interventions. It ensures that the views and experiences of those directly impacted by the intervention are considered, and it contributes to a more well-rounded and impactful assessment of the BornFyne-PNMS platform's role in improving RMNCAH in rural settings.
Keywords
Background
The process of stakeholder engagement in the implementation of a digital health platform is vital, especially in low-resourced countries like Cameroon, where the digital health ecosystem is still in an emerging stage. 1 The ongoing process of stakeholder engagement allows for continuous building and strengthening of relationships that would otherwise inhibit the project from realizing its full potential.1,2 Stakeholder engagement can make meaningful contributions to a project allowing for increased project visibility and reach, uptake, acceptability, and sustainability.1–3 However, collaboration among stakeholders during stakeholder engagement cannot be implied. Therefore, to foster collaboration among stakeholders, Chinyio and Akintoye recommend the effective use of communication and negotiation as an overarching approach. 4 Bourne also identifies effective communication as a strategy for maintaining support from key positive stakeholders and reducing opposition from negative stakeholders. 5
Sequel to the article describing important lessons on the levels of stakeholders’ influence on the design and implementation of the BornFyne-PNMS digital health platform, 1 this article focuses solely on intersectoral collaboration amongst stakeholders in the implementation of the BornFyne-PNMS digital health platform in Cameroon. The implementation of the BornFyne-PNMS digital health platform has been a complex and large project, involving more stakeholders than were involved in the design phase. For projects of this magnitude, studies show that in addition to effective communication, organizational/institutional and project governance allows for desirable project performance.4–7 Khan and colleagues in their 2019 study, demonstrate that good project governance is consistent with the principles of stakeholder engagement 7 . Evidently, continuous stakeholder engagement is important in project implementation, especially large projects that involve multiple intersectoral collaborations. However, the implementation process of these intersectoral collaborations remains to be adequately documented.8–13
Information technology tools have been used recently to facilitate stakeholder engagement and enhance effective communication strategies including social media and other platforms.9,10 As a result, these tools and strategies tend to foster intersectoral collaboration among a wider stakeholder group in the health care industry.11–15 Thus, engaging and fostering collaboration among stakeholders in the implementation of a digital platform is a multifaceted process that requires a balance of stakeholders for a sustainable management approach.1–5
In the prior report that this article follows, 1 we held a number of stakeholder sessions during the project design phase and continuously involved stakeholders in the implementation process. The team planned a follow-up stakeholder meeting with a mid-term evaluation of field results 10 months after the initial stakeholder meeting (during which the project was introduced). During the design phase, the first stakeholder meetings were held at the district, followed by the region, and the central levels, respectively.
At the central level, health policy formulation takes place through the Ministry of Public Health, while the regional level defines it into practical applicability, and the district level operationally implements it.
During the second phase of the stakeholder meeting, the goal was to present the midterm results of the BornFyne project and to assess stakeholder perspectives on the outcomes, aiming to strategically identify key players for scaling and resource mobilization for the project's next phase. This approach follows insights gained during the initial stakeholder meeting, 1 held in conjunction with the Department of Family Health. At that meeting, it was determined that not all stakeholders may realize the significance or the advantages of the digital tool during the design phase. It was therefore planned from the start to showcase midterm results to engage other crucial stakeholders who play significant roles in the implementation of the digital platform as the project progresses towards transition-to-scale and national integration. At the said stakeholder meeting of 2022 which is a prequel to this article, 1 Cameroon had not launched its pilot phase for universal health coverage (UHC). Considering this, the team reversed the approach of the stakeholder meeting in this implementation phase and began the stakeholder meeting at the central level. Thereafter, subsequent stakeholder meetings were held at the regions and the districts. The rationale for this was based on the timing of activities and the trend of events that were ongoing at the time of organizing the stakeholder meeting. This is in addition to the team's continuous one-on-one discussions/engagement with strategic stakeholders at the central level, necessary to present the midterm results. This article documents stakeholders’ identification and the process for intersectoral collaborations for the implementation of the BornFyne project's transition to scale phase and how the outcomes from these collaborations are being integrated towards the implementation of the BornFyne PNMS digital platform in the next phase.
Methodology
Study design
This article is part of a larger study, and this study employed a participatory action research approach using stakeholder discussions, feedback from participants, questions during stakeholder meetings, and suggestions to inform the progress and continuous implementation of the BornFyne PNMS digital platform.1,11 This also included follow-up discussions with stakeholders from various sectors. Participants were purposefully invited to stakeholder meetings. Some of the stakeholders had been engaged in the design phase and prior informal meetings were held with some of the stakeholders. The intersectoral meeting at the central level took into consideration a wider perspective in the implementation process through the following: (1) the launch of the universal health coverage phase 1 which is under pilot testing in selected districts in Cameroon, explored ways that the BornFyne-PNMS digital platform could be leveraged, (2) the need to involve the telecommunication sector arose in response to reviewing the software application, and (3) identifying entry points on how network coverage can be better managed. Through the Department of Family Health, (4) the country's Information System Management department was identified to assess the implementation process, provide guidance on ample data management strategies, and plan for data interoperability to align with the national strategy. With the goal of integration within the country's system in line with the Health Management Information System, and the District Health Information Software 2 (dhis2) currently being implemented in Cameroon. Last, other in-country-based international partners like the United Nations Population Fund (UNFPA), the United States Agency for International Development (USAID), World Health Organization (WHO), Jhpiego, Care International, Plan International, and others including local NGOs working to improve maternal health in Cameroon, were engaged during the stakeholder meeting through the Department of Family Health to provide their feedback on the mid-term results from the implementation of the BornFyne-PNMS digital platform in the four districts.
Study framework
The framework used in this article has been extensively described in our earlier article including the analytical grid,1,16 and the identification of intersectoral level of stakeholders. We discuss the outcome of the stakeholder meetings using Yang and Shen's model relevant to the process of continuous stakeholder engagement, namely: Inform: Provide stakeholders with fair, unbiased information that will assist them in comprehending problems, potential solutions, and/or alternatives. Consult: Stakeholder input on the analysis, choices, and/or decisions should be sought. Engage: Work closely with participants throughout the process to make sure that their needs and wants are continually recognized and taken into account. Collaboration: Joint effort with stakeholders on all decision-related issues. Empower: Give stakeholders the power to make the final choice 12 .
Identification of stakeholders in the implementation phase
As described in our earlier study, we categorized stakeholders as primary providers, secondary, primary recipients, and secondary recipients.1,16 We have illustrated the steps in the stakeholder intersectoral engagement process in Figure 1, which incorporates seven steps as described in the article.
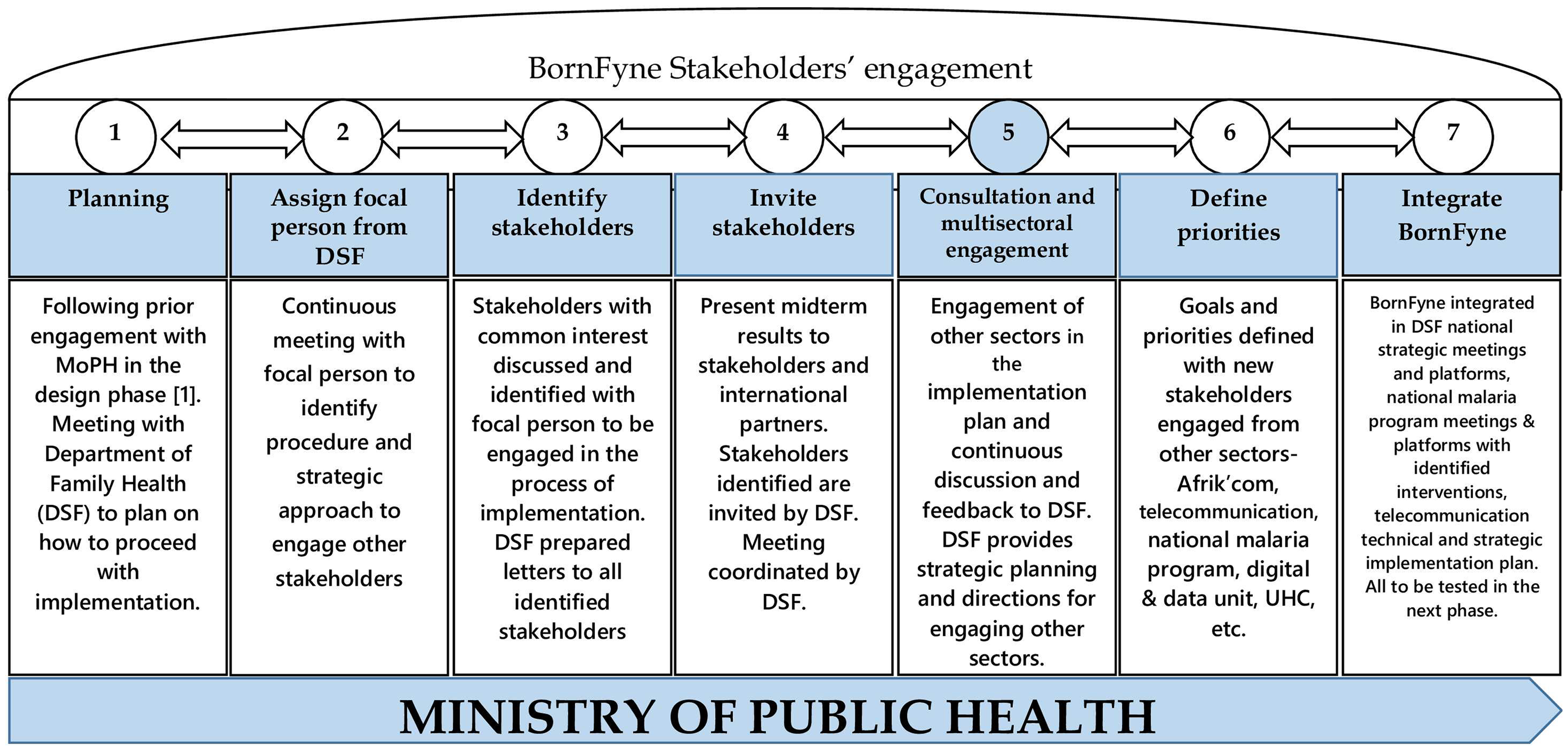
BornFyne stakeholders’ intersectoral engagement process.
Central level
Building on our prior work outlined in a previous article, 1 the BornFyne project has forged a strategic partnership with the Department of Family Health within the Ministry of Public Health. From the early stages of the project, subsequent to the initial stakeholder meeting in 2022, the department designated a focal person from the directorate's secretariat specifically to oversee the BornFyne portfolio. This focal person was actively involved in the project, working closely with the BornFyne team. Regular meetings were held to address project challenges, seek strategic advice, and understand procedural navigations within the department. The BornFyne team consistently consulted with this focal person or directly with the Director of Family Health before moving forward with any significant discussions or decisions, ensuring that all actions were aligned with departmental guidance and strategy.
A number of meetings were held with the Directorate of Family Health at the Ministry of Public Health to strategize and identify relevant stakeholders needed to be engaged in the stakeholder meeting. Introductory letters and emails were sent out to all the identified stakeholders inviting them to attend the BornFyne-PNMS stakeholder meetings and to assess the progress of the implementation process. The letters were prepared under the leadership of the Department of Family Health at the Ministry of Public Health. These stakeholders included international organizations and local organizations including other structures within the Ministry. Furthermore, the BornFyne team suggested to invite selected health providers from each of the pilot districts who were earlier trained (during the design phase) and are using the BornFyne-PNMS at their health facility. This was to allow for the demonstration of their acquired knowledge and skills before policy makers and partners, and their experience with utilizing the digital tool to register pregnant women at their health facilities.
Expectedly, the health care providers led the demo sessions on how to use the tool during the stakeholder meeting. This approach was different from the initial stakeholder meeting in 2022 where the project team and the information technology (IT) team presented the demo version and how the platform was expected to work. However, during the mid-term stakeholder meeting, the earlier-trained health care providers (HCP) demonstrated their use of the platform to enter data and deliver care, while the project and IT team provided support. To reflect inclusion in the process, select community health workers (CHW) who support women in utilizing the platform at the household level were also invited from each district to present their experiences at the central-level stakeholder meeting.
Other details that were shared during this meeting included the number of pregnant women recruited versus the number who expressed their willingness to use the BornFyne platform, but do not have a smartphone, the household survey conducted, the various health facilities involved in the project, summary of midterm results for intervention and control areas and an overview of the workshop that was conducted to assess the WHO digital adaptation kit guidelines for antenatal care versus the health facility registers (detailed outcome of the workshop is presented in a subsequent article), the project challenges experienced by community health workers and health care provider and the next steps in the project implementation. Finally, the team officially launched a campaign titled “changing lives with one mobile phone, an impact model of BornFyne-PNMS project.” The BornFyne team explained that the campaign is based on the findings of the preliminary research work that was presented. Looking at what one mobile phone that is connected to a health facility can do to change the live of a rural poor woman, especially in rural settings, households, and the community. Further at a health facility level, changing the mindset of health providers regarding the way they deliver care and how data is collected to inform decision-making, and improving quality of care, and at the health system level, how it can help strengthen health management information system and availability of data all geared towards achieving universal health coverage and reducing maternal mortality.
At the close of the stakeholder meeting, the project team met with each invited representative and scheduled a follow-up meeting with strategic country representatives of the organizations. Also, follow-up meetings were scheduled with other stakeholders from different sectors. This meeting was to engage stakeholders that were identified to ensure alignment with the priorities and objectives of BornFyne and further facilitate beneficial ways of interacting with the digital platform. As the country is embarking on data harmonization for digital platforms, it was essential to engage with potential partners to understand the capabilities of BornFyne-PNMS in the area of reproductive maternal newborn child and adolescent health (RMNCAH). All while noting that the BornFyne-PNMS is one of the first digital platforms that connects pregnant women to health facilities and collects RMNCAH data that integrates the WHO digital adaptation guidelines for antenatal care (ANC) in Cameroon. The initial stakeholder meeting that was held in 2022 at the central level involved only national sectors 1 . Subsequently, as the project progresses, the implementation strategies and ongoing discussions with the Ministry of Public Health especially with the launch of the UHC pilot phase, there was a need to engage other stakeholders and international organizations working for RMNCAH.
Regional and district level
During this implementation phase, the regional and district stakeholder meetings were combined for efficiency. Letters of invitation were sent to all stakeholders who were invited during the design phase. Additionally, word-of-mouth by CHW helped to invite some of the women who have used the BornFyne-PNMS alongside their male partners. The purpose of the stakeholder meeting at this level was to share updates on the progress results of the project and gather feedback on how to better refine/adjust the platform moving forward.
International level
The team continuously engaged the digital health team at the WHO and provided updates on the progress of the project on the integration of the digital adaptation kit (DAK) content for ANC into the BornFyne-PNMS content. Feedback was solicited from the team who also engaged with the local WHO office. The WHO digital team provided the BornFyne team with a template to document country experiences in the process of integrating the DAK for ANC content into the BornFyne-PNMS content.
Data collection and analysis
Stakeholder meetings to present mid-term results were held from June to September 2023. The stakeholder meetings were organized in various sessions and phases, with the Directorate of Family Health team strategically assisting in identifying stakeholders for the central level meeting, especially those involved in combatting maternal mortality in the country, the digital unit, and telecommunication. At the central level, the meeting was held at a convenient location accessible to stakeholders. All meetings lasted between 2 and 3 hours and in the fashion of focus group discussions using a presentation format followed by questions and answers and facilitated by the Department of Family Health and the project team at the central level and at the district level, facilitated by the project team. Questions were asked by the stakeholders randomly following the presentation of the project. No interview was conducted, it was all in a format of a presentation, followed by a question-and-answering format as documented in Table 3. Specifically at the central level stakeholder meeting, the department of family health presented their observations and feedback from the field in monitoring the BornFyne project activities across the four districts.
At the district level, the discussions were led by the BornFyne project coordinators for each region with assistance from the project lead. The project coordinators presented an overview of the project's progress and results and challenges. Health providers who attended the central-level stakeholder meetings were also asked to present to the district their experiences and observations, recommendations, and expectations from attending the central stakeholder meeting.
Each stakeholder meeting commenced with a general introduction of the project considering that some of the stakeholders were not present in the initial stakeholder meeting that was held in August 2022. 1 The presentation briefly stated the 2-way user system/platform allows pregnant women to communicate with their healthcare facility/provider and vice versa. It consists of six features, two of which can be accessed offline. The objective was to test the functionality and the feasibility of the digital application in a real-life situation, where limited support of equipment was provided. The objective of the meetings was mainly to share the midterm results of the project and discuss avenues for further collaboration during the project implementation. The team also shared the requirements for the continuation of the project in Cameroon with the various stakeholders. Extensive notes were taken by three team members (RS, EK, OK) as well as observations, as there were no audio recordings. Responses, questions, and answers from participants were documented and presented in Table 3. Experiences and observations from the use of the platform, as well as recommendations and expectations, were noted.
We noted the level of power and influence of each category of stakeholder on a 3-point scale as described in our prior study using Namazzi and colleagues’ approach (high-level influence; moderate, and low, and high-level support; moderate, and low) including terminologies as opinion leader and decision makers.1,16 Strong agreement was characterized by acknowledgment of project objectives aligning with stakeholders mandate or goals without any hesitation from body language or communication style, moderate agreement was characterized by hesitation from body language and low agreement was outright disagreement or miss alignment of project objectives to stakeholder's mandate or vision.
The notes by the three team members were exported into MaxQDA for analysis. Feedback and comments were coded deductively using a content analysis approach by identifying concepts present in the text, and relationships between the identified concepts.17–19 Thereafter, all codes were categorized into themes, assessed by MN and OP, and further reviewed by AWF and SY. The level of agreement was assessed by MN and PO and reviewed by VN, OK, and FW.
Ethics
Ethical approval for this study has been obtained from the National Ethics Board of Cameroon Ref 2022/07/1467/CE/CNERSH/SP and the University of Ottawa Social Science Ethics Board Ref # H-05-22-8077. Administrative clearance was received from the Ministry of Public Health at the national level in Cameroon D30-1440 No. 631-3822, in collaboration with the Division for Health Operations Research (DROS) in Cameroon, the Southwest Regional Delegation of Public Health ref# P412/MINSANTE/SWR/RDPH/CB:PF/941/618, and Central Regional Delegation of Public Health were also received ref# 1393-4/AAR/MINSANTE/SG/DRSPC. Lastly, there was a memorandum of understanding with all the district medical officers in the respective districts. Participants were voluntarily enrolled in the study on the basis of free and informed consent. Participants were informed that feedback would help refine the application and information collected from the stakeholder meetings would be used to inform the next phase and further refinement. Due to the nature of the stakeholder meetings, written consent was not taken from participants. Stakeholders were verbally informed during the discussions that the presentation of the results and their feedback and questions which are presented in Table 3 will be documented and published. However, all providers and women enrolled in the project and attended the stakeholder meetings provided written informed consent from the onset of the project inclusive of all project activities.
Results
A total of five stakeholder meetings were held during the implementation phase and a total of 174 stakeholders were engaged at all levels (see Table 1). Of the 19 official letters prepared by the Department of Family Health and addressed to strategic departments including international partners to introduce the BornFyne-PNMS project at the central level meeting, 14 responded to the invitation and attended the meeting or sent a representative from their organization, and five international partners could not attend, and did not send a representative. It was observed that a high-level meeting chaired by the WHO local office coincided with the meeting. Thus, three stakeholders sent out a notification for their absence but did not send a representative. However, a follow-up meeting was scheduled to present an overview of the project to those who were absent.
Stakeholders identified and engaged during the BornFyne-PNMS project implementation

Our findings are centered on six major themes that emerged from the coded data and they are as follows: (1) aligned goals and objectives; (2) enhanced health care delivery; (3) data quality and availability; (4) accessibility issues; (5) intersectoral collaboration for universal health coverage; and (6) equity aspects.
Aligned goals and objectives
There was a generally strong agreement on project objectives aligning with the objectives or mandate of the stakeholders. There was no observed low disagreement, but one moderate agreement (see Table 2). Stakeholders expressed their continued support for the project and described it as “innovative.” With the BornFyne digital platform, stakeholders including international partners, identified the alignment of the project's objectives with theirs such as the ministry's launch of a digital framework as well as the UHC launch in Cameroon. This alignment of objectives indicates a strong interest in the project and support with the goal of reducing maternal mortality by strengthening health systems and data availability and quality. The BornFyne project's goal is to achieve optimal health across the lifespan of the population it serves through advanced digital health systems. To improve maternal and child health the project focuses on quality antenatal care, prompt reporting, quality data and e-networking. By doing this, the project in collaboration with the department of family health is making a step toward the achievement of the sustainable development goals and the country's goal of 2035. [Central level national stakeholder] This is a very innovative and important project, in fact the paper [method of maternal and child health data collection is becoming too much, and we need to transform to digital. [Central level international stakeholder]
Summary of stakeholder's characteristics, influence, and acceptability of the BornFyne -PNMS project

An analytical grid highlighting identified stakeholders’ interests and acceptability of BornFyne-PNMS project (Adapted from Namazzi et al., 2013 and sequel to Obegu et al., 2023).
Enhanced healthcare delivery
Stakeholders acknowledged the project's implementation in enhancing community mobilization and participation. CHW and HCPs especially described the enrollment process as “engaging” wherein women were excited to be captured on the platform and looked forward to participating in ANC visits. In the same vein, stakeholders shared that the project implementation encouraged healthcare delivery in a more personalized way with a level of trust between health providers and recipients of care. The digital platform has greatly increased trust between the women and the healthcare providers through familiarizing them to one another. Those who are not enrolled in the project should also benefit from this connection and familiarity that community health workers and health care providers develop with the pregnant woman. [District level stakeholder] It has positively affected and changed the way health care providers and community health workers view antenatal care. It has become more personalised, and it entails building a relationship. This is an opportunity for community health workers and health care providers to strive to attain a “zero death” in maternal care. [District level stakeholder]. The mobilization that I experienced at the central level stakeholder meeting changed my perception about this project and I am willing and ready to put in effort to ensure that the project remains in this district, especially with the impact the project has created in this health district. [District level stakeholder]
The BornFyne application is useful in limiting unnecessary hospital visits, as you can communicate directly with your HCP. [Primary recipient]
The application has also made us to realize that there is a gap in communication between the providers and pregnant women and this is an important component in building patient-provider relationship. Therefore, providers who are here can see for themselves how the application is trying to close this gap and making us realize clearly that we have not been doing well in this aspect of communication and the results and outcome of this BornFyne intervention are clear. [District level stakeholder]
Data quality, availability, and adherence
Stakeholders at both central and district levels as well as HCPs and CHWs community health workers and health providers expressed their thoughts about collecting quality data as well as available RMNCH data. Impressively, they highlighted the digital platform's role in improving data collection and increasing ANC visits among pregnant women across regions in Cameroon.
One participant at the district level highlighted significant observations at a facility since the introduction of BornFyne, particularly in relation to the attendance for prevention of HIV mother-to-child transmission programs. They expressed that their primary reason for attending the stakeholder meeting was to discuss these observations and advocate for expanding the BornFyne platform to the entire facility and other health facilities to enhance adherence and data quality. Before BornFyne, as reported by the participant, attendance rates were below 50%, but there has been a noticeable improvement since its introduction. The participant believes that the reminder messages sent to women through BornFyne have helped increase their adherence to antenatal care and subsequently improved their commitment to PMTCT treatment and improved data. When it comes to the challenges, we face in collecting quality data, I can see BornFyne digital platform as a means to resolve the problem of missing data. This platform has a great potential in ameliorating family planning and useful for intermittent preventive treatment recalls ameliorating maternal health. [Central level stakeholder] I am pleading that this platform should be introduced to other health facility because the attendance to PTM [prevention of mother to child service before the digital platform was low with only about 49%. After the platform was introduced, it increased to over 60% since the beginning of 2023 and can be attributed to the regular reminder messages. I hope this project will be expanded to all the health facilities to improve attendance and coverage of this service. [District level stakeholder] Providing a platform at the peripheral level to collect disaggregated data to enhance adherence to clinical practice is commendable. I will strongly recommend that the project align with the national information system to ensure data that is collected can be accessed. [Central level stakeholder]
Accessibility issues
A concern with access to smartphones was raised in relation to enrollment coverage on the digital platform. Stakeholders, particularly health providers described the lack of smartphones as a challenge during enrollment. Despite the limited access to smartphones in rural areas, health providers emphasized the benefits of the digital platform for maternal and child health care delivery. Providers also mentioned how women are coming and requesting to be registered after the research team stopped the recruitment of participants to observe and evaluate the outcome so far. it was a great experience to meet with the other partners at the central level and also to understand that the project was moving forward and able to demonstrate what we have been trained and doing for the project to the other partners. [District level stakeholder] Many women are still willing to register, and they keep coming to us requesting that they want us to enrol them and give them access to the application. [District level stakeholder]
Equity in coverage and Internet network challenge
An important equity challenge was presented by the BormFyne project team and also observed and discussed by stakeholders. This was in line with the limited possession of smartphones by women and the number of women who expressed willingness to use the phone. According to health providers, it was a huge challenge for them as women were eager to get connected but limited phones. In addition to the smartphone challenge, the internet challenge was also reported by women and health providers. However, despite this equity gap in accessing smartphones, the healthcare providers and community expressed their willingness to continue using the platform in a single phrase as presented below. You cannot bring light to women and take it back! [HCP Tiko/BornFyne breastfeeding mother Ayos]
In a similar fashion, stakeholders were pleased with the project’s objective of targeting rural areas to enhance equity in addressing maternal health issues. Most especially rural areas face more challenges in accessing maternal health services and see the project to be different from other digital platforms that have been introduced to them. I am very impressed with this project because you have chosen to target a specific population. that we often abandon, the rural areas. Trying to provide an intervention to remote population. connecting them to a network of transportation to facilitate movement for pregnant women. during emergency is something that anyone will listen to what you are saying, and we will. continue to support your efforts to ensure this platform is scaled across all districts. If you had targeted urban cities, it would not have meant anything to us because we have seen similar. interventions before, but your choice of rural settings is making a difference, and we will ensure this project is scaled and sustained. [Central level stakeholder]
During stakeholder meetings, the project team explored with the community what they would suggest especially with limited phones, and to gather from women and the community what they think about the project after experiencing it. They suggested that if the platform could be accessible on regular phones, it would greatly address the equity challenge because women saw it as an innovation and an experience that they had not seen and even the health providers saw it as facilitating their work.
The team presented some of their challenges in the implementation process and highlighted constant power outages and poor connectivity which sometimes hinder the reception of reminder messages in a timely manner. Most women are willing to get connected to their health providers but do not own a smartphone which presents an important equity gap. The team also presented their initial collaboration with Orange Cameroon in phase 1 and the need to work with the telecommunication company to facilitate some of the implementation process, especially in the completion of the emergency feature which they are looking to have it accessible offline. Details on the challenges and questions posed by stakeholders and recommendations proposed during the stakeholder meeting at the central and district levels are presented in Table 3.
Project implementation challenges and solutions discussed with stakeholders.

Intersectoral collaboration for universal health coverage
Discussions about introducing the next phase of the project were brought up by stakeholders in relation to the launch of UHC in the country. Stakeholders identified the need to pilot test the digital platform in at least one of the districts currently pilot testing the UHC program, in light of harmonizing health data interoperability. The BornFyne team was urged by stakeholders to participate in inter-ministerial discussions on digital health and interoperability, among whom were represented in the stakeholder meeting. I want to first applaud this team for this wonderful innovation to help strengthen our health information system it is important to also note that there is an inter-ministerial committee for digital health which covers all aspects around digitalisation. It will be good for the BornFyne team to engage with us and work with us as a subgroup of the committee and especially as we work together towards interoperability. [Central level stakeholder] I am impressed with this innovation especially as it connects to the household and women who are living in rural areas especially in this digital age. Even if a woman cannot use a phone, their children can teach them. This is very important and innovative, and I would like to know when the next phase will commence because this project is important to us in supporting the universal health coverage agenda for the country and harmonizing data within our central digital unit. [Central level stakeholder]
Key outcomes of the stakeholder meeting and intersectoral collaboration and how the BornFyne team integrated the feedback
Much of the feedback and outcomes from the stakeholder meeting indicated that additional resources are required for full implementation and integration of the feedback in the next phase as described below. Nevertheless, the team has made significant progress immediately following the meetings by establishing feedback mechanisms and discussing frameworks and directions as we explore additional funding opportunities. Below, we outline the outcomes and describe how we have integrated the feedback and outcomes, pending further resources to ensure seamless implementation of the next phase.
Outcome 1: Referral to work with telecommunication sector
The BornFyne team was advised to collaborate with telecommunications companies to facilitate access to BornFyne features to funciton on egular phones in the next phase, aiming to expand coverage and address some equity gaps. Following this recommendation, the team initiated consultations with Afrik’com, a pivotal public-private partner working with telecommunication firms. The team successfully established a memorandum of understanding to secure a USSD code for BornFyne, enhancing the system's implementation in the forthcoming phase (see Table 2). This arrangement will enable the conversion of some key features into regular phone functionalities to broaden coverage.
Outcome 2: Recommendation from international stakeholders to engage with the national malaria program
The BornFyne team was requested to meet with the national malaria program to discuss intervention strategies and address data challenges within the department. After presenting results, which included some key malaria variables developed within the BornFyne platform. The platform garnered interest from international stakeholders as a potential tool to enhance data quality for the malaria program. Consequently, the BornFyne team engaged in extensive consultations with key stakeholders from the national malaria program. These discussions led to the endorsement of the BornFyne platform as a potential platform to facilitate the uptake of IPT3. Further details on how the team engaged the malaria program and identified variables to be incorporated for the next phase of the project through these consultations are outlined in a separate paper.
Outcome 3: Meeting with the national digital unit and data unit responsible for DHIS2
The team was directed to meet with the Department for Health Data and the digital unit to discuss strategies concerning interoperability and data ownership. Representatives from the digital unit and DHIS2, who attended the stakeholder meeting, scheduled follow-up sessions with the digital unit team. During these meetings, they shared the national strategic framework for data and interoperability, as well as national variables and indicators. Working closely with the data unit, the BornFyne team identified steps to adapt a national ANC guideline, ensuring systematic integration of key variables and indicators. In subsequent discussions, the national digital unit outlined essential elements for interoperability, including training, capacity building, and logistical support, crucial for smooth implementation and data hosting as the project moves towards national data ownership in its next phase.
Outcome 4: Follow-up with the universal health coverage team
Further discussions took place with the UHC unit to explore integrating the platform into districts currently implementing UHC for the project's next phase. This resulted in a recommendation to include an additional district currently piloting UHC. Additionally, BornFyne will enhance communication efforts by utilizing the application's U1 features to engage households on UHC components. The BornFyne team will collaborate with the UHC team to develop content for household communication and integrate this into the BornFyne medical advice module in the next phase.
Outcome 5: Contextualize national ANC guidelines using the WHO DAK tool for ANC
The BornFyne research team identified a significant gap while attempting to define variables for the revised BornFyne version 2.0: the lack of ANC guidelines at health facilities. This issue was presented to stakeholders, leading to a consensus on the need for a national committee to support this effort. This committee, led by the Department of Family Health and including strategic and technical members, aims to review and adapt WHO digital adaptation guidelines for ANC to fit the Cameroonian context. Following the meeting, the BornFyne team and the Department of Family Health initiated the process by identifying key strategic and technical stakeholders to support this effort. This process is pending additional resources for the BornFyne team to collaborate effectively with the Ministry of Public Health to fully implement the defined strategies.
Challenges in engaging stakeholders
Throughout the BornFyne project, which commenced during the design phase in collaboration with the Ministry of Public Health's Department of Family Health, numerous challenges have been encountered, primarily related to delays in meeting key stakeholders. These delays necessitate patience and continuous follow-up, as it is common for meetings or consultations with a stakeholder to be rescheduled multiple times before finding a suitable date. Most consultations are conducted face-to-face, further complicating scheduling as meetings often need to be postponed or rescheduled. A significant challenge involves coordinating times with focal persons from different sectors and directors who have demanding schedules. The Department of Family Health has facilitated these meetings by providing referrals and contact details.
In addition, each new director or various sub-structures within a single department may require separate meetings to ensure comprehensive feedback and input from all relevant sub-committees. This process involves presenting the BornFyne demo versions multiple times to incorporate all feedback and understand the best ways to support data quality initiatives. Introducing a digital platform to directors who may not be familiar with digital tools poses its own set of challenges, especially in the absence of key technical staff. This issue was carefully managed with the focal persons throughout the project to ensure smooth integration and understanding.
Discussions
This article underscores the vital role that continuous stakeholder engagement plays in intersectoral collaboration at all levels in implementing digital health projects, especially on RMNCAH. An important lesson learnt on RMNCAH oroject is not only as a multisectoral initiative that involves various sectors and stakeholders to be on the same page for the implementation in achieving desirable outcomes, but important to engage all active partners both national and international to get updated on national priorities, strategies, and interests and helps avoid redundancy in project activities in the field. There is need to engage telecommunication companies, identifying other sectors like the digital health unit responsible for interoperability with other platforms, the statistic and data unit, and other international stakeholders that are implementing activities in relation to RMNCAH.
Based on the results, support for the project was strong at all levels and especially at the central level with a focus on how the project perfectly aligns with the national digital health framework and strategies, the need to improve data, reduce maternal mortality, improve quality of care, and health information system for the country, need for digital transformation of skills, the need to build capacity of health providers in using digital platforms and health facilities, the need to improve on clinical guidelines and adherence to protocol 20 , the need to establish interoperable layers and the launch of universal health coverage pilot phase which saw the project as an avenue to leverage to facilitate implementation as listed in Table 2. At the community or district level, the support was strong with acceptance of women in using the innovative platform which to them was the first time to get such an experience, at the level of health providers it was a dual experience, as a first time to use the digital platform to deliver care, but also helps to introduce them to the use of technology, which some of them have not used before. Thus, helps build the capacity of providers and prepare them for the future of digital health in Cameroon.
The idea of bringing health care providers and CHWs who have been trained and are using the BornFyne platform to physically demonstrate to policymakers and international partners, the skills they’ve acquired within the 10–12 months of project implementation at the central-level stakeholder meeting was applauded by many partners. This approach represents a departure from the more traditional practice of having central stakeholders meet to present outcomes only in numbers trained without any physical demonstration of what the impact of the numbers represents and/or has been acquired in practice. This demonstrates a commitment of the project team to foster collaboration and communication among various stakeholders in the healthcare system in the following ways:21–27
Inclusivity: by involving both healthcare providers and CHWs from the district and health facilities implementing BornFyne during the central stakeholder meeting, it ensures that voices and perspectives from different levels of the healthcare system are heard. This can lead to more comprehensive and effective decision-making. Intersectoral Collaboration: Such collaborative stakeholder platforms encourage healthcare providers and CHWs from different districts and health facilities (public, private, and confessional) to engage and share experiences. This intersectoral collaboration can also result in more holistic and patient-centered approaches and improve motivation and performance. Efficiency: This approach also allows an efficient way of sharing information and resources; it also reduces the need to consult with multiple stakeholders to present the same result and save time and resources. Networking and partnership building: The stakeholder platform provides an opportunity for partners to connect and collaborate which can lead to valuable partnerships and synergies towards the implementation of the project. Enhanced communication: Bringing healthcare providers and CHWs to interact directly with central stakeholders can improve communication and understanding between these groups and decision-makers in the way policies are designed and also understanding challenges at the grassroots (operational level) and interventions that can help address the challenges. Comprehensive Solutions: Digital health interventions are complex healthcare interventions that require multiple sectors to be engaged, for example, transport, telecommunication, IT, and data units, etc. It, therefore, requires input and cooperation from various stakeholders. Therefore, bringing different groups together allows for the development of a more comprehensive direction and solution to address the challenges.
As indicated earlier, the findings of this article are discussed using Yang and Shen's model relevant to the process of continuous stakeholder engagement, namely: inform, consult, engage, collaborate, and empower.
Inform: The BornFyne team employed various approaches to inform the stakeholders with the aim to mainly share the midterm results of the project implementation phase. It was a perfect avenue for other partners to get first-hand information on what the project is all about and how they can best strategize their resources to align with the priorities and interests of the Ministry of Public Health and the Department of Family Health. In addition, other sectoral representatives of universal health coverage and maternal mortality programs strongly provide and communicate to other potential partners and funders the priority and agenda to support the project. Thus, this avenue provided a platform for other potential funders and sectoral collaborators to pose questions, provide feedback to help inform the project, and also identify gaps and areas of improvement for the platform with information that will assist them to better understand the intervention.
Consult: The use of strategic, one-on-one discussions and follow-up meetings with stakeholders, especially the ones who attended the presentation of the mid-term results to solicit stakeholder feedback on the analysis, alternatives, and/or decisions made provides insights to the project team and guide the team on who to engage, at what level, and how to proceed at scale to ensure a smooth implementation for project sustainability.
Involve: The BornFyne team involved the Department of Family Health at the Ministry of Public Health from the onset of the project. As a result, it was easier for the team to identify relevant and strategic stakeholders at various levels, and when to engage and work with. For example, through the Directorate of Family Health, the team was able to engage with Afrik’com and established a partnership agreement for the BornFyne project to provide access to a telecommunication network that will provide broader coverage, and the team is better position to work with the telecommunication companies to ensure the platform reach a wider audience which was an important outcome from the stakeholder meeting. These are stakeholders that the team would not have identified as a strategic channel to use to engage the telecommunication company. This approach provides a balance of information and strategy because it enables the team to stay in constant communication with all intersectoral units within the Ministry of Public Health that are involved in RMNCAH and maintain and understand their communication strategy that will be of benefit to the Ministry of Public Health and its objectives.
Collaborate: As the BornFyne team partners with the Department of Family Health, it facilitates continuous communication and collaboration with other sectors and stakeholders involved in the fight against maternal mortality (see Figure 1). Thus, the team works in collaboration with other potential partners who are working on the same objectives. For example, as a result of the stakeholder central level meeting which engaged other partners, the BornFyne team was referred to meet with the malarial program to review challenges in data collection and strategize to support data collection for the next phase.
Empower: The BornFyne team with the approach employed places decisions in the hands of the Department of Family Health and Ministry to ensure that the data that is collected within the platform will be stored and secured by the Ministry. Thus, this approach will facilitate country ownership and sustainability. Most importantly, this approach gives access to the final decision-making in the hands of stakeholders. For example, The Department of Family Health leads all key stakeholder meetings, and the team discusses with the data and digital health department and explores ways to collaborate to ensure interoperability will be led by the national digital unit team to align with the national strategy to facilitate scale and sustainability. Thus, empowering the local team as a step towards transitioning to ownership to effectively manage the platform for sustainability.
Strength and limitation
Evidence indicates that engaging a wide range of national and international stakeholders to gather their views and perspectives is important in project implementation and scaling28–30. In the context of the BornFyne-PNMS digital platform as an intervention, particularly in the context of rural settings and with a focus on RMNCAH, this approach is a strength for several reasons and informed from the literature28–32:
Diverse inputs: Involving a broad spectrum of stakeholders ensures diverse input and insights. Different stakeholders bring unique perspectives, experiences, and expertise to the discussion, enriching the understanding of the intervention's impact and challenges as listed in Tables 2 and 3. Holistic approach: RMNCAH is a complex and multifaceted area of healthcare, therefore, engaging a wide range of stakeholders allows for a more comprehensive assessment of the intervention's effectiveness and potential areas for improvement as described in Table 3. Global relevance: By including both national and international stakeholders, the article can provide insights that are not only relevant at the local level but also have broader applicability and implications for RMNCAH interventions in other regions and countries. Local context sensitivity: Rural settings often have unique challenges and healthcare needs. Input from local stakeholders helps ensure that the intervention is sensitive to the specific context and can be effectively tailored to meet the needs of rural communities as listed in some of the questions in Table 3. Participatory decision-making: Engaging stakeholders fosters a sense of ownership and participation in decision-making. When stakeholders have a say in the design and implementation of interventions, they are more likely to be invested in the success and sustainability of the intervention as listed in Table 2 and the recommendations from stakeholders in the outcome section and also in Table 3. Validation and credibility: Gathering views and perspectives from a wide array of stakeholders can serve as a form of validation of the relevance of the intervention. It adds credibility to the findings and recommendations presented by the stakeholders and listed in Table 3. Policy and program development: The insights gained from stakeholders can inform policy development and program planning. This can lead to more targeted and evidence-based approaches to addressing RMNCAH challenges. This aligns with the engagement of the national malaria program and the strategy for BornFyne to support program outcomes by testing key indicators in the UHC districts in the next phase to inform policy. Also, the UHC unit recommends additional districts to be included in the next phase to inform strategic policy directions for UHC using digital platforms. Collaboration opportunities: The article demonstrates strength in stakeholder engagement and how it often opens doors for future collaboration. Such partnerships and collaborations with stakeholders are instrumental in scaling up and sustaining the interventions.
The article presents some important limitations as it did not collect demographic information of stakeholders because it was not designed as an in-depth interview or focus group discussion. It focused on documenting questions and feedback from stakeholder during the presentation of the midterm results and their perspectives and was not audio recorded. Therefore, there was no data saturation assessment. We assumed this approach would help minimize bias in stakeholder participation. Though three note-takers were assigned to document feedback and questions and answers, it is possible to miss out on some points. However, continuous consultations and meetings with stakeholders help minimize this limitation. The article was not designed to assess differences in the districts as this is further assessed in subsequent articles. The purposeful sampling frame employed to identify and invite stakeholders was based on emails and letters of invitation sent to identified stakeholders and word-of-mouth invitations. This approach may likely bias some potential participants that may have been left out.
Conclusion
Generally, this article underscores the relevance of engaging a diverse group of stakeholders as a strength. It ensures that the views and experiences of those directly impacted by the intervention are considered, and it contributes to a more well-rounded and impactful assessment of the BornFyne platform's role in improving RMNCAH in rural settings. Overall, the initiative appears to be a positive step in introducing the intervention to a wide range of partners, promoting collaboration, and ultimately improving health outcomes. Thus, recognizing the value of involving all relevant stakeholders in the decision-making process and fostering an environment of cooperation and shared goals.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241287963 - Supplemental material for The role of intersectoral collaboration and continuous stakeholder engagement in the implementation of the BornFyne PNMS project in Cameroon
Supplemental material, sj-docx-1-dhj-10.1177_20552076241287963 for The role of intersectoral collaboration and continuous stakeholder engagement in the implementation of the BornFyne PNMS project in Cameroon by Miriam Nkangu, Pamela Obegu, Ngo Valery Ngo, Franck Wanda, Regina Sinsai, Evrard Kepgang, Mwenya Kasonde, Odette Kibu, Victor Ndiforchu, Arone Wondwossen Fantaye, Ronald M. Gobina, Nkengfack Fobellah and Sanni Yaya in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank all the stakeholders and their valuable contributions during the various stakeholder sessions, which will help inform the development of the BornFyne PNMS platform. The authors would also like to acknowledge the district team, the collaborators, and the feedback received from stakeholders on this project. Authors would like to thank WHO digital team for their support and feedback. Special thanks to the Ministry of Public Health in coordinating the central stakeholder meeting and their immense support and for creating an enabling environment to ensure a smooth implementation of the project.
Contributorship
MN conceived the idea and led the design and methods. MN led data collection with assistance from NV, FW, OK, RG, VN, and NF. Transcription was supported by RS and EK. The coding was done by MN and PO and validated by AWF. SY and MN wrote the first draft of the manuscript. PO provided additional inputs. MN, PO, AWF, SY, MK, NF, RG, VN, and FW critically revised the manuscript and provided feedback. All authors reviewed and agreed on the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The project is supported by Grand Challenges Canada transition-to-scale funding.
Grand Challenges Canada, (grant number TTS-2209-55037).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.