
Abstract
Background
Digital health technologies offer promising avenues for addressing challenges in healthcare systems, particularly in regions such as Sub-Saharan Africa, including Cameroon. These technologies can improve access to care, enhance quality, and optimize healthcare delivery and monitoring through better data management and interoperability. This study aimed to assess the landscape of digital health implementation for data services in Cameroon, focusing on governance, interoperability, and the adoption of digital platforms.
Methods
We used a mixed methods approach, administering questionnaires (n = 60) and conducting in-depth interviews (n = 6) with digital health experts. The sample was purposively selected to include individuals with experience in digital health projects. Data were analyzed to assess the extent of digital health adoption, including challenges related to interoperability with the District Health Information System 2 (DHIS2).
Results
The study revealed significant gaps in governance and policy support for digital health in Cameroon, with 85% of respondents unaware of any existing guidelines. This gap in governance highlights the need for comprehensive policies to guide digital health initiatives. Moreover, 86.7% felt there was inadequate policy support for digital health implementation, particularly among those with higher academic qualifications (f = 16.033, p = 0.001) and those working at the central level (90.9%). This lack of policy support underscores the necessity for stronger governance and specific policies to support digital health implementation. While 63.3% of organizations had used digital platforms, only 63.3% of respondents received formal training, and 80% were aware of DHIS2. However, 45% reported challenges in interoperability between their systems and DHIS2, which was significantly more common among males (χ² = 4.411, p = 0.036) and those with a Master's degree (f = 12.057, p = 0.003). These interoperability issues indicate a need for technical solutions and training to ensure seamless data exchange between different health information systems.
Conclusion
Cameroon faces critical challenges in digital health implementation, particularly in governance, policy support, and system interoperability. Addressing these issues requires a concerted effort to develop comprehensive digital health policies, enhance training, and ensure interoperability of health information systems. These measures are essential for leveraging digital health technologies to improve healthcare delivery and outcomes in Cameroon.
Introduction and background
Digital transformation has recently emerged as a critical tool for enhancing healthcare delivery and health outcomes globally, including in Sub-Saharan Africa and Cameroon. The adoption of digital technologies in healthcare is transforming the delivery of health services, improving access, enhancing the quality of care, increasing accountability, and reducing costs. 1 Cameroon, like most African countries, faces numerous challenges within its health system, including insufficient funding, inadequate infrastructure, and shortages of skilled healthcare workers. Digital transformation presents a unique opportunity to address these challenges and improve health outcomes for millions of Cameroonians. Additionally, if well-implemented, digital technologies provide numerous opportunities to strengthen Cameroon's health system, from minor improvements to radical changes that can help the country address traditional barriers to meeting the population's health needs. This includes the collection, sharing, and use of data, as well as the development of more efficient logistics and supply chains, to improve healthcare and public health for African populations. 2 To ensure adequate service planning and delivery, the use of timely and good-quality health information at different levels in the health system is key, ranging from influencing policy to programming actions and ensuring evidence-informed practices. 3 The Ministry of Public Health (MoPH) in Cameroon uses the District Health Information System 2 (DHIS2) as the official digital platform for monitoring and reporting the country's health data. The DHIS2 is an open-source, web-based platform commonly used as a health management information system (HMIS). Approximately 3.2 billion people reside in countries that utilize DHIS2. Including NGO-based programs, DHIS2 is in use in more than 100 countries. Today, DHIS2 is the world's largest HMIS platform, used by 80 low- and middle-income countries (LMICs). 4 Given that DHIS2 is the official platform for HMIS in Cameroon, the adoption and use of other platforms must align their interoperability with the former. Interoperability will enable seamless data exchange, streamlined workflows, and improved data analysis, ultimately leading to better-informed decision-making and improved healthcare outcomes. This usually is not the case, as most health-related programs/projects implemented using digital health do not ensure that these platforms are interoperable with DHIS2. 5 Cameroon has a well-articulated health sector strategy (HSS) that emphasizes the importance of the availability of quality data. 6 This document, however, does not mention anything regarding digital health. The National digital health strategic plan also highlights the absence of a policy to govern the implementation of digital health in Cameroon. 5 While digital health adoption is expanding globally, evidence on its implementation for data services in Cameroon remains limited. Existing studies focus mainly on disease-specific applications, with little examination of system-wide integration, governance, and interoperability. There is a paucity of research capturing expert perspectives on operational challenges, workforce readiness, and sustainability. This gap limits the ability to inform context-specific strategies for scaling digital health solutions in the country. It is most likely that, in the absence of a governing framework in the country currently, health programs/projects, and startups implementing digital projects have not considered many aspects that would make their projects align with the country's direction, including interoperability. To gain more insight into the current state and potential for digital health implementation in Cameroon, specifically in data management, monitoring, and reporting (Health Information Systems [HIS]), it is important to understand its current state. This includes identifying the common digital platforms that are being used in the country, understanding how these systems function in terms of interoperability with the standard system, and identifying knowledge gaps among users on the various tools. This study aimed to analyze the landscape of digital health implementation for data services in Cameroon, to evaluate the current state, identify challenges and opportunities, and provide actionable insights to support informed decision-making and policy development in healthcare technology. The research specifically focused on the implementation of HIS.
Methods
Study Design: A mixed-method cross-sectional exploratory design was used, involving both a survey and in-depth interviews, and a desk review. A survey questionnaire was used to collect quantitative data, while in-depth interviews were conducted to obtain quantitative data from digital health content experts to assess the current landscape of digital health for data services in Cameroon. A desk review was also conducted to gather insights on existing digital health systems for data services in Cameroon. Data were collected between January and April 2024.
Study Settings: The study was conducted this study in four regions in Cameroon, selected based on regional representation: Extreme North Littoral, Northwest, Center, and the Southwest Regions. The study area was selected due to the sizeable number of health experts who work in those regions, especially in the area of digital health.
Participants: A purposive sampling method was used to select organizations and health facilities. This approach was chosen because the research targeted health experts operating at various levels of the health system. Cameroon's health system operates across four levels: the central level, led by the MoPH, focuses on policy formulation, strategic planning, and oversight; the intermediate level, managed by Regional Delegations for Public Health, adapts and implements national policies at the regional scale; the operational level, encompassing health districts, oversees service delivery, program implementation, and monitoring at the district level; and the peripheral level, consisting of health areas and community health workers, delivers primary healthcare, preventive services, and community engagement. This decentralized structure aims to ensure effective service delivery and alignment with national health goals, but faces challenges such as resource shortages, infrastructure gaps, and inequities in rural service delivery. Participants who did not provide consent to take part in the study were excluded. The respondents were seasoned health and public health experts with extensive and direct experience in implementing and managing digital health initiatives. This high level of expertise ensured the credibility and representativeness of their responses, providing informed and authoritative insights into the research context.
Data collection
The quantitative survey questionnaire collected data on Governance and leadership, Standards and interoperability, Services and Applications, and infrastructure and adoption of digital health. Quantitative data were collected using a semistructured guide that was piloted with five health experts and refined accordingly.
The qualitative interview guide included questions to gain more insight into the current landscape of digital health for data services in Cameroon. The in-depth interviews were done virtually, and coordinated by the principal investigator, and notes were taken in the process while the session was being recorded. The development of both quantitative and qualitative research tools was informed by the World Health Organization (WHO) Global Strategy on Digital Health (2020–2025). 1 It provides a comprehensive framework for leveraging digital technologies to enhance health systems and improve health outcomes globally. The strategy is built on four strategic objectives, including promoting global collaboration, advancing national digital health strategies, optimizing the digital health ecosystem, and integrating digital health to achieve universal health coverage and the Sustainable Development Goals. These objectives emphasize equity, sustainability, innovation, and partnerships to create robust, inclusive, and effective digital health systems.
Strategic Objective 3: Optimizing the Digital Health Ecosystem and Infrastructure is central to creating enabling environments for digital health. It highlights the importance of governance and coordination through effective policies, building interoperable digital infrastructures, fostering innovation, and ensuring the scalability and sustainability of digital health initiatives. The objective also stresses the need for partnerships among governments, the private sector, and other stakeholders to drive adoption and implementation while addressing disparities in access and use. This strategic objective guided the development of our questionnaire for the study. Questions were designed to assess governance frameworks, the alignment of digital health initiatives with national strategies, and the effectiveness of infrastructure, such as system interoperability and secure platforms. The qualitative interview guide was developed to facilitate an in-depth exploration of the same thematic areas. Drawing upon principles from the WHO National eHealth Strategy Toolkit, 7 the guide included questions aimed at uncovering nuanced insights into policy implementation, operational challenges, and strategic opportunities in the digital health ecosystem.
The National Digital Health Strategic Plan 2020–2024 and the HSS 2016–2027 were reviewed, and it also provided insight into the current status of digital health in the country.
Study size: The qualitative design had a total of six (06) Digital Health experts. We applied a saturation principle for data collection. Using Yamane's formula, the quantitative design had a total of 60 Digital Health experts who were selected from the different regions employing the proportionate for size principle.
The key informants for the qualitative study were selected based on their knowledge of the current state of digital health in Cameroon. Six respondents were interviewed.
Data analysis
Quantitative data were input into MS Excel and later exported into SPSS version 26 for analysis. Questionnaires that were less than 85% completed were discarded. Results were represented using frequency tables and graphs. Due to the small sample size (60), the Fisher exact test was used to test for association among variables, and a p-value of 0.05 was used as a cutoff point.
Qualitative interviews were transcribed verbatim and expanded with field notes. Data analysis involved familiarizing oneself with the transcripts through repeated reading, followed by coding concepts identified by the researchers. Thematic analysis was conducted using both inductive and deductive reasoning to identify differences and similarities within codes and categories. The themes were then interpreted and reduced to essential concepts, resulting in four categories informed by the WHO Global Strategy on Digital Health. 1 ATLAS Ti software was utilized for data analysis, matching codes to content, and generating outputs for interpretation. Related codes were grouped into themes. Confidentiality was maintained through participant anonymity and secure data storage.
Ethical approval for the study was obtained from the Faculty of Health Sciences Institutional Review Board of the University of Buea, Cameroon. Participants were fully informed about the study and provided both verbal and written consent before interviews.
Results
Sociodemographic characteristics of the study population (n = 60)
We interviewed a total of 60 participants, 63.3% males and 36.7% females, identified as experts in public health within the Cameroonian context. Participants’ ages were spread across four age groups, with those between 30 and 39 years being the most represented (62%). Fifty percent of respondents were master's degree holders, among other qualifications, with over 37% of the participants currently working in the Centre region of the country. Participants worked across various sectors, including private (33%), international NGOs (38%), and government institutions (23%) (Table 1).
Sociodemographic characteristics of the study population (n = 60).

Six Digital Health Content experts provided more detailed information through in-depth interviews as key stakeholders, 50% males and 50% females.
To present a comprehensive landscape of digital health implementation for data services in Cameroon, we grouped our results into four major themes: Governance and leadership, Standards and interoperability, Services and Applications, and infrastructure and adoption of digital health
Governance and leadership
Governance is the vision and system-level strategy to guide the implementation of digital health across health systems. Governance ensures the policy and regulatory environment of health systems guards’ privacy, security, stewardship, and accountability.
More than three-quarters (85%) of respondents indicated they are not aware of any policies/guidelines from the government or relevant authorities that guide digital health implementation in Cameroon. With regard to assessing perceptions of adequate policy support from the government or relevant authorities for digital health implementation, results were more divided (Table 2A). While 86.7% of respondents overall believed there was no adequate policy support from the government or other relevant authorities, there were statistically significant differences based on academic qualification (f = 16.033,
Correlation of utilization of digital platforms for data services and demographic characteristics.

Correlation of utilization of digital platforms for data services and demographic characteristics.

Feedback from in-depth interviews revealed similar findings as respondents noted that the current policies, guidelines, and strategies around digital health in Cameroon are not sufficient to guide Digital health implementation in the country. Cameroon so far has just a Digital health strategic plan developed in 2021. There is no information so far on the implementation progress of this plan. Currently, Cameroon lacks the policy and frameworks to effectively guide the implementation of digital health in the country [P1]. Very limited normative documents are available to back up digital health implementation, especially for HIV, as most are still under production [P5].
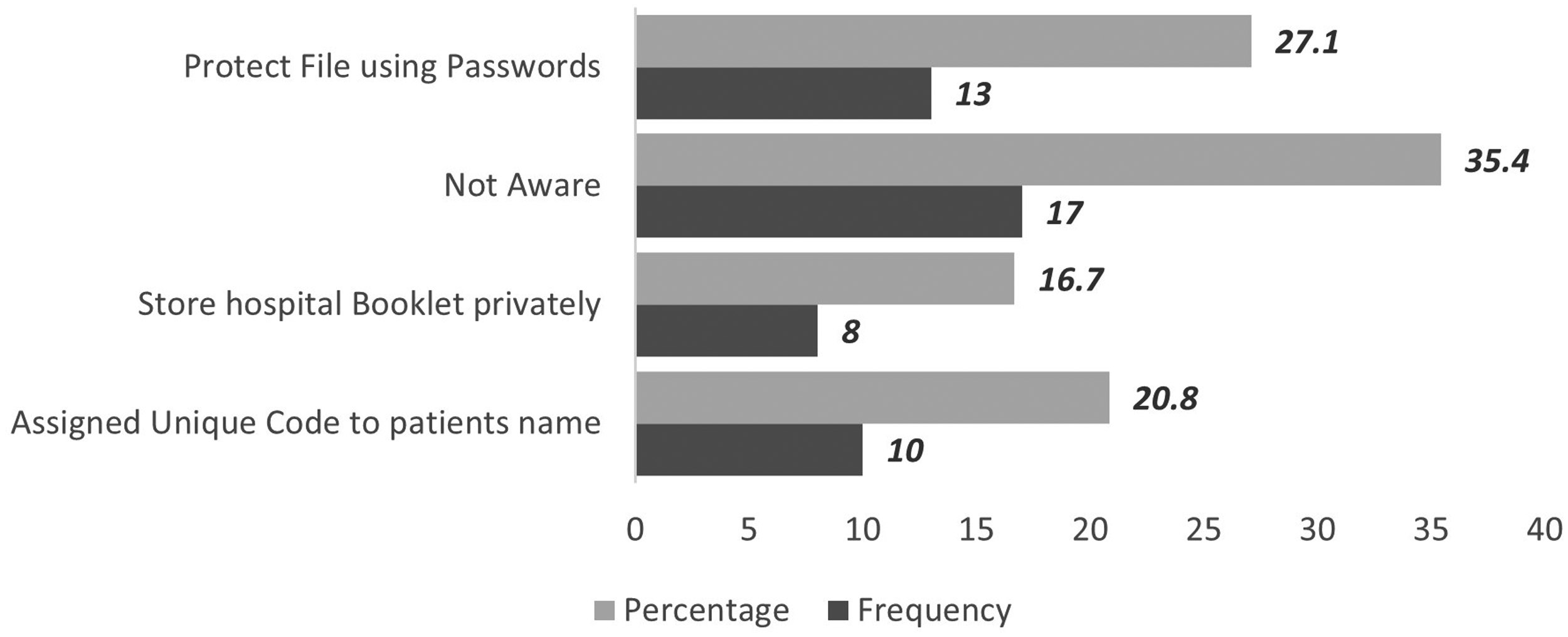
In terms of data privacy and data protection measures, 55% of health experts reported having specific measures in place to protect patient data at their respective workplaces (Table 2B). Among the measures in place, 27% of respondents said that their organization uses the method of password protection, followed by 20.8% who cited unique codes assigned to patients to maintain anonymity. A significant proportion of the respondents, 35.4%, noted that they are not knowledgeable about their organization having or implementing data protection measures (Figure 1).

Measures put in Place to Ensure Data Security.
Respondents from the private sector as well as those from international NGOs were more likely to note that their institutions have specific measures in place to ensure that there is data privacy and data protection (
Standards and interoperability
Most respondents (63.3%) noted that their organization is either currently using or has once used in the past an electronic/digital platform(s) for data services, and they acknowledged they had received formal training on the use of this. The digital platform is primarily utilized for various purposes within the realm of data management and healthcare operations. The majority of its usage revolves around data reporting, constituting 29% of its utilization, followed closely by data collection at 26%. Additionally, data management accounts for 23% of its usage, while data analysis comprises 21% (Figure 2).

Purpose of electronic/digital platforms in organization for data service.
Over 80% of the respondents acknowledged they know DHIS2. Among those who knew what DHIS2 is, 55% of them noted there are no interoperability issues between their respective digital health systems and DHIS2. Respondents operating at the central, intermediate, and operational levels were all found to be significantly more (100%) knowledgeable on how the DHIS2 tool functions, as compared with those operating at the peripheral level (44.4%) (
Participants who acknowledged that they face challenges in interoperability and data exchange between their systems and the DHIS2 noted challenges primarily revolving around technical issues and human factors. Following challenges faced in interoperability, a significant number of respondents from Extreme North (75%) and the Center Region (72%) argued that there exist challenges in data exchange between their system and DHIS2. And this association was found to be significant (
Thirty-eight respondents (63.3%) reported having received formal training on the use of digital platforms, while 22 (36.7%) indicated no training. Gender differences were notable, with a higher proportion of males (73.7%) than females (54.5%) having received training (χ² = 4.781, p = 0.029). Across academic qualifications, training was more common among those with Master's degrees (70.0%) compared to Bachelor's degree holders (18.2%). All respondents with PhDs reported no formal training. At the regional level, significant variation was observed (χ² = 10.696, p = 0.023), with training being more frequent in the Littoral (62.5%) (Table 2B).
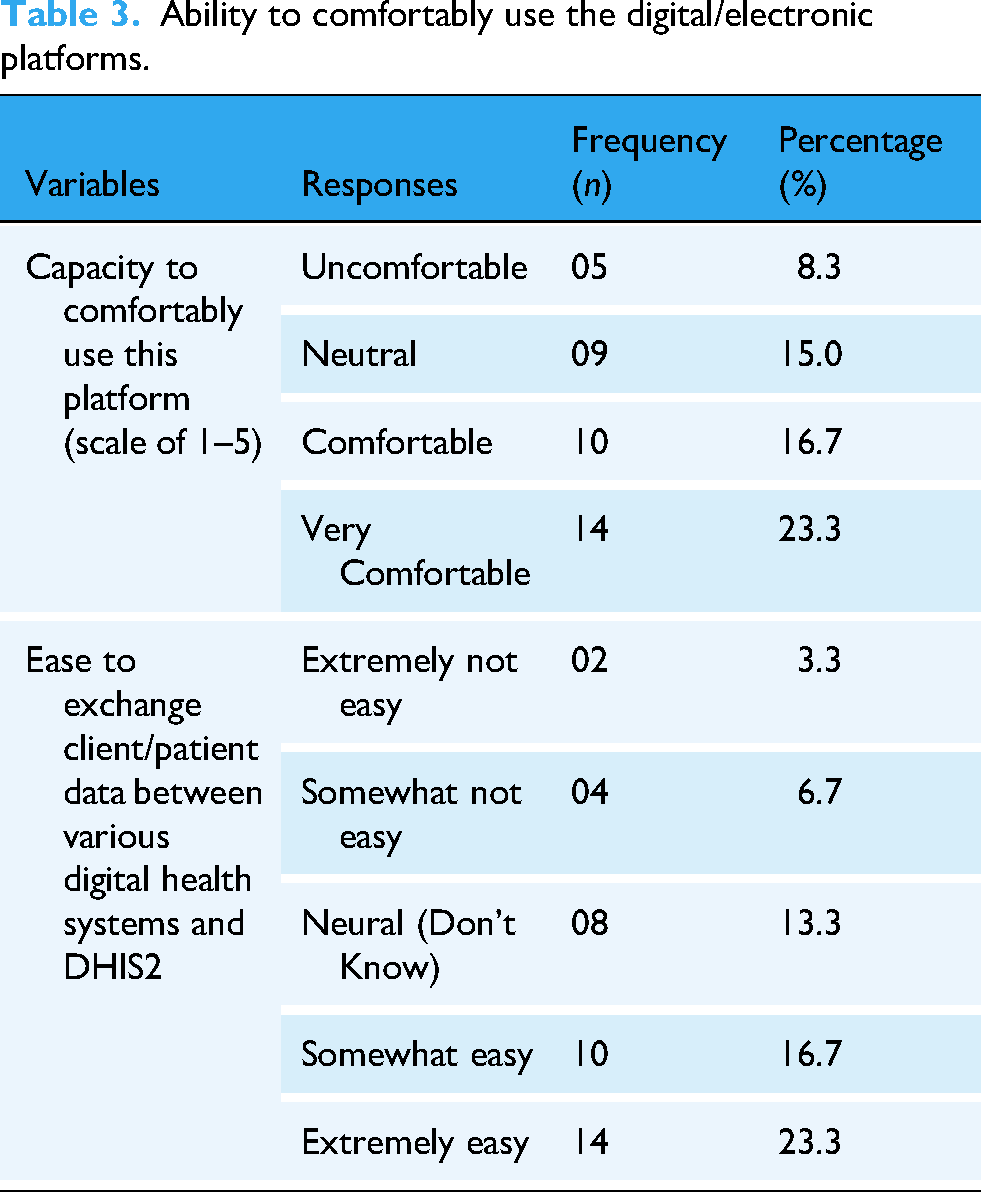
A good number of respondents, 23.3%, rated themselves as being “very comfortable” in using the digital health platforms. A total of 8.3% expressed the unfriendly nature of electronics/digital platforms, noting that they feel uncomfortable using digital platforms.
Concerning the ease of data exchange between their organization and the DHIS2 tool, most of the participants, 23% and 17%, noted that the data exchange was extremely easy and somewhat easy, respectively (Table 3).
Ability to comfortably use the digital/electronic platforms.
Feedback from in-depth interviews with key stakeholders noted various perspectives regarding interoperability “In terms of health, interoperability can improve the quality and efficiency of health care delivery, increase access to health information and services, enhance patient safety and satisfaction (with feedback mechanism), also improve public health decision-making.” (Participant P1.)
This response was further supported by Participant P4, who added that; “Interoperability allows for an electronic system to have like a seamless communication, that is to say, the data flow between systems is very efficient and it's very cost-effective because there is no room for manual transfer of health data and equally there is no need to have like a build in the platform through which data would be manually transmitted. It is also necessary for the continuity of care. For instance, when a patient leaves from one health facility to another, it is easy to pull up some basic info about that person and then continue care from where the previous hospital stopped. It also assists in public health monitoring where health data aggregate is easily pulled out from several different sources to ease decision making.”
On their thoughts on whether interoperability is being considered by developers or organizations that introduce new Systems for data services in Cameroon, we had several respondents who answered “yes,” acknowledging the fact that it has been considered. Participant P5, for instance, shared his views as follows. “In Cameroon, I think interoperability is being considered by developers and organizations. For example, Organization xx right now is using Dama and EMR but then there are still limitations when it comes to the extent to which those systems are interoperable, In the sense that certain patient-level info is identical in both sources but they have different names, so it is difficult to have like aggregate of same data from both sources, so I think it's been considered right now since EMR is in a pilot phase. So yes, I think it's been considered by developers and organizations.”
However, some respondents felt otherwise, as P4 stated: “Since the digital health environment is still at the conception stage in the country, most systems piloted don’t consider interoperability as a key aspect as they focus mainly on developing systems that meet the immediate needs of the respective projects.”
Services and applications
The innovative approach in information and communication technology (ICT) considers the need for policy interventions in purchasing infrastructure as the key to the successful implementation of eHealth systems. Figure 2 shows a graphical response of participants regarding the type of Electronic/Digital Platforms used by their organization for data services. Results showed that the DHIS2 platform is the most used 26.3% platform for data services within organizations,
A review of applications in use and in-depth interviews provided more information regarding various applications and services currently being used in Cameroon. Table 4 presents a comprehensive overview of various digital health systems deployed across Cameroon, encompassing a range of interventions and functionalities to support healthcare delivery. These systems include:
Open Medical Record System (OpenMRS) and GNU Health for electronic medical records (EMR), OpenMRS and GNU Health are open-source HIS designed to enhance healthcare delivery, particularly in resource-limited settings. OpenMRS focuses on EMRs and provides a modular platform for managing patient data, encounters, and reporting, making it highly adaptable to various healthcare contexts. Its global community supports implementations in areas such as HIV care, tuberculosis treatment, and maternal health, especially in LMICs. OpenMRS excels in integration and flexibility, enabling healthcare facilities to tailor the system to their specific needs. GNU Health emphasizes a holistic approach by integrating clinical, social, and demographic data into a comprehensive health and hospital management system. It supports modules for hospital operations, public health, and epidemiology, making it suitable for larger-scale health systems and public institutions. DHIS2 COVID-19 Tracker, a digital tool developed to support real-time data collection and management for pandemic response. It enables case-based surveillance, contact tracing, vaccination monitoring, and analytics, helping health systems track COVID-19 cases, monitor interventions, and generate actionable insights PlaCARD (Platform for COVID-19 Analytical Research and Decision-making) is a digital solution that streamlines and manages COVID-19 data flow. It provides an integrated platform for collecting, analyzing, and visualizing data to support pandemic response efforts. Designed to enhance data-driven decision-making, PlaCARD consolidates information from various sources, including case surveillance, laboratory testing, hospitalizations, and vaccination programs. CommCare, a mobile-based application designed for program monitoring, particularly in health and social services. It enables frontline workers to collect, manage, and analyze data in real time using mobile devices, even in remote or resource-limited settings.
Scoping of existing digital health systems for data services in Cameroon.

Other systems focus on specific areas such as TB surveillance, HIV/AIDS, and health research. Compatibility with DHIS2, custodianship, and health system levels vary across the systems, reflecting the diverse landscape of digital health infrastructure in Cameroon (Table 4).
Infrastructure and adoption of digital health
Infrastructure refers to both physical technology and platforms or digital services that support information sharing within the health sector. In terms of health structures equipped with ICT at the national level, the review of documents revealed that only 32.1% of health facilities have their computers, while 16.8% use private computers, with internet access limited to 27% of health facilities. Concerning information and communication, private mobile phones purchased by staff but used by the health facility are the most used means of communication by health facilities (52.7%), followed by mobile phones belonging to the facility (33.2%), and private mobile phones with airtime paid for by the health facility (23.1%). This information was supported by an ICT focal person working at the central level of the Ministry of Health.
Qualitative feedback on the current situation of Infrastructure with regard to digital health in Cameroon, we had all respondents stating that there are indeed gaps concerning the state of digital health infrastructure in Cameroon, “There are still some gaps with regard to the infrastructural capacity of Cameroon to effectively accommodate digital health in the country. These gaps include Insufficient internet coverage nationally, insufficient coverage of electricity, lack of qualified Human resources as well as equipment at the operational” (Respondent P2)
Equally, we had most respondents saying the government has not adequately invested in Digital Health in the country. For example, P3 stated that “Given its importance, and considering the role it can play in transforming the health sector, the government has not adequately invested in digital technology.”
Participant P4 further added: “Yes, but not adequately, because we still have lots of gaps in our digital health system, and it's not being implemented/promulgated across all the health services. “It still not possible to track an HIV client from any hospital, other than the clients’ primary care hospital, in Cameroon.”
Assessing the perspective of the level of adoption of digital health technology for data services in Cameroon, data showed that the level of digital health technology adoption among the users is predominantly rated positively. Most respondents (59%) rated the adoption at level 3, indicating a moderate level of adoption. Additionally, 30% of respondents rated it at level 4, representing a relatively high level of adoption. There were fewer ratings at levels 1 and 2, comprising 2% and 9% of responses, respectively (Table 5).
Adoption of digital health technology among users.

For this study, the levels of digital health technology adoption among users can be interpreted as follows:
Low Adoption (1): Minimal or no use of digital health technologies, reflecting limited engagement or knowledge. Limited Adoption (2): Some use of digital tools, but it is inconsistent or limited to basic applications. Moderate Adoption (3): Regular use of digital health technologies for specific tasks such as data collection or communication. High Adoption (4): Advanced and consistent use of multiple digital health technologies, demonstrating significant integration in workflows. Very High Adoption (5): Comprehensive and integrated use of advanced digital health systems, showcasing leadership and innovation.
The challenges associated with the adoption of digital health technologies are multifaceted. Firstly, cost presents a significant barrier, particularly in low-resource settings or for individuals with limited financial resources, as highlighted by 19% of respondents. Security concerns regarding the privacy and confidentiality of personal health information (through the use of personal gadgets by some staff to report patient data), if not adequately addressed, constitute another challenge, noted by 4% of respondents. Integration issues with existing health systems and workflows, leading to compatibility issues and data fragmentation, were cited by 10% of respondents. Additionally, the generation of large amounts of data by digital health technologies, without adequate mechanisms for interpretation and actionability, poses challenges, as mentioned by 5% of respondents. Lack of training and education among healthcare professionals, affecting their effective use of digital tools, was reported by 23% of respondents. Connectivity issues, relying on reliable internet access, were highlighted by 19% of respondents. Lastly, cultural and mindset barriers, such as resistance or skepticism towards technology among health providers or patients, were cited by 17% of respondents (Figure 3).
Reasons for poor adoption of digital health technology.
Discussion
The findings highlight significant gaps in the governance and leadership framework, inadequate infrastructure, and interoperability issues that hinder effective digital health implementation, essential for the effective implementation of digital health services in Cameroon.
Governance and leadership
Governance, which includes the vision and system-level strategy for digital health, plays a pivotal role in ensuring that health systems protect privacy, security, stewardship, and accountability. Our data reveal a considerable lack of awareness and perceived inadequacy in policy support for digital health implementation among stakeholders, particularly those with higher academic qualifications and those working at central levels, where a significant portion (86.4%) acknowledged the absence of such policies. This aligns with findings by Elkhwsky et al., who note that most LMICs still currently lack governance guidance/regulation; thus, long-term leadership and support at a very high level are necessary for them to succeed in the endeavor of integrating digital health. 8 There, however, exists a National Digital Health Strategic Plan (2020–2024). 5 The strategic plan, notwithstanding, is not backed by any policy or framework within the country. The lack of leadership and specific mention of digital health in the National HSS 2016–2027 for Cameroon indicates a gap in policy support. Al Meslamani, in his paper explaining why digital health policies are crucial, notes the importance of policies to guide digital health implementation, taking into consideration the country's context. 9
Additionally, results indicate a strong perception of inadequate policy support for digital health, more pronounced among those with a Master's degree (100%) and central-level workers (90.9%). Despite the development of the Digital Health Strategic Plan in 2021, limited information on its implementation progress and the lack of comprehensive policies hinder effective digital health initiatives, especially in specific areas like HIV, where normative documents are still under development. Cameroon's National Digital Health Strategic Plan (2020–2024) lacks binding regulations requiring system conformity to a defined interoperability standard. Without legal or regulatory compulsion, vendors and implementers default to minimal integration work. These findings align with the work by Marcelo et al., who, in the conceptualization of a digital health framework for Asia, highlight the slow adoption of ICT governance. 10
Data privacy and protection measures are another critical aspect of digital health governance. While 55% of health experts reported having specific measures in place at their workplaces, there is considerable variability in the types of measures employed. Password protection (27%) and using unique patient codes (20.8%) are common methods, but over 35.4% of respondents indicated a lack of knowledge about their organization's data protection measures. Although the National HSS's successful implementation relies on its digital component, it's crucial to highlight that utilizing digital technology comes with potential privacy and individual freedom concerns, given the absence of comprehensive digital health legislation in Cameroon. The strategic plan, however, highlights that Cameroon has some legal and regulatory instruments that regulate ICT, including Decree No. 2012/180 of 10 April 2012 on the organization and functioning of the National Agency for Information and Communication Technologies (ANTIC). The mission of ANTIC is to regulate, control, and monitor activities related to the security of information systems and electronic communication networks, as well as electronic certification, in collaboration with the Telecommunications Regulatory Agency, and promote ICTs. The document goes further to indicate the absence of a regulatory and ethical framework for the implementation of digital health interventions and also the absence of instruments that guarantee confidentiality and the right to privacy. 5 No single authority (e.g., ANTIC or MoPH ICT unit) has the mandate or resources to certify digital health solutions for interoperability compliance. This leads to parallel development of siloed platforms without central review or accreditation processes. A similar situation exists in Jordan, according to Nemer et al., who noted that the increased use of digital systems is, however, not accompanied by clear regulatory policies, especially when it comes to privacy and security of personal data, and how these data are governed. 11 A multifaceted approach, including policy development, stakeholder engagement, education, and infrastructure development, can be key to supporting a secure and effective digital health ecosystem for data services in Cameroon.
Standards and interoperability
The effective implementation of digital health platforms is fundamentally dependent on adherence to standards and the interoperability of systems, both of which are underpinned by the capacity of health workers to competently use these tools. In LMICs such as Cameroon, variability in training, infrastructure, and institutional coordination often results in fragmented digital health ecosystems, where systems operate in silos and fail to achieve their intended impact. 1 Building workforce competencies through structured training is, therefore, not only a critical enabler of data quality and system functionality but also a prerequisite for achieving interoperability across platforms and alignment with global digital health standards. 12
The observed finding that 63.3% of respondents reported having received formal training on digital platforms, together with significant variation by gender, qualification, and region, aligns with existing evidence that capacity-building is a key determinant of routine HIS (RHIS) performance and digital tool uptake in LMIC settings. Studies from Cameroon and comparable LMIC settings have shown that facility and programme units that receive dedicated training on DHIS2 and related HIS tasks demonstrate better completeness, timeliness, and data-use practices, reinforcing the functional importance of formal training for system performance.13,14 The gendered pattern we observed (higher proportion of trained males) is consistent with broader analyses of the digital health ecosystem, which document a persistent “digital gender gap” in access to digital tools, skills, and career opportunities; these structural inequities frequently translate into differential access to training unless explicitly addressed by policy. 15 evidence on capacity-building modalities indicates that blended and virtual training approaches (including scalable e-learning) can effectively expand reach and sustain competencies among health workers in LMICs, suggesting pragmatic avenues to close the observed regional and qualification-related gaps, while noting that effectiveness depends on quality of instructional design, mentorship/supervision, and local infrastructure. 16
Interoperability ensures that different health applications can communicate seamlessly, facilitating the secure exchange of data and enabling value-added services. A significant portion of organizations (63%) currently use or have used electronic platforms for data services, primarily for data reporting (29%), collection (26%), management (23%), and analysis (21%). Despite the widespread use of these platforms, challenges in interoperability persist, impacting the efficiency of health data utilization.
Participants with PhD-level education were more likely to be associated with organizations using electronic platforms and demonstrated higher knowledge of the DHIS2 system. This suggests a correlation between higher academic qualifications and familiarity with digital health systems, indicating the need for broader training initiatives to close the existing capacity gaps. The National Digital Health Strategic Plan emphasizes the importance of technical interoperability to enhance the efficiency of health services. However, significant regional disparities exist, with respondents from the Littoral and Centre Regions more frequently using digital platforms. Over 80% of participants are aware of DHIS2, with 55% reporting no interoperability issues. Yet, significant challenges remain, especially in regions like the Extreme North and Centre, where technical issues and human factors hinder data exchange (75% and 72%, respectively).
Interoperability is essential for improving healthcare delivery, patient safety, and public health decision-making. Feedback from in-depth interviews supports this, highlighting the benefits of seamless data flow between systems. However, challenges such as system crashes, slow loading times, poor internet connectivity, and a lack of offline capabilities with DHIS2 impede effective data sharing. These findings align with the WHO's emphasis on interoperability to support integrated health service delivery and enhance health system efficiency. 1 The National Digital Health Strategic Plan 2020–2024 also calls for the development of standards to ensure systems can communicate effectively, yet the implementation appears incomplete, with many health facilities still experiencing significant interoperability issues. 5 Existing guidelines 5 mention “interoperability” in broad terms but provide no detailed technical specifications (e.g., required API endpoints, authentication schemas, data dictionaries). As a result, local developers lack clear reference implementations or test suites.
Services and applications
Although at its initial stages, the landscape of digital health for data services in Cameroon is diverse and reflects the strategic priorities outlined in the National Digital Health Strategic Plan. This plan highlights the importance of policy interventions in purchasing infrastructure as crucial to the successful implementation of eHealth systems. 5 Study results show that the DHIS2 platform is the most widely used for data services. This aligns with its popularity in developing countries, as over 80 LMIC currently use DHIS2. 4 This widespread adoption can be attributed to DHIS2's versatility and strong endorsement by the MoPH as the national standard for health information management.
In-depth interviews and the review of literature further revealed a comprehensive range of digital health systems deployed across Cameroon, each tailored to specific health needs and interventions. For instance, OpenMRS and GNU Health are pivotal in managing EMR for HIV and TB care, indicating their critical role in chronic disease management. The DHIS2 COVID-19 Tracker and PlaCARD are essential for pandemic response, demonstrating the adaptability of digital health platforms for data services in addressing emergent public health crises. Additionally, mobile-based applications such as CommCare facilitate program monitoring and data analysis at the community level, highlighting the importance of mobile technology in extending healthcare services to remote and underserved areas. The positive effect of digital systems for data services is shown in the work by Tchatchueng et al., who noted a decreased median turnaround time for providing COVID-19 results after the introduction of SMS result notification in PlaCARD. 17
These findings align with the WHO’s Global Strategy on Digital Health 2020–2025, which advocates for the harmonization of digital health initiatives and the establishment of interoperable systems to enhance health outcomes and service delivery. 1 The diverse digital health applications in Cameroon, while reflecting a fragmented landscape, bring to attention the need for continued efforts to achieve interoperability and integration. By aligning with global digital health strategies, the MoH can strengthen its digital health infrastructure, promote data-driven decision-making, and ultimately improve healthcare delivery and outcomes across the country.
Infrastructure and adoption of digital health for data services
The infrastructure and adoption of digital health in Cameroon present a landscape marked by significant challenges and some progress, as highlighted in the National Digital Health Strategic Plan. Despite the plan's emphasis on strengthening digital health infrastructure, our study reveals that only 32.1% of health facilities possess their own computers, and internet access is available in just 27% of these facilities. Kozlakidis and Sargsyan allude that the lack of infrastructure is a consistent parameter of operating within LMICs, and equally for supporting digital health advancements. 18 This lack of basic ICT infrastructure is compounded by the fact that private mobile phones, often purchased by staff, are the primary means of communication within health facilities. This scenario highlights the infrastructural gaps that could hinder the effective implementation and utilization of digital health technologies for data services in Cameroon.
Qualitative feedback from stakeholders further accentuates these infrastructural deficiencies. Respondents consistently pointed out the insufficient national coverage of internet and electricity, the lack of qualified human resources, and inadequate equipment as major obstacles. This sentiment was reflected in statements highlighting the government's underinvestment in digital health, which has impeded the comprehensive rollout of digital health systems across all health services. For example, the inability to track HIV patients across different hospitals indicates significant gaps in the interoperability and integration of HIS, a critical component emphasized in both the national strategic plan and WHO's Global Strategy on Digital Health 2020–2025.1,5
Despite these challenges, the level of adoption of digital health technologies for data services shows moderate to relatively high acceptance among users. Our data indicate that 59% of respondents rated the adoption level at 3, while 30% rated it at 4. This positive trend is encouraging; however, several barriers still impede wider adoption. These include the high cost of digital technologies, security concerns regarding personal health information, integration issues with existing systems, and a lack of training for healthcare professionals. Connectivity issues and cultural resistance also pose significant hurdles. Addressing these challenges requires a multifaceted approach, aligning with the strategic priorities outlined in the National Digital Health Strategic Plan and supported by WHO guidelines, to build a resilient and inclusive digital health ecosystem in Cameroon.
Recommendations to enhance the adoption of Digital Health for data services in Cameroon.
Infrastructure and Connectivity: To support the effective implementation of digital health initiatives, addressing infrastructural challenges is paramount. This includes improving internet connectivity and providing access to adequate digital devices (such as laptops and desktops). A consistent maintenance and upgrade system should be established to prevent disruptions in service delivery. Investing in these areas will create a foundation for the successful adoption of digital health systems. Governance and Leadership: Strong leadership and political commitment are crucial to advancing the digital health agenda. The government must play a central role in leading and coordinating digital health initiatives, supported by clear and robust policies, regulations, and frameworks. This should be coupled with adequate funding and resource allocation to ensure the successful implementation and monitoring of digital health strategies. Public and Private Sector Collaboration: Due to existing parallel digital systems, building collaborations among various stakeholders, including public health institutions, private organizations, and local NGOs, is key to creating a unified approach to digital health. The government should encourage private sector involvement and ensure that public–private partnerships are aligned with national health priorities. Interoperability: Creating interoperability guidelines for digital health platforms and systems is critical to ensuring smooth data flow and integration. This will allow the digital health system to offer accurate and timely information, supporting effective disease management and epidemiological surveillance. Data Privacy and Security: Sensitization campaigns should address data privacy and security concerns, promoting awareness among both healthcare workers and the public. The development of clear policies and frameworks to protect patient data will foster trust and encourage the adoption of digital health systems. Policy and Resource Support for NGOs: Recognizing the role of local NGOs and private health facilities is important. While some private facilities have adopted digital health solutions, they often revert to traditional methods due to policy and infrastructural challenges. Therefore, policies should be designed to support and incentivize digital health adoption among private and nongovernmental organizations, ensuring alignment with national health objectives.
Future impact analysis
As Cameroon continues to implement policies and improve infrastructure for digital health, the potential impact of increased digitalization could be transformative. With enhanced connectivity, robust training, and streamlined governance, digital health systems for data services have the capacity to revolutionize healthcare delivery, making it more efficient, accessible, and data-driven. Improved data management will enable better tracking of diseases, more accurate diagnoses, and timely interventions, ultimately reducing morbidity and mortality rates. The integration of digital tools will foster a more collaborative health ecosystem, promoting partnerships between the public and private sectors, and empowering local communities with real-time health information. As these systems evolve, Cameroon could set a regional example for digital health innovation, improving health outcomes while ensuring the sustainability of healthcare services for future generations.
Conclusion
The landscape of digital health for data services in Cameroon, as highlighted by the study, reveals significant infrastructural and governance challenges that prevent or slow down the full implementation and utilization of digital health technologies. Even with the multiplicity of digital systems such as OpenMRS and DHIS2, and their moderate to high adoption rates, there are still significant gaps in internet connectivity, policy support, and skilled personnel. To support an integrated and successful digital health ecosystem in Cameroon, these findings highlight the necessity of an integrated approach that includes strong policy frameworks, increased infrastructure investment, and extensive training programs that are in line with the major strategic documents currently in place.
Study limitations
Potential Response Bias: Given that the study relies on self-reported data from participants, there is a risk of response bias. Some participants may have provided socially desirable answers or may not accurately recall details about digital health policies or implementation in their respective organizations. To address this, researchers implemented strategies such as ensuring participant anonymity to encourage honest responses and providing clear and concise questions to reduce ambiguity.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251395551 - Supplemental material for Assessing the landscape of digital health implementation for data services in Cameroon
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251395551 for Assessing the landscape of digital health implementation for data services in Cameroon by Frankline Sanyuy Nsai, Palle John Ngunde, Anna Longdoh Njunda, Nicholas Tendongfor, Cho Sabastine Anye, Juliet Nabyonga-Orem and Omer Njajou in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to express our sincere gratitude to all the participants who contributed to this study. Your willingness to share your experiences, insights, and time was invaluable to the success of this research.
ORCID iDs
Ethics statement
Ethical approval for this study was obtained from the Institutional Review Board of the Faculty of Health Sciences, University of Buea, Cameroon, Ref: 2020/1241-06/UB/SG/IRB/FHS.
Contributorship
(I) Conception and design: F.S.N., O.N., A.L.N., P.J.N.; (II) Administrative support: F.S.N., O.N., N.T.; (III) Provision of study materials or patients: F.S.N.; (IV) Collection and assembly of data: F.S.N., O.N., C.S.A., JNO; (V) Data analysis and interpretation: F.S.N., O.N., C.S.A., JNO; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest related to this study. Specifically, there are no financial, personal, or professional relationships that could inappropriately influence or appear to influence the conduct, analysis, or reporting of this research. The authors affirm that they have not received any funding or support that could present a potential conflict of interest. Furthermore, none of the authors serve on the editorial board of the journal to which this manuscript has been submitted.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.