
Abstract
Background
Globally, health information systems have been improved by District Health Information System Version 2 (DHIS2), which promotes consistency and integrity in collecting data, processing, and utilization. This success has been attributed to its user-friendly interface and incorporation of advanced data analysis and validation features.
Objective
This study aimed to assess DHIS2 data utilization among health professionals working at private hospitals in the Amara region.
Methods
An Institution-based cross-sectional study design was conducted from 9 May to 30 June 2022. A simple random sampling technique was used to select participants, with a total of 395 health professionals participating. Data was collected using a self-administered paper-based questionnaire. Data entry was performed using the Kobo Collect tool, and data analysis was conducted using STATA version 14.0. Bivariable and multivariable logistic regression analyses were used and p < .05 with a 95% CI was considered to measure statistically significant variables.
Result
Out of 395 participants, about 37.72% of the participants had good DHIS2 data utilization. Had good data analysis skills (adjusted odds ratio (AOR) = 6.5, 95% CI [3.1–13.8]), regular supportive supervision and feedback (AOR = 5.2, 95% CI [2.8–9.5]), monthly salary > 5000 ETB (AOR = 2.0, 95% CI [1.1–3.7]), ease of use (AOR = 5.4, 95% CI [2.8–10.2]), and district health information system training (AOR = 4.2, 95% CI [2.2–7.3]) were enabling factors for utilization of DHIS2 data.
Conclusion
Private healthcare providers had limited utilization of DHIS2 data. It is highly recommended to provide DHIS2 training, supervision, and feedback focused on private health facilities. Additionally, enhancing data analysis skills and prioritizing ease of use are crucial to improving DHIS2 data utilization.
Background
The completeness, accuracy, and timeliness of data production and use are vital for quality healthcare services. 1 However, quality data generation and utilization remains limited in low- and middle-income countries. 2 As a result, the quality of healthcare services is also challenged due to the absence of evidence-based decision-making, which has direct implications for the quality of patient care.3–5 Evidence-based decision-making, which is a unique aspect of modern healthcare services, is crucial to the healthcare system. 6 It improves patient outcomes, establishes the standard of care, enhances resource utilization, informs policy development, and encourages transparency and accountability.7–12 The foundation for providing excellent patient care is successfully utilizing healthcare data. 13 One of the building blocks of the health care system is the health information system (HIS), which is essential for planning, prioritizing issues, improving the standard of patient care, and making decisions based on scientific evidence.14–17 Additionally, healthcare budgeting and planning rely on the availability and use of strong health information. 18 Strong HIS driven by the digital health system to monitor and enhance the use of patient-centered, evidence-based healthcare services. 19 In particular, District Health Information System Version 2 (DHIS2) has enhanced overall data management capacity. 20 Globally, health information systems have been improved by DHIS2, which promotes consistency and integrity in collecting data, processing, and utilization. 21 Currently, DHIS2 has become known as the world's largest digital health platform, having been utilized by more than 80 low and middle-income countries.22–25
The study showed that data completeness from DHIS2 reports reached 100%. However, in the manual-based system from 33% to 66%. 26 DHIS2 provides the foundation for making evidence-based decisions across all healthcare systems by offering dynamic data entry, user-friendly interfaces, strong data validation, role-based accessibility, powerful data analysis and quality control capabilities, and an open platform that facilitates offline and online use. 27 DHIS2 has enabled more effective healthcare data analytics and utilization in an easily manageable way, saving time for healthcare providers at all levels up to higher-level managers. 28 Approximately 92.7% of government organizations worldwide reported data in the DHIS2 system. In contrast, only 15.3% of private facilities made use of the same reporting system. 29
Ethiopian Ministry of Health has been implementing a national digital health software called DHIS2 since 2017.3,30
District Health Information System 2 is referred to as DHIS2. Health data is collected, validated, analyzed, and presented using this free and open-source software platform in both offline and online environments. 31
Studies demonstrate that DHIS2 is more effective than the traditional data management system in the eyes of health care professionals. 32 Reportedly raised questions across health data in low- and middle-income nations, including Ethiopia, lack of timelines, and completeness. 2 A study conducted in Nepal revealed that DHIS2 has the ability to enhance the accuracy and timeliness of health data reporting. 2
The acceptance of digital systems is ensured by their quality, ease of use, and usefulness for end users. 33 The reliable, precise, and productive use of information in healthcare systems has been enhanced by DHIS2. 34 This success has been attributed to its user-friendly interface and incorporation of advanced data analysis and validation features like geographic information systems (GIS), user-specific dashboards, and scorecards with pivot tables. 35
Moreover, DHIS2 has verification techniques built into the system that aid in detecting and reporting possible errors, and improve data quality and data integrity. 36 A technique called data audit trail and data validation. 37 An audit trail in DHIS2 refers to a system that detects and documents all actions and modifications done inside the DHIS2 platform. 38 Even though DHIS2 is the cornerstone for enhancing healthcare systems, Ethiopia still faces significant challenges in utilizing DHIS2 to its maximum capacity. 21 In Ethiopia, the utilization rate of DHIS2 in public health facilities ranges from 57.3% to 70.3%, which is indicating a good level of usage.39,40 However, in private facilities it is currently low at 36%. To address this, the Ethiopian Ministry of Health has planned to increase the proportion of DHIS2 from 36% to 50% within the period of 2024 to 2026. 41
Technical challenges, a lack of power backup, unreliable internet access, insufficient training, a lack of digital health competent workers, a lack of resources, lack of information use culture, a lack of security policies and procedures, lack of motivation, lack of supportive supervision, and a lack of organizational support are some of the factors causing low DHIS2 utilization.42–46
The other factor is that the Ethiopian government prioritizes public health facilities over private ones when it comes to DHIS2 training, monitoring, and supervision.39,44 The usability of DHIS2 is crucial, as it includes cost-saving benefits by reducing expenses related to paper and other manual processes, and life-saving advantages by minimizing data entry and processing errors. This reduces the likelihood of incorrect decisions in patient management, ultimately improving effectiveness and efficiency from the individual to the organizational level.47,48
According to our research skills, there are limited published studies on the extent of DHIS2 data utilization in private health facilities in Ethiopia. This study aims to assess the utilization DHIS2 data in private hospitals in the Amara Region.
Methods
Study design and setting
An institutional-based cross-sectional study was conducted. Amara region is one of the regions from 12 regions of Ethiopia. The capital of the region, Bahir Dar is located 552 km from Addis Ababa, the capital of Ethiopia.
According to the planning department of the regional health bureau report, there are 3560 health posts, 874 health centers, 86 public hospitals, 12 private hospitals, and 1301 clinics (all types), and an estimated total population of 23,215,999 which is 11,646,296 (50.1%) female and 11,569,703 (49.9%) male based on the central statistical agency data 2022. 49
Eligibility criteria
The study included health professionals who were permanently working for 6 months or more in private hospitals, as they are considered permanent in the Ethiopian context after this duration. Health professionals who were seriously ill were excluded from the study.
Sample size determination and sampling procedure
The sample size was calculated using a single population proportion formula, considering the following assumptions:

There are 12 private hospitals in the Amhara region, namely Weizero Sihin, Ayu, Nur, Yifat, Selam, Bati, Ethio, Ibex, Dream Care, GAMBY, Adinas, and Afilas Hospital. To ensure proportional allocation, individual participants were selected from each hospital based on the total number of healthcare providers in each hospital. Individual participants from each private hospital were selected using a simple random sampling method from the administrative health workers’ list of records, see Figure 1.

The sampling procedure of district health information system 2 data utilization among health care professionals at 12 private hospitals found in Amara region, Ethiopia/2022.
Study variables and operational definitions
Dependent variable
The dependent variable for this study was DHIS2 data utilization.
Independent variable
Sociodemographic variables (age, sex, profession, year of service, educational status, and salary)
Organizational and behavioral variables (supportive supervision, training, availability of computer, internet availability, printer availability, budget, separate room for DHIS2, availability of reference material/manual)
Technical variables (skill of DHIS2, ease of use, data analysis skills).
Operational definitions
Data collection procedure and quality assurance
After conducting a comprehensive analysis of relevant literature and obtained necessary permission from copyright holders, a self-administered paper-based questionnaire was utilized. The questionnaire, which was adapted and modified from various literature sources.3,6,39,44,46,50 In total, 39 questions were collected from respondents, six questions on sociodemographic characteristics, 16 questions about organizational and behavioral characteristics, nine questions about technical characteristics, and eight questions about utilizing DHIS2 data.
Data quality assurance
Training was given to seven data collectors and three supervisors for 2 days on how to approach study participants, objective, content, and rationale of the study including research ethical principles and how to use the questionnaire. Properly designed and pretested questionnaires were used. Continuous supervision is made to control the data collection procedure. After data collection, questionnaires were reviewed and checked for completeness and the data was cleaned to check for errors and missed values, and any errors were corrected.
The questionnaires were utilized in this study once they had been validated from previous studies.39,44 The pretest was conducted in Tezena Hospital among 42 health workers (10%) of the sample. The internal consistency for each dimension of the data collection instrument was checked using Cronbach's alpha the result was greater than 0.8.
Data management and statistical analysis
After collection the data were downloaded from the Kobo collect tool as a form Excel extension and checked, and cleaned in Excel to identify errors, incompleteness, and missing, data, and corrections were made based on assessing original questionnaires. Then it exported to Stata 14 for statistical analysis.
All descriptive analysis was computed using Stata Version 14.0 software. Preliminary data analysis was conducted to describe the study sample via the mean, median, and frequency. Bivariable and multivariable logistic regression was fitted to identify factors associated with the outcome variables. A variable that has a p-value less than .2 in bivariable analysis was used for multivariable logistic regression.
To evaluate multicollinearity, the mean value of the variation inflation factor was calculated, with a threshold set at 10. The analysis revealed no evidence of multicollinearity among the predictor variables. The fitness of the model was assessed using the Hosmer-Lemeshow Test, which indicated a good fit for the data.
Results
Sociodemographic characteristics
A total of 395 healthcare providers participated in the study, with a response rate of 96%. Two hundred forty-one (61.1%) of the respondents were female health workers. Regarding the professional categories, the majority of the respondents were 251 (65.3%) nurses. In terms of the level of education, about 261 (66%) of the respondents were bachelor of science (BSc) and above (Table 1).
Sociodemographic characteristics of private health professionals on utilization of DHIS2 data in Amara regional state, north west Ethiopia, 2022.

DHIS2: district health information system 2.
Organizational and behavioral factors
Three-quarters 318 (80.5%) of participants have DHIS2 units. Approximately half of participants 195 (49.37%) of the participants had ICT equipment availed for DHIS2 in the workspace. A majority of 299 (75.7%) healthcare professionals had computer training and 174 (44%) had DHIS2 training as well. Of 147 (37.3) healthcare workers, DHIS2 data use supervision was given (Table 2).
Organizational and behavioral characteristics of private health professionals in Amara region, Ethiopia, 2022 (n = 413).
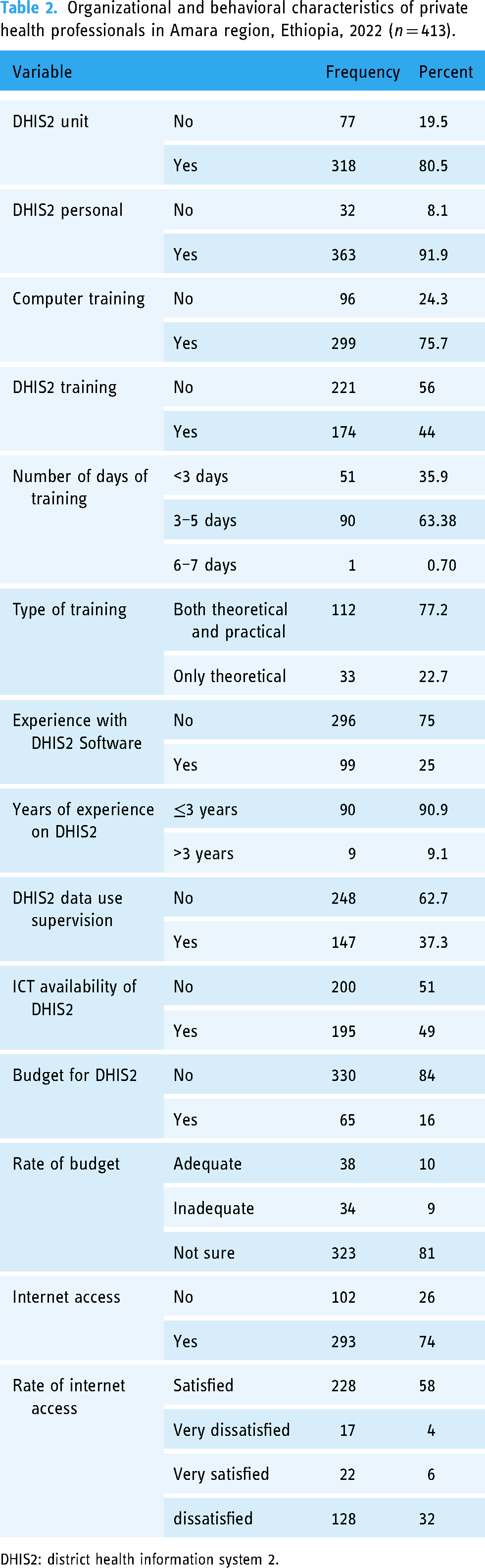
DHIS2: district health information system 2.
Technical factors
Of 62 (16%) out of all healthcare professionals received training on data use. The majority of 310 (78.4%) of the facility's health professionals have good data analysis skills, and also 87 (22%) of them used DHIS2 to perform a quality check (Table 3).
Technical characteristics of private health professionals in Amhara region, Ethiopia, 2022 (n = 413).

DHIS2: district health information system 2.
Utilization of DHIS2 data
Among all healthcare professionals, 37.72% (95% CI [33–42%]) of them had good utilization of DHIS2. More than half of 62.28 5% of healthcare provider had poor utilization of DHIS2 data (Figure 2).
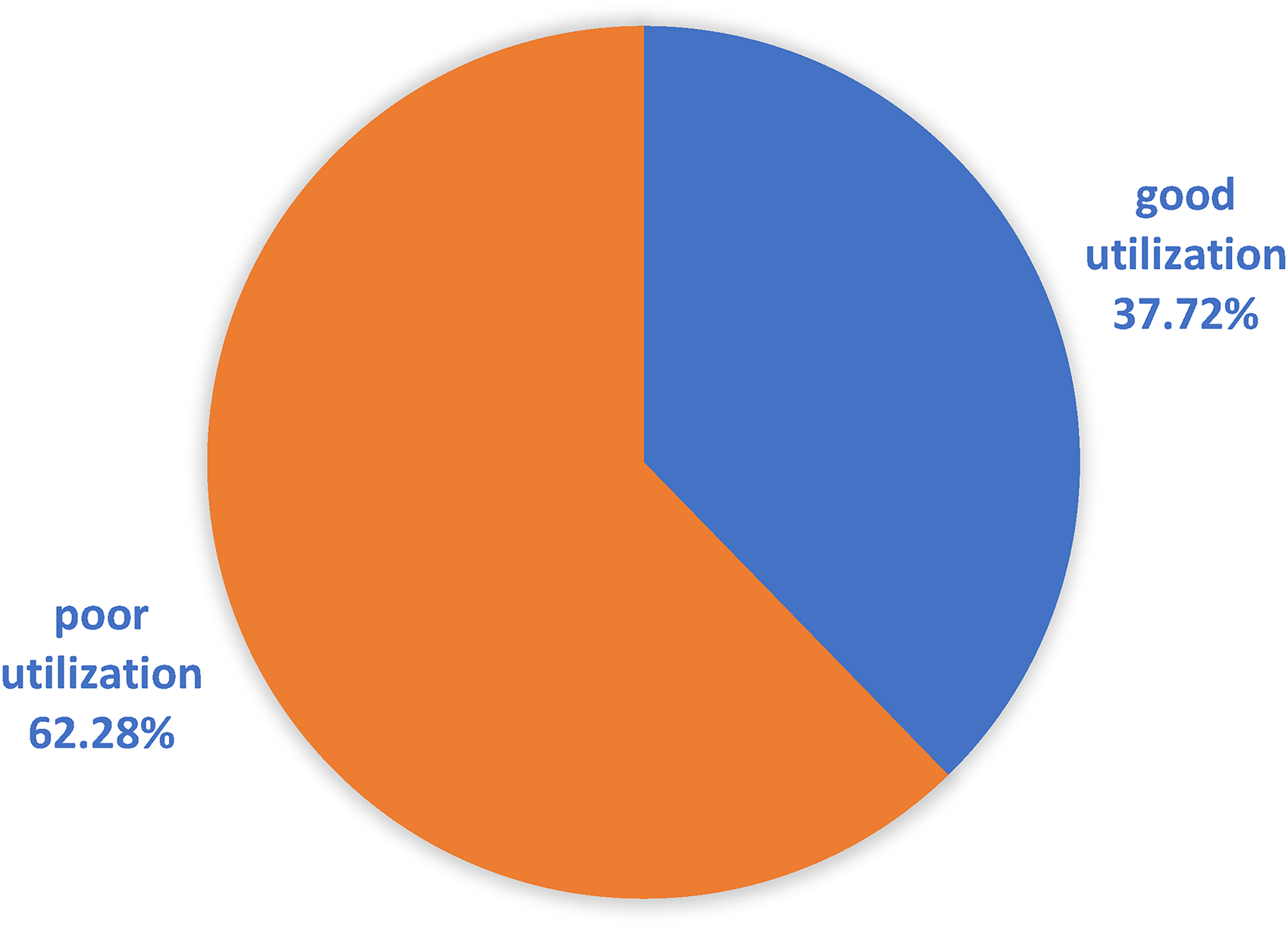
Utilization of DHIS2 data.
Factors associated with the utilization of DHIS2 data
In both bivariable and multivariable analysis, had good data analysis skills, regular supportive supervision and feedback, monthly salary > 5000 ETB, ease of use, and DHIS2 training were significant variables in the utilization of DHIS2 data on health professionals (Table 4).
Multivariable analysis for factors associated with utilization of district health information system 2 data in private hospitals of Amara region, 2022.

DHIS2: district health information system 2; AOR: adjusted odds ratio; COR: crude odds ratio.
*Significance at p-value < .05.
Discussion
This study assessed the utilization of DHIS2 data among health professionals in Amara Regional State, North West Ethiopia. Factors like data analysis skills, supportive supervision and feedback, monthly salary, perceived ease of use, and DHIS2 training were found to be significantly associated with the utilization of DHIS2.
This study showed that the proportion of DHIS2 data utilization in private health facilities by health professionals was 37.72% (95% CI [33–42%]).
This study's findings are lower than those reported in studies conducted in Eastern Ethiopia (70.3% 44 ), Northwest Ethiopia (46%), 6 Oromia Special Zone, Ethiopia (52.8%), southwest Ethiopia (57.3%),42,51 and Gojam, Northwest Ethiopia (45.8%). 52 The possible explanation for this difference could be the Ministry of Health and other stakeholders give greater priority to public health facilities. DHIS2, training supervision primarily focused on public hospitals than private. 40 Government hospitals might have more skilled health informatics professionals to promote effective data use, support other healthcare providers, identify gaps in service, and provide capacity-building training. Almost all nongovernmental organizations are involved in the government health facilities health data initiative than private health facilities.
This can be seen in the allocation of funding for information systems, including infrastructure, training, and support for technical issues. 53 Our study revealed that only seven health informatics professionals were hired from a pool of eight private hospitals. This finding indicates that private health facilities must recruit health informatics professionals for DHIS2 and other data-related activities. However, this study higher than the utilization rate reported in Addis Ababa (41.7%), 54 Kenya 30%, 55 Ghana 21%, 56 and Botswana 26% 57 and West Amara, Ethiopia (38%). 58 The possible explanation for this difference might be the variation in study periods, sample size difference, and study populations.
Those who had good data analysis skills at the health facility were found to increase the odds of utilizing DHIS2 data by 6.5 times compared to their counterparts. Which is in line with a study conducted in Western Ethiopia 59 and Saudi Arabia. 60 Studies show that DHIS2 data use has decreased as a result of a lack of analysis skills. 61 This might be because using health information can be easy after analysis. Competence in data analytics could improve the use of data for healthcare provision, allocating resources, and budget planning. 62
This shows the significance of improving healthcare professionals’ data analysis skill through extensive practical training to enable better DHIS2 data utilization. 63
The odds of DHIS2 data utilization among health professionals who were given regular supportive supervision and feedback on DHIS2 utilization were greater than those who were not given (AOR 5.2, 95% CI [2.8–9.5]). According to studies, ongoing monitoring is vital to enhance information use culture would be effective and this might be true because telling health professionals about their strengths and weaknesses might motivate them to use data more frequently. 62 This result was supported by the studies conducted in southwest Ethiopia, Uganda, and Australia.42,61,64
The odds of DHIS2 data utilization are higher for those who have a monthly salary > 5000 ETB than those <5000 ETB (AOR 2.0, 95% CI [1.1–3.7]). This might be due to a person who earns a high salary is motivated to do a good job and keep his employment. 65
According to this study, perceived ease of use is another factor that has a significant association with DHIS2 data utilization (AOR 5.4, 95% CI [2.8–10.2]). Which is supported by the study conducted in Botswana Tanzania.48,66 Based on evidence, the perceived ease of use has been identified as the most influential factor in enhancing the usability of DHIS2 data. End users have highlighted that improved data availability and quality, as well as a reduction in workload burden, are key benefits. These findings demonstrate that by prioritizing ease of use, healthcare providers can more effectively enhance the usability of the system, ultimately improving their ability to utilize it.47,66 This study also indicated that taking DHIS2 training was found to have a significant association with the utilization of DHIS2 data (AOR 4.2, 95% CI [2.2–7.3]).
This result was supported by the study conducted in Ethiopia which showed being trained about health information was positively correlated with the utilization of DHIS2 data. 67 Other studies conducted in Ethiopia and Ghana stated that being trained was positively associated with the utilization of DHIS2 data.42,68 It is a fact that receiving DHIS2-focused training can help develop their DHIS2-related skills and enhance their confidence when using the system.62,69,70
Strength and limitation
The findings of this study serve as a valuable resource for policymakers and healthcare managers in the private health sector. As the first study of its kind, it provides insights and recommendations to improve utilization rates. This study included all private hospitals found in the Amara Region, but not include public hospitals this could also affect the generalizability of the study. The other limitation of this study was due to the utilization of a self-administered questionnaire, there is a possibility of self-reporting bias. Moreover, the cross-sectional methodology employed in this study presents challenges in establishing temporal associations.
Conclusion
Private healthcare providers had limited utilization of DHIS2 data. It is highly recommended to provide DHIS2 training, supervision, and feedback focused on private health facilities. Additionally, enhancing data analysis skills and prioritizing ease of use are crucial to improving DHIS2 data utilization.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076241283239 - Supplemental material for District health information system 2 data utilization among health professionals in Amara region private hospitals, Ethiopia
Supplemental material, sj-pdf-1-dhj-10.1177_20552076241283239 for District health information system 2 data utilization among health professionals in Amara region private hospitals, Ethiopia by Abraraw Gebre Mesele, Abreham Yeneneh Birhanu and Atsede Mazengia Shiferaw, Nebebe Demis Baykemagn in DIGITAL HEALTH
Footnotes
Availability of data and materials
The corresponding author will provide the datasets for this study upon a reasonable request.
Acknowledgments
We express our gratitude to the University of Gondar Institute of Public Health for providing us with ethical clearance. We would also like to extend our appreciation to the private hospitals for their cooperation and for providing us with all the necessary information. Lastly, we would like to thank the dedicated data collectors and supervisors for their hard work and commitment.
Contributorship
Each of the authors made substantial contributions to the study, including involvement in the conception, study design, execution, data acquisition, analysis, and interpretation. Additionally, all authors contributed to drafting, editing, and critically reviewing the article, and they collectively assumed full responsibility for every aspect of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The ethical review was conducted following the principles of the Helsinki Declaration. Ethical clearance was obtained from the ethical review board of the University of Gondar with reference number IPH/16/05/2022. Communication with the different official administrators of each Amara Region health bureau and private hospitals was made through ethical clearance obtained from the University of Gondar. Written informed consent was obtained from each study participant after telling the objective of the study. Participants were informed about the benefits and risks of the study. The data collection procedure was anonymous and their privacy was also kept.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
ABM & NDB.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.