
Abstract
Background
Mental health challenges are common among older adults with mild cognitive impairment. Despite growing use of digital health interventions to improve cognitive function, their effects on mental health remain unexplored.
Objective
To assess the overall and subgroup-specific effectiveness of digital health interventions on mental health in older adults with mild cognitive impairment.
Methods
A systematic review and meta-analysis of randomized controlled trials was conducted following PRISMA guidelines, searching seven databases from inception to March 2024. Evidence quality was assessed using the GRADE framework and risk of bias with the Cochrane Collaboration's tool. Interrater agreement for screening and data extraction was assessed using the Kappa coefficient. Subgroup analyses assessed differences based on intervention characteristics such as type, setting, and duration, while meta-regression and sensitivity analysis identified other sources of heterogeneity and tested robustness.
Results
Eleven studies involving 610 participants met the criteria. Digital health interventions significantly reduced depressive symptoms (Standardized Mean Difference [SMD] −0.55, 95% CI −0.92 to −0.19) and anxiety symptoms (SMD −0.47, −0.76 to −0.18), but showed no significant effects on positive (SMD 0.74, −0.46 to 1.94) or negative affect (SMD −0.23, −0.60 to 0.14). Subgroup analyses indicated that hospital or nursing home settings with non-portable modality were optimal. Interventions over 6 weeks, with sessions exceeding 30 min up to 2 per week, were more effective for depressive symptoms. Among intervention types, only robot interventions reduced depressive symptoms. Fully digital interventions showed greater effectiveness than hybrid formats and yielded more favorable outcomes compared to controls. Overall, digital health interventions showed a significant benefit over usual care, while effects compared to waitlist controls were larger but not statistically significant.
Conclusions
This review indicates that digital health interventions hold promise for enhancing mental health in older adults with mild cognitive impairment. Future research should integrate digital therapeutic technologies to optimize interventions.
Keywords
Introduction
Dementia is recognized as a significant global public health concern, with mild cognitive impairment (MCI), its preclinical stage, considered a critical target for dementia prevention efforts. 1 MCI serves as a transitional stage between normal age-related cognitive decline and dementia. 2 Increasing evidence indicates that mental health issues are highly prevalent among older adults with MCI. Depressive, apathy, and anxiety symptoms are prevalent among individuals with MCI, affecting approximately 42.0%, 39.5%, and 31.2% 3 of this population, respectively. Severe depressive symptoms in older adults with MCI may disrupt homeostasis, potentially elevating the risk of falls. 4 Meanwhile, sleep disorders, prevalent in 14 to 60% of older adults with MCI,5,6 are also associated with negative affect, which may exacerbate cognitive decline.7,8 Notably, older adults with MCI and depressive symptoms exhibit a higher dementia conversion rate (31%) compared to those without depressive symptoms (13.5%), 9 underscoring the compounding effect of mental health and MCI on cognitive decline and dementia progression. 10
Despite the widespread occurrence of mental health issues in individuals with MCI, these concerns have often been overlooked, with limited access to psychotherapy.11,12 Traditional psychosocial interventions, including music therapy to enhance well-being and reduce anxiety, pet therapy to provide emotional support and sensory stimulation, socially oriented interactions through real or simulated presence, and reminiscence therapy eliciting positive autobiographical memories, have demonstrated benefits for affect. 13 However, these approaches rely heavily on direct human interaction, limiting scalability and long-term feasibility in an already strained care environment. 14 Currently, the rapid integration of internet technologies into healthcare is transforming psychological and cognitive interventions for older adults, marking a transformative era of digital therapy. 15
Digital Health Interventions (DHIs) utilize a range of technological platforms like mobile apps, email, wearable devices, and virtual reality (VR) to deliver cognitive and psychological interventions and support for physical or mental health conditions.16,17 They are particularly valuable for individuals facing mobility, social, or geographic barriers, with growing evidence showing that DHIs can deliver personalized, flexible support with meaningful cognitive benefits.18–20 Beyond cognitive benefits, DHIs may also improve mental health in older adults with MCI through interacting neurobiological, psychological, and social pathways. At the neural level, computerized cognitive training (CCT), VR programs, and robot-assisted interventions may strengthen executive control and memory systems that partly overlap with neural circuits for emotion regulation. In particular, fronto-limbic circuits involving the dorsolateral and ventromedial prefrontal cortex, anterior cingulate cortex, hippocampus, and amygdala are implicated in both higher-order cognitive control and the top-down regulation of negative affect.21,22 Repeated practice of goal-directed, attentionally demanding tasks has been associated with increased efficiency of prefrontal control networks and altered functional coupling with limbic regions, which in turn may facilitate more effective reappraisal of stressors, stronger inhibition of maladaptive emotional responses, and reduced amygdala reactivity to negative stimuli.23,24 Trials of serious-game cognitive training in MCI, for example, have shown concurrent reductions in depressive symptoms and apathy, suggesting that enhanced cognitive control, task mastery, and perceived competence, possibly mediated through these fronto-limbic control networks, translate into improved mood. 25 VR-based multisensory interventions for MCI further provide enriched, immersive environments that may stimulate hippocampal-prefrontal plasticity and are associated with small but notable improvements in depression and quality of life. 26 Psychologically, some DHIs may influence the mental health of individuals through motivational and cognitive-affective mechanisms grounded in self-efficacy, self-determination, and behavioral activation theory frameworks. Many digital programs deliberately combine gamification, adaptive difficulty, and performance-based feedback to generate repeated mastery experiences, thereby strengthening perceived competence and self-efficacy while supporting more autonomous, intrinsically motivated engagement. CCT, for example, provides immediate, performance-based positive feedback and visible progress indicators, which can enhance self-confidence, counteract negative interpretation biases (such as feelings of uselessness or anticipated failure), and promote sustained behavioral activation in cognitively demanding activities among older adults with MCI. 27 In parallel, immersive and interactive VR environments embed cognitive tasks within emotionally salient, enjoyable scenarios that capture attention, offer rich positive reinforcement, and provide structured opportunities for success; these features are thought to reduce avoidance, increase approach-oriented behavior, and support momentary mood repair, consistent with behavioral activation models.28–30 Socially, DHIs may improve mental health by reshaping patterns of social support, loneliness, and perceived security. Digital platforms that embed videoconferencing, messaging, and online group activities may expand both the structural and functional dimensions of social support by increasing the frequency, accessibility, and perceived quality of contact with family, peers, and healthcare professionals. By compensating for limited face-to-face interactions, such platforms could help alleviate loneliness and social isolation, enhance self-esteem, and contribute to reductions in depressive and anxiety symptoms through social engagement.31,32 Furthermore, assistive robots further contribute by monitoring safety, emotional and physiological states, and supporting basic and instrumental activities of daily living, helping individuals with MCI maintain independence and continuity of valued roles in the home environment, 33 which may reduce worry and perceived burden, indirectly alleviating depressive and anxiety symptoms.
Despite promising results, most studies have focused on the cognitive effects of DHIs, while evidence for their impact on mental health outcomes in older adults with MCI remains limited and inconsistent. Although one meta-analysis reported that digital interactive tools alleviated depressive and anxiety symptoms in older adults, including those with neurocognitive disorders, 31 a more recent meta-analysis targeting MCI populations found only minimal effects on depressive symptoms. 32 Moreover, several studies reported mixed findings, suggesting that the effectiveness of DHIs may depend on individual characteristics, intervention type, and duration.14,34,35 Additionally, most research on DHIs in the context of MCI has predominantly concentrated on cognitive function, with less emphasis on mental health outcomes. Therefore, a holistic approach is essential to evaluate the broader impact of DHIs on mental health outcomes in individuals with MCI.
This meta-analysis aimed to evaluate the effectiveness of DHIs on mental health outcomes in older adults with MCI, with three primary objectives. First, to compare the effectiveness of DHIs with non-DHI approaches. Second, to examine how intervention characteristics (e.g., DHI type and modality, and intervention setting) influence specific mental health outcomes. Third, to identify the advantages of DHIs in improving mental health and to provide insights for developing more effective health management strategies for older adults with MCI.
Methods
Study design and ethical considerations
This systematic review and meta-analysis were registered in PROSPERO (CRD42024522342), conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline 36 (Supplementary File 1), and the protocol was previously published. 37 Ethical approval was not required as only previously published data were used. Rigorous ethical standards were maintained, including transparent reporting, bias minimization, and the inclusion of ethically approved studies.
Search strategy and eligibility criteria
The search process followed the Cochrane Handbook of Evaluation. Relevant studies were identified in CINAHL, Web of Science, PubMed, Cochrane Library, Embase, and Chinese database (i.e., CNKI and WanFang) from their inception to March 7, 2024. In addition, the reference lists of retrieved articles were screened manually to identify additional relevant records. Search strategy and terms were designed to identify studies involving participants (older adults with MCI), DHIs (eHealth, mHealth, application, mobile phone, wearables, tablet, artificial intelligence, email, and robot, etc.), as well as mental health outcomes (depressive symptoms, anxiety symptoms, apathy, stress, suicidal ideation, psychological distress, and loneliness, etc.), as outlined in Supplementary File 2, eTable 1. In this review, “older adults” were defined as individuals aged 60 years or older, consistent with UN and WHO conventions.38,39 The eligibility criteria, encompassing both English and Chinese randomized controlled trials (RCTs), were formulated based on the population, intervention, comparison, outcome, and study design (PICOS) framework, with details provided in Table 1.
Study selection criteria in PICOS format.

Study selection and data extraction
The identified studies were managed using EndNote 20 for de-duplication and screened for eligibility by two independent reviewers (A.G. and A.H.) Data from the included studies were systematically extracted into a standardized table, and any discrepancies were resolved through consensus with a third reviewer (X.L.) The extracted data included study characteristics (first author, country, year), population characteristics (participant numbers, age), DHI characteristics (type, modality, setting, session frequency, dose, duration, and content), comparators (types of interventions), and mental health outcomes. Inter-rater agreement was evaluated using the Kappa coefficient, with values interpreted as follows: ≤0.20 indicating no agreement, 0.21–0.39 minimal, 0.40–0.59 weak, 0.60–0.79 moderate, 0.80–0.90 strong, and >0.90 almost perfect agreement. 40
Risk of bias and quality appraisal
Two independent reviewers (A.G. and A.H.) assessed the risk of bias in the included studies using the Cochrane Collaboration's tool, with analyses performed in Review Manager (version 5.3). This evaluation covered various bias types, including selection, performance, detection, attrition, reporting, and other biases. 41 Each criterion was assigned a rating of low, high, or unclear risk of bias. Discrepancies were resolved through consensus with a third reviewer (X.L.), and inter-rater agreement was assessed using the kappa coefficient. In addition, the quality of evidence for each primary mental health outcome was appraised with the GRADE approach and classified as high, moderate, low, or very low. 42 A summary of findings table was generated with the GRADEpro Guideline Development Tool, recording the rationale for all downgrading decisions.
Data synthesis
The meta-analysis was performed using R (version 4.4.1) and STATA (version 17.0). The standardized mean difference (SMD) and 95% confidence interval (CI) were used for continuous data to aggregate the pooled effect of DHIs on mental health outcomes. Effect sizes were categorized as small (0.2–0.5), moderate (0.5–0.8), and large (> 0.80). 43 Estimates were calculated using the median, range, sample size, and/or interquartile range when the mean and standard deviation (SD) were unavailable. 44 When the heterogeneity test indicated P > .10, studies were considered homogeneous and a fixed-effects model was applied; when P ≤ .10, a random-effects model was used, and subgroup as well as meta-regression analyses were conducted to explore potential sources of heterogeneity. Heterogeneity (I2) was categorized as unimportant (0%-40%), moderate (30%-60%), substantial (50%-90%), or considerable (75%-100%). 45 Sensitivity analysis was further performed to assess the robustness of the findings. Additionally, publication bias was evaluated using funnel plots and the Egger test when the analysis included 10 or more studies. 46 Statistical significance was defined as P < .05.
Results
Study selection
The initial search across seven databases identified 1686 studies, with 272 duplicates subsequently removed, leaving 1414 potentially eligible studies. These were screened by titles and abstracts, resulting in 52 studies for full-text review. After detailed screening, 41 studies were excluded for not meeting the inclusion criteria, resulting in 11 studies being selected for analysis and quantitative synthesis (Figure 1). Interrater agreement for title/abstract and full-text screening was Kappa = 0.83 and Kappa = 0.85, respectively, reflecting strong consistency between reviewers.
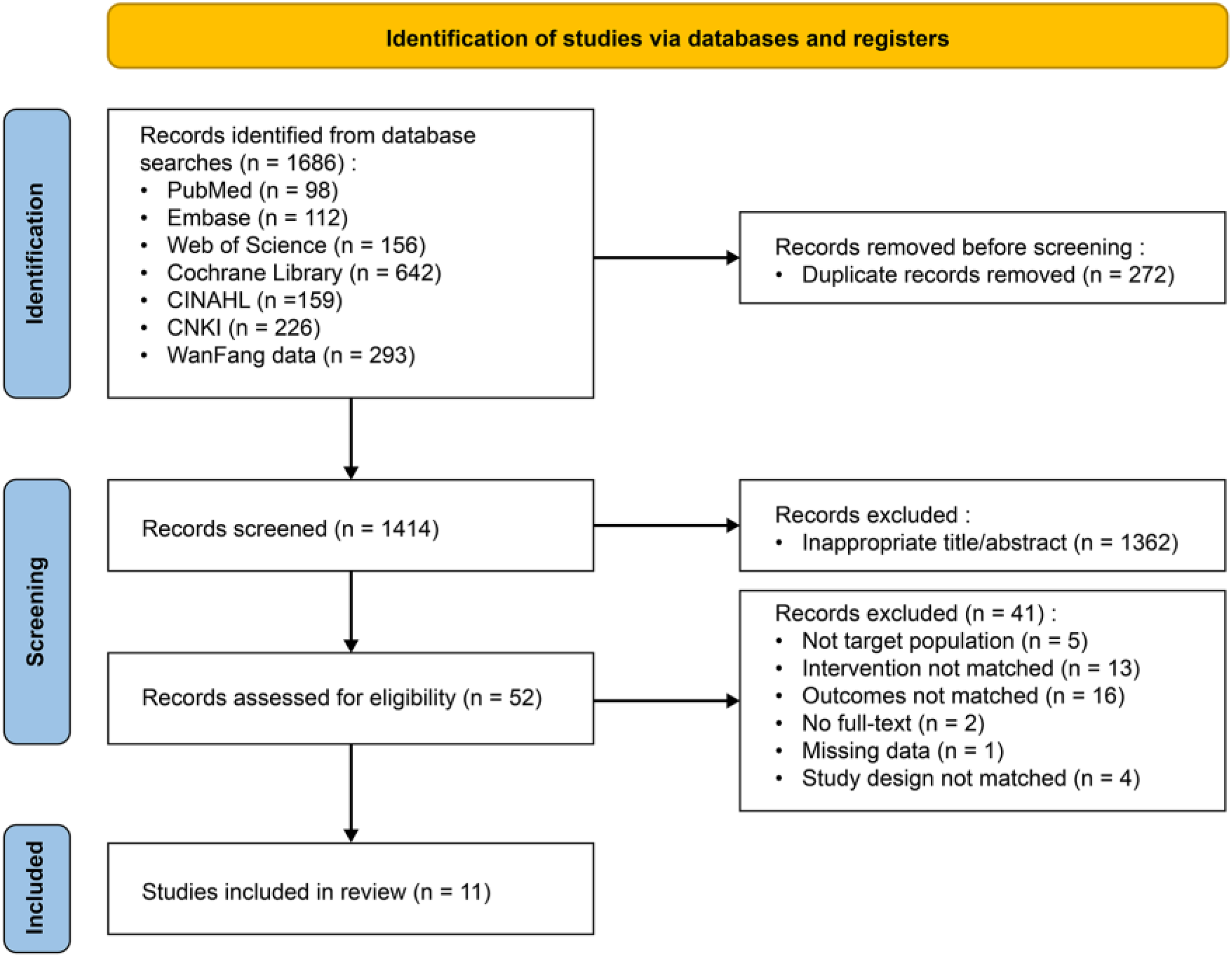
Flowchart of the study selection process.
Study characteristics
Eleven RCTs published between 2017 and 2024 were included, involving 610 older adults with MCI. Four studies were conducted in China,29,47–49 five in Korea,28,50–53 and two in Greece 54 and Iran. 55 Most participants came from hospitals (54.5%), followed by nursing homes (18.2%) and community or home settings (18.2%). All included studies had pre- and post-intervention assessments, with only one study conducting a 3-month follow-up. 55 Among the 11 included studies, most used usual care28,48–51,53–55 as the control (n = 8), with two employing a waitlist control29,52 and one an active control. 47 The details are in Supplemental File 2, eTable 2.
Characteristics of the DHIs
The characteristics of DHIs varied across studies, with sessions lasting 20–90 min, occurring 1–5 times per week over 4 weeks to 6 months, and classified into five types. First, tablet-based interventions included serious games that adapt to cognitive abilities, provide positive feedback, and promote a positive attitude. 47 Another approach adapts the Ubiquitous Spaced Retrieval-based Memory Advancement and Rehabilitation Training program into an iPad application, featuring progressive retrieval intervals, difficulty adjustments, and automated verbal guidance. 53 Second, intervention robots included devices designed for cognitive training, equipped with sensors to monitor participants’ signals, adjust task difficulty, and assess mood, interest, and engagement. 50 Another type involves humanoid robots with Human-Robot Interaction technology that display facial expressions, recognize participants’ intentions and emotions, and guide them through activities like problem-solving and physical exercises to enhance motivation and reduce depressive symptoms. 52 Third, VR interventions, employed in five studies, used VR technology for multi-component cognitive training with headset displays and computer interfaces; participants engaged in tailored games, received feedback, faced increasing task difficulty, and were motivated by visual or vocal cues to achieve high scores and promote social interaction.28,29,51,54,55 Fourth, computer-assisted interventions involved computerized training guided by psychotherapists, targeting multiple cognitive domains with 3–7 programs aligned with daily living and progressively increasing task difficulty. 48 Fifth, web-based remote interventions used online platforms where participants engaged in activities such as music, dance, and visual art, with task difficulty adjusted to individual abilities to reduce negative affect, stimulate creativity and social interaction, and enhance self-esteem. 49 The characteristics of DHIs are detailed in Supplemental File 2, eTable 3.
Characteristics of mental health outcomes
Participants in the 11 included studies typically exhibited normal to mild-moderate depressive symptoms28,29,47–55 and normal to mild anxiety29,49,50,55 at baseline on validated scales; positive and negative affect were relatively low where reported.28,49 One study additionally reported moderate-severe apathy, 28 higher self-esteem, 49 and higher subjective mental-health scores. 29
Depressive symptoms were the most frequently assessed outcome after intervention,28,29,47–55 measured using the 15-item or 30-item geriatric depression scale (GDS),28,29,47–49,54,55 or the Geriatric Depression Scale Short Form: Korean Version (GDSSF-K).50–53 Anxiety symptoms, assessed in 4 studies,29,49,50,55 were measured by self-rating anxiety scale (SAS) or geriatric anxiety inventory (GAI). In two studies, positive and negative affect were measured using the positive and negative affect schedule (PANAS) 28 and the Memorial University of Newfoundland Scale of Happiness (MUNSH). 49 Positive and negative affect represent broad dimensions of emotional experience, with positive affect encompassing states such as alertness and enthusiasm, and negative affect encompassing lethargy and sadness.28,56,57 In contrast, depressive and anxiety symptoms are specific clinical clusters, characterized by low mood and anhedonia, or excessive worry and tension, respectively. Thus, while depressive and anxiety symptoms indicate disorder-specific clinical outcomes, positive and negative affect reflect general emotional states. 58 Another study used the 18-item Apathy evaluation scale (AES) for apathy. 28 Self-esteem was measured by the self-esteem scale (SES) in one study, 49 while subjective feelings were measured in another study through the Mental Component Scale (MCS) of the 12-item Short-Form Health Survey (SF-12). 29
Risk of bias and evidence quality appraisal
All included studies exhibited a low risk of attrition and reporting bias. Five studies employed appropriate random allocation methods, indicating a low risk of bias in sequence generation.28,29,49,51,53 Allocation concealment was reported in six studies,47–49,51,52,55 and four described blinding of participants and personnel,49,50,52,53 with seven studies blinding outcome assessment.29,47–49,52,54,55 Eight studies were assessed as having a low risk of other biases.28,29,47–50,53,54 Overall, the main bias were selection, performance, and detection, with detection bias contributing to the highest risk (Kappa = 0.74, Supplemental File 2, eFigure 1). Additionally, the quality of evidence assessed with GRADE ranged from moderate to very low (Supplemental File 3): depressive symptoms were rated moderate, anxiety symptoms low, and negative and positive affect very low. Interrater agreement on GRADE ratings was Kappa = 1.00. Downgrading was driven primarily by methodological limitations, small sample sizes, and wide confidence intervals.
Overall effects of DHIs on mental health outcomes
As depicted in Figure 2, the effectiveness of DHIs compared with control groups was assessed across 11 studies: 11 for depressive symptoms,28,29,47–55 4 for anxiety symptoms,29,49,50,55 and 2 each for negative and positive affect.28,49 The pooled SMD was −0.55 (−0.92 to −0.19) for depressive symptoms and −0.47 (−0.76 to −0.18) for anxiety symptoms, indicating DHIs group had lower post-intervention symptoms than the control group. However, the effect size was more pronounced for depressive than anxiety symptoms. Additionally, considerable heterogeneity was found (I2 = 79% for depressive symptoms), leading to the adoption of a random effects model for the analysis. The results showed no significant SMD favoring DHIs over the control group for negative affect (SMD −0.23, 95% CI −0.60 to 0.14, I2= 0.00%) and positive affect (SMD 0.74, −0.46 to 1.94, I2= 88%, Figure 2). None of the included studies reported mental health outcomes related to stress, psychological distress, or loneliness, and with only one study assessing subjective measures such as self-esteem and apathy, a meta-analysis was not feasible, so a narrative summary was provided.

Forest plot of the effectiveness of DHIs on depressive, anxiety symptoms, negative and positive affect (R v4.4.1).
Subgroup analyses of intervention scheduling
Subgroup analyses were conducted to identify potential sources of heterogeneity in the effectiveness of DHIs on depressive symptoms (Figures 3–5). Intervention-dose cut-offs (duration >6 weeks, session length >30 min, frequency ≤2 sessions/week) were pre-specified based on clinical conventions and the empirical distribution of our data, supported by evidence from recent meta-analyses.59–63 First, regarding intervention duration, interventions over 6 weeks (n = 4) showed a statistically significant medium effect size (SMD −0.67, −1.29 to −0.05, I2 = 84%), whereas those lasting 6 weeks or less (n = 7) did not demonstrate a statistically significant effect (SMD −0.48, −0.96 to 0.00, I2 = 74%, Figure 3). Second, regarding intervention dose per session, sessions exceeding 30 min (n = 5) had a statistically significant medium effect (SMD −0.62, −1.12 to −0.13, I2 = 80%) in reducing depressive symptoms, while sessions of 30 min or less (n = 6) showed no significant difference (SMD −0.50, −1.08 to 0.08, I2 = 78%, Figure 3). Third, regarding intervention frequency, interventions conducted up to 2 per week (SMD −0.52, −0.94 to −0.09, I2 = 81%, n = 9) reduced depressive symptoms. In contrast, interventions more than 2 per week (n = 2) showed no significant difference compared to the control group (SMD −0.72, −1.51 to 0.08, I2 = 67%, Figure 3).

Forest plot of subgroup analyses on intervention scheduling for depressive symptoms (R v4.4.1).

Forest plot of subgroup analyses on intervention setting/modality for depressive symptoms (R v4.4.1).

Forest plot of subgroup analyses on intervention type and delivery/control format for depressive symptoms (R v4.4.1).
Subgroup analyses of intervention setting and modality
Regarding intervention setting, DHIs implemented in hospitals or nursing homes (n = 8) demonstrated a small effect size of −0.48 (−0.90 to −0.06), suggesting a reduction in depressive symptoms among older adults with MCI compared to the control group. However, interventions conducted at community or home settings (n = 2) showed no significant difference (SMD −0.94, −2.10 to 0.22, I2 = 90%, Figure 4). Regarding intervention modality, non-portable modalities of DHIs (n = 5) showed a large effect size in reducing depressive symptoms (SMD −0.88, −1.46 to −0.30, I2 = 81%). However, portable modalities (n = 5) did not demonstrate a significant difference (SMD −0.28, −0.73 to 0.17, I2 = 62%, Figure 4).
Subgroup analyses by intervention type and delivery or control format
Regarding the intervention type, only robot interventions (SMD −0.44, −0.79 to −0.09, I2 = 0.00%, n = 2) significantly reduced depressive symptoms. In contrast, tablet-based (SMD −0.19, −0.52 to 0.15, I2 = 11%, n = 2) and VR interventions (SMD −0.60, −1.31 to 0.11, I2 = 79%, n = 5, Figure 5) did not show significant effects. In subgroup analyses by delivery format, fully digital interventions were associated with a significant reduction in depressive symptoms (SMD −0.44, −0.80 to −0.07; I2 = 66%, n = 9), whereas hybrid interventions showed no significant effect (SMD −0.98, −2.04 to 0.08; I2 = 89.2%, n = 2, Figure 5). Regarding differences by control format, the single study with an active control (n = 1) could not be pooled. Versus waitlist control, DHIs showed a large but non-significant effect (SMD −1.05, −2.21 to 0.12, I2 = 86.1%, n = 2). In contrast, comparisons with usual care yielded a statistically significant effect (SMD −0.45, −0.89 to −0.01, I2 = 81.4%, n = 8, Figure 5), indicating greater improvements than usual care, although the substantial heterogeneity warrants cautious interpretation.
Narrative summary
Other mental health outcomes, including subjective feelings, 29 self-esteem, 49 and apathy, 28 were assessed in single studies and thus were not eligible for meta-analysis. A narrative synthesis was therefore conducted to summarize the findings following DHIs. One study assessed subjective feelings using the MCS score and reported significant improvements in the DHI (VR) group from baseline to six weeks (P < .05), with no significant change observed in the control group (P = .48); Between-group comparisons further favored the DHI (P < .05). 29 Another study used the SES to evaluate changes in self-esteem. Participants who received a web-based remote intervention showed significant improvements from baseline and compared to controls (P < .05). 49 A third study measured apathy using the AES, and results showed a significant reduction in apathy among participants in the DHI (VR) group compared to controls (P < .05). 28 Although each of these outcomes was assessed in a single study, the findings consistently suggest that DHIs may positively impact broader aspects of mental health in older adults with MCI.
Meta-regression and sensitivity analysis
Meta-regression (Supplemental File 2, eTable 4) was conducted to identify sources of heterogeneity, with no covariates emerging as significant contributors (all P > .05). No studies were excluded after sensitivity analysis (Figure 6), which revealed no disruptive changes in the combined results, indicating robustness in the study's findings. Meanwhile, excluding hybrid trials yielded similar pooled estimates, indicating that the main findings are robust to delivery-format exclusions (Supplemental File 2, eFigure 3).

Sensitivity analysis of DHIs on depressive symptoms (Stata v17.0).
Publication bias
Although the funnel plot exhibited an asymmetrical distribution (Supplemental File 2, eFigure 2), no publication bias was detected in this study, as confirmed by the Egger test (P = .930).
Discussion
Summary of findings
This study assessed the effectiveness of DHIs on mental health outcomes in older adults with MCI. Significant improvements were found in depressive and anxiety symptoms, though no effects on negative or positive affect. Interventions over six weeks, with sessions exceeding 30 min and occurring up to 2 per week, were more effective in reducing depressive symptoms. Hospital or nursing home settings were optimal for DHIs, in which non-portable, fully digital interventions, such as robot-based ones, proved most effective.
Overall effects of DHIs on mental health outcomes
Prior studies have consistently highlighted the beneficial effects of DHIs on mental health outcomes,64,65 with a recent meta-analysis further confirming their effectiveness as an alternative to traditional face-to-face therapy. 66 The findings of our study align with this evidence. Despite evidence supporting DHIs, older adults often favor traditional in-person treatments. However, stigma and cost barriers associated with face-to-face therapies can discourage treatment-seeking behavior and reduce adherence. 67 In contrast, DHIs could provide flexibility and accessibility alternatives. These digital platforms are scalable and adjustable, catering to the specific needs of diverse populations while overcoming barriers like geographic location, limited access to trained clinicians, and time constraints.64,68
Furthermore, our meta-analysis found no significant improvements in overall positive or negative affect following DHIs, likely reflecting limited reporting and small sample sizes, as only two studies included these outcomes.28,49 Nevertheless, the evidence indicates nuanced affective modulation. For instance, in one study, the VR group exhibited increases in positive affect and decreases in negative affect relative to controls, 28 whereas in another Web-based remote intervention, the intervention group showed increased positive affect from baseline despite no between-group differences. 49 Prior research suggests that older adults with MCI may experience modest gains in positive affect and slight reductions in negative affect through the use of a mobile cognitive training app, potentially supported by preserved cognitive capacities that facilitate engagement and affective responsiveness. 69 Therefore, an aggregate affect score may obscure item-specific or subtle affective responses. To better elucidate such subtle effects, it is essential to consider the underlying mechanisms. Specifically, DHIs engaging multiple sensory and cognitive modalities through visual, tactile, and perceptual stimuli may enhance multimodal integration and modulate affective processing. 49 Neuroimaging evidence further indicates increased regional homogeneity in the anterior cingulate and dorsolateral superior frontal regions, areas implicated in affect regulation, reinforcement learning, and conflict monitoring, suggesting subtle neural modulation underlying minor affective changes.49,70,71
Intervention characteristics impacts DHIs effectiveness on mental health outcomes
Subgroup analysis revealed that interventions over six weeks, with sessions exceeding 30 min and occurring up to 2 per week, were more effective in reducing depressive symptoms. It is suggested that older adults with MCI, limited by physical and cognitive impairments, may show reduced engagement with DHIs. 72 Longer intervention duration and higher doses may provide a sustained impact and be crucial for adaptation behavior, as they offer the brain more time and stimulation to undergo changes, reinforce new neural connections, and help individuals integrate learned behaviors into daily routines, resulting in long-term adaptations. 73 A systematic review found that interventions over six weeks using information and communication technology were effective for individuals with MCI. 60 Another review demonstrated that computerized cognitive training sessions exceeding 30 min were most effective, 74 likely due to synaptic plasticity after 30 to 50 min of training activities. 75 On the other hand, a frequency of up to 2 per week may better suit participants, as over three sessions could lead to cognitive fatigue and resistance. 74 These findings suggest that a well-structured DHI schedule could promote practical implementation and optimize effectiveness by aligning with cognitive and physical capacities.
This study found hospital or nursing home settings demonstrated greater effects for DHIs. However, Kim et al. reported better outcomes for VR interventions in community setting, 76 potentially due to reduced commuting burdens and individual preferences. Furthermore, home or community settings also present challenges, including delays in technical support and unstable internet connections, which may compromise adherence and efficacy. In contrast, hospital or nursing home often provide supervision and coaching, fostering higher trust and adherence, which ensures that interventions are administered consistently and correctly. Additionally, hospital or nursing home settings may help mitigate social isolation through positive interactions, 77 potentially contributing to the enhanced effectiveness of DHIs.
Subgroup analyses by intervention modality, type, and delivery/control format indicated that DHIs delivered via non-portable devices were associated with significant reductions in depressive symptoms. Although portable devices, such as wearable technologies, have advanced in medical applications, their complexity and operational challenges can impose cognitive burdens on older adults. 78 Furthermore, age-related declines in vision, hearing, and dexterity, along with concerns about comfort, privacy, and lack of support, reduce adherence and limit their effectiveness in improving mental health outcomes.72,78,79 Additionally, non-portable devices may allow for regular scheduling of intervention in fixed settings, providing a stable environment that enhances the quality of the intervention. VR interventions showed no significant effect on depressive symptoms in this study, possibly due to the types of devices used. Non-immersive VR employs computer-based methods, while immersive VR uses headset displays. Moreover, immersive technologies currently face challenges such as security and privacy concerns, cost issues, connectivity problems, usability challenges, and design- related technical difficulties, which may explain the lack of statistical significance in the impact of headset displays. 80 In addition, our findings suggest that fully digital interventions tended to show more consistent improvements than hybrid formats in reducing depressive symptoms, highlighting the advantage of exclusive digital delivery. Results were similar when hybrid trials were excluded, but given the limited hybrid evidence (n = 2) and potential residual confounding from in-person components, these findings remain exploratory. The effectiveness of DHIs also varied by control type: significant improvements were observed versus usual care, whereas larger but non-significant effects were seen versus waitlist, reflecting the limited number of studies and substantial heterogeneity. However, comparative effectiveness versus active intervention remains uncertain due to the paucity of trials. With ongoing advances in technology, DHIs have become more accessible and engaging for older adults with MCI, allowing DHIs to be tailored to this population and appear more effective than traditional training. 60
Notably, studies on DHIs for mental health in older adults with MCI have predominantly been conducted in East Asia and the Middle East, driven by several factors. Increased mental health awareness has led many countries to prioritize mental health in public health policies. The scarcity of mental health professionals and the uneven distribution of healthcare resources, can render traditional face-to-face services insufficient for large populations. DHIs could offer remote care at lower costs and expand access to a wider population, especially in resource-limited settings. Additionally, technological advancements in these regions, coupled with government-led digital transformation initiatives, may further facilitate the infrastructure needed to implement and expand digital health solutions.
Advantages of DHIs for mental health outcomes and recommendations
Current DHIs for MCI, primarily focusing on cognitive training, enhance mental health by combining adaptive tasks and interactive elements. These interventions adjust difficulty based on cognitive abilities, provide positive feedback, and promote engagement through real-time guidance. Robot-assisted and VR-based therapies monitor mood and motivation, offering personalized encouragement,29,52 while creative programs delivered online stimulate mental health through activities like music and storytelling. 49 From a technological advancement perspective, DHIs that combine cognitive training with psychological techniques, including mindfulness and cognitive-behavioral therapy, hold potential for further improvement. Integrating adaptive algorithms, real-time data analysis, and machine learning would allow these platforms to dynamically tailor intervention strategies based on individual progress and responses. This optimization could significantly enhance cognitive function and alleviate depressive and anxiety symptoms by creating a more efficient synergistic effect.
Furthermore, DHIs offer accessibility, adjustability, and extensibility, overcoming time and space constraints. 81 They are particularly beneficial in resources-limited areas by addressing physician shortages and providing timely, high-quality services. 82 However, overly complex interfaces may distract individuals with MCI, causing disorientation due to cognitive decline. Interfaces should be simplified and adapted to users’ abilities, minimizing distractions and reducing cognitive load. 83 As Castilla et al. suggest, key usability improvements include linear navigation, expanding interaction areas beyond the visual buttons to enhance the user's direction sense, and employing natural interfaces, such as audio interfaces, to match the user's cognitive abilities, ensuring usability and effectiveness. 84
Personalization is another key advantage of DHIs, as interventions can be tailored to individual needs. Participants can be matched to appropriate difficulty levels based on cognitive abilities. Real-time emotion recognition through sensor technology enables responsive adjustments, while smartphone apps allow users to select preferred stimuli (images, faces, or words) and track personalized data (physical activity and location) through their built-in sensors, providing real-time feedback. 85 Additionally, younger age, male gender, higher education levels, urban residency, and employment are associated with better internet access and digital skills, potentially enhancing DHIs outcomes. 16 Therefore, DHIs’ designs should consider these factors and incorporate users’ values, preferences, history, and treatments to deliver the most personalized psychological intervention.
Limitations and future directions
The findings of this study should be considered in light of several limitations. First, because this review excluded grey literature and studies published in languages other than English or Chinese, some relevant studies may have been missed, which could affect the comprehensiveness of the findings. Moreover, primary outcomes were based on self-reported symptoms, and the use of different measurement tools may explain the heterogeneity observed across the included studies. Second, although sensitivity analysis confirmed the reliability of our findings, considerable heterogeneity was observed in depressive outcomes. This variability may be attributed to individual differences, as well as in types, modalities, and other intervention characteristics. Additionally, subgroup analyses considering population characteristics or specific MCI subtypes were not performed. Therefore, caution is warranted when generalizing the effectiveness of DHIs to individuals with specific pathologies. Future development of DHIs should emphasize the need for personalized interventions, with features tailored to accommodate variations in demographics, cognitive, emotional, and physical abilities. Third, although stress, psychological distress, and loneliness were prespecified outcomes, no data were available from the included trials. Thus, future studies should incorporate validated measures of these constructs to enable synthesis. Fourth, despite providing valuable insights, the included studies exhibited some methodological limitations, heterogeneity in interventions and outcomes, and small sample sizes, resulting in imprecise effect estimates. Consequently, the quality of evidence by GRADE ranged from very low to moderate, and true effects may differ from the observed estimates. Future research should prioritize well-designed, adequately powered RCTs using validated, standardized outcome measures to generate more reliable and generalizable evidence. Fifth, although MCI is a chronic and progressive condition, the relatively short follow-up durations in the included studies limit the ability to evaluate the long-term sustainability and potential risks of DHIs for mental health. Continuous monitoring and outcome tracking are essential to better understand user trajectories and determine sustained benefits. Future research should use these technologies to assess the safety and long-term effectiveness of DHIs.
Conclusions
Given the potential of DHIs in managing mental health among older adults with MCI, this meta-analysis provides the first comprehensive analysis of the existing evidence, suggesting that DHIs may offer a cost-effective solution. Future research should identify treatment moderators to develop personalized interventions for this population, with collaboration between healthcare providers and researchers being key to successful implementation. Additionally, increased government support is essential to sustainably integrate DHIs into healthcare systems, thereby expanding access to mental health care.
Supplemental Material
sj-png-1-dhj-10.1177_20552076261420265 - Supplemental material for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis
Supplemental material, sj-png-1-dhj-10.1177_20552076261420265 for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis by An Gu, An Huang, Bei Wu, Xueqi Liu, Cheng Huang, Xichenhui Qiu and Lina Wang in DIGITAL HEALTH
Supplemental Material
sj-png-2-dhj-10.1177_20552076261420265 - Supplemental material for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis
Supplemental material, sj-png-2-dhj-10.1177_20552076261420265 for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis by An Gu, An Huang, Bei Wu, Xueqi Liu, Cheng Huang, Xichenhui Qiu and Lina Wang in DIGITAL HEALTH
Supplemental Material
sj-tif-3-dhj-10.1177_20552076261420265 - Supplemental material for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis
Supplemental material, sj-tif-3-dhj-10.1177_20552076261420265 for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis by An Gu, An Huang, Bei Wu, Xueqi Liu, Cheng Huang, Xichenhui Qiu and Lina Wang in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076261420265 - Supplemental material for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis
Supplemental material, sj-docx-4-dhj-10.1177_20552076261420265 for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis by An Gu, An Huang, Bei Wu, Xueqi Liu, Cheng Huang, Xichenhui Qiu and Lina Wang in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076261420265 - Supplemental material for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis
Supplemental material, sj-docx-5-dhj-10.1177_20552076261420265 for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis by An Gu, An Huang, Bei Wu, Xueqi Liu, Cheng Huang, Xichenhui Qiu and Lina Wang in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076261420265 - Supplemental material for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis
Supplemental material, sj-docx-6-dhj-10.1177_20552076261420265 for Effectiveness of digital health interventions in improving mental health in older adults with mild cognitive impairment: A systematic review and meta-analysis by An Gu, An Huang, Bei Wu, Xueqi Liu, Cheng Huang, Xichenhui Qiu and Lina Wang in DIGITAL HEALTH
Footnotes
Acknowledgments
We want to express our gratitude to the National Natural Science Foundation of China (No. 72174061; 71704053), China Scholarship Council Foundation (No. 202308330251) and the Key Research and Development Program of Zhejiang Province (No. 2026C02A1146) for their support.
Author contributions
An Gu: Conceptualization, Methodology, Data curation, Writing-original draft. An Huang: Conceptualization, Methodology, Data curation. Bei Wu: Writing-review & editing. Xueqi Liu: Conceptualization, Methodology, Data curation. Cheng Huang: Supervision, Validation. Xichenhui Qiu: Supervision, Validation. Lina Wang: Conceptualization, Methodology, Validation, Writing-review & editing, Funding acquisition. All authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the China Scholarship Council Foundation, National Natural Science Foundation of China, and the Key Research and Development Program of Zhejiang Province (grant number 202308330251, 71704053, 72174061, 2026C02A1146).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data relevant to this study are included in the article and its supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.