
Abstract
Background
With dementia cases increasing worldwide, the demand for creative and accessible strategies to support cognitive health in at-risk older populations has become urgent. Mobile applications offer a valuable method for promoting cognitive wellbeing, particularly for independently living older individuals with mild cognitive impairment (MCI)
Objective
This preliminary study evaluated the feasibility and usability of a mobile-based cognitive training game among older Korean adults diagnosed with MCI.
Methods
A single-arm experimental design was adopted with 40 participants aged 65 and above who met eligibility criteria on the Korean Mini-Mental State Examination (K-MMSE). Participants used the Descartes Care application three times a week for 12 weeks. Feasibility was assessed through changes in game scores and completion times, while usability was evaluated using participant satisfaction, efficiency, learnability, safety, and intention to reuse.
Results
Thirty-eight participants completed the study. Significant improvements were observed in 69% (18 of 26) of mini-games for performance and efficiency (p < 0.05). In terms of feasibility, 88% (23/26) of subgames showed significant score improvements and 62% (16/26) demonstrated reductions in completion time, indicating consistent gains in performance efficiency. Regarding usability, the overall satisfaction score was 6.63, and the retention rate across the 12-week program was 95%, supporting a high level of user acceptability and sustained engagement. Mean scores across all usability domains exceeded 6.0, and participants reported strong intention to continue using and recommending the app.
Conclusions
Findings support the feasibility, safety, and acceptability of mobile technology-based cognitive training for older adults with MCI. This intervention shows promise as an accessible, engaging tool for cognitive health promotion. Future randomized controlled trials are needed to validate efficacy and assess long-term outcomes.
Keywords
Introduction
Dementia prevention has become a critical global public health focus due to a drastic increase in dementia prevalence that has resulted in over 55 million people currently living with dementia worldwide.1,2 Research outcomes have stressed the importance of participation in individualized programs and activities to lower dementia risk. 3 In a recent study, involvement in cognitively stimulating tasks and leisure-time physical activities effectively enhanced cognitive performance and decreased the likelihood of developing dementia.4–6 Substantial research findings have provided evidence that cognitive impairment and decline are associated with lower quality of life, and an increased risk of developing severe neurodegenerative diseases such as dementia.7,8 Recent research highlights that individuals with mild cognitive impairment (MCI) represent a particularly vulnerable population, as they face a heightened likelihood of progressing to dementia. Studies have provided evidence that the prevalence of MCI significantly rises with age, ranging from 6.7% among older adults aged 60–64 to approximately 25.2% in those aged 80–84. 9 These studies highlight the critical importance of early treatment or intervention to delay or reduce the risk of developing dementia in people living with MCI.7,8,10
In South Korea, older adults with MCI face unique challenges that may limit their successful engagement with digital health interventions. OECD (2023) data indicate that smartphone adoption rates among Korean seniors are approximately 40% lower than those of their Western counterparts, 11 and cultural norms rooted in Confucian values emphasize family-assisted care that may reduce acceptance of standalone technologies. 12 Additional obstacles include language barriers, low digital literacy, and culturally specific preferences, factors underscore the urgent need for mobile cognitive training solutions that are culturally adapted to improve accessibility, engagement, and adherence in this underserved population.
To address these barriers, we utilized the Descartes Care application, a mobile cognitive training program developed by Descartes Co., Ltd that incorporates simplified Korean-language interfaces, culturally relevant game content (e.g. traditional number games and hanbok-clad avatars), ultra-simplified navigation requiring only three taps to begin training, and a family-linked progress reporting system that aligns with intergenerational caregiving practices. Additional interactive features—such as visuals, rewards, reminders, and progress tracking—are included to enhance user engagement. This culturally tailored approach is supported by growing evidence that health interventions adapted to local cultural contexts can achieve significantly higher adherence and satisfaction rates compared to generic programs.13,14 Our study was specifically designed to bridge an identified gap by operationalizing these design elements to address the real-world needs of older Korean adults living with MCI.
The primary aim of this study was to evaluate the feasibility and usability of the Descartes Care intervention using objectives that were directly linked to measurable expected outcomes. We hypothesize that our culture-specific gamification features such as hanbok-clad avatars and traditional number games will achieve approximately 30% higher adherence rates compared to generic cognitive training applications. This hypothesis is grounded in prior findings that provided empirical evidence that culturally tailored health interventions can improve retention by 25–35%. 15 Accordingly, session completion rates were selected as the primary outcome measure to assess whether these culturally adapted design elements translated into higher sustained engagement among older Korean adults with MCI.
Background
Current state of the art
A growing body of literature suggests that mobile technology-based applications offer a wide variety of personalized and innovative features that encourage high levels of motivation and engagement by older adults.10,16,17 These studies have demonstrated that digital technologies play a significant role in preserving or improving the cognitive function of older adults, which helps to lower the risk of dementia.17–19 For example, Cho et al. 18 conducted a randomized controlled trial involving 101 older adults and reported notable enhancements in phonemic naming skills alongside increased prefrontal cortex activation. However, the absence of long-term follow-up in this study limited our understanding of sustained effects. Similarly, Kim et al. 19 implemented a 12-week mobile cognitive training program and found significant attention improvements, but excluded individuals with MCI, which restricted applicability to high-risk populations, and Lee et al. 20 reported that mobile cognitive training attenuated cognitive decline more effectively than paper-based programs.
Evidence from MCI-focused studies is promising yet limited. Lampit et al. 13 found that mobile technology-based interventions improved the attention, working memory, and adherence rates of MCI populations when compared to traditional methods. Han et al. 21 conducted a pilot study of 19 older adults with MCI, and reported a 95% retention rate and significant cognitive improvements after 60 training sessions with no adverse outcomes—highlighting feasibility, safety, and potential long-term engagement.
In addition to these findings, prior research findings have shown that mobile technology-based gamified cognitive training that incorporates interactive elements—such as visuals, sounds, rewards, reminders, and progress tracking—enhances the engagement of older adults.10,19,20 Such person-centered approaches have been associated with better adherence and improvements in attention and working memory compared to traditional methods.14,22 Despite these advantages, few current programs have been culturally tailored to address the linguistic, technological, and motivational needs of Korean older adults with MCI. A gap underscores the need for interventions that integrate evidence-based engagement features with culturally relevant adaptations.
Theoretical framework
Our intervention is grounded in well-established cognitive and motivational theories. Neuroplasticity research demonstrates that sustained and targeted cognitive challenges can stimulate neural reorganization, even in MCI populations. 15 This principle is operationalized in the Descartes Care application through adaptive difficulty algorithms that maintain optimal challenge levels for each user that maximize cognitive engagement and potential benefits.
In addition, this program incorporates Self-Determination Theory 23 that identifies autonomy, competence, and relatedness as key drivers of intrinsic motivation. Autonomy is supported through user choice in task selection and difficulty levels, while competence is enhanced by progressive achievement systems, real-time performance feedback, and personalized content, and relatedness is fostered through family-linked progress sharing and culturally familiar game elements. These features are designed to encourage sustained engagement and higher adherence rates by older adults.
The Descartes Care program
The Descartes Care program targets five cognitive domains—cognitive reasoning, linguistic ability, memory, calculative skills, and concentration—that are mapped to established neuropsychological frameworks. Each game within the program was reviewed and validated by an expert panel to ensure alignment with the intended cognitive targets. Pilot usability and feasibility testing with older adults (n = 15) confirmed that the tasks were culturally acceptable, well understood by users, and feasible to perform.
Methodology
Study design
This study employed a single-group experimental design to evaluate the feasibility and usability of a mobile game designed to improve the cognitive functioning of older adult users living with MCI. The mobile application was used by participants three times a week over a 12-week period, with each session lasting 1 h. Each session included the use of a variety of games targeting specific cognitive domains such as memory, attention, and problem-solving. Data on feasibility were collected at baseline and 12 weeks after the baseline.
Participant recruitment and data collection
Inclusion criteria targeted participants aged 65 or older who: (1) scored 20–24 on the Korean version of the Mini-Mental State Examination (K-MMSE), (2) possessed and demonstrated the ability to use a smartphone, and (3) were not currently participating in a similar technology-based program. Study exclusion criteria included: (1) diagnosis of dementia or other severe psychiatric or neurological disorders; (2) significant sensory impairment (uncorrected vision or hearing loss) or motor impairments preventing smartphone use; (3) failure to provide written informed consent in addition to agreeing verbally to participate; (4) inability to continuously participate in the game training sessions during the intervention period; or (5) prior use of other cognitive training games or similar programs.
Participants were recruited from Yeonhui Senior Welfare Center in Incheon, South Korea from May to June 2023. The research team obtained permission from the center director and provided an orientation session to potential participants. Once potential participants expressed interest in participating in the study, our research team conducted a screening process and provided them with detailed instructions on the purpose, procedures, and duration of the study. Following the signing of an informed consent form, participants received an introduction to the game app and instructions on how to use it. The app was then installed on their smartphones and preliminary training was conducted (30-min individual face-to-face training) to ensure that participants could use the app without difficulty. A total of 40 older adults diagnosed with MCI were initially recruited for the study. Of these, 38 participants (4 males and 34 females) successfully completed the intervention and were included in the final analysis. Specifically, two participants withdrew before completing the intervention, both due to difficulties in attending the scheduled training sessions consistently because of family caregiving duties. These reasons were unrelated to the intervention itself and were not associated with any adverse events. Ethical approval for the research was granted by the institutional review board at Catholic Kwandong University International St Mary's Hospital (IRB approval number: IS23EISE0031).
The Descartes Care program mobile technology-based intervention
The Descartes Care program was designed to reduce the risk of developing dementia by improving the cognitive function of users living with MCI. This application focuses on the comprehensive management of brain health using brain exercise games, home-based training, learning activities, and mindfulness instruction. It provides personalized cognitive health management services to users by customizing the difficulty and types of activities based on user interaction data. The Descartes Care program includes a variety of games and activities designed to engage and enhance (1) Reasoning, (2) Observation, (3) Memory, (4) Calculation, and (5) Attention.
The assignment of each game to a specific cognitive domain was based on established neuropsychological frameworks and evidence from prior research that demonstrated that targeted, game-based tasks can strengthen cognitive abilities.10,13,18,19,21 For example, matching and recall tasks have been shown to improve visual and spatial memory, while word-based games enhance lexical access and verbal fluency, as arithmetic and problem-solving tasks can enhance working memory and executive function. During the app design phase, domain assignments were validated through expert panel reviews involving neuropsychologists and occupational therapists that ensured precise theoretical alignment with cognitive training principles. In addition, pilot usability and feasibility testing with older adults (n = 15) confirmed that the intended cognitive targets of each game were understood by users, were feasible to perform, and supported their inclusion in the final program.
Participants had the option to select a suitable type of training program at an appropriate difficulty level when accessing the cognitive training on their personal mobile devices. Users were instructed to engage in sessions lasting roughly 1 hour each, three times per week. Representative screenshots from the mobile application are presented in Figures 1.
The Reasoning component of the Descartes Care program includes activities designed to enhance spatial awareness, response inhibition, problem solving, and memory. Hand Identification and Puzzle Assembly focus on spatial reasoning, while Rock-Paper-Scissors targets impulse control. Line Connection and Sequence Arrangement challenges participants to identify patterns and sequences and tests their attention and logical thinking, while the OX Quiz fosters quick and accurate decision making using general knowledge questions. The Observation segment of the Descartes Care program strengthens verbal fluency and lexical access through a series of targeted activities. The Word Typing game improves typing speed and language processing, Picture Match enhances word-picture association and vocabulary, Word Search develops quick lexical retrieval and pattern recognition, and the Initial Sound Game focuses on phonemic awareness and word recall. The Memory component of the Descartes program is focused on enhancing several aspects of memory including numerical recall, spatial memory, visual memory, linguistic memory, and location identification. Activities like the Lotto Number Recall challenge users to remember and reproduce numbers, Order Recall and Location Recall test the recall of sequences and specific locations to enhance spatial memory. The Matching Game boosts visual memory by requiring participants to find identical images, and English Sentence Construction exercises linguistic memory through asking the user to arrange words into sentences. The Calculation section of the Descartes Care program targets the strengthening of numerical and arithmetic abilities through a variety of tasks including Comparative Analysis that tests the ability of users to remember and compare numbers, Number Construction that involves creating specific numerical values through combinations or meeting set criteria, Addition Mastery and Arithmetic Operations that assess and improve computational skills and speed in basic math, and deep sea exploration, a unique activity that integrates memory skills with arithmetical tasks within an engaging thematic setting. The Attention segment of the Descartes Care program is designed to enhance focus and attentiveness through a set of tasks that require precise timing, rapid decision making, and attentive observation. The Elevation task challenges users to adapt to timing and speed changes, while the Jumping Obstacle and Layered Descent activity tests the ability of users to effectively navigate and respond to visual cues. The Unique Shape Identification and Directional Decision tasks focus on rapid recognition and decision-making skills. The Disoriented Navigation task strengthens concentration by requiring users to orient themselves and make decisions based on limited information.
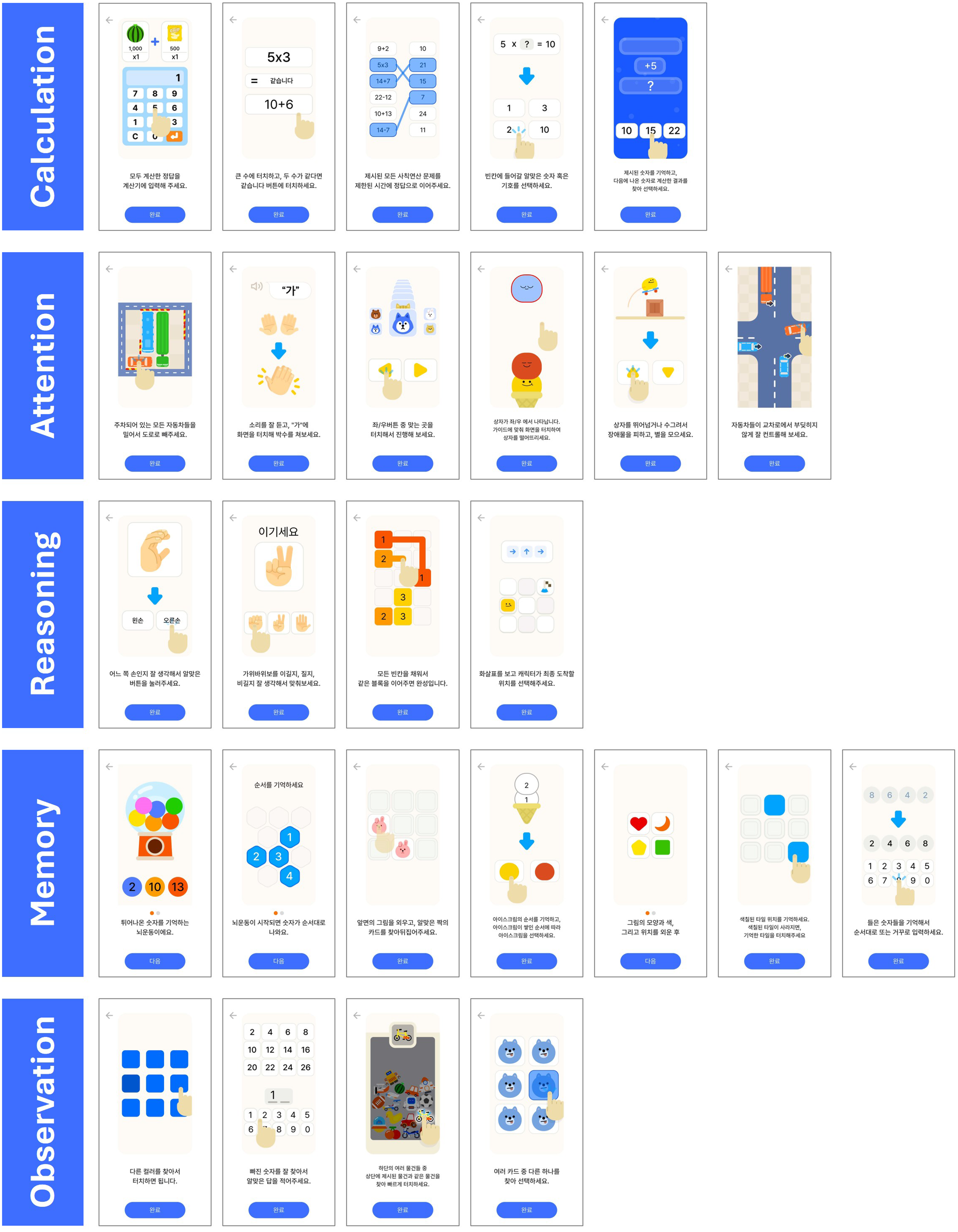
Representative of screenshots of cognitive training tasks across five domains in the Descartes Care program. Source: Descartes Co., Ltd.
Data measurement
During the initial session, participants provided baseline demographic and health information including age, sex, educational background, chronic conditions (e.g. hypertension, diabetes, hyperlipidemia), and lifestyle factors like smoking habits, alcohol consumption, physical activity. Participants also reported their initial perception of the feasibility of the mobile game. Data for evaluating feasibility were automatically recorded by the internal Descartes system and included game scores, number of correct answers, and duration of use. The same assessments were administered again at the end of the 12-week intervention. Feasibility analyses compared early and late phase data to assess changes in performance, with improvement defined as a statistically significant increase or decrease in scores/duration according to game-specific scoring rules (p < 0.05).
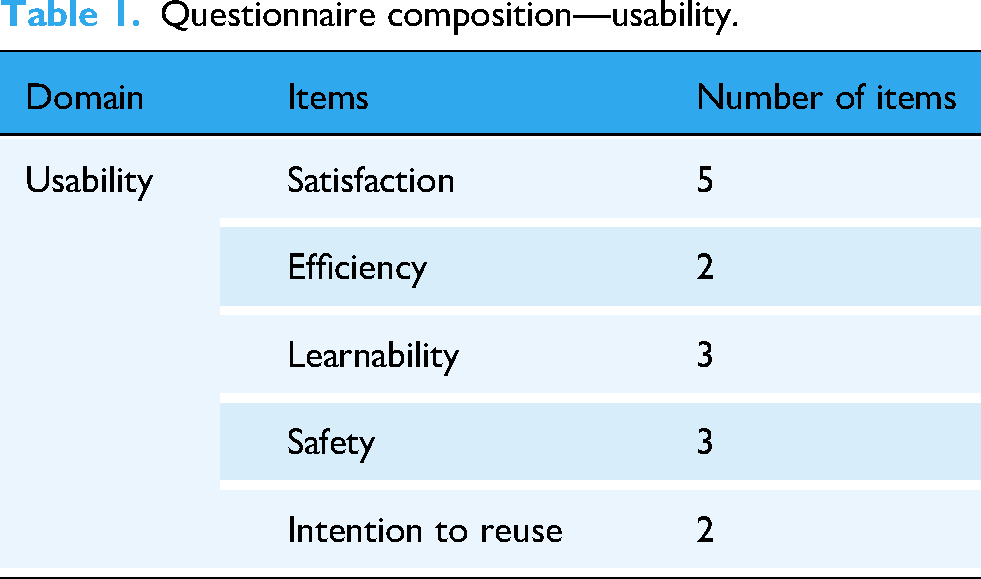
Usability was measured using a structured questionnaire developed by adapting items from established validated usability instruments 22 including the System Usability Scale (SUS) and prior mobile app usability frameworks, with modifications to reflect the cultural and linguistic context of older Korean adults living with MCI. Additional items were developed to assess safety (three items) and intention to reuse (two items) that were tailored to the specific requirements of the study population. Content validity was evaluated by a panel of three experts in cognitive rehabilitation, digital health applications, and gerontology. A pilot test with five older adults living with MCI was conducted to examine clarity, comprehensibility, and cultural relevance, the results of which were minor wording adjustments. The final questionnaire assessed five domains—Satisfaction (5 items), Efficiency (2 items), Learnability (3 items), Safety (3 items), and Intention to Reuse (2 items)—as detailed in Table 1. Internal consistency in the sample indicated acceptable to excellent reliability, with Cronbach's α values of 0.93 for Satisfaction, 0.86 for Efficiency, 0.87 for Learnability, 0.72 for Safety, and 0.78 for Intention to Reuse. All items were rated on a seven-point Likert scale ranging from 1 (“Strongly Disagree”) to 7 (“Strongly Agree”).
Questionnaire composition—usability.
Satisfaction was assessed using five items. Satisfaction refers to the level of comfort and enjoyment felt or the degree to which the expectations and needs of users are met. Therefore, satisfaction was measured using the following five items: “The product is generally likable in terms of comfort and enjoyment,” “The app content is engaging,” “App use is expected to be effective in meeting the expectations and desires of users for cognitive improvement,” “The app is novel and unique compared to other methods for cognitive improvement,” and “The app encourages voluntary participation in games.”
Efficiency refers to the ability of the user to complete tasks and was assessed by collecting speed and accuracy data using the following two sub-items. First, regarding accuracy: “The app provides training that accurately matches the purpose of cognitive improvement.” Second, regarding the usage speed: “The composition and amount of the content provided by the app are appropriate.”
Learnability refers to how easily a user can use a system they are encountering for the first time without referring to guides or documentation. In this study, learnability was measured using the following three items: “The game app's menu configuration is convenient,” “The information presented on the screen is clear and precise,” and “The progress and results of the game can be easily checked on the provided screen.” Participants rated each statement using a seven-point Likert scale, ranging from 1 (“Strongly Disagree”) to 7 (“Strongly Agree”).
Data analysis
The data was analyzed using Stata version 18.0 software descriptive statistics and paired t-tests. First, to evaluate the feasibility of the game, data from game usage (e.g. scores, number of correct answers per attempt, and duration of use) were used. The initial 10% and final 10% of game session data were compared to assess changes between early and late stages of the intervention. This approach was used to reduce the influence of day-to-day performance fluctuations, account for initial familiarization with the games, and capture stable performance trends toward the end of the program. This method has been used in previous cognitive training studies to provide a clearer comparison of early versus late-phase outcomes while minimizing mid-program variability. Paired sample t-tests were then conducted to compare mean scores before and after the intervention within each group.
The threshold for statistical significance was established at p < 0.05. To assess usability (user experience and perception), factors including satisfaction, usability, safety, and intention to use were measured. Descriptive statistics were used to calculate mean values to identify the central tendencies of the data for each factor.
We analyzed log data from 38 participants who engaged in the Descartes cognitive-training game over a 12-week period (three 1-h sessions per week). Only completed plays were included in the analysis. For each mini-game, the play sequence was ordinalized per participant, and the relative position within each participant × game series was computed. The earliest 10% of plays was designated as the early phase and the latest 10% as the late phase. Performance for each phase was summarized by the median, yielding paired early–late observations as the unit of analysis.
The Normality of paired differences was assessed using the Shapiro–Wilk test. When normality was met in both phases, a paired t-test was applied; otherwise, the Wilcoxon signed-rank test (two-sided, α=0.05) was used. Effect sizes were calculated as Cohen's d for t-tests and as r = |z|/√N for Wilcoxon tests, with magnitude interpreted according to conventional thresholds.
Because scoring rules varied for each game, the interpretation of score changes was game-specific: in nine games (game ids 1, 3, 5, 6, 7, 13, 16, 17, and 23), higher scores reflected better performance (direct relationship), whereas in the remaining games, lower scores indicated better performance (inverse relationship). For duration of use, lower values indicated better performance in all games. Median change scores (Δ = late − early) were interpreted in alignment with these rules.
Result
Demographic features
The average age of the study participants was 76.94 years (SD = 6.69), and the majority possessed at least a secondary education. Most participants were in generally good health, and though some participants reported chronic conditions such as hypertension or diabetes, these conditions did not interfere with their successful participation in the study.
Feasibility
Duration
Paired analysis of per-game duration outcomes.
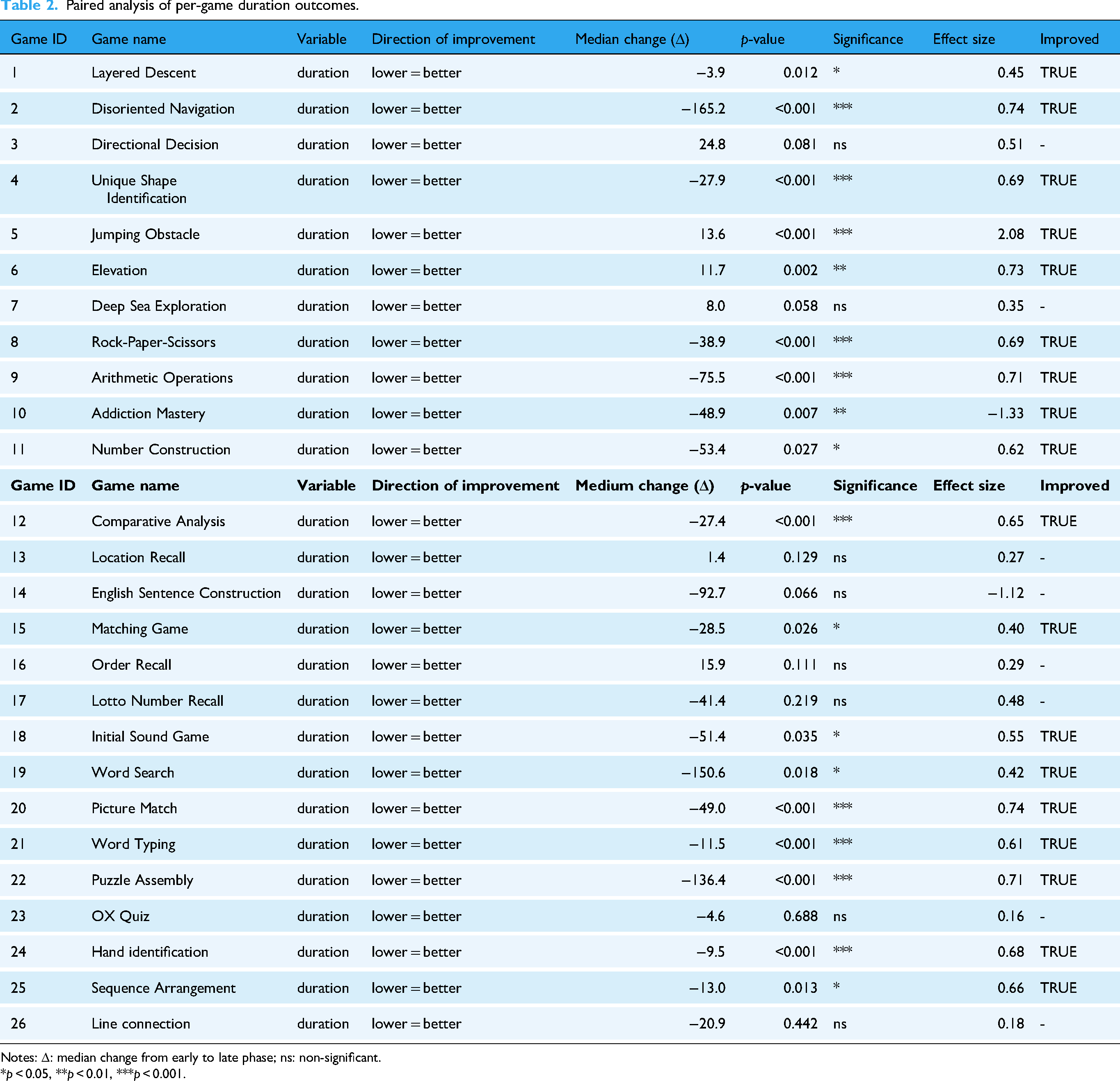
Notes: Δ: median change from early to late phase; ns: non-significant.
*p < 0.05, **p < 0.01, ***p < 0.001.
Score: Among the 26 mini-games with valid paired comparisons, 23 exhibited statistically significant improvements in late-phase performance relative to the early phase, while 3 did not reach statistical significance. Effect sizes, which varied from small to large, are presented in Table 3.
Paired analysis of per-game score outcomes.

Notes: Δ: median change from early to late phase; ns: non-significant.
*p < 0.05, **p < 0.01, ***p < 0.001.
Overall, improvements in both time efficiency (shorter duration) and task performance (higher scores) were consistently observed across multiple mini-games. The analytic procedure—phase-based comparison, normality-contingent choice of paired tests, and concurrent reporting of statistical significance and effect sizes—was designed to capture game-specific performance characteristics while conveying both inferential and practical importance.
Usability
The usability assessment of the cognitive improvement mobile game provided evidence that the majority of participants were satisfied with the game. The survey responses regarding satisfaction, learnability, efficiency, safety, and intention to reuse were predominantly positive, with most items scoring above six on a seven-point scale, which indicates that the elderly participants in the study were generally satisfied with and enjoyed using the game. Responses in the safety, efficiency, and satisfaction domains were evenly distributed, suggesting a positive impact on participant intention to continue using the game in the future.
Satisfaction was measured using five items, and mean scores for each satisfaction item are presented in Table 4. The highest scores among these items were for the overall likability of the app and its ability to include voluntary participation, both scoring 6.47. This indicates a high level of likability related to using the app that leads to an increase in user intention to participate voluntarily in games compared to other satisfaction measures. The perception of app effectiveness for cognitive improvement scored 6.39 (compared to similar apps scoring 6.26), and the perception of content engagement scored 6.24. Overall app satisfaction was measured at 6.63. This overall satisfaction score was not calculated as the average of the five detailed satisfaction items, but rather assessed as an independent item. This finding provides empirical evidence that the overall satisfaction score exceeded the arithmetic mean of the five detailed items, which was 6.36. Moreover, overall satisfaction was higher than any of the sub-section user satisfaction scores, reflecting a very positive user perception of the app as a whole.
The result of satisfaction mean scores.

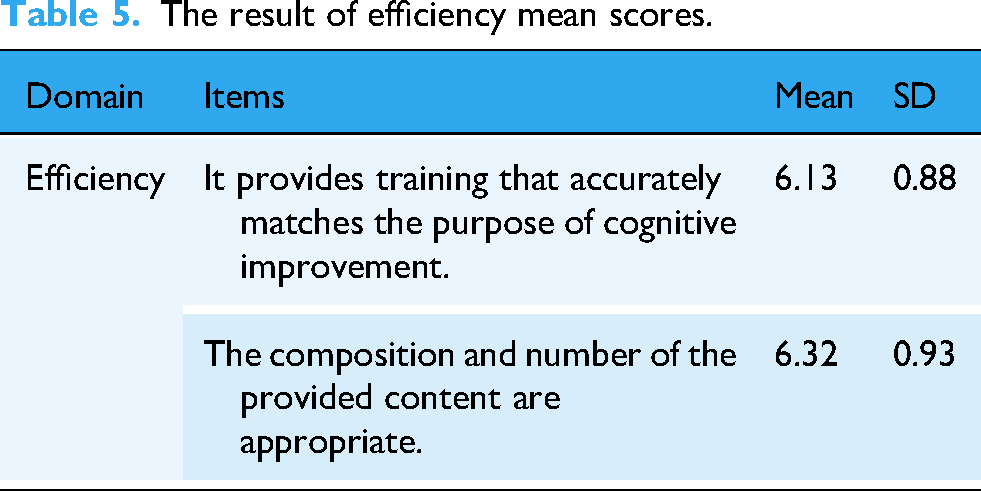
In the efficiency results, the aspect with the lowest average score (6.13) pertained to the alignment of training with the purpose of cognitive improvement, as shown in Table 5. We believe that this somewhat lower score is related to ambiguities that users may have experienced in two areas. First, there was potential uncertainly regarding the expectation that cognitive improvement effects will result from using the app. As users encountered the app for the first time, they may have found it difficult to accurately assess whether the cognitive improvement effects would or were occurring. Second, there was a lack of understanding about the cognitive improvement training itself. Despite these ambiguities, the high absolute value of satisfaction responses indicates that users held a very positive perception of the relationship between app use and cognitive improvement. Further, the perception of content diversity (6.32) was slightly higher than the perception of accurate training (6.13). This suggests that, given the elderly target audience, the app provided an adequate variety of content to accomplish the assigned tasks.
The result of efficiency mean scores.
Learnability was measured using three items. The response to the question that asked if the information provided on the interface was easy to understand and accurate scored a high 6.29, as presented in Table 6. However, the convenience of the app menu configuration (6.18) and the ease of checking game progress and results on the interface (6.05) were relatively lower. This indicates that, from the user perspective, there was a lower level of understanding of the app interface structure compared to its utility and information comprehensibility. In other words, when users had less experience with digital devices, it is necessary to supplement the app with usage explanations such as tutorials to improve the overall user experience.
The result of learnability mean scores.

The assessment of the level of comfort experienced by users of the cognitive improvement training game app resulted in a score of 6.29, as detailed in Table 7. This score indicates a low level of reluctance to use the app that will, it is assumed, potentially enhance the likelihood of voluntary use. Additionally, the response to the question that assessed whether there was a possibility of harm due to incorrect information when using the app scored 2.03, suggesting a very high level of trust in the information provided. The overall satisfaction score reported by participants with the perceived safety of the app was 6.34, which is somewhat lower than the overall satisfaction with app usage (6.63). This suggests that contextual factors such as limited prior familiarity with the app should be taken into consideration given that the primary users were older adults whose association with mental stability, risks of information errors, and a general lack of affinity with digital devices should be considered.
The result of safety mean scores.

Regarding intention for continued use, the intention to continue using the app for cognitive improvement scored 6.53 (Table 8), indicating a high level of positive perception. Further, the intention to recommend the app to others scored a similar 6.50, suggesting high reliability in responses regarding overall satisfaction with app usage, safety, and efficiency.
The result of intention to reuse mean scores.

Discussion
We examined the feasibility and usability of a mobile technology-based game application among older Korean adults living with MCI. The overall results of this study indicate that participants reported high levels of satisfaction, usability, ease of learning, perceived safety, and willingness to reuse the app. Improvements were also observed in game performance metrics that suggest that the intervention was both engaging and easy to adopt. These results suggest that mobile-based interactive games may serve as an accessible and engaging tool to support cognitive health in this population.
Although standardized neuropsychological tests were not administered, the observed gains in in-game performance provide preliminary evidence of potential cognitive benefits that are aligned with the findings of previous studies that reported the cognitive benefits of mobile-based multi-domain interventions,19,20 as well as prior evidence showing that digital technology can improve cognitive function and serve as a dementia prevention strategy for older adults at high risk of dementia.10,13,20,21 Our findings are consistent with this literature and support the feasibility, safety, and acceptability of mobile technology-based cognitive training for Korean older adults living with MCI.
Mobile technology-based interventions have been shown to increase adherence rates and strengthen certain cognitive functions (e.g. memory and working memory) of older adults.13,21 These merits—particularly their ability to individualize training and sustain engagement—are reflected in our high safety, efficiency, and satisfaction scores, and in the strong intention reported by participants to continue use and to recommend the app to others. Such results indicate strong user receptivity that can serve as a foundation for the ongoing refinement and development of the intervention.
Future research should focus on further enhancing these positive user experiences by continuously updating app features and content, and by actively incorporating user feedback. Doing so may further improve long-term user adherence and the real-world impact of the intervention.
Limitations and future directions
Several limitations to the interpretation of our study findings must be acknowledged. First, the single-group design limited our ability to attribute observed improvements solely to the intervention. Without a passive waitlist or active control (e.g. traditional paper-based cognitive exercises), we cannot rule out potential practice effects from repeated testing or placebo responses as explanations for the observed improvements.
Second, the non-blinded nature of the trial may have introduced bias. Participants were aware of receiving an experimental intervention and may therefore have exhibited Hawthorne effects, and researchers conducting assessments may have been influenced by expectation bias. Most usability items exhibited high mean values (6.1–6.6 out of 7) with relatively low variability (SD < 0.6), indicating a potential ceiling effect. Such restricted variance may have reduced the ability of the instrument to detect differences between subgroups or changes over time. Potential contributing factors include social desirability bias, limited perceived anonymity during survey administration, and the influence of item phrasing or the evaluative context of response patterns. These factors should be considered when interpreting our findings, and future studies should incorporate blinded assessment procedures to minimize these risks.
Third, reliance on self-reported usability surveys poses a methodological limitation. Social desirability and acquiescence biases—particularly among older Korean adults—may have inflated satisfaction scores.
Fourth, recruitment from a single senior welfare center in Incheon may have introduced selection bias, and the gender imbalance (34 women, 4 men) further limits generalizability. Lifestyle factors collected at baseline were not analyzed in relation to outcomes as they were intended for descriptive purposes. Recruiting more diverse and gender-balanced samples across multiple sites will be important in future research to enhance external validity.
Fifth, no structured observations of participants interacting with the application were conducted. Such data could have provided insights into any navigation related challenges that were experienced by participants, interaction patterns, and unreported usability barriers.
Finally, the 12-week intervention period may have been insufficient to induce measurable neuroplastic changes. The duration was chosen for operational feasibility and to minimize participant burden, but the absence of follow-up prevents definitive conclusions about the sustainability of benefits.
Future studies should address these limitations by employing randomized controlled trials that include an active control condition, thereby enabling more definitive conclusions regarding the efficacy of the intervention, incorporating blinded assessment procedures, integrating objective behavioral metrics (e.g. login frequency, session duration, dropout rates) with self-reports, recruiting a more diverse and sex-balanced sample across multiple sites, analyzing relevant lifestyle and demographic moderators, extending the duration of the intervention beyond 12 weeks, and including follow-up assessments (e.g. at six months post intervention) to evaluate the persistence of effects.
Conclusion and future research
Despite these limitations, the findings of this study confirm the practicality and user acceptance of a mobile application designed to enhance the cognitive functions of older adults living with MCI. The 95% retention rate observed in this study notably exceeded the ∼60% average reported for paper-based cognitive training programs, 13 highlighting the potential of gamified digital platforms to address adherence challenges that often undermine the success of traditional MCI interventions. This is particularly significant given that poor adherence is a major reason for failed cognitive training trials in older adults with MCI and mild dementia. 24 Culturally tailored and gamified approaches such as ours may enhance the long-term viability and scalability of cognitive interventions for this population, and sustain engagement.
Building on these findings, we recommend a three-phase validation process to further establish the effectiveness, scalability, and real-world applicability of this intervention:
For clinicians, the findings of our study suggest that mobile technology-based cognitive interventions could be prescribed as adjunct therapy during the critical period between MCI diagnosis and dementia onset. For policymakers, the high adherence rates observed in this study provide a rationale for initiating pilot subsidy programs to increase accessibility, particularly in rural and underserved areas with limited availability of cognitive specialists. Moreover, the customizable features of this app have the potential to facilitate its integration into national dementia prevention strategies, enabling adaptation to diverse cultural, linguistic, and regional contexts.
Overall, the findings of our study offer foundational evidence to support the development and expansion of personalized, culturally relevant cognitive health initiatives for aging populations who are living with MCI. Continued refinement of the intervention, coupled with rigorous multi-site trials and long-term follow-up, are essential for confirming its effectiveness and ensuring its sustainability in real-world practice.
Footnotes
Acknowledgements
The authors gratefully acknowledge the technical and logistical support provided by Descartes Co., Ltd under Project No. 20230106.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of Catholic Kwandong University International St Mary's Hospital (IRB approval number: IS23EISE0031).
Contributorship
Areum Han led the conceptualization and design of the study, and drafted the initial manuscript. Junhyoung Kim and Yong Seop Kim made substantial contributions to data analysis and were involved in revising the manuscript critically for important intellectual content. Sang Joon An and Hyo Jin Ju jointly served as corresponding authors, supervising the overall research process and providing critical manuscript revisions. Sol Jung and Heeyong Choi contributed to data collection and interpretation. All authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from Descartes Co., Ltd (Project No. 20230106).
Declaration of conflicting interests
The authors declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.