
Abstract
Background
Digital health interventions are transforming hypertension management, yet the evolution and focus of this research domain remain underexplored. This study provides a comprehensive bibliometric analysis of global research trends and hotspots in digital health for hypertension management.
Methods
Relevant publications were retrieved from the Web of Science Core Collection. Bibliometric and visualization analyses were conducted using VOSviewer, CiteSpace, and R-Bibliometrix, covering the period from 1992 to 2025.
Results
A total of 1368 English-language articles, authored by 8918 researchers from 5268 institutions in over 100 countries/regions, were identified. These articles appeared in 435 journals, with publication output showing rapid growth since 2011 and peaking in 2022. The United States led in both productivity and international collaboration, with Duke University, the University of California System, and Harvard University as the top institutions. Bosworth HB emerged as the most prolific and influential author, while JMIR mHealth and uHealth and the Journal of Medical Internet Research were the leading journals. Keyword co-occurrence analysis revealed five major research clusters: (1) Digital interventions and patient management; (2) Population health and lifestyle factors; (3) Clinical practice, guidelines, and measurement; (4) Disease burden, outcomes, and epidemiology; and (5) Health equity, access, and technology utilization. Evidence suggests that digital health interventions improved patient self-management, medication adherence, and blood pressure control, highlighting their potential for better clinical outcomes. Recent burst keywords such as “burden,” “telehealth,” “meta-analysis,” and “United States” indicate shifting research priorities toward implementation, health equity, and real-world impact.
Conclusion
This study identified rapid growth and diversification in digital health research for hypertension, with the United States, leading academic institutions, and journals such as JMIR mHealth and uHealth at the forefront. Five major research clusters were revealed, spanning digital interventions, clinical practices, lifestyle factors, disease burden, and health equity. Recent trends show increased focus on telehealth, implementation challenges, and equity of access. Future research should further integrate digital health solutions into routine hypertension care, address disparities, and systematically evaluate their real-world impact.
Introduction
Hypertension represents a significant contributor to the global burden of disease, affecting approximately 1.4 billion adults worldwide, according to the latest statistics from the World Health Organization, with its prevalence markedly increasing. 1 As a principal risk factor for cardiovascular disease, hypertension imposes substantial social and economic burdens, leading to increased healthcare costs, diminished workforce productivity, and premature mortality. 2 Nonetheless, despite the well-documented benefits of blood pressure (BP) reduction, overall control of hypertension remains insufficient, with less than one-fifth of patients globally achieving adequate management. 3 Challenges such as poor adherence to complex medication regimens, the presence of associated side effects, and the heterogeneity of hypertensive populations exacerbate this issue.4,5 There remains a deficiency in effective strategies for the management of hypertension.
In recent years, the management of hypertension has undergone a significant transformation, moving from a purely pharmacological perspective to a more integrated and patient-centered approach. Modern hypertension management emphasizes not only medication but also lifestyle modification, patient empowerment, and self-management strategies. Self-management—including home BP monitoring, behavioral interventions, and patient education—has been shown to enhance patient engagement and improve long-term outcomes. 3 The incorporation of digital technologies has further expanded the possibilities for individualized care and continuous support.
In response to these challenges, digital health technologies have emerged as promising instruments in healthcare, particularly for the management of chronic diseases such as hypertension. 6 These technologies facilitate remote monitoring, personalized treatment plans, and mobile applications specifically designed for hypertension management.7,8 By leveraging data analytics and artificial intelligence, digital health solutions can effectively address adherence issues, monitor BP trends, and provide timely interventions.9,10 However, despite their potential, digital health technologies also present several challenges, including data privacy concerns, interoperability issues, and the necessity for robust validation studies.11,12
Beyond general digital health, there has been increasing interest in digital interventions and digital therapeutics for nonpharmacological management of hypertension. Recent research highlights the effectiveness of digital interventions—including web-based programs, mobile apps, and digital therapeutics platforms—in delivering behavioral therapy, lifestyle coaching, and self-management support without relying solely on medication. These nonpharmacological digital approaches have demonstrated promising results in lowering BP, improving adherence, and facilitating sustained lifestyle changes, especially in populations with limited access to traditional care models. 6
Bibliometrics is a quantitative method for analyzing scientific literature, offering insights into research productivity, collaboration, and trends. 13 Although studies have examined digital health and hypertension management separately,14–16 an integrated analysis is lacking. The primary aim of this study is to systematically map and analyze global research trends, influential contributors, and collaborative networks in digital health for hypertension management from 1992 to 2025. The secondary aim is to identify emerging research hotspots, thematic clusters, and gaps in the literature, thereby providing evidence-based guidance for prioritizing future research directions and supporting the development of personalized hypertension management strategies.
Materials and methods
The literature search for digital health in hypertension management was conducted on the Web of Science Core Collection (WoSCC), a multidisciplinary academic literature abstract and index database that provides access to global academic information. 17 The search formula was (TS = (“digital health” OR “digital health care” OR “digital medicine” or “eHealth” OR “eHealth care” OR “e-medicine” OR “telehealth” OR “tele-health” OR “telehealthcare” OR “tele-healthcare” OR “telemedicine” OR “tele-medicine” OR “mHealth” OR “m-health” OR “mHealthcare” OR “m-healthcare” OR “mobile health” OR “mobile healthcare” OR “mobile medicine” OR “online health” OR “online healthcare” OR “online medicine” OR “digital intervention” OR “digital therapeutic” OR “digital therapeutics”)) AND TS = (Hypertension OR “High Blood Pressure*”).18,19 The search was conducted on September 3, 2025. Only English-language articles were included, and non-English and other publication types (e.g., conference abstracts, letters, editorials) were excluded. Studies were included if they: (1) focused on digital health, digital interventions, or digital therapeutics in hypertension management; (2) were original research articles or reviews; and (3) were published in English. Studies were excluded if they were conference abstracts, editorials, letters, or not directly related to the topic. All retrieved records were exported in text format from WoSCC. The extracted data included publication year, title, author names, affiliations, countries/regions, keywords, journal name, and citation counts. Two independent researchers performed screening and data extraction. Discrepancies were resolved by discussion or by consulting a third researcher. The study also conducted a PubMed search for clinical studies, including randomized controlled trials and observational studies, related to digital health in hypertension.
Statistical analysis
The relevant data were obtained from bibliographic records, with bibliometric indicators being calculated by Microsoft Excel. A thorough academic analysis was then carried out utilizing visualization tools including VOSviewer (V 1.6.20), CiteSpace (V 6.3.R1), and R-Bibliometrix 4.3.3. VOSviewer depicted the co-occurrences of countries, institutions, authors, and keywords within the selected literature, revealing key research themes and collaborations. 20 In these network maps, nodes represented these entities, with their size reflecting the frequency of occurrence and color distinguishing between research clusters or indicating the average publication year for keywords. Thicker lines connecting the nodes denoted stronger co-occurrence relationships. 21 CiteSpace examined the burst of research trends regarding digital health in hypertension management over time. 22 This analysis spanned from January 1992 to September 2025, utilizing keywords as node types and slicing the data annually. A visual timeline was generated, highlighting the top 5 keywords in each slice through a combined pruning method. The resulting maps exhibited clusters of research topics, where the color gradient indicated the duration of research activity across time. 23 R4.3.3 enabled advanced statistical analysis and the computation of bibliometric indices, such as the H-index, G-index, and M-index, for prominent authors and institutions. 24 Specifically, the H-index assesses both productivity and citation impact, the G-index focuses on a broader range of citation counts, and the M-index strikes a balance between paper production and citations.25,26 In this study, the authors’ H-indices were directly retrieved from the WoSCC database. To assess journal influence, Journal Citation Reports metrics were utilized, including the impact factor (IF) for 2023 and quartile ranking (Q1–Q4) for 2023. The IF measures the average number of citations per article published in the journal within a year, while quartile ranking divides journals into four impact groups, with Q1 representing the highest tier of journals.
Results
Overview of publications
According to the updated search strategy, a total of 1980 studies on digital health in hypertension management were initially identified in the WoSCC (Figure 1). After screening and exclusion of non-original research types and non-English records, 1368 English-language articles were ultimately included for subsequent analysis. These publications represent the work of 8918 authors from 435 sources, with contributions from international collaborations accounting for 26.17% of articles. The research was published across a wide range of journals, referencing 39,582 sources and utilizing 2577 unique author keywords (Figure 2A). On average, each publication received 19.39 citations, and the average number of coauthors per document was 8.35.

Flowchart of the bibliographic retrieval process.

Analysis of the general information. (A) A summary of quantitative analysis of the publications. (B) Annual output of research.
From 1992 to 2025, the annual growth rate of publications in this field was 15.92%. In the early years (1992–2010), the annual number of publications remained very low, often fewer than 10 articles per year. However, from 2011 onward, a marked increase was observed, with publication numbers rising rapidly and peaking at 192 articles in 2023. By 2025, the cumulative number of publications reached 1368 (Figure 2B). The most cited article in this field was “Design of an mHealth app for the self-management of adolescent type 1 diabetes: a pilot study” published in Journal of medical Internet research (IF 2023 = 5.8) in 2012 with a total of 449 citations, 27 followed by “Self-monitoring of blood pressure in hypertension: A systematic review and individual patient data meta-analysis” published in PLOS medicine (IF 2023 = 10.5) in 2017 (425 citations), 28 and “Cuffless Blood Pressure Estimation Algorithms for Continuous Health-Care Monitoring” published in IEEE transactions on bio-medical engineering (IF 2023 = 4.4) in 2017 (410 citations) 29 (Table S1).
Distribution and collaborative networks of countries
A total of 1368 articles originating from multiple countries and regions were analyzed. The United States was the clear leader, contributing 543 articles (39.7% of the total), with the highest number of multiple country publications (MCP = 75) and a total of 10,879 citations, giving an average of 20 citations per article. China ranked second, with 144 articles (10.5%), 29 MCPs, and a total of 2119 citations (average 14.7 citations per article). The United Kingdom was third in total publications (52 articles), with a notably high MCP ratio (0.404) and 1569 total citations (TCs) (average 30.2 citations per article) (Figure 3A, Table S2). Among the 103 countries involved in international collaborations with a minimum of 1 article, the United States had the highest number of collaborations (strength = 386), mainly with India, Canada, and the United Kingdom. Furthermore, the United Kingdom (strength = 298) and Canada (strength = 165) ranked second and third in collaborations, respectively (Figure 3B).
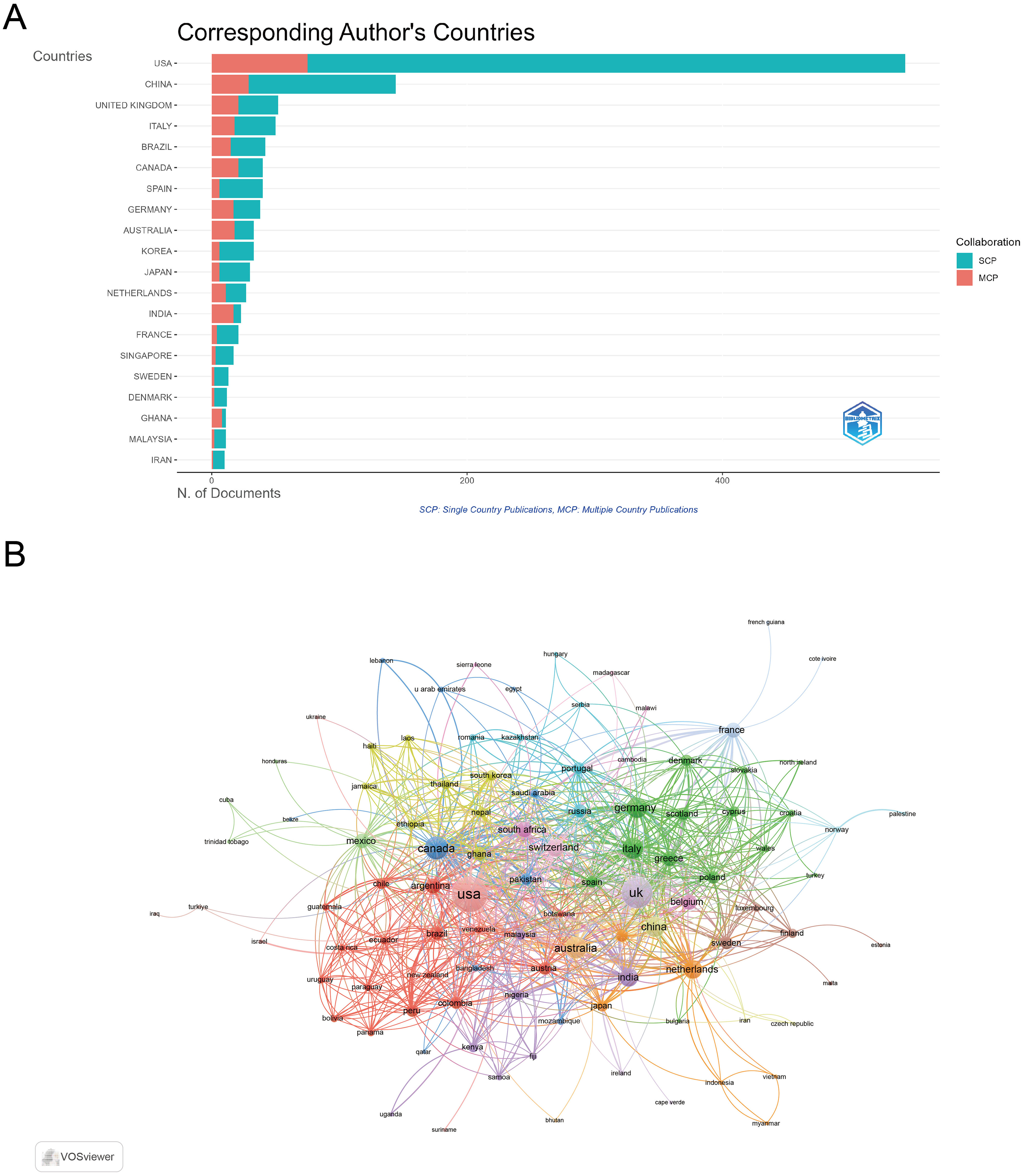
Analysis of countries. (A) Distribution of responding author's publications by country. (B) Visualization map depicting collaboration among different countries.
Distribution and collaborative networks of institutions
A total of numerous institutions contributed to the publication of relevant articles in the field. Among the top 10 most productive institutions, Duke University stands out as the leading contributor with 227 articles. This is followed by the University of California System with 128 articles, and Harvard University with 105 articles (Figure 4A). Among the 130 institutions engaged in international collaborations with at least six articles, Duke University boasted the highest number of collaborations (strength = 74). It was closely followed by the Harvard University (strength = 72) and the The London School of Hygiene & Tropical Medicine (strength = 67) (Figure 4B).

Analysis of institutions. (A) Top 10 institutions ranked by article count. (B) Visualization map depicting collaboration among different institutions.
Authors and coauthors
A total of 8918 authors contributed to the publications in this field. Bosworth HB emerged as the most prolific and influential author, with an H-index of 18, G-index of 35, M-index of 0.95, and the highest total number of publications (TP = 37) as well as TC (1272). Omboni ranked second, with an H-index of 12, G-index of 18, M-index of 0.80, and 18 publications with 1012 citations. Parati et al. also demonstrated high impact, with an H-index of 12, G-index of 13, and 13 publications accumulating 1082 citations (Table S3).
The cooperation network diagram among authors examined the 197 authors involved in international collaborations with at least three articles, revealing the formation of several distinct research clusters differentiated by various colors. Bosworth had the highest number of collaborations with other authors (strength = 151), followed by Prabhakaran (strength = 93) and Jindal (strength = 90) (Figure 5).

The visualization map depicting collaboration among authors.
Contributions and collaborative networks of journals
The publications in this field were distributed across a total of 435 journals. Among these, JMIR mHealth and uHealth (IF 2024 = 6.2, Q1) achieved the highest H-index of 26, followed closely by the Journal of Medical Internet Research (IF 2024 = 6.0, Q1) with an H-index of 25 and the highest total number of publications (TP = 83) and citations (TC = 1194) among all journals. Telemedicine and e-Health (IF 2024 = 2.0, Q3) ranked third in H-index (20), with strong publication output as well. Notably, the journal Hypertension had the highest IF (2024 = 8.2, Q1) within the list, reflecting its prominence in cardiovascular research, while also maintaining a high TC count (TC = 1006) (Table S4).
In the Journal co-occurrence network, the frequency of joint citations among journals within the same articles is measured, where strong links signify thematic convergence. Among 98 journals with at least three occurrences, the three key journals with the highest total link strength were JMIR mHealth and uHealth (strength = 188), Journal of Medical Internet Research (strength = 188), and Journal of Hypertension (strength = 108) (Figure 6A).

Analysis of journals. (A) The co-occurrence networks of journals. (B) The coupling networks of journals.
The journal coupling network evaluates interconnectedness by examining common references in articles, with strong links indicating substantial overlap in these references and highlighting a shared intellectual foundation. Among 98 journals with at least three couplings, the three key journals with the highest total link strength were Journal of Medical Internet Research (strength = 6.875), JMIR mHealth and uHealth (strength = 5721), and Trails (strength = 3814) (Figure 6B).
Keyword coexistence network and burst keywords
A total of 125 keywords with at least 10 occurrences were identified and mapped for co-occurrence network analysis (Figure 7A). These keywords were grouped into five major clusters, each representing a distinct research theme: Cluster 1 (Red): Digital Interventions and Patient Management. This cluster centers on keywords such as “adherence,” “intervention,” “care,” “self-management,” “primary-care,” and “outcomes,” reflecting research on implementing and evaluating digital health interventions, patient engagement, and therapy optimization. Cluster 2 (Green): Population Health and Lifestyle Factors. Comprising terms such as “adults,” “behavior-change,” “risk,” “obesity,” “physical-activity,” “medication adherence,” and “mhealth,” this cluster addresses epidemiological studies, behavioral interventions, and risk reduction in various populations. Cluster 3 (Blue): Clinical Practice, Guidelines, and Measurement. Including “hypertension,” “management,” “guidelines,” “trial,” “home blood-pressure,” “self-measurement,” “validation,” and “system,” this cluster represents studies focusing on diagnostic accuracy, guideline implementation, and monitoring strategies. Topics such as diabetes and obesity appear in this cluster because they are frequently studied as comorbid conditions within hypertension research, reflecting their shared risk factors and overlapping management approaches. Cluster 4 (Yellow): Disease Burden, Outcomes, and Epidemiology. Keywords here include “burden,” “prevalence,” “mortality,” “cardiovascular-disease,” “epidemiology,” “experience,” and “global burden,” highlighting research on disease impact, health outcomes, and population-level trends. Cluster 5 (Purple): Health Equity, Access, and Technology Utilization. This group features terms such as “access,” “disparities,” “barriers,” “telehealth,” “technology,” “telemedicine,” “united-states,” and “women,” underscoring studies on healthcare accessibility, digital divides, and equity in digital health deployment.

Analysis of keywords. (A) Visual analysis of keyword co-occurrence network. (B) Visual analysis of keyword co-occurrence network (temporal evolution). (C) Top 20 keywords with the strongest citation bursts. (D) Visual analysis of keyword co-occurrence network based on PubMed database.
The temporal co-occurrence map (Figure 7B) shows an evolution in research focus over time. Early years (2017–2018, dark blue) were characterized by foundational themes such as “system,” “reliability,” and “self-measurement.” From 2019 onward (green to yellow), attention shifted to “risk,” “adults,” “prevalence,” “burden,” and “cardiovascular disease,” reflecting growing interest in real-world effectiveness, population impact, and advanced management strategies.
Analysis of keyword citation bursts (Figure 7C) further highlights these trends. From 2001 to 2010, “system” and “reliability” dominated, indicating a focus on foundational digital infrastructure. Between 2012 and 2015, keywords such as “interventions,” “home telehealth,” “technology,” and “randomized controlled trial” experienced rapid growth, reflecting early clinical evaluations of digital solutions. In subsequent years, keywords such as “prevention,” “guidelines,” “mobile phone,” and “atrial fibrillation” emerged as new hotspots. Most recently, since 2021, terms including “burden,” “telehealth,” “united states,” and “physical activity” have shown the strongest citation bursts, indicating a transition toward research in implementation, equity, and broader public health impact.
Clinical evidence from PubMed-indexed studies
Our targeted PubMed search identified a total of 377 clinical studies on digital health in hypertension, encompassing both randomized controlled trials and observational studies. A cluster analysis revealed five main research themes (Figure 7D). PubMed Cluster 1 (Red): Chronic Disease Management. This cluster focuses on using “mobile technologies” and “applications” to manage chronic diseases such as hypertension, atrial fibrillation, and stroke, emphasizing how “clinical trials” and “lifestyle interventions” can improve patients’ quality of life. PubMed Cluster 2 (Green): Blood Pressure Monitoring in Specific Populations. This cluster centers on BP monitoring for hypertension, with a particular focus on “pregnancy-related conditions” such as “preeclampsia.” It also addresses the feasibility of “digital health” interventions delivered by “community health workers” in the “public health” domain. PubMed Cluster 3 (Blue): Mobile Health (mHealth) for Diabetes and Obesity. This cluster explores the use of “mHealth” in managing “diabetes” and “obesity.” These studies typically target specific groups such as “rural residents” and “Black or African Americans,” focusing on “self-management” and “cost-effectiveness analysis.” PubMed Cluster 4 (Yellow): Cardiovascular Disease and the COVID-19 Pandemic. This cluster highlights research on “telemedicine,” large-scale “screening,” and “disease management” for “cardiovascular disease” during the global health crisis, with a specific focus on “U.S. veterans.” PubMed Cluster 5 (Purple): Study Population Characteristics. This cluster describes the diverse populations included in the studies, covering keywords such as “men,” “women,” the “elderly,” and the “young,” as well as geographical locations like “Brazil,” which indicates a broad look at the impact of these health interventions on different groups.
Discussion
This bibliometric analysis of 1368 English-language articles on digital health in hypertension management, spanning from 1992 to 2025, reveals a rapidly expanding and increasingly interdisciplinary research landscape. The annual publication trend demonstrates substantial and sustained growth, particularly from 2011 onward, which can be attributed to technological advances, heightened global awareness of hypertension as a critical health issue, and the increasing prioritization of preventive healthcare strategies. The most cited article, “Design of an mHealth app for the self-management of adolescent type 1 diabetes: a pilot study,” demonstrated that digital tools can enhance self-monitoring behaviors, thus offering the potential for improved health outcomes through tailored adherence mechanisms. 27 Its high citation count underscores the early and ongoing scholarly interest in mobile health applications for chronic disease management.
In terms of country and institutional contributions, the United States stands out as the leading contributor, reflecting its substantial investment in research, advanced infrastructure, and vibrant academic ecosystem—all of which have fostered strong international collaborations. Interestingly, while China ranks second in publication volume—far surpassing Italy and Canada—it ranks only seventh in terms of international collaboration strength. This discrepancy may be due to several factors. One possible reason is the language barrier, as English remains the predominant language of international scientific communication, which may limit Chinese scholars’ participation in global collaborations. Additionally, cultural differences and differences in research funding mechanisms may shape collaborative patterns, with many Chinese researchers prioritizing domestic partnerships or national projects over international ones. These factors highlight the importance of fostering environments and policies that encourage cross-border research, language training, and international academic exchanges to enhance global cooperation.4,5 Notably, Canada and European countries such as the United Kingdom and Italy also contribute significantly, particularly in international multi-center studies.
Institutional analysis further highlights that leading organizations, predominantly from the United States (e.g., Duke University, University of California System, Harvard University), continue to drive innovation and research productivity in this field. The emergence of distinct research clusters, as revealed by keyword co-occurrence network analysis, showcases an ecosystem that nurtures interdisciplinary collaboration—spanning digital interventions, population health, clinical practice, epidemiology, and health equity. Journal analysis indicates that JMIR mHealth and uHealth, Journal of Medical Internet Research, and Telemedicine and e-Health are the most influential publication venues, with high H-indices and citation rates. Their focus on digital health and telemedicine mirrors the field's interdisciplinary character and highlights the central role of these journals in disseminating cutting-edge research at the intersection of technology, healthcare delivery, and chronic disease management.
Hotspots and frontiers
Digital interventions and patient management
The first cluster highlights the centrality of digital interventions, adherence, and patient management in contemporary research. The prominence of keywords such as “adherence,” “care,” “self-management,” and “intervention” aligns with accumulating evidence that digital health tools can substantially improve medication adherence and enable more patient-centered care models.30,31 For example, meta-analyses have consistently shown that technology-facilitated self-management interventions lead to better BP control and improved patient outcomes.31,32 The inclusion of terms such as “primary-care” and “outcomes” further reflects the integration of digital solutions into everyday clinical workflows, echoing findings that collaboration between digital tools and primary care providers is crucial for long-term success.32,33 Notably, the burst of keywords such as “home telehealth” and “interventions” in the last decade demonstrates the acceleration of research on remote care modalities, particularly in response to the increasing need for scalable, accessible hypertension management strategies.34,35 The literature also points to persistent challenges, including sustaining long-term patient engagement and integrating these solutions into complex healthcare systems. 36
Population health and lifestyle factors
Cluster 2's focus on “behavior-change,” “obesity,” “physical-activity,” and “risk” highlights the growing recognition of lifestyle modification as a cornerstone of hypertension management.33,37 Recent studies underscore the effectiveness of digital coaching and remote monitoring in promoting healthy behaviors and reducing cardiovascular risk factors. 35 The emergence of “mhealth” and “medication adherence” as key terms points to the increasing reliance on mobile health applications to deliver personalized interventions at scale.27,30 This is consistent with the literature, which demonstrates that mHealth interventions can reduce barriers to care and improve outcomes across diverse populations.31,38 However, as research expands, there is a need to address disparities in digital literacy and ensure that these interventions are accessible to older adults and underserved communities, a concern echoed in recent systematic reviews. 39
Clinical practice, guidelines, and measurement
The third cluster, featuring terms such as “hypertension,” “guidelines,” “management,” and “self-measurement,” reflects the critical importance of standardized clinical practice and measurement in both research and routine care.32,38 The burst of keywords such as “randomized controlled trial” and “validation” between 2012 and 2018 parallels the surge in large-scale clinical trials assessing the effectiveness of digital interventions. 31 Literature increasingly emphasizes the necessity of integrating guideline-based care with real-time data from home monitoring devices to facilitate timely clinical decisions. 38 Additionally, diabetes and obesity are included in this cluster as they are frequently studied as comorbidities of hypertension. Their inclusion reflects shared risk factors, such as metabolic syndrome, and overlapping management strategies, which are often addressed in hypertension-related clinical research. The sustained attention to “guidelines” in both the co-occurrence and burst analyses underscores the field's ongoing efforts to harmonize digital innovations with established clinical frameworks.35,38 The challenge remains to ensure that new digital modalities are rigorously validated and that evidence is systematically translated into practice.
Disease burden, outcomes, and epidemiology
Cluster 4 draws attention to the epidemiological and health outcomes dimensions of digital health in hypertension, with keywords such as “burden,” “prevalence,” “mortality,” and “global burden.”32,33 The recent burst of keywords such as “burden,” “association,” and “meta-analysis” since 2021 reflects a maturing field that is increasingly focused on understanding the societal and economic impact of hypertension and its management. 32 The literature corroborates this trend, highlighting the growing use of digital health tools not only for individual patient management but also for population-level surveillance and risk stratification.33,37 Additionally, the presence of keywords such as “chronic diseases,” “prevention,” and “guidelines” in this cluster not only signifies a broadening of scope toward chronic disease management but also points to the increasing clinical importance of digital intervention and nonpharmacological therapy, as supported by recent studies. 40 As new evidence emerges, researchers are better equipped to quantify the benefits and limitations of digital health in reducing adverse outcomes and healthcare costs.32,36
Health equity, access, and technology utilization
The final cluster, comprising keywords such as “access,” “disparities,” “telehealth,” “technology,” and “united-states,” signals a critical shift toward addressing health equity and policy issues in digital hypertension management.36,39 The COVID-19 pandemic catalyzed a rapid expansion of telehealth, elevating concerns around equitable access, digital divides, and infrastructural readiness. 36 The persistent burst of terms such as “telehealth” and “united states” in recent years mirrors global discussions about ensuring that technological advancements do not exacerbate existing disparities. 39 The literature calls for targeted strategies to improve access among marginalized populations, as well as robust policy frameworks to support sustainable, inclusive digital health ecosystems.36,39
The comparison of search results from the PubMed and WOSCC databases reveals a high degree of consistency in the research themes of digital health in hypertension. While specific cluster names and keywords may differ, the core research topics overlap. Both databases show that research in this field focuses on using digital technologies for patient management and self-care, especially for chronic conditions like hypertension.41,42 Furthermore, both highlight population health and epidemiology, studying the application and impact of digital interventions across diverse populations, while also emphasizing technology accessibility and health equity.43,44 The main difference is that PubMed's clusters tend to focus more on specific diseases and particular technological applications,45,46 whereas WOS leans toward a classification based on methodology and research themes (e.g., epidemiology, clinical practice). The WOS data also provide a dynamic view of how research focus has evolved over time. In conclusion, both databases collectively paint a clear picture of the field's evolution from foundational technical research toward real-world application, population impact, and health equity.
Recommendation
Going forward, research should focus on overcoming barriers to integration, enhancing interoperability and data privacy, and ensuring digital health solutions are both effective and accessible across diverse patient populations.31,36,39 Going forward, research should focus on overcoming barriers to integration, enhancing interoperability and data privacy, and ensuring that digital health solutions are both effective and accessible across diverse patient populations. Addressing these challenges will be essential for realizing the transformative potential of digital health in hypertension management.36,39
Limitations
The present bibliometric analysis is not devoid of limitations. Firstly, our study relied solely on the WoSCC database, which, while large and multidisciplinary, may not capture all relevant articles in the field. For example, PubMed is a widely used biomedical database that may include additional publications not indexed in WoSCC. The use of a single database may therefore restrict the comprehensiveness of the dataset and introduce selection bias. Future research could benefit from integrating data from multiple sources, such as PubMed or Scopus, to enhance coverage and robustness. Secondly, the focus on English-language articles may exclude important research published in other languages, introducing linguistic bias and potentially providing an incomplete picture of the global research landscape. Furthermore, the study's reliance on bibliometric data alone may overlook other important aspects of research, such as practical applications, patient outcomes, and policy implications. A more holistic approach, integrating both qualitative and quantitative data, could provide a more comprehensive understanding of the field's impact and relevance.
Conclusion
This comprehensive bibliometric analysis demonstrates that research on digital health in hypertension management has expanded rapidly in recent years, with significant contributions from the United States, China, and leading academic institutions. The field is characterized by strong interdisciplinary collaboration, though notable disparities in international cooperation remain. Five major research clusters were identified: digital interventions and patient management, population health and lifestyle factors, clinical practice and guidelines, disease burden and epidemiology, and health equity and technology utilization. Recent trends indicate a growing emphasis on telehealth, real-world implementation, and equitable access to digital health solutions.
Despite these advances, there are persistent gaps, including limited long-term outcome data, challenges in integrating digital strategies into routine care, and disparities in digital health adoption. Future research should focus on fostering international collaboration, improving the accessibility and effectiveness of digital interventions, and generating robust evidence on long-term clinical and system-level impacts. Such efforts will be essential to fully realize the potential of digital health for improving hypertension management globally.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261416710 - Supplemental material for Global research trends and hotspots in digital health in hypertension: A comprehensive bibliometric analysis (1992–2025)
Supplemental material, sj-docx-1-dhj-10.1177_20552076261416710 for Global research trends and hotspots in digital health in hypertension: A comprehensive bibliometric analysis (1992–2025) by Hailong Zhang, Yanan Xing, Qinglong Tang and Jing Su in DIGITAL HEALTH
Footnotes
Contributorship
HZ and YX carried out the studies, participated in collecting data, and drafted the manuscript. QT and JS performed the statistical analysis and participated in its design. HZ and YX participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated or analyzed during this study are included in this published article.
Guarantor
HZ.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.