
Abstract
Background
Tier 2 multi-component lifestyle interventions are integral to the National Health Service weight management pathway. While eHealth delivery may increase accessibility of these interventions many digital programmes lack specificity and repeatability, making it challenging to evaluate which components are most effective.
Objective
This study reports on a tier 2 eHealth weight management intervention, designed using the rehabilitation treatment specification system (RTSS), delivered in an ethnically diverse population.
Methods
The tier 2 eHealth intervention was developed using the RTSS, which includes treatment components containing three elements of treatment theory: a target, a mechanism of action and ingredients. Participants (≥18 years) had body mass index >30 or >27.5 kg/m2 ethnic-specific. Primary outcomes were weight change and the proportion of participants achieving at least 3% and 5% weight loss. Secondary outcomes included physical activity, dietary quality, eating behaviours and quality of life.
Results
Of 579 enrolled participants, outcome data were available for 322. Programme completion rate was 45%. Forty per cent of the programme completers lost ≥3% of weight (9.2 ± 11.3 kg (10%)), and 27% lost ≥5% (−11.8 ± 13 kg (12.4%)). Improvements in secondary outcomes were observed across ethnic and deprivation groups.
Conclusion
Programme completion for this tier 2 eHealth intervention was below the recommended levels but is consistent with the literature. Weight and behavioural improvements were observed across ethnicities and deprivation levels. The RTSS-based intervention provides a replicable framework that enhances intervention fidelity, supports evaluation and informs future programme development. Further research is needed to optimize completion rates to improve outcomes.
Background
Obesity is a global health problem, 1 and despite significant research investigating its mechanisms, contributing factors and management strategies, 2 the prevalence of obesity continues to rise.3,4 In England, 39% of adults are overweight, and an additional 28% live with obesity, with men (67%) disproportionately affected compared with women (61%). 5 Obesity-related co-morbidities include type 2 diabetes, cardiovascular disease, certain cancers 6 and reduced quality of life. 7 The economic consequences of overweight and obesity are significant, with costs estimated to increase from 2.19% to 3.3% of total gross domestic profit in 161 countries. 8 In the UK, 2–8% of the health budget is attributed to obesity-related costs, and wider societal costs are approximately £27 billion. 9
Obesity management in the UK is guided by the National Institute of Health and Care Excellence (NICE), 10 and includes a four-tier system to support people living with overweight and obesity. 11 Provision encompasses universal support in primary care (tier 1) and specialist bariatric services (tier 4). Tier 2 adult services are typically 12-week multi-component commissioned programmes (diet, physical activity and behaviour change components) and are designed to be offered and sufficiently tailored for all of including disadvantaged and underserved communities. 11
There is evidence that clinically significant weight loss of 5–10% improves obesity-related co-morbidities, including liver, peripheral insulin sensitivity and cardiovascular risk.12–14 However, the proportion of participants who achieve ≥5% weight loss through tier 2 weight management interventions varies extensively, ranging from 10% to 50%. 15 Tier 2 designed services have been shown to yield small-to-moderate short-term improvements in weight loss and weight maintenance, but long-term results are inconsistent. 16 This variability could be attributed to heterogeneous study designs, a challenge common in other areas of health and rehabilitation.17,18 Furthermore, poorly specified intervention components based on treatment theory may limit the ability to attribute outcomes to specific aspects of the intervention. For example, despite recommending valid improvements in their mixed-methods evaluation of tiered service delivery, Ells et al. cannot recommend how improved service ingredients actively change treatment targets because they are not specified. 15
The rehabilitation treatment specification system (RTSS) offers a framework to specify rehabilitation treatments using professionally agnostic and common language. The RTSS focuses on a treatment component, which includes three elements of treatment theory: a target (directional, measurable aspect of function to be changed), a mechanism of action (hypothesized or known causal link between targets and ingredients) and ingredient(s) (what the clinicians do). 17 Through a priori specification, the clinician or researcher is challenged to articulate a clear treatment theory, enabling reasoned, replicable, modifiable, teachable and testable treatment components.
The COVID-19 pandemic created a unique opportunity to develop a physiotherapy-led tier 2 eHealth service intervention in an ethnically diverse population in southeast London. Despite physiotherapists’ expertise in long-term condition management, exercise prescription in complex co-morbid conditions and behaviour change application, their potential to support weight management services remains unreported and under-utilized. By applying the RTSS from the outset, the intervention was pre-specified to enhance transparency, reproducibility and theoretical clarity for the weight management community while also providing a professionally novel treatment theory for physiotherapists. Herein, we describe a real-world tier 2 eHealth programme specified through the RTSS and report an interim evaluation of the service.
Methods
Study design
This project was registered and approved as a service evaluation at Guy's and St Thomas’ National Health Service (NHS) Foundation Trust (reference number 15239), in accordance with the Trust's Clinical Audit and Service Evaluation Policy. As a service evaluation, the project involved no change to usual care, no additional procedures and no collection of identifiable data. In line with Trust policy and national guidance, written informed consent was not required, nor was Research Ethics Committee review necessary. Patients are informed via Trust patient information materials that their anonymized data may be used for audit and service evaluation purposes. All data used in this evaluation were anonymized. STROBE cross-sectional reporting guidelines were used in the reporting of this study. 19
Population
The participants included adults (≥18 years) enrolled in the eHealth programme from September 2020 to July 2022 and had a body mass index (BMI) > 30 kg/m2 for White ethnicities or >27.5 kg/m2 for Black, South and East Asian ethnicities. Internet access and access to video- and microphone-enabled devices such as laptops, iPads or smartphone were needed. The participants were referred to the programme by their general practitioner (GP) or other healthcare professionals.
Intervention
The tier 2 eHealth programme consisted of 12 weekly 60-min sessions delivered by physiotherapists, physiotherapy technical instructors and healthy living practitioners trained in nutrition. Sessions included a 30-min exercise class and 30-min of lifestyle and nutrition education utilizing behaviour change techniques. Delivery was live via a remote video platform (Blue Jeans™), and access to an app was provided for group members to contact each other and the facilitators and to self-track food intake and physical activity. The exercise component varied weekly, with a focus on reaching a moderate to vigorous level of intensity via circuits, high-intensity interval training, movement to music and dynamic stretching (Table 1). This provided an opportunity to practice exercise with real-time feedback and adjustments from facilitators. Lifestyle education was delivered via pre-recorded videos and podcasts, PowerPoint presentations and problem-solving tasks in small groups in breakout rooms.
Specification of the tier 2 eHealth weight management programme based on the rehabilitation treatment specification system.

The overall goal is maintenance of weight loss.
All exercise sessions were proceeded and followed by an appropriate warm up and cool down, respectively.
Group – O: organ; S: skills and habits; R: representations; Type – NV: direct target for non-volitional or passive; RPE: rate of perceived exertion; DV: direct target for volitional; V: separate volition target as needed; HIIT: high intensity interval training; UL: upper limb; LL: lower limb.
The theoretical framework of the intervention was underpinned by capability, opportunity, motivation, behaviour model 20 with specific treatment components targeting aspects of participants’ capability, opportunity and motivation. Behaviour change was facilitated through modifying beliefs via open-ended discourse, augmenting self-efficacy through positive feedback, informing knowledge with permission, avoiding persuasion, using reflective listening statements and summarizing group or individual points to demonstrate active listening. Within our intervention, each clinician would adapt the delivery of each behaviour change therapy dependent on factors related to that specific group, such as the group dynamics, self-efficacy, previous experiences of weight management interventions and stage of change. This allowed for flexibility and patient centred treatment yet underpinned by theory and evidence-based interventions. As mentioned, the intervention content was pre-specified via the RTSS17,18 (Table 1). While all the treatment groups were targeted, the predominant treatment group specified was representations. Representation-level treatment components are designed to modify thoughts, behaviours, motivation and affect through ingredients that alter cognitive information processes. 17
Data collection
Initial assessment (pre-programme) and exit data collection (post-programme) were completed via telephone consultation with a member of the service provider team via online surveys and questionnaires. The data collected included age at baseline; patient and GP post-code and nominal representations of sex, ethnicity, marital status, living arrangements and source of referral. Patient post-code was used to derive an area-level index of multiple deprivation (IMD) score, which was ordinally reported as deciles. BMIs were calculated from self-reported weight and height. Body weights were self-reported at weeks 1, 4, 8, 10, 11 and 12. Patients were advised to record their weight at the same time of day and in similar, minimal clothing to provide an accurate comparison. However, due to the remote nature and real-world aspect of this there was no standardization or enforcement of this advice.
Programme completion
Session attendance records informed programme completion, specified as attending 75% of the programme, 11 which we operationalized as participants attending and having weight recorded at sessions 10, 11 or 12. If participants did not attend two sessions during the programme prior to session 10, they were discharged. Programme non-completers were defined as those who did not attend or did not complete.
Outcomes
The primary outcomes were changes in weight and the proportions of participants who achieved 3% and 5% weight loss. The secondary outcomes included self-reported physical activity, health-related quality of life, diet quality and emotional eating.
Physical activity
Physical activity was assessed using the validated the 9-item International Physical Activity Questionnaire-Short Form (IPAQ-SF), 21 which categorizes activity over the previous week in terms of sitting, walking and moderate and vigorous intensity. Physical activity examples were provided to support the completion of the questionnaire and the scoring criteria. A total score in metabolic equivalents (Mets) per week was calculated as per the published IPAQ protocol. 21 Aerobic capacity and endurance were assessed via Timed Walk application (app). The app measures the distance walked in 6 min and provides an indication of exercise capacity and general health status 22 and is validated for clinical use. 23 Participants were instructed to complete the 6-min walk test using the Timed Walk app in the setting most preferable to them (i.e. at home or outdoors). For consistency, they were asked to use the same setting for both pre- and post-intervention assessments. These instructions were additional to the standardized instructions on the app.
Diet quality
Dietary intake was assessed via the UK Diabetes and Diet Food Frequency Questionnaire (FFQ), 24 which is validated for use in people with or at high risk of type 2 diabetes. This 22-item questionnaire, which has good test–retest reliability, assesses the frequency of consumption of certain foods. Higher scores are indicative of lower dietary quality.
Emotional eating behaviours
The participants completed emotional eating questionnaires, which are part of the validated three-factor eating questionnaire (TFEQ). 25 It consists of three statements: (1) When I feel anxious, I find myself eating; (2) When I feel blue, I often overeat and (3) When I feel lonely, I console myself by eating. There are four options for answers: definitely true (4 points), mostly true (3 points), mostly false (2 points) and definitely false (1 point). A composite score was calculated (the maximum score was 12, and the minimum score was 3), with higher values indicating greater emotional eating.
Quality of life
Health-related quality of life was measured via the validated EQ-5D-5L questionnaire, 26 which assesses five domains: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Overall health is self-rated via a visual analogue scale ranging from 0 (the worst health imaginable) to 100 (the best health imaginable). Higher total composite scores indicate greater health-related quality of life.
Statistical analysis
Frequencies and descriptive statistics were used to characterize the cohort. Data normality was assessed using the Shapiro–Wilk test (p < 0.05 indicated non-normality) and visual inspection of Q–Q plots. Independent t tests or chi-square tests were used to assess differences in baseline characteristics between the whole cohort and the completer cohort. Pre- and post-intervention comparisons were made for absolute and relative weight changes and BMI. Pre–post comparisons are also reported for the secondary outcomes via paired t tests Mann–Whitney U test and chi-square tests, as appropriate. Pearson's correlation coefficient was used to determine the strength of associations between continuous variables, and Monte Carlo simulations were used to correct where chi-square tests (χ2) were otherwise invalid. Data for completers, as defined above, are reported as the means ± standard deviations (SDs) or numbers (percentages; n (%)). A probability of ≤5% was defined as statistically significant.
Missing data for weight at programme end was addressed using the last observation carried forward (LOCF) imputation method. For participants that were missing weight, the most recent available weight from an earlier session, or the baseline weight, was carried forward and used as the end-point data.
A sub-analysis was performed to examine differences in outcomes between ethnic groups and between groups of various socio-economic deprivation levels to identify potential variations within these sub-populations. These sub-analyses are reported descriptively due to reduced sample sizes in the sub-groups.
Results
Participant characteristics
We enrolled a cohort of 579 participants who were predominantly female (81%). The majority identified as Black (50% Black African (36%) and Black Caribbean (14%)), with 30% identified as White. Most participants were single (56%) or married (32%), and 30% reported living with children. The GPs referred 92% of the participants to the service. Deprivation levels were high, with a mean IMD decile of 3 ± 1.5 (Table 2). At baseline, 17% reported type 2 diabetes, 16% reported pre-diabetes and the cohort was predominantly hypertensive (Table 2). The mean baseline weight and BMI were 100.6 ± 16.5 kg and 36.3 ± 5.1 kg/m2, respectively and did not differ between completers and non-completers. Participant characteristics by ethnicity are reported in Supplemental Table 1.
Participant characteristics of the total enrolled cohort and programme completers for the tier 2 eHealth weight management programme.
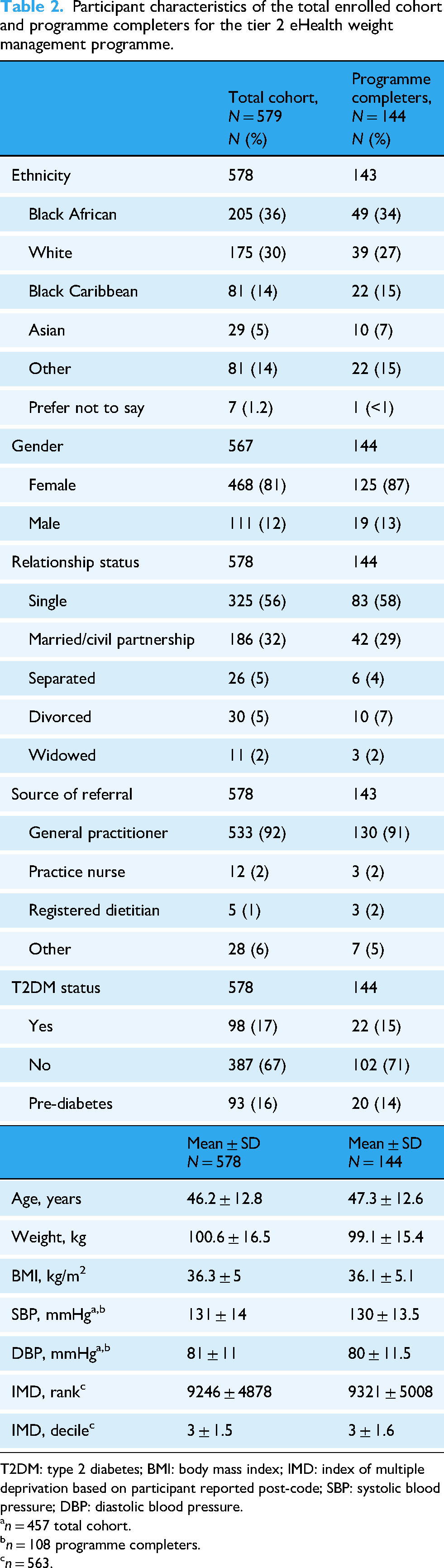
T2DM: type 2 diabetes; BMI: body mass index; IMD: index of multiple deprivation based on participant reported post-code; SBP: systolic blood pressure; DBP: diastolic blood pressure.
n = 457 total cohort.
n = 108 programme completers.
n = 563.
Programme outcomes
At the time of analysis, 579 participants were enrolled in the programme, with programme data available for 322 participants. Among these, 45% (n = 144) completed the programme, while 25% (n = 82) did not attend one session and an additional 30% (n = 96) did not complete the programme (Figure 1).
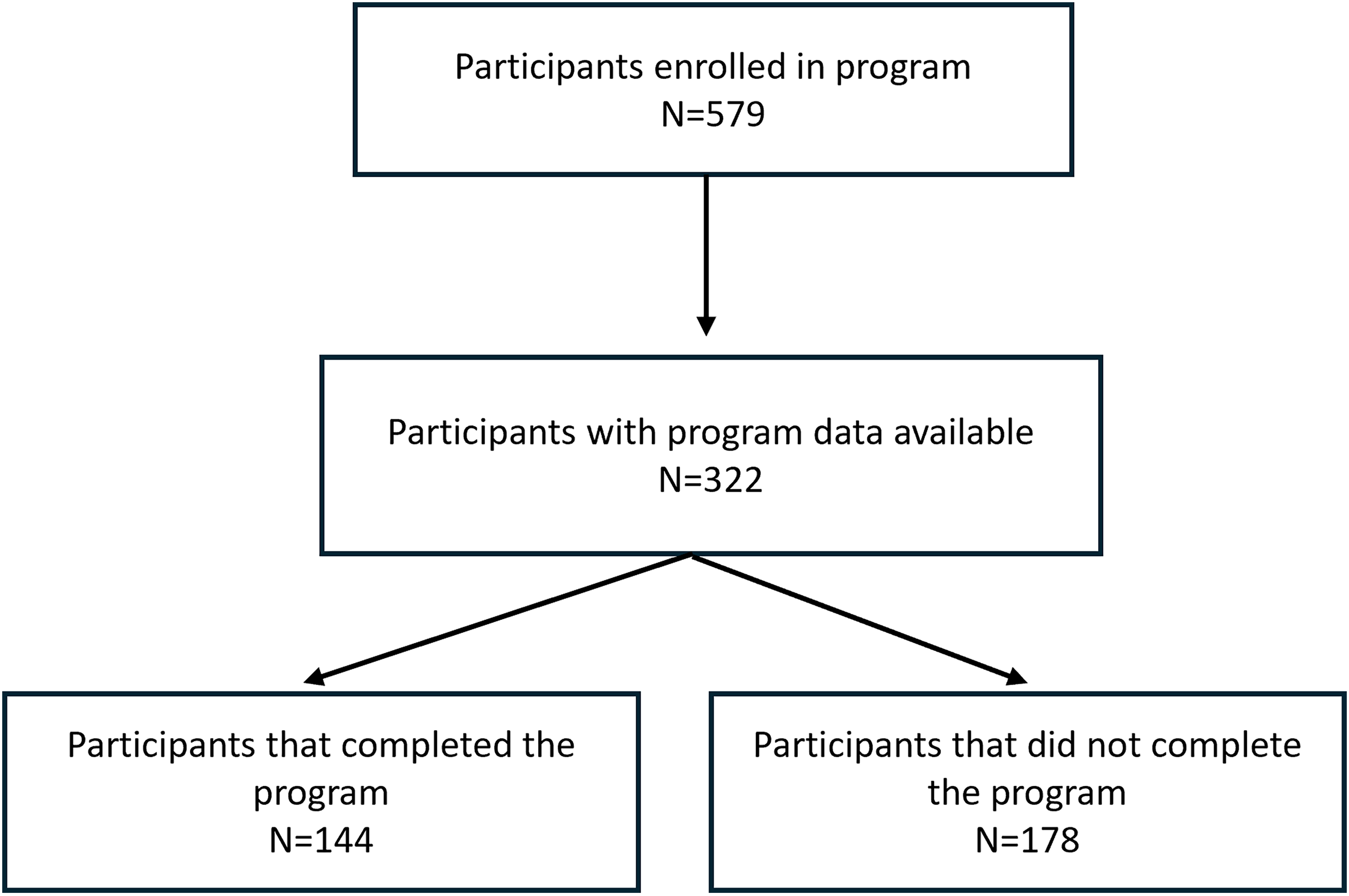
Participant flow diagram. Of those that completed the programme (n = 144), paired data (baselined and programme end) was available for 108 participants.
Among the programme completers (n = 144), data were available for 81% of the completer cohort, and paired data (baseline and programme end) were available for 75% of the completer cohort. The sex, ethnicity, age and clinical status of the programme completers mirrored those of the full cohort. The sex (p = 0.13) and ethnicity (p = 0.828) of the completers and non-completers did not differ, and the weights at baseline were similar (completers 99.1 ± 5.4 kg vs. did not attend 100.4 ± 15.2 kg vs. did not complete 103.2 ± 15.4 kg, p = 0.159). Programme completion did not differ by age (completers 47.4 ± 12.6 years vs. did not attend 45.4 ± 12.1 years vs. did not complete 43.1 ± 13.4 years, p = 0.062), nor was there a correlation between age and weight change (r = −0.168, p = 0.082). Programme completion rates did not vary by ethnicity (χ2 = 0.244, df(2), p = 0.885) or deprivation status (χ2 = 4.248, df(2), p = 0.120).
Weight
Among programme completers, the weight change from baseline to programme end was −3.6 ± 8.7 kg (95% confidence interval (CI) −5.27, −1.95), t(107) = –4.31, p < 0.001, Cohen's d = –0.42 (95% CI −0.61, −0.22) which was equivalent to a −4% (±11% weight change) (Table 3). Forty per cent of completers (n = 43/108) lost ≥3% weight, and among those who lost ≥3% of their average weight, the average weight loss was 9.15 ± 11.3 kg (9.6 ± 15%). Twenty-seven per cent of participants (n = 28/108) lost ≥5%, equating to 11.8 ± 13 kg (12.4 ± 17.4%). BMI was also significantly reduced by the end of the programme (–1.2 ± 3.8 kg/m2, (95% CI 0.5, 1.96), t(107) = 3.316, p = 0.001, Cohen's d = 0.319) (Table 3).
Impact of the tier 2 eHealth weight management programme on body weight and body mass index from baseline to programme end.

BMI: body mass index; CI: confidence interval.
Data is presented for programme completers and split by ethnic group. Paired data reported for programme completers (n = 108). Data as means ± SD. Black includes Black African and Black Caribbean; Other ethnic group includes Asian, other and prefer not to say.
Statistical significance considered at p > 0.05. Paired t-test (two-sided).
There was a significant difference in weight change by completer status at programme end using LOCF, completer 95.8 (17.1) kg versus non-completer 102 (15.4) kg, Z = –3.468, p < 0.001. Significant weight reduction from baseline to programme end was also observed when participants were grouped by ethnicity (Black: −2.49 ± 5.17 kg, (95% CI 0.96, 4.03), t(45) = 3.278, p = 0.02, Cohen's d = 0.483; White: −3.57 ± 6.67 kg (95% CI 1.28, 5.86), t(34) = 3.166, p = 0.03, Cohen's d = 0.535); Other: −2.68 ± 4.08 kg, (95% CI 1, 4.4), t(25) = 3.294, p = 0.03, Cohen's d = 0.359) (Table 3) and deprivation (high: −3.91 ± 10.3 kg, (95% CI 1.40, 6.41), t(67) = 3.119, p = 0.03, Cohen's d = 0.374); moderate: −4.07 ± 5.21 kg, (95% CI 2.06, 5.8), t(31) = 4.288, p ≤ 0.001, Cohen's d = 0.758), except for the low deprivation category (−1.24 ± 2.60 kg, (95% CI −0.93, 3.43), t(7) = 1.351, p = 0.219, Cohen's d = 0.478). The percentage weight changes by ethnicity were −2.5% (Black), −3.3% (White) and −2.7% (Other), and those by deprivation category were −3% (high), −4.1% (moderate) and low (–1.2%).
Weight change did not differ between ethnic groups (Black, White, Other; H(2) = 0.134, p = 0.935). Similarly, weight change did not differ between the IMD categories (high, moderate, low H(2) = 1.869, p = 0.393).
Physical activity
There was a significant difference in physical activity, based on IPAQ categories (low, moderate, high), from baseline to programme end (χ2(4) = 13.9; p = 0.008), as confirmed by Monte Carlo simulations (p = 0.006; Table 4). When participants were grouped by ethnicity (Black, White, Other), there was a statistically significant difference in physical activity based on IPAQ categories (low, moderate, high) from baseline to the end of the programme among participants of Other ethnicities (χ2(4) = 13.4; p = 0.009), as confirmed by Monte Carlo simulations (p = 0.005). No difference was observed for the Black ethnicity group (χ2(4) = 8.09; p = 0.088) or the Monte Carlo method (p = 0.078) or for the White ethnicity group (χ2(4) = 8.23; p = 0.082) or the Monte Carlo method (p = 0.070) (Table 4). Physical activity (IPAQ categories) by deprivation status tended to improve only in the low deprivation group (χ2(4) = 10.8; p = 0.029), but this finding was not confirmed by Monte Carlo simulations (p = 0.054). No additional statistically significant differences were observed in the moderate or high deprivation categories.
Impact of tier 2 eHealth weight management programme on IPAQ physical activity categories based for programme completers and by ethnicity.

IPAQ: International Physical Activity Questionnaire; CI: confidence interval.
Chi-square and Monte Carlo test (based on 10,000 samples, 95% CI). Starting seeds all completers (2,000,000), White ethnicity (334,431,365), Black ethnicity (221,623,949) and other ethnicity (1,535,910,591).
Monte Carlo simulation data.
Statistical significance considered at p < 0.05.
Physical activity (Mets) also significantly changed from baseline to programme end, with increases observed for total activity (+322 ± 1051 Mets, p < 0.001) and walking (+113 ± 578 Mets, p = 0.021), and there was a small non-significant trend towards increased moderate activity (+80 ± 478 Mets, p = 0.091). Vigorous activity (p = 0.25) was unchanged (Table 5). Aerobic capacity and endurance assessed via the timed walk test did not change following completion of the programme (477 ± 102 vs. 417 ± 198 (p = 0.519) baseline vs. programme end, respectively).
Impact of the tier 2 eHealth weight management programme on physical activity assessed by International Physical Activity Questionnaire (IPAQ) for programme completers and split by ethnicity.

CI: confidence interval.
Wilcoxon signed rank test. Black includes Black African and Black Caribbean; Other ethnic group includes Asian, other and prefer not to say.
n = 113.
n = 49.
n = 26.
Statistical significance considered at p < 0.05.
In the Black ethnicity group, moderate activity (+160 ± 360 Mets, p = 0.06) and total activity (+321 ± 810 Mets, p = 0.003) improved and in the Other ethnic group, walking (+337 ± 681 Mets, p = 0.048) and total activity (+321 ± 877 Mets, p = 0.006) improved. No differences were observed in the White group. Aerobic capacity and endurance, assessed via the timed walk test following completion of the programme, were not significantly different among any of the ethnic groups. Walking (+185 ± 501 Mets, p = 0.003) and total activity (+269 ± 1064 Mets, p = 0.037) improved in the high deprivation group, and improvements in total activity were also observed in the moderately deprived group (+494 ± 706 Mets, p = 0.001).
Diet quality and emotional eating behaviours
Dietary quality improved with the tier 2 intervention, with a total FFQ score reduction of −8 ± 9.6 (p < 0.001) from baseline (34.3 ± 11.2) to the end of the programme (26.3 ± 10). Similar improvements were observed in the White group (Δ−7.9 ± 10.5 (36.6 ± 12.3 to 28.6 ± 9.2, p = 0.001)), Black group (Δ−8.4 ± 9.8 (34.1 ± 9.8 to 25.6 ± 7.6, p < 0.001)) and Other ethnic groups (Δ−7.1 ± 8.5 (32.5 ± 12.5 to 25.4 ± 13.9, p < 0.001)).
Emotional eating behaviours, assessed via the TFEQ, improved from baseline to the end of the programme (7.4 ± 3.1 vs. 6.5 ± 3, p < 0.001). Emotional eating behaviours improved in the Black (7.3 ± 3.1 to 6.6 ± 3.0, p = 0.01) and Other (7.1 ± 3.5 to 5.5 ± 3.1, p = 0.004) ethnic groups, but no improvements were observed in the White group. Dietary quality by deprivation status also demonstrated marked improvement in the high −7.9 ± 9.7 (34.9 ± 11.3 to 26.9 ± 10.4, p = 0.002) and moderately deprived groups (8.1 ± 9.1 (34.7 ± 9.9 to 26.5 ± 8.5, p = 0.001)). A similar trend was observed for eating behaviours in these groups (high deprivation −7.4 ± 3.1 to 6.5 ± 3.0, p = 0.002) and moderate deprivation −7.3 ± 3.1 to 6.4 ± 2.9, p = 0.03).
Health-related quality of life
Health-related quality of life significantly improved among programme completers (baseline 58.1 ± 22.4 vs. programme end 62.1 ± 20.6, p = 0.02). However, across the different ethnic groups, a significant improvement was observed only in the Other ethnic group (52.1 ± 22.5 to 59.3 ± 19.7, p = 0.017), with no changes observed for Black or White group participants. By deprivation category, quality of life improved in the high-deprived (57.2 ± 23.5 to 61.4 ± 21.2, p = 0.044) and moderately deprived groups (60.4 ± 17.8 to 67.0 ± 16.0, p = 0.016).
Discussion
This service evaluation reports on a tier 2 weight management programme serving a multi-ethnic cohort living in southeast London. The programme was physiotherapy-led and professionally novel. Moreover, it was delivered by professional and para-professional physiotherapists in a novel way because the programme was specified a priori using the RTSS. Programme completion was 45%, average weight loss among completers was 4%, and improvements in health-related behaviours were observed in the total cohort and across different ethnic and deprivation groups. Participant characteristics, including weight at baseline, did not differ between programme completers and non-completers.
The absolute weight loss among programme completers was −3.4 ± 8.7 kg, which is consistent with national prospective data from NHS digital weight programmes, −3.9 kg (95% CI −3.99 to −3.84). 27 Among those who completed the programme, 40% lost ≥3% of their baseline weight. Even modest weight loss (3–5%) is associated with significant metabolic improvements, including improved insulin sensitivity and a reduced risk of type 2 diabetes complications.12,14,28 This amount of weight reduction is significant given that 15% of our completer cohort had type 2 diabetes, leading to a potentially meaningful impact on their metabolic health and glycaemic control. In our service evaluation, participants classified as achieving at least 3% and 5% weight loss lost on average, 10% to 12% of their body weight (–9.2 to −11.8 kg, respectively), indicating that some participants experienced considerable health benefits. The proportions of completers who achieved ≥3% and ≥5% weight loss was 40% and 27%, respectively. While these data are similar to those reported in an evaluation of a tier 2 programme in Cornwall, England, where 48.8% and 24.6% achieved ≥3% and ≥5% weight loss, respectively, 29 they are greater than those reported in another English study (North Yorkshire), where only 30% of participants achieved 3% weight loss. 15 However, the North Yorkshire evaluation included pooled data from multiple services within Northeast England, and BMI was not reported at baseline. The eligibility criteria for the services included a BMI between 25 and 35 kg/m2, which is lower than our enrolled participants’ mean BMI (36.3 ± 5 kg/m2). Interestingly, the Cornish cohort 29 had a similar BMI to our population (36.7 ± 7.1 kg/m2 for completers and 38.8 ± 8.1 kg/m2 for non-completers), with similar absolute weight loss outcomes as our cohort (−3.15 kg). Variations in baseline BMI may explain some of the differences in weight loss outcomes. Evidence suggests that individuals with higher initial BMI tend to lose more weight in absolute terms, even if the percentage loss remains consistent across BMI categories. 30 Not unexpectedly, we observed greater weight loss in participants that completed the programme aligning with existing research. 27 Positive associations between greater engagement and weight loss are documented elsewhere.31,32 Higher initial weight, 33 participant characteristics 34 and early weight loss 35 are associated with greater reductions in weight and treatment time 34 is independently associated with weight loss. 31 In the current study, there was no significant difference in baseline characteristics between completers and non-completers or initial weight, so these factors do not explain the difference in weight change by completion status. Regarding engagement, recorded weight can be considered a proxy measure of programme engagement as it was reported by session attended and it demonstrates better engagement in the completer compared to the non-completer group, suggesting that it is the engagement that, at least in part, explains the differences in weight loss outcomes. Detailed investigation of participant engagement with the services is not available for the study however, future research should investigate how frequently participants engage and interventions should be tailored to maximize early and sustained engagement. Overall, tier 2 weight management services achieve clinically meaningful outcomes, often meeting or exceeding the benchmark that at least 30% of participants should achieve ≥5% weight loss. 10 However, persistently high attrition rates undermine overall programme effectiveness. Therefore, efforts to improve completion rates are important not only for service delivery but also for optimizing participant health outcomes and should be prioritized. 36
Our programme achieved a completion rate of 45%, with no differences observed between the ages of the completers and non-completers. This contrasts with the findings of Ells et al., who reported that younger participants were less likely to complete their 12-week multi-component tier 2 programme. However, completion rates in their service varied depending on geographical district, ranging from 8.4% to 73.4%. 15 The marked differences in participant characteristics between the North Yorkshire cohort and our southeast London cohort, particularly in terms of deprivation status, ethnic diversity and age, may, in part, explain the divergence in completion rates. However, more comparable completion rates to our findings include a recent national service evaluation of 63,937 participants in NHS digital weight management 12-week programmes between April 2021 and March 2022, which reported a completion rate of 45%. 27 Similarly, 38% of the participants completed the tier 2 programme in Cornwall, 29 despite differences in referral source (82% of participants self-referred) and ethnicity (92% were White British). Conversely, data from an international-site randomized controlled trial (RCT) 37 comparing a 12-month commercial weight management programme to usual care revealed significant differences in attrition rates between nations in which the number of participants not completing the programme was highest in the UK (64%) and Australia (41%) and Germany (25%). Comparing the UK cohort with our own cohort, we observed a lower number of non-completers (55%). However, differences in programme duration and the lack of definition of completion in RCTs limit comparisons. There is also a paucity of data on programme completion rates for tier 2 interventions among specific ethnic groups. 38 In our multi-ethnic cohort, programme completion did not vary by ethnicity or deprivation level, indicating that the programme is contextually relevant to the population and warrants further evaluation to understand the factors contributing to adherence. Efforts to understand determinants of and strategies to support completion among tier 2 participants are needed, particularly as programme completion rates are lower than the minimum 60% completion rate recommended by NICE. 10
Tier 2 weight management services are multi-component interventions that include physical activity, diet and active behaviour change components. In addition to the reductions in weight, we also observed significant improvements in physical activity and dietary quality and improved health-related quality of life. Similar improvements in diet and physical activity have been reported qualitatively by Ells and colleagues. 15 However, outcome reporting on the behavioural components of tier 2 services is lacking; for example, the NHS digital weight management programme had no outcomes related to behaviours, only weight and engagement. 27 The absence of data limits our understanding of the wider impact of these programmes. The suitability of weight as a primary outcome for behavioural weight management programmes should be carefully considered, and the core outcomes identified for weight management programmes are a welcome addition to support standardized reporting. 36 Updated obesity management guidelines from the NICE 10 recommend the waist-to-height ratio as a more accurate measure of central adiposity in individuals with a BMI <35 kg/m2, which underscores the prediction of health risks associated with obesity. Further research is needed to understand how success is defined from the perspective of participants and commissioners, as there may be discrepancies between these perspectives. Agreement of key performance indicator criteria is essential to appropriately evaluate tier 2 service effectiveness. There is increasing evidence that peer and facilitator support is fundamental to successful weight loss efforts, but an understanding of which behaviours should be considered primary outcomes is still lacking. With the emergence of weight inclusive care39,40 this approach will become increasingly relevant.
One of the persistent problems in weight loss interventions, and most other rehabilitation treatments, is their lack of theoretical or intervention specificity. Usually, what an intervention is and how it works is inadequately described. The Yorkshire 15 and Cornwall 29 studies compared our work with those that do not sufficiently specify their interventions, limiting their replicability and ability to critically evaluate which elements of the intervention are (or are not) effective. In contrast, our study is the first tier 2 weight management programme to be pre-specified by physiotherapists via the RTSS. In doing so, a transparent, structured and theory-driven approach to specifying the treatment components of the intervention is open and available for criticism, adoption, replication or modification, which is among the reasons the RTSS was designed.17,41 Moreover, it enhances facilitator fidelity during intervention delivery by supporting facilitators’ understanding of treatment intentions and the ingredients to deploy. Discerning the effectiveness of behaviour change strategies aimed at improving programme retention is urgently needed because while programme completers achieve significant outcomes, high dropout rates remain a concern. The RTSS framework can support this important ambition by providing a framework to analyse non-adherence more systematically. A better understanding of the underlying mechanisms of adherence can then be identified. Together with this aspiration is the emerging role of the physiotherapist in weight management, as demonstrated here, who can provide valuable contributions to this field by designing robust theoretically informed behaviour change interventions and increasing the quality and reasoning of treatment.
Despite the positive effects on weight and behavioural outcomes observed in this real-world setting, interim service evaluation, it is not without limitations. First, anthropometric data are self-reported, which deviates from NICE recommendations 10 and reduces the accuracy of measurements. Second, the internal validity of the programme is limited because of the absence of a comparison group or control intervention. Sample sizes used in the sub-group analyses were small and under-powered. The exploratory nature of the sub-group analyses was hypothesis generating rather than providing definitive conclusions. No formal adjustment for multiple testing was applied so the p-values, which are reported in full, need cautious interpretation and should be considered with the reported estimated effects and CIs rather than on statistical significance alone. Lastly, some of the assessments used are limited by the self-report nature or may lack sensitivity. For example, we observed no change in aerobic capacity across ethnic groups using the Timed Walk app despite changes in physical activity. While instructions on how to complete the assessment were provided to participants, completion of the test may have been compromised. Salvi and colleagues purport the benefits of the app outside of the clinical setting but they also acknowledge it may work best in a younger population (<50 years) and recommend that the app is subject to an RCT to compare usual 6-min walk test to the app-based version. 23 Additionally, while the app is based on the validated 6-min walk test, delivery of this assessment via the app may not be sufficiently sensitive and open to recording error. Despite these limitations, evaluating the intervention in the real world contributes to its external validity. However, caution is needed when these findings are generalized to wider populations because of the limited previously explained methodology.
A notable strength of the current programme includes the digital service delivery model, which has the potential to increase reach and access. 42 However, concerns regarding the digital divide should be acknowledged, as it may widen health inequalities among those that cannot access eHealth services.
In a recently published ethical framework for eHealth interventions core components for successful interventions including behavioural theory, evaluation, feedback in addition to goal setting, personalization, motivation and recognition of digital literacy are recognized 43 ; and our intervention aligns with this framework. Additionally, Richardson et al. highlight the digital determinants of health approach to eHealth interventions and specify the importance of equitable access. 44 Given that there are notable inequalities in overweight and obesity, future services should carefully consider digital intervention is not disproportionally benefiting already advantaged groups. While we report no differences in outcomes by deprivation future evaluations should consider broader definitions of disadvantage and digital deprivation 45 should also be investigated to ensure eHealth interventions are not widening inequalities. Lastly, long-term outcomes of digital interventions for weight management are lacking 46 and sustainability of impact will be an important metric of intervention design. At the time of this analysis, longer-term data was not available, but data collection is ongoing and will be reported as part of a larger evaluation.
Conclusion
Future research should focus on enhancing strategies regarding service engagement and programme completion to increase the number of participants who achieve significant weight loss. Clinical services should continue to evaluate tier 2 eHealth interventions and report long-term outcomes, which are currently lacking. It is also recommended that qualitative investigations explore participants’ experiences of services to ensure that the programmes are aligned with the needs of local communities. Finally, the adoption of standardized reporting for core outcomes, both weight-related and behavioural, across short- and long-term follow-ups is crucial for facilitating comparisons and improving service development.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251411211 - Supplemental material for Effectiveness of a specified physiotherapy-led tier 2 eHealth weight management programme in a multi-ethnic cohort: A cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251411211 for Effectiveness of a specified physiotherapy-led tier 2 eHealth weight management programme in a multi-ethnic cohort: A cross-sectional study by Jade Sampford, Jamie Gibson, Gareth D. Jones, Richard Myers-Ingram, Emiliano Pena-Altamira, Alastair Duncan and Majella O’Keeffe in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251411211 - Supplemental material for Effectiveness of a specified physiotherapy-led tier 2 eHealth weight management programme in a multi-ethnic cohort: A cross-sectional study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251411211 for Effectiveness of a specified physiotherapy-led tier 2 eHealth weight management programme in a multi-ethnic cohort: A cross-sectional study by Jade Sampford, Jamie Gibson, Gareth D. Jones, Richard Myers-Ingram, Emiliano Pena-Altamira, Alastair Duncan and Majella O’Keeffe in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251411211 - Supplemental material for Effectiveness of a specified physiotherapy-led tier 2 eHealth weight management programme in a multi-ethnic cohort: A cross-sectional study
Supplemental material, sj-docx-3-dhj-10.1177_20552076251411211 for Effectiveness of a specified physiotherapy-led tier 2 eHealth weight management programme in a multi-ethnic cohort: A cross-sectional study by Jade Sampford, Jamie Gibson, Gareth D. Jones, Richard Myers-Ingram, Emiliano Pena-Altamira, Alastair Duncan and Majella O’Keeffe in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
We greatly acknowledge the wider Healthy Living Team for their continued support in delivering wonderful care to our service users. We also appreciate and acknowledge the clinical leads and heads of service across Physiotherapy and Nutrition & Dietetics for their unwavering commitment to innovation and service development. Their encouragement and advanced leadership provide an environment for this work to flourish.
ORCID iDs
Ethical considerations
This cross-sectional service evaluation was ethically approved by the Quality Improvement and Patient Safety (QIPS) oversight committee (reference number 15239) at Guy’s and St Thomas’ NHS Foundation Trust, London. Consent to participate was not required by the QIPS approval given that the data was collected as part of a service evaluation for an approval clinical service.
Author contributions
JS, RM-I, GDJ and JG: conceptualization, writing – original draft preparation, editing, and submission. EP-A: data analysis, writing and draft review. AD: review of the drafts. MO’K: writing – original draft preparation, data analysis, interpretation and submission. All the authors read and approved the final manuscript. Generative AI and AI-assisted technologies were not used in the writing process.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: JG and RM-I are supported by National Institute for Health and Care Research (NIHR) Pre-doctoral Clinical & Practitioner Academic Fellowship awards. GDJ is supported by an NIHR Senior Clinical & Practitioner Researcher Award. This service evaluation was conducted and funded as part of routine clinical responsibilities within Guys and St Thomas’ NHS Foundation Trust. There was no external grant allocated for this work, the evaluation was supported through employment as clinicians within the Trust (JS, JG, GDJ, RM-I, AD). As such, there is no grant or funding number to provide. The service evaluation was independently led by the corresponding author, and the funder had no role in the design of the evaluation, analysis, interpretation of data or the writing of the manuscript. This is an open access article under the CC BY NC 4.0 license.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The dataset generated and analysed during the current study are not publicly available due to fact that the data was collected as part of a clinical service. Reasonable requests for the data can be made via the corresponding author but the release of the data will be subject to approval by the clinical service leads and the Quality Improvement and Patient Safety oversight committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.