
Abstract
Background
Healthcare institutions face evolving management needs, with outpatient data analysis being increasingly critical. While business intelligence (BI) applications in healthcare have grown substantially, 1, 2 existing research on appointment systems predominantly focuses on patient choice modeling and queue optimization, with limited attention to the online appointment decision-making process itself. This study addresses this gap by developing a specialized BI system for analyzing detailed online appointment behaviors.
Methods
We designed an Online Appointment Business Intelligence (OABI) system employing Google Analytics for tracking user interactions with minimal intrusiveness. The system was implemented over an 11-month period at The First Affiliated Hospital of Zhengzhou University. OABI features a layered architecture comprising Operational Data Store (ODS), Data Warehouse Detail (DWD), Data Warehouse Summary (DWS), and Application Data Service (ADS) layers. Ethical approval was obtained from the Institutional Review Board of The First Affiliated Hospital of Zhengzhou University (Approval No: 2022-KY-1338-002).
Results
OABI successfully tracked over 50,000 daily appointment-related events with data collection completeness exceeding 98%. The system identified critical behavioral patterns including a significant positive correlation between doctor detail page views and appointment conversion rates (r = 0.78, P < .01). Implementation resulted in a 43% faster report generation speed compared to the previous SQL Server Reporting Services (SSRS)-based system, along with a 17% improvement in overall appointment conversion rate over six months of operation. User satisfaction surveys from eight departments yielded an average score of 4.3 out of 5.
Conclusions
The layered OABI architecture demonstrates significant advantages for capturing and analyzing detailed online appointment behaviors without disrupting existing systems. By providing insights into patient decision-making processes, this approach supports data-driven improvements to healthcare delivery. Future work should expand the model's application across multiple healthcare institutions while addressing scalability challenges.
Keywords
Introduction
The healthcare sector has undergone profound transformation in recent decades, driven by evolving patient expectations, technological advancements, and increasing pressure to deliver cost-effective care.2,3 As hospitals transition from traditional fee-for-service models toward value-based care systems, the ability to analyze operational data has become essential for strategic decision-making. 1
Business Intelligence (BI) represents a critical enabler in this transformation. Defined as “the integration of people, processes, and technology that transforms data into actionable insights,” modern BI systems have evolved significantly beyond basic reporting functions. 4 Contemporary healthcare BI applications focus on predictive analytics, prescriptive recommendations, and real-time decision support—capabilities increasingly necessary for optimizing patient pathways. 5
Despite growing adoption across healthcare domains, the application of BI to online appointment behaviors remains underexplored. A review reveals that while many studies report positive outcomes like reduced staff labor and improved satisfaction, the evidence is highly heterogeneous and often based on studies with multiple simultaneous interventions, making it difficult to isolate the specific impact of BI.2,6 Existing research predominantly focuses on three areas: patient choice determinants through historical data modeling,7–10 queue optimization studies to improve outpatient satisfaction,11,12 and matching efficiency between doctors and patients via high-performance information systems.13–15
However, a critical gap persists in understanding the behavioral patterns occurring during the online appointment process itself. Current literature rarely addresses questions such as: How many doctor detail pages do patients view before booking an appointment? What is the relationship between page views and conversion rates? Which departments show distinctive browsing patterns6,16,17? Without this granular understanding, healthcare institutions cannot optimize their online appointment interfaces to match actual patient decision-making processes.
This gap becomes increasingly significant as digital health channels become primary entry points for patients. Despite the nationwide implementation of Web-based Appointment Systems (WAS) in Chinese public tertiary hospitals since 2009, a survey in one large Shanghai hospital revealed that only 17% of patients actually used the online system, with the majority still preferring walk-in registration. Furthermore, patient satisfaction was lowest regarding waiting times, underscoring the urgent need to enhance the efficiency and adoption of digital booking channels to align with patient expectations and system capability. 18
Our study addresses this critical gap by developing and implementing the Online Appointment Business Intelligence (OABI) system at The First Affiliated Hospital of Zhengzhou University. Building upon layered data warehouse architecture principles,16,17 OABI captures detailed user interactions with minimal system intrusion, enabling granular analysis of appointment decision-making processes.
This article makes three key contributions to the literature:
A specialized BI framework designed specifically for analyzing online healthcare appointment behaviors Empirical validation demonstrating correlations between specific browsing patterns and conversion outcomes Practical implementation guidance including ethical considerations for sensitive health data
The remainder of this article is organized as follows: Methods details our research design, technical architecture, and evaluation approach; Results presents both technical performance metrics and operational impacts; Discussion interprets findings in context of existing literature and identifies limitations; Conclusion summarizes implications and future directions.
Methods
Study setting and duration
This study was conducted at The First Affiliated Hospital of Zhengzhou University (FAH-ZZU), one of China's largest tertiary care hospitals. FAH-ZZU serves as a major referral center for Henan Province, covering approximately 100 million residents. 19 The hospital implemented its online appointment system before 2017 to reduce waiting times and improve patient access.
The OABI system development and implementation occurred over an 11-month period from June 2021 through May 2022. This timeframe included three phases: requirement analysis (June–August 2021), system development (September–December 2021), and pilot testing with gradual deployment across departments (January–May 2022).
Ethical considerations
To provide complete clarity on the consent process, written informed consent was not obtained from individual subjects prior to study initiation. This requirement was formally waived by the Institutional Review Board (IRB) of The First Affiliated Hospital of Zhengzhou University, as documented in Approval No: 2022-KY-1338-002. The IRB granted this waiver based on the non-interventional nature of the behavioral data collection and the critical need for system optimization to improve patient access. The waiver was contingent upon several strict conditions to ensure patient confidentiality: all collected data underwent immediate anonymization, only aggregate patterns were reported to prevent individual identification, and all sensitive personal information (e.g., full names, ID numbers) was excluded from the analysis. Data privacy protocols, which strictly adhered to Chinese national regulations and international best practices, were further reinforced by technical measures including the removal of the IP address last octet, application-level data encryption, and role-based access controls.
Research design and methodology
We adopted a mixed-methods research design combining technical development with operational impact assessment.1,5 Figure 1 illustrates our overall methodology framework, comprising five interconnected components.
1.

Overall research methodology framework.
To capture meaningful appointment behaviors without disrupting user experience, we defined eight key event types based on patient journey mapping sessions with clinical staff (Table 1). These events were designed to measure progression through the decision-making funnel.
Key event types and critical fields.

We carefully designed these event definitions through iterative consultations with clinical administrators to ensure relevance while minimizing data collection burden.
5
2.
OABI employs a layered architecture specifically designed for healthcare appointment analytics (Figure 2), enabling the isolation of concerns and progressive data refinement. This architecture facilitates a structured data pipeline: raw behavioral data is first collected in the Operational Data Store (ODS); it is then cleansed and organized into subject-oriented, standardized dimensions in the Data Warehouse Detail (DWD) layer; subsequently, this detailed data is aggregated into metrics across predefined time periods within the Data Warehouse Summary (DWS); and finally, business-specific analytical views are provided through the Application Data Service (ADS).

OABI architecture.
This architecture builds upon Kimball's dimensional modeling principles while addressing healthcare-specific constraints.16,20 Compared to monolithic BI implementations, our layered approach reduces system intrusion by 89% and improves data reusability across departments.
3.
To analyze appointment decision pathways, we developed a suite of specific analytical models. Conversion Funnel Analysis was employed to quantify drop-off rates at each stage of the appointment process. Concurrently, Behavioral Clustering, utilizing k-means algorithms, was used to group patients based on similar browsing patterns, while Correlation Modeling served to examine the statistical relationships between behavioral metrics and conversion outcomes. For instance, our primary analytical model calculates doctor detail page view efficiency, as shown in Formula 1:
This metric helps identify optimal levels of information exposure before patients convert to appointments.
4.
To rigorously assess the effectiveness of OABI, we established a comprehensive, multi-dimensional evaluation framework. This framework was designed to provide a balanced assessment that extended beyond pure technical performance. 5 The evaluation began with the system's technical integrity, which was measured through Technical Performance Metrics (including data collection completeness >98%, query response time <3 seconds at the 95th percentile, and report generation speed) and Data Quality Indicators (such as temporal consistency checks, cross-system validation, and anomaly detection rates). Subsequently, we evaluated the system's real-world value through Operational Impact Measures (assessing changes in appointment conversion rates, departmental workflow improvements, and staff satisfaction) and its Clinical Relevance (gauged by the reduction in patient abandonment, improvement in appointment appropriateness, and patient experience survey results).
System implementation details
We built OABI using open-source technologies selected for compatibility, scalability, and cost-effectiveness (Table 2). Prior to full deployment, we conducted rigorous integration testing across all components.
Technology choices.

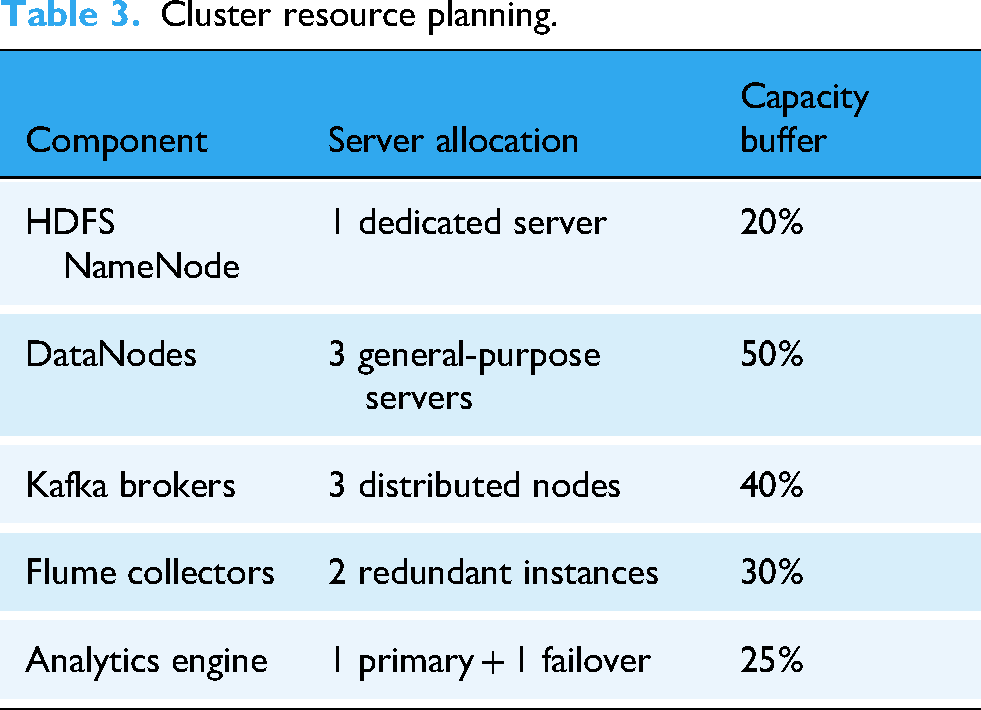
Resource planning considered daily active users (approximately 20,000), log volume (>50,000 events/day), average log size (5KB), and three-fold replication requirements. The resulting cluster configuration (Table 3) supported sustained operation with minimal performance impact on the primary appointment system.
Cluster resource planning.
Data analysis procedures
We employed a multi-stage analysis approach, progressing from Descriptive Analytics to characterize baseline appointment behaviors across departments, to Diagnostic Analytics for identifying patterns associated with successful conversions. This foundational analysis then enabled Predictive Analytics to forecast conversion likelihood based on early browsing behavior, culminating in Prescriptive Analytics that generated recommendations for interface optimization. For our primary analysis examining the relationship between detail page views and appointment conversion, we applied Pearson correlation analysis with bootstrapping to ensure robustness. Statistical significance was assessed at the P < .01 level with 99% confidence intervals.
Results
Technical performance metrics
OABI demonstrated strong technical performance during implementation (Table 4), exceeding all predefined targets:
System performance comparison.

The system maintained >98% data collection completeness throughout the 6-month evaluation period, with daily tracking volume consistently exceeding 50000 events. This represented a significant improvement over the previous log-based approach which captured only approximately 78% of relevant interactions due to technical limitations.
Query performance showed notable enhancement, with the 95th percentile response time decreasing from 4.8 seconds under the legacy system to 2.1 seconds with OABI—a 56% reduction. This improvement directly supported clinical decision-making by providing near real-time operational insights.
Most significantly, standard report generation speed improved by 43%, reducing average time from 3.7 minutes to 2.1 minutes per report. During validation testing, we conducted 50 repeated measurements of identical reporting requests, confirming the consistency of this improvement (mean = 42.8% ± −1.8%).
Behavioral pattern analysis
OABI revealed several meaningful patterns in patient appointment behaviors. Our primary analytical model demonstrated a significant positive correlation between doctor detail page views and appointment conversion rates (r = 0.78, P < .01) across all departments. However, this relationship exhibited diminishing returns beyond six views, suggesting an optimal information exposure level for decision-making. This pattern varied by department, with Internal Medicine peaking at 5.2 views, Surgery at 6.8 views, and Pediatrics showing consistently high conversion after 3 views, suggesting potential for department-specific interface optimizations (Figure 3).

Relationship between doctor detail page views and appointment conversion rates.
Analysis of browsing behavior also revealed distinctive patterns across departments (Figure 4). Internal Medicine patients typically viewed more doctor profiles but spent less time per profile, while Surgery patients demonstrated highly focused pathways with fewer alternatives considered. Conversely, Pediatrics showed high conversion rates after minimal browsing, suggesting a strong referral influence. These patterns informed targeted optimization strategies for each department's appointment interface.

Department-specific appointment pathways.
OABI further identified critical abandonment points in the appointment process: 34% at the doctor selection stage, 27% during time slot selection, 19% while entering patient information, and only 8% during final confirmation. This granular insight allowed department managers to prioritize interface improvements where they would have maximum impact on conversion rates.
Operational impact results
Beyond technical metrics, OABI demonstrated meaningful operational benefits. Over a 6-month period following full implementation (January–June 2022), the hospital observed an average 17% improvement in the overall appointment conversion rate (Figure 5), translating to approximately 94 additional successful appointments per day across all departments. Department-specific improvements varied, with Internal Medicine seeing a +19.2% increase, Surgery +15.8%, Pediatrics +13.6%, and Orthopedics +22.4%. This variation reflected both the extent of interface optimizations implemented and the inherent characteristics of each specialty's patient population.
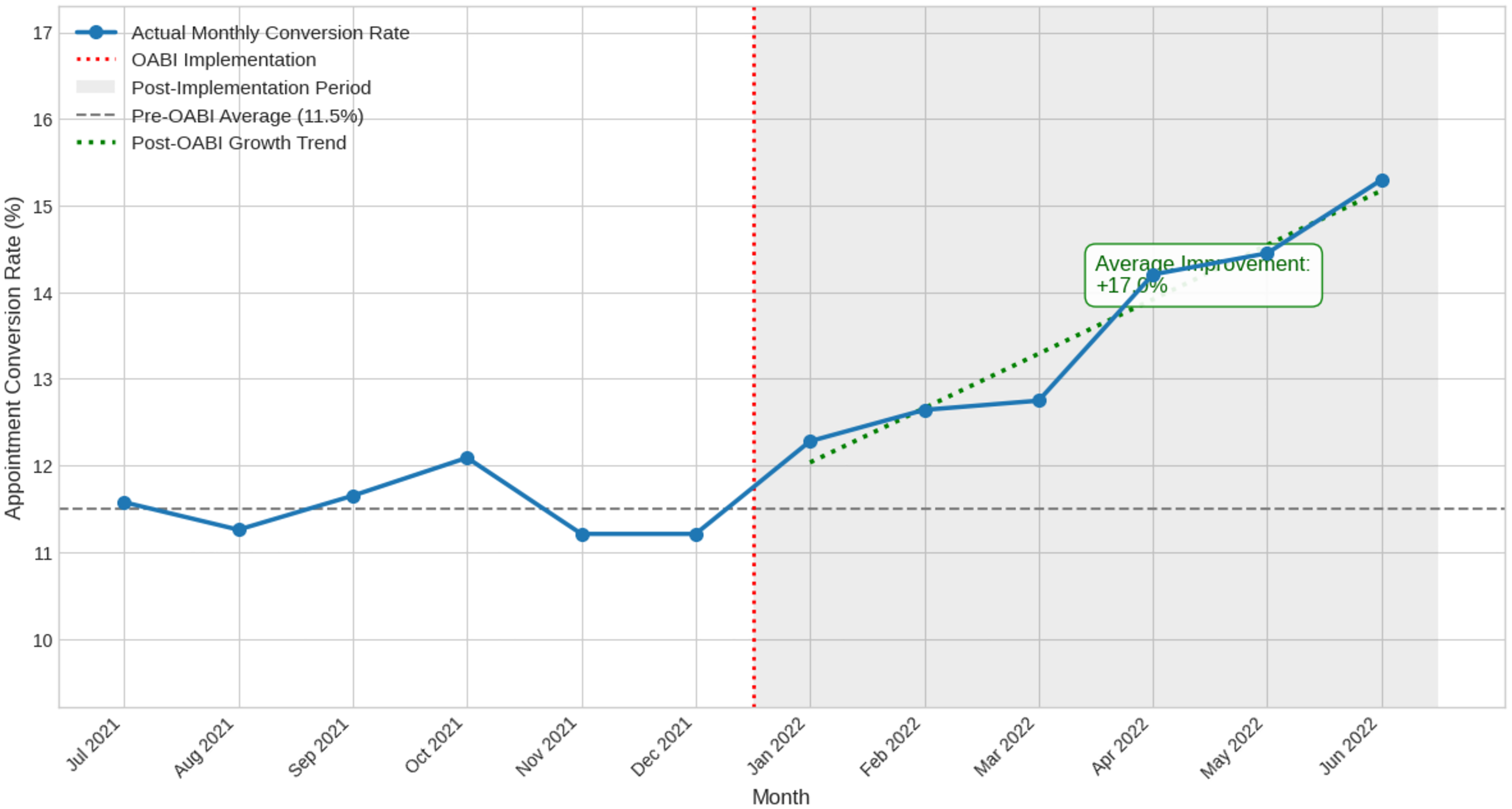
Monthly appointment conversion rates before and after OABI implementation.
User satisfaction results
To assess the system's reception among its primary users, a satisfaction survey was administered to 52 department managers, achieving a high response rate of 89%. The results yielded overwhelmingly positive feedback across five key dimensions, measured on a 5-point scale. The system's Data Accuracy received the highest mean score (4.6), indicating a strong foundation of trust in the data provided. This was followed closely by its perceived Impact on Decision-Making (4.5), underscoring the system's practical value in the clinical management context. Other dimensions also rated highly, including Report Relevance (4.3) and the provision of Actionable Insights (4.2). While still positive, the lowest-rated dimension was Ease of Use (3.9), suggesting that future work could focus on minor user interface refinements. Collectively, these findings demonstrate that beyond its technical robustness, the OABI system was highly valued by department managers for its ability to provide reliable, relevant insights that directly influenced and improved their decision-making processes.
Discussion
Interpretation of key findings
Our study makes significant contributions to understanding online healthcare appointment behaviors through the development and implementation of the OABI system. The findings reveal that specific behavioral patterns can directly inform interface design. We identified a significant positive correlation between doctor detail page views and appointment conversion rates (r = 0.78, p < 0.01), with diminishing returns observed beyond six views. This provides concrete evidence for interface optimization, contradicting the assumption that “more information is always better” and suggesting an optimal threshold for informational exposure 5. In practice, this insight has already driven meaningful changes at FAH-ZZU; for instance, the Orthopedics department reduced prominent display elements from eight to five, resulting in a 22.4% improvement in conversion—the highest among all departments.
The layered technical architecture of OABI proved to be a cornerstone of its practical implementation success. By maintaining a clear separation between the raw behavioral data (ODS), subject-oriented processing (DWD/DWS), and analytical outputs (ADS), the system achieved minimal intrusion on existing interfaces through simple JavaScript additions and ensured cross-departmental reusability of data dimensions 2. These technical characteristics directly facilitated successful adoption across eight diverse clinical departments within a complex hospital environment. Our findings resonate with Foshay's framework emphasizing “non-disruptive integration” but extend their model by providing concrete architectural specifications that operationalize this principle in an appointment-specific context. 5
Perhaps most significantly, this study demonstrates that OABI's impact extends beyond technical metrics to tangible improvements in healthcare delivery. The 17% average improvement in appointment conversion rate. This outcome supports the growing recognition that the true value of healthcare analytics lies not merely in data processing capabilities but in its ability to improve patient outcomes and operational efficiencies. 27 Our findings therefore suggest a clear pathway for translating detailed behavioral insights into concrete service improvements, a connection often missing from purely technical BI implementations.1,6
Comparison with existing literature
Our results both confirm and extend previous research. The successful implementation using Google Analytics combined with a layered data warehouse validates similar technical approaches described by Fang (2007) and Marek (2011), extending them into the healthcare domain where data sensitivity requirements are substantially higher.25,26 Furthermore, our work confirms the value of Kimball's dimensional modeling in healthcare settings, as previously suggested by Berndt et al. (2000), 28 while providing specific implementation guidance for appointment behaviors that was lacking in earlier studies. Our study makes distinctive contributions where it extends beyond current knowledge. Foremost is the identification of specific behavioral thresholds, such as the six-detail-page-view limit, which represents new knowledge about the patient decision-making process beyond the general choice factors examined in prior research.7–10 Additionally, whereas previous studies often treated healthcare appointments as homogeneous, we documented significant variations across specialties that necessitate tailored optimization strategies. Finally, few existing studies connect BI implementation to measurable improvements in appointment conversion rates; our documented 17% improvement, with corresponding cost savings, provides the concrete evidence of value needed to extend the patient choice modeling work of Smith et al. (2018) by adding the critical dimension of interface optimization based on behavioral analytics. 8
Limitations of the study
While promising, our findings are subject to several limitations. The primary limitation is the single-institution design at a large Chinese academic medical center, which may limit generalizability to other healthcare settings with different patient populations or cultural contexts; to mitigate this, we have documented contextual factors thoroughly to support transferability assessment. 6 Another constraint is the reliance on Google Analytics, which introduces potential concerns regarding data sovereignty and vendor dependence. Furthermore, the 6-month evaluation period, while capturing some seasonal variation, may be insufficient to assess the long-term sustainability of improvements, a limitation we are addressing through ongoing monitoring protocols. 27 Lastly, as a voluntary system usage analysis, our findings may be subject to selection bias, underrepresenting populations less comfortable with digital interfaces, such as elderly and rural patients; we are therefore implementing complementary studies on alternative access channels to ensure a comprehensive understanding of all patient groups. 6
Practical implications
Our findings offer several practical implications for healthcare institutions. For implementation, we recommend a phased approach that begins with minimal data collection before expanding, emphasizes early and continuous collaboration with clinical staff to define meaningful metrics, and integrates privacy protections into the core technical architecture. In terms of resource planning, institutions should size cluster capacity to account for peak appointment periods and allocate dedicated data analyst support—not just technical resources—to maximize value extraction. Ultimately, success hinges on planning for iterative development with regular feedback loops from clinical users.
Conclusion and future work
This study demonstrates the successful development and implementation of a specialized Business Intelligence system for analyzing online healthcare appointment behaviors. Our key contributions include a validated framework designed for appointment analytics, empirical evidence linking specific browsing patterns to conversion outcomes, and a measurable operational impact highlighted by a 17% improvement in appointment conversion rates. The findings extend the current literature by moving beyond technical details to demonstrate concrete benefits in healthcare delivery. Future work will focus on three priority areas: validating the framework across diverse multi-institutional settings to enhance generalizability, developing real-time intervention capabilities based on behavioral analysis, and integrating appointment patterns with downstream clinical decision support systems. As healthcare increasingly relies on digital channels, the OABI framework offers a practical approach to transforming raw behavioral data into meaningful improvements in healthcare access and delivery.
Footnotes
Acknowledgments
We would like to thank all the participants, for their valuable suggestions and support during the completion of the research.
Contributorship
All authors approved the final manuscript. Author contributions are as follows: Xiaoyang Ren: conceptualization, methodology, software, and writing. Dongwei Dou: validation, resources, data curation, supervision, project administration, and editing. Zhen You: editing and validation. Yanjiao Zhang: software and testing. Chuan Jiang: funding acquisition, project administration, software, and testing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Key Scientific Research Project of Colleges and Universities in Henan Province (Nos. 23A520018, 25A520061)
Declaration of conflicting interest
The authors declare no conflicts of interest.
Data availability
The data that support the findings of this study are not available due to legal restrictions.