
Abstract
Background
The integration of artificial intelligence and Internet of Things (AIoT) technologies is transforming healthcare delivery systems globally. However, comprehensive evaluation frameworks are needed to assess AIoT technological impact on sustainable healthcare development across economic, organizational, and social dimensions.
Objectives
This research investigates how AIoT technology affects sustainable healthcare development by examining the interconnections between individual economic viability, organizational responsibility, and social equity within the framework of Sustainable Development Goals (SDGs).
Methods
A dual-methodology approach was employed combining factor analysis for quantitative assessment and triple-dimensionality method for qualitative evaluation. The study examined six inter-influence correlations across three dimensions using Social Learning Theory's triadic reciprocal determinism framework. Data analysis focused on healthcare professionals’ AIoT applications, institutional governance, and social equity outcomes.
Results
Healthcare professionals driving socially beneficial AIoT applications achieved the highest comprehensive weight (0.0927), indicating strong correlation between individual economic advantages and social equity outcomes. Medical healthcare professionals’ AIoT skills scored 0.0914, while responsible AIoT governance (healthcare professionals to gain the AIoT skills) achieved 0.0926. These findings validate bidirectional economic-organizational dynamics and demonstrate significant organizational-social equity integration with measurable reciprocal stimulation effects.
Conclusions
AIoT technology represents a paradigmatic shift toward sustainable healthcare systems, creating self-reinforcing ecosystems where improvements in any dimension enhance outcomes across all areas. The study provides empirical validation that AIoT serves as a comprehensive catalyst for achieving “Good Health and Well-being” SDG targets while establishing economically viable and organizationally sustainable healthcare delivery systems.
Keywords
Introduction
Since 2015, the United Nations has stated the 2030 Agenda for Sustainable Development, which proposed 17 core Sustainable Development Goals (SDGs) for global sustainable development. Significantly, it aims to guide governments, local governments, businesses, civil society groups, and other actors in their decision-making, investment, and action directions over the next 15 years, and to jointly create a world where every country achieves stable, inclusive, and sustainable economic growth and everyone has a decent job. Particularly, one of the most important SDGs is the third: 'Good Health and Well-being,' which aims to 'ensure healthy lives and promote well-being for all at all ages.' Nowadays, the global healthcare industry faces unprecedented challenges in achieving this United Nations SDG, driven by rising costs, resource constraints, aging populations, and increasing environmental impacts. 1 These challenges are particularly severe in developing regions with limited healthcare infrastructure. Consequently, sustainable healthcare development has emerged as a critical priority, requiring integrated approaches that address individual economic viability, organizational responsibility, and social equity. 2 Then, the convergence of Internet of Things (IoT) and Artificial Intelligence (AI) technologies into Artificial Intelligence IoT (AIoT) systems presents a promising solution to these healthcare sustainability challenges. 3
The AIoT technology enables massive information sharing through IoT sensors while leveraging AI's analytical capabilities for automated medical data processing and decision-making support. This integration facilitates comprehensive analysis of large healthcare datasets and provides real-time clinical decision support, potentially transforming healthcare delivery through remote consultations, telemedicine, and distance-based medical education programs that transcend geographical and temporal barriers. As a result, in terms of the research gap and issue, despite growing interest in AIoT applications for healthcare, there remains a significant gap in comprehensive evaluation frameworks that systematically assess the impact of the AIoT technology on sustainable healthcare development across multiple dimensions. Current research predominantly focuses on technical implementations rather than holistic sustainability assessments that integrate economic, organizational, and social perspectives. Furthermore, limited empirical studies examine how AIoT technology specifically contributes to achieving SDG health targets through measurable impacts on healthcare accessibility, quality, and equity.
However, making a comprehensive survey on a series of current global healthcare related researches, there is on one to be able to synthetically cross-employ the synergy of individual economic viability, organizational responsibility and social accountability to evaluate the advanced impacts of the AIoT technology on the sustainable development of medical and healthcare through the AIoT Technology in this emerging digital health epoch. For the reason, this research addresses this gap by investigating how AIoT technology influences sustainable global healthcare development through three analytical perspectives: Individual economic viability, organizational responsibility, and social equity accountability.
This investigation addresses the research question: How to effectively and efficiently evaluate the advanced impacts of the sustainable development of the global healthcare through AIoT from individual economic viability, organizational responsibility and social equity analytical perspectives in this emerging digital health epoch? Figure 1 illustrates the study's three primary aims: (1) Constructing an integrated assessment model to measure AIoT's diverse effects on healthcare sustainability, (2) investigating empirical relationships among financial, institutional, and societal elements within AIoT-integrated health systems, and (3) delivering research-informed recommendations for strategic AIoT deployment that supports long-term healthcare sustainability objectives. In detail, the conceptual structure presented in Figure 1 to address this research question, the study adopts an analytical lens grounded in core triple dimensions (individual recognition, organizational development and social tendency) of the recognition-behavior social learning theory (SLT) 4 among interconnected factors. Figure 1 visualizes six reciprocal pathways connecting three fundamental domains: Personal perception (individual financial accessibility—healthcare services transcending temporal constraints), institutional evolution (healthcare organizations’ clinical obligations), and collective orientation (societal fairness corresponding to priority SDGs). This theoretical approach proves especially relevant for examining AIoT healthcare applications because it acknowledges continuous, multidirectional influences among user actions, organizational frameworks, and environmental contexts—rather than assuming unidirectional cause-and-effect sequences. Such bidirectional dynamics are essential for comprehending how digital health innovations reshape care delivery systems. 5 Therefore, through systematic analysis of these three analytical dimensions and their six interconnected relationships (depicted in Figure 1), this study assesses AIoT technology's contribution to advancing sustainable healthcare in the contemporary digital transformation period.

The social learning theory (SLT) triadic reciprocal determinism of the research concept.
In order to effectively and comprehensively assess these six inter-influence correlations of the triadic reciprocal determinism of the SLT, this research adopts a novel dual-analytical framework that synergistically combines the factor analysis (FA) 6 and triple-dimensionality (TD) 7 methodologies to examine the intricate web of relationships within the triadic reciprocal determinism model applied to AIoT healthcare ecosystems. The rationale for this methodological fusion stems from the inherent complexity of healthcare digitalization, which demands both empirical quantification of observable patterns and nuanced interpretation of multidimensional interactions that transcend conventional analytical boundaries. While singular methodological approaches typically excel in either statistical correlation identification or interpretive depth, they fall short of capturing the bidirectional causality and dynamic equilibrium that characterize triadic systems in healthcare technology adoption. The analytical process unfolds through three interconnected phases designed to maximize methodological complementarity while ensuring scientific rigor.
The initial phase centers on the FA operationalization, commencing with comprehensive dataset assembly encompassing AIoT implementation metrics across personal, institutional, and societal levels. Data preprocessing ensures conformity to the FA prerequisites through sample adequacy verification, distributional normality assessment, and variable standardization to enable cross-scale comparisons. Significantly, factor extraction employs principal axis factoring with eigenvalue thresholds exceeding unity, supplemented by scree plot visualization for optimal factor retention decisions. The orthogonal or oblique rotation techniques optimize factor interpretability, while communality calculations reveal the proportion of variance shared among variables within the triadic framework. This quantitative foundation establishes empirically grounded relationships between individual healthcare empowerment, organizational capability enhancement, and societal equity advancement through AIoT integration.
The second phase operationalizes the TD analysis through structured qualitative inquiry that maps the theoretical dimensions of triadic reciprocal determinism onto empirical phenomena. The analytical architecture encompasses three investigative domains: Personal healthcare autonomy and economic sustainability, institutional care delivery transformation and accountability, and collective health equity realization aligned with sustainable development objectives. Data acquisition utilizes multiple qualitative channels including semi-structured stakeholder consultations, organizational case documentation, and policy analysis across diverse healthcare contexts. Thematic analysis procedures employ iterative coding cycles that identify recurring patterns within each dimension while simultaneously exploring cross-dimensional linkages. Weight assignment protocols evaluate thematic prominence through evidence frequency, conceptual depth, and stakeholder consensus, with expert validation ensuring analytical credibility and methodological transparency. Finally, the culminating integration phase synthesizes FA-derived quantitative insights with TD-generated qualitative understandings through convergence analysis and weighted synthesis procedures. Methodological triangulation compares statistical factor patterns with qualitative thematic structures to identify areas of mutual reinforcement and highlight analytical discrepancies requiring additional investigation. This synthetic approach generates comprehensive evaluation metrics for each reciprocal correlation while maintaining analytical transparency and methodological accountability.
Literature reviews
AIoT applications and challenges of healthcare in the SLT's exploration
Specifically, the SLT's exploration was suited to AIoT applications and challenges of healthcare for three critical reasons: Firstly, dynamic interdependence: AIoT healthcare systems inherently involve continuous feedback loops between individual users (patients and healthcare professionals), institutional structures (hospitals and healthcare organizations), and broader social contexts (regulatory frameworks and equity considerations). The triadic model captures these simultaneous, multidirectional influences that static models cannot adequately represent. Secondly, multi-level analysis: The complexity of AIoT implementation requires examining impacts across individual, organizational, and societal levels simultaneously. The triadic framework provides a structured approach to analyze how technological adoption at one level influences and is influenced by changes at other levels. Finally, sustainable development context: Given that this research examines AIoT's contribution to the third most important SDGs, the triadic model's emphasis on reciprocal causation aligns with sustainability thinking, which recognizes that lasting change requires integrated transformation across personal, institutional, and social dimensions.
In detail, the first inter-influence correlation demonstrates how individual economic viability through borderless healthcare access (defined as patients’ and healthcare professionals’ capacity to obtain medical services and knowledge without temporal or geographical constraints via AIoT technology) directly strengthens institutional treatment accountability (operationalized as healthcare organizations’ commitment to delivering quality care through technology-enabled services). Specifically, patients achieve enhanced economic viability by accessing superior medical treatments remotely through AIoT platforms, while healthcare professionals develop the medical and healthcare professionals AIoT skills***** (MHP-AIoTS) 8 which operationally defined as proficiency in utilizing AIoT technologies for continuous professional development and clinical practice—thereby increasing their personal economic prospects. Consequently, enhanced individual economic viability among both patient and professional populations directly reinforces institutional treatment accountability.
The second inter-influence correlation reveals how institutional treatment accountability reciprocally enhances individual economic viability. To fulfill their treatment obligations, healthcare institutions invest in comprehensive AIoT training programs, including real-time monitoring systems and automated alert mechanisms, that cultivate the MHP-AIoTS among their workforce. Additionally, institutions establish professional cloud platforms, predictive analytics infrastructure, and interoperability standards that enhance care quality, collectively constituting the organizational responsibility-taking success with AIoT tools (OR-AIoTT) 9 which defined as institutional capacity to leverage AIoT technologies for fulfilling healthcare delivery commitments.
The third inter-influence correlation demonstrates how institutional treatment accountability advances social equity accountability (operationalized as healthcare systems’ responsibility to ensure fair access and outcomes aligned with the third-priority SDGs). Medical institutions employ the responsible AIoT governance (R-AIoTG) 10 which defined as ethical frameworks governing algorithmic transparency and data protection which is alongside the transparent AIoT decision-making processes (T-AIoTDP), 11 operationalized through accessible performance dashboards that enable public scrutiny of healthcare outcomes.
Implementing responsible governance and transparent protocols requires addressing three foundational ethical dimensions: Bias prevention and mitigation: Healthcare AIoT systems require systematic fairness mechanisms ensuring equitable care across demographic groups through algorithmic auditing, representative data curation, and equity-conscious design practices that prevent technological amplification of healthcare disparities.
Data governance and custodianship: Effective information stewardship encompasses collective data rights and jurisdictional considerations beyond individual privacy. Governance frameworks must establish clear custodial boundaries, protocols for cross-border data transfers, and community-based decision authority, particularly for vulnerable populations requiring enhanced protection.
Dynamic consent frameworks: Contemporary healthcare AIoT environments necessitate sophisticated consent mechanisms transcending traditional single-authorization models, enabling continuous patient agency through adaptive permission structures that provide granular control over data utilization in machine learning systems.
Through investments in advanced technologies—including fifth-generation networks and quantum-resistant encryption—organizations implementing the organizations implementing robust AIoT data protection protocols (OIR-AIoTDPP), 12 such as blockchain-based health records, attract specialized talent in cybersecurity and data science, achieving the better responsible AIoT deployment (R-AIoTD) 13 which operationalized as continuous monitoring systems that reduce institutional liability while enabling enhanced care delivery.
Furthermore, the ethical AIoT practices (E-AIoTP) 14 of the AIoT technology which defined as human-in-the-loop systems maintaining human oversight in automated healthcare decisions—empirically build patient trust and service quality, advancing social equity accountability. The organizational investment in the AIoT technological bias mitigation (OI-AIoTBM), 15 encompassing diverse training datasets, calibration procedures, and inclusive machine learning models, directly addresses equity concerns by ensuring universal device compatibility and equitable treatment access.
The fourth inter-influence correlation reveals how social equity accountability reciprocally drives the public scrutiny of AIoT healthcare applications (PS-AIoTHA) 16 which operationalized through regulatory monitoring and patient advocacy for data rights—compels organizations to implement stronger ethical frameworks, including privacy-by-design architectures. The public health outcome monitoring (PHOM), 17 utilizing real-time population health analytics, creates feedback mechanisms improving organizational practices through evidence-based algorithm refinement. Additionally, the social pressure for healthcare equity, 18 manifested through demands for transparent systems, drives institutions to develop inclusive AIoT solutions featuring diverse datasets, multilingual interfaces, and culturally-adapted technologies.
The fifth inter-influence correlation demonstrates how social equity accountability enhances individual economic viability. The social health improvements from accountable AIoT deployment (SHIA-AIoTD), 19 comprising public health interventions and data transparency platforms, reduce individual healthcare costs through preventive algorithms, early detection systems, and personalized wellness recommendations. Socially responsible development creates the new treatment opportunities in medical and healthcare technology (SR-AIoTDNEOHTE) 20 through novel security analysis and investigative digital systems. The transparent AIoT systems (T-AIoTS), 21 featuring accessible performance metrics, build patient confidence and increase service demand through verified AI-assisted diagnoses and evidence-based recommendations.
Finally, the sixth inter-influence correlation illustrates how individual economic viability reciprocally stimulates social equity accountability. Economically successful individuals and professionals invest in the social health initiatives using AIoT technology (SHIU-AIoT) 22 through foundation grants, technology donations, and pro-bono services while healthcare professionals driving innovation in socially beneficial AIoT applications (HPDISB-AIoTA) 23 establish integrated analytics platforms. These efforts create the medical and healthcare prosperity and evolution from AIoT adoption (IP-AIoTA), 24 operationalized through patent licensing for social healthcare, open-source contributions, and collaborative research initiatives that advance social equity accountability.
Measurement frameworks and skill assessment tools
In terms of research theory, the SLT has been extensively employed since Miller and Dollard first explored interactive imitation learning within the framework of human behavior in 1941, moving beyond the early tradition of strict behaviorism to establish foundational principles for understanding how individuals acquire behaviors through observation. Furthermore, Rotter introduced the concept of expectation into the human learning process in 1954, incorporating early cognitive elements that would later prove instrumental in expanding beyond purely behavioral explanations of learning. 25
Then, in the 1960s, Albert Bandura integrated cognitive elements into the human learning process and realized that human learning behavior is accomplished in a social context through observation, imitation, and modeling. This pivotal development marked the transition from traditional behaviorism to a more comprehensive understanding of learning that acknowledged the part of individual cognition, organizational context, and environmental and social factors in forming behavior. Hence, the basic theoretical approach of the SLT is the modular concept of triadic reciprocal determinism, which emphasizes that individuals are both products and producers of their environment. 26 This the triadic reciprocal determinism examines six inter-influence correlations among three interactive factors: Personal conditions (cognitive abilities, beliefs, attitudes; individualism), organizational influences (sense of belonging, organizational identification, organizational culture; organizationalism) and social reactions (social context, social conventions; socializationism). These six inter-influence correlations include: Person to organization (self-efficacy beliefs determine organizational choices) and organization to person (organizational performance outcomes change self-perception); organization to society (organizational culture changes social identity) and society to organization (social identity establishes organizational norms); society to people (social models direct individual behavior learning) and people to society (individual traits trigger different social reactions). 27
Specifically, building upon this foundational framework, the triadic reciprocal determinism reveals six inter-influence correlations that demonstrate the complex interplay between economic incentives, organizational dynamics, and social accountability mechanisms. These six inter-influence correlations illuminate how learning occurs not merely through individual cognitive processes, but through dynamic interactions that involve economic considerations and social responsibility factors. 28 This integrated framework demonstrates that triadic reciprocal determinism of the SLT operates not only through cognitive and behavioral mechanisms but also through complex economic and social accountability systems. The six inter-influence correlations reveal that learning in organizational and social contexts involves continuous negotiations between individual economic interests, organizational responsibility imperatives, and social accountability expectations. The theoretical significance of this integration lies in its demonstration that human learning behavior in organizational and social contexts cannot be fully understood without considering the economic dimensions of behavioral choices and the accountability mechanisms that govern social interactions. These correlations show that the observational learning, imitation, and modeling processes identified by Bandura are deeply embedded within economic and social responsibility frameworks that shape both the content and context of learning experiences. 29
The complete set of six inter-influence correlations creates a comprehensive cycle: Individual economic benefits drive organizational responsibility (first), which enhances individual economic viability (second), while organizational responsibility drives social accountability (third), which in turn enhances organizational responsibility (fourth) and individual economics (fifth), ultimately leading to individual economic success supporting social goals (sixth). This cyclical pattern demonstrates the self-reinforcing nature of the triadic relationships and illustrates how positive behaviors and outcomes in one domain can catalyze improvements across all three domains 30 as shown in Figure 2.

The main triadic reciprocal determinism of the social learning theory (SLT).
Statistic methodology
With respect to the statistic methodology, first of all, the research methodology utilized the Likert scale because this measurement tool generates quantitative information that delivers extensive insights while maintaining simplicity in administration and interpretation, facilitating straightforward analysis of gathered data. 31 Furthermore, the Likert scale demonstrates versatility in assessing personality characteristics, viewpoints, conduct, attitudes and perspectives. Rather than limiting responses to binary choices, investigators can construct questions with multiple response options across a continuum. Consequently, owing to these distinctive features of analytical capability and adaptability, the Likert scale has become extensively implemented across diverse and multifaceted social science investigations, as participants can indicate their level of agreement or disagreement with presented statements, yielding data that is more efficient and manageable to process compared to responses from open-ended, qualitative questionnaire items. 32
Secondly, the investigation of interdependencies among evaluated attitudes, criteria, and sub-criteria employed a comprehensive methodological triangulation incorporating the SLT, the quantitative analysis FA approach and quantitative analysis TD method. This integrated framework facilitated the systematic examination of large-scale questionnaire responses enhanced by expert weighting procedures to provide robust analytical insights into complex measurement systems. In light of contemporary developments within quantitative analysis of social science methodology, the FA has established itself as a robust investigative instrument for examining latent associations and interconnections within extensive survey datasets. The main reason is that the FA approach was employed to assess the quantitative data from large-scale Likert scale questionnaires with higher research adaptability and representativeness in quantitative analysis. This is because high factor loadings and communalities from the FA approach indicate that items accurately represent a construct, thereby contributing to construct validity.
In detail, in consideration of research validity, the validity of Kaiser–Meyer–Olkin (KMO) test in determining if the data is appropriate for the FA which means the high KMO values indicate that the variables share common variance due to underlying factors, suggesting the data's suitability for the FA. 33 Kaiser 34 introduced a measure of the KMO statistic, which can vary from 0 to 1, indicates the degree to which each variable in a set is predicted without error by the other variables. A value of 0 indicates that the sum of partial correlations is large relative to the sum correlations, indicating FA is likely to be inappropriate. A KMO value close to 1 indicates that the sum of partial correlations is not large relative to the sum of correlations and so FA should yield distinct and reliable factors. It means that patterns of correlations are relatively compact, and so FA should yield distinct and reliable factors. Values smaller than 0.5 suggest that you should either collect more data or rethink which variables to include. 35 Specifically, Kaiser 36 defined that the KMO >0.9 were marvelous, in the .80 s, meritorious, in the 0.7 s, middling, in the 0.6 s, mediocre, in the 0.5 s, miserable, and less than 0.5, unacceptable. Recently, Cureton 37 suggest accepting the evaluated factors for FA approach during the KMO is bigger than 0.5; the evaluated factors are mediocre for FA approach during the KMO is between 0.5 and 0.7, and the evaluated factors are good for FA approach during the KMO is between 0.7 and 0.8.
On the other hand, in sight of research reliability in quantitative analysis, the Bartlett's Test of Sphericity (STS) of the FA approach tests whether a matrix (of correlations) is significantly different from an identity matrix (filled with 0) in the quantitative measurements and simultaneously, the STS can test whether the correlation coefficients in the testing computation of the probability that the correlation matrix has significant correlations among at least some of the variables in a dataset, a prerequisite for FA to work as well. It is very important that while it is often suggested to check whether Bartlett's test of sphericity is significant during implementing with the FA approach, one needs to remember that the test is testing a pretty extreme scenario (that all correlations are non-significant). As the sample size increases, the STS test used to be identified the quantitative analysis research reliability by measuring the significance of the evaluated data, which makes it particularly useful or informative in well-powered studies. Significantly, the significance number of the STS test is highly equivalent to test of the Cronbach's alpha (“ Cronbach's
To evaluate the validity and reliability of the FA measurement approach, multiple analytical procedures were implemented. Firstly, internal consistency was examined through the composite reliability (CR) calculations by computing the factor loading of each evaluated factors. 40 The CR is calculated by summing the squares of the standardized factor loadings and dividing it by the sum of the squares of all standardized factor loadings and the residuals. CR quantifies the amount of shared variance between the latent construct and its measured variables. A larger CR value indicates greater internal consistency and better measurement of the construct. Significantly, previous studies have shown that the CR of latent variables should be higher than 0.6, and recent research generally recommends that the CR value should be at least 0.70 to ensure that the construct has good internal reliability. 41
Then, convergent validity was tested to verify that indicators measuring identical constructs demonstrate strong correlations, and discriminant validity was analyzed to ensure that indicators measuring distinct constructs show minimal correlation. 42 Moreover, regarding convergent validity, the examination confirmed that indicators demonstrated substantial loadings on their corresponding constructs and that the average variance extracted (AVE) for each construct surpassed the 0.5 threshold, demonstrating that each construct maintains a robust connection to its underlying theoretical framework. 43 The results showed that indicator loadings were statistically significant for their respective constructs, AVE values for all constructs exceeded the 0.5 criterion, and CR coefficients for all constructs surpassed the 0.7 benchmark, confirming that the indicators demonstrate strong associations with their corresponding theoretical constructs. 44 Then, in consideration with the discriminant validity, confirm that different constructs are not too highly correlated by comparing the AVE of two constructs to the square of their correlation coefficient, or by examining the off-diagonal elements of the correlation matrix to ensure they are lower than the square root of the AVE for each construct. If the square root of the AVE of each construct is greater than its correlation coefficient with other constructs, it means that the construct has good discriminant validity and shows uniqueness among the constructs. 45 Statistically, the equations for the CR and AVE are expressed in Appendix A-2.
Following the completion of quantitative analysis through the FA methodology, this research interdisciplinarily implemented the fluid-mechanics entropy technique and procedure to establish a qualitative evaluative TD structure. The entropy procedure was chosen because it exhibits substantial validity and dependability when implemented in suitable circumstances, demonstrating strong associations with conventional dependability measures. This strategy was formulated to comprehensively evaluate and scrutinize the six mutual correlation configurations of the SLT when appraising expert surveys, while incorporating the findings obtained from the quantitative FA approach. Moreover, to preserve methodological rigor and augment analytical exactness, the research employed the TD structure as a qualitative evaluation method utilizing weighted assessments to examine experts’ responses. This technique was specifically constructed to appraise professionally developed questionnaire data and guarantee elevated research trustworthiness and exactness through the incorporation of entropy-driven multi-attribute decision-making mechanisms. The “entropy method” is a technique used to assess the trustworthiness of qualitative research using Lincoln and Guba's four criteria: Credibility, transferability, dependability, and confirmability. Researchers establish credibility by ensuring findings are believable to participants through techniques like member checking. Transferability is achieved by providing rich, detailed descriptions of the context for other researchers to assess applicability. Dependability is established by a thorough audit trail that documents the entire research process, allowing for replication. Confirmability is demonstrated by ensuring findings are grounded in the data, rather than the researcher's biases, through methods like reflexivity and peer debriefing.
Specifically, the credibility and dependability of the qualitative analysis employing the TD methodology were evaluated using Cronbach's
The consolidation of the quantitative analysis FA approach for analyzing the large-scale questionnaire and qualitative analysis of TD method for assessing the expert's questionnaire is vital for completely articulate evidence of four primary elements: Credibility, confirm-ability, dependability, and transferability of outcomes, to ensure the trustworthiness of the measured results and evaluated conclusions extracted are meaningful and accurate with the higher reliability and validity. 55 In detail, this research establishes credibility by ensuring that measured results are believable to participants through multiple perspectives (large-scale and expert questionnaires) during the data collection process, thereby ensuring data rationality. 56 Transferability is achieved through thorough description of research results across multiple data collection methods, making the measured results more applicable to similar situations or individuals by providing rich, detailed descriptions of the research context to assess applicability. 57 Dependability is established through a comprehensive audit trail that documents the entire research process, allowing for replication by using rigorous data collection techniques, procedures, and analysis methods that are adequately documented. Finally, confirmability is demonstrated by ensuring that findings are grounded in the data rather than researcher biases, achieved through triangulation and member checking of data, as well as through group interviews and practice reflection to address potential personal biases. 58
Research design
Research steps
This research adopts a dual-method research design that synthesizes quantitative FA with qualitative TD to investigate connections among AIoT technological elements spanning three evaluative perspectives: Patient and professional economic accessibility without geographical constraints, healthcare organizations’ clinical accountability, and equitable healthcare delivery corresponding to SDG priorities. The investigation proceeds through four distinct stages:
Foundation-building stage: Determining suitable analytical approaches that align with research aims and grounding the investigation in SLT's reciprocal influence principles. Construct operationalization stage: Translating the three evaluative perspectives and their six reciprocal pathways into measurable indicators for assessing AIoT's contribution to sustainable healthcare advancement. Empirical investigation stage:
Survey-based analysis: Collecting responses from 300 participants and utilizing FA techniques to reveal primary technological enablers and cross-dimensional connections. Measurement quality verified through CR and AVE metrics to establish internal coherence and convergent validity. Expert consultation analysis: Gathering insights from 30 healthcare specialists and employing TD approaches to extract thematic patterns. Analytical rigor confirmed through Cronbach's α coefficients to demonstrate credibility, consistency, and applicability of outcomes. Convergence and interpretation stage: Merging survey-based and expert consultation findings to produce holistic understanding that resolves the central research inquiry and establishes a research-informed model for strategic AIoT deployment within sustainable healthcare frameworks.
Figure 3 depicts these four investigative stages in sequence.

Main research design and steps.
Data collection
To enhance representativeness and methodological rigor in quantitative data collection, this research adapted a Likert scale survey to be the surveyed instrument targeting 300 Taiwanese and 30 experts adult participants through face-to-face interviews in order to successively assess participants’ attitudes. Because the Likert scale application in the questionnaire was specifically designed for capturing quantitative data suitable for statistical analysis. In detail, this measurement tool of Likert scale generates quantitative information that delivers extensive insights while maintaining simplicity in administration and interpretation, facilitating straightforward analysis of gathered data. 59 Furthermore, the Likert scale demonstrates versatility in assessing individual characteristics, viewpoints, conduct, attitudes, and perspectives. Rather than limiting responses to binary choices, investigators can construct questions with multiple response options across a continuum, 60 such as a 5-level scale: Extremely important, important, normal, not important, extremely not important. Due to these distinctive features of analytical capability and adaptability, 61 the Likert scale has become extensively implemented across diverse and multifaceted social science investigations, 62 as participants can indicate their level of agreement or disagreement at each level of the Likert scale. Inductively, the yielding data with presented statements of Likert scale in quantitative analysis that is more efficient and manageable to process compared to responses from open-ended, qualitative questionnaire items of qualitative analysis. In detail, the primary survey question examined participants’ perceptions regarding the significance of the MHP-AIoTS in balancing the individual medical no time-boundaries economic viability considerations with the medical and healthcare institutions treatment responsibilities toward the achievement of the social equality accountability of the third most important SDGs on the sustainable global healthcare advancement. Responses were captured using a five-point Likert scale ranging from “extremely unimportant” to “extremely important.” Furthermore, the question of 300 questionnaire was designed as “Please to tell me, what importance of the MHP-AIoTS during evaluating the impact of the artificial intelligence internet of things (AIoT) on sustainable development of medical and healthcare?”
With respect to the Institutional Review Board (IRB) requirement, this research belongs a waiver of IRB requirements in social science research. 63 The officially main reasons: First of all, this research is the social science research; not the human subject research. Secondly, the data collection of this research was just only to collect the interviewees’ questionnaire's comments with following the six waiver conditions 64 of the IRB requirements of Academia Sinicam, Center of Taiwan Academic Research Ethics Education, Taiwanese Ministry of Science and Technology and Ministry of Education: (1) The entire interviewees were directly interviewed in person with the understanding of this research content 65 ; (2). the entire interviewees did totally agreed with the questionnaire's responses to be utilized for this research 66 ; (3) the entire were over 18-year-old which is the legal age in Taiwan; (4) the entire interviewees were directly consent 67 ; (5) no any personal information or concrete participants’ identification was disclosed in the research and questionnaires ; (5) only questionnaire fill-out action was required in public place and no interactive and invasive measures were used in the collection processes and (6). the project was assessed as minimal risk, ensuring that participation did not expose subjects to risks greater than those faced by nonparticipants. 68
Thirdly, in view of minimal risk studies of the 45 CFR 46.116 (Common Rule) for waiving research approval requirements, which established from the National Institutes of Health (NIH), 69 United States Federal regulation 70 and recent US Food and Drug Administration (FDA) Guidance, the questionnaire data collection of this research was to completely poses no more than minimal risk to participants with six respects of the waiver of Taiwan's IRB requirement which totally did not counter the definition of Minimal risk (45CFR 46.102) 71 : The probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests 72 and completely respect the minimal risk standard 73 : Is often defined by comparing the probability and magnitude of anticipated harms with the probability and magnitude of harms ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests. 74
Specifically, waived IRB requirement cases must not involve vulnerable populations such as minors, detainees, Indigenous peoples, pregnant women, persons with disabilities, individuals with mental illness, or others deemed to be under undue coercion or incapable of independent decision-making. Furthermore, the research must present minimal risk, with no greater risk to participants than that experienced in daily life. Critically, this research clearly completely and accordingly qualifies as a waiver of IRB requirement in social science research. 75
Taking next step, with respect to the expert evaluation component for the qualitative analysis incorporated the TD method through expert consultation, the Delphi method was applied for the data collection because the anonymity of the participants also helps prevent the “halo effect,” which sees higher priority given to the views of more powerful or higher-ranking members of the group. 76 By conducting Delphi method, consensus can be reached over time as opinions are swayed, making the method very effective. In contrast with many other types of interviews and focus groups, Delphi method allow participants to rethink and refine their opinions based on the input of others, contributing to a more reflective and thoughtful process. 77 As a result, the stability and reliability of a research instrument or indicator was measured through the consensus of multiple experts in the Delphi method to effectively reach the higher expert's reliable 78 and simultaneously, whether a research instrument can truly measure the claimed concept or content was assessing through experts’ judgment to efficiently achieve the higher expert's reliable. 79 Therefore, the Delphi method is powerful method to make the survey questions in a questionnaire accurately reflect the concept being measured to obtain the higher research validity and reliability. 80 Particularly, the expert's questionnaire of this research adapted the Delphi method because the Delphi method was created for a structured decision support technology that aims to obtain relatively objective information, opinions and insights through the independent and repeated subjective judgments of multiple experts during the information collection process 81 by affirming the research group and most studies use between representative 15 and 20 experts under the higher expert's validity and reliability in the research. 82 Specifically, in sight of the most appropriate expert's survey number of Delphi method, Ludwig 83 directly confirmed that in conditions of homogeneity, 10–15 experts are enough to achieve the higher expert's reliability and validity as well. Successively, Witkin, Altschuld, and Altschuld 84 groundbreakingly point out that a Delphi panel under 50 experts could be sufficient. Recently, Delbecq 85 provide a systematic guideline for the design and administration of a survey number of the Delphi method, 86 showing that the number of expert panel members can vary in relation to the specific aims and context of the research with the higher expert's validity and reliability. 87 Especially, in consideration of the professional validity and reliability of the Delphi method, the Delphi method seeks to aggregate opinions from a diverse set of professional experts, and it can be done without having to bring everyone together for a meeting. 88 Since the responses of the participants are anonymous, individual panelists don’t have to worry about repercussions related to their opinions. 89
Critically, taking the expert panel composition and rationale into consideration, established methodological standards for mixed-methods research designs stipulate that expert participants should comprise a minimum of 15–30 in order to maintain validity and reliability within Delphi framework applications. This threshold ensures adequate specialist representation while preserving analytical integrity in accordance with the Delphi method disciplinary. Consequently, thirty domain experts were recruited through purposive sampling and engaged via structured in-person interviews during questionnaire administration.
The Delphi method can facilitate comprehensive engagement with complex survey instruments while enabling immediate clarification of technical terminology, thereby optimizing response quality and construct validity. In detail, the expert panel comprised four distinct professional categories: Ten academic researchers with extensive experience (>10 years) in AIoT-related investigations, ten senior healthcare industry professionals with substantial field experience (≥10 years), five AIoT application specialists with proven expertise (≥5 years), and five healthcare sector practitioners with relevant professional background (≥5 years). This composition ensured diverse perspectives while maintaining sufficient expertise depth across all relevant domains.
Particularly, experts and specialists evaluated comparative assessments and frameworks between the healthcare professionals to gain the AIoTS and the comprehensive professional communication and education, effectively constructing the AIoT-enabled preventive care (CPS-AIoT-PC). In detail, the expert's interviewed question was designed as “Please to tell me, what importance do you compare the importance of the medical and healthcare professionals AIoT skills (MHP-AIoTS) with the medical and healthcare professionals AIoT skills (MHP-AIoTS) during evaluating the impact of the artificial intelligence internet of things (AIoT) on sustainable development of medical and healthcare?”. The expert judgments utilized a five-point Likert scale spanning from “negligible significance” to “paramount importance” within pairwise comparison matrices.
Evaluated measurements
FA measurements of quantitative analysis
Following the computational procedures outlined in equations (1) and (2) within the quantitative FA methodology, comprehensive survey instruments were deployed to systematically gather extensive empirical data. From an initial distribution of 300 surveys, 278 responses met validity criteria, yielding an acceptance rate of 92.67%. The exclusion of 22 instruments resulted from participants’ refusal to authorize utilization of their responses for research purposes, necessitating their removal from the analytical dataset. The accepted responses encompassed four geographical divisions across Taiwan: The northern territory (including Chilung, Taipei, New Taipei, and Taoyuan municipalities), the central zone (comprising Hsinchu, Miaoli, Taichung, and Changhua municipalities), the southern area (encompassing Yunlin, Chiayi, Tainan, and Kaohsiung municipalities), and the eastern territory (covering Yilan, Hualien, and Taitung municipalities). The demographic characteristics and distributional properties of these 278 validated survey responses are presented in Table 1.
The descriptive statistics of 278 valid large-scale questionnaires.

Chilung, Taipei, New Taipei, and Taoyuan cities.
Hsinchu, Miaoli, Taichung, and Changhua cities.
Yunlin, Chiayi, Tainan, and Kaohsiung cities.
Hualien and Taitung counties.
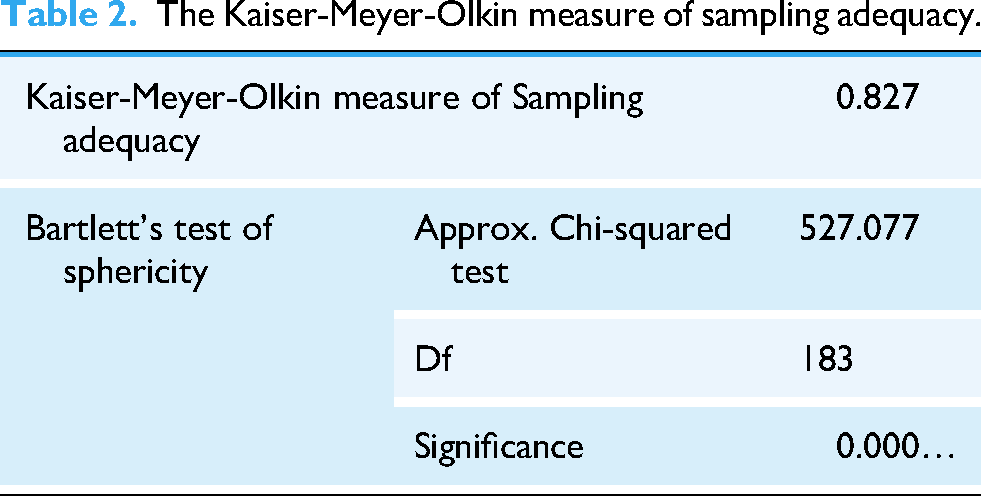
Consequently, the 278 valid questionnaires contained the 169 (60.78%) males questionnaires and 109 (39.12%) female questionnaires and 123 of 278 valid questionnaires were collected form the middle Taiwan. Significantly, the 184 (67.27%) of 278 valid questionnaires never use the AIoT to handle healthcare issues before and 234 (84.17%) of 278 valid questionnaires have heard the third critical SDGs before. Critically, 231 (80.09%) of 278 valid questionnaires are willing to learn the AIoT technological applications for achieve the third critical SDGs. Subsequently, the FA quantitative approach proved entirely suitable for examining the 278 validated survey responses. This appropriateness was confirmed through statistical adequacy measures: The KMO sampling adequacy index yielded a value of 0.827, substantially exceeding the recommended threshold of 0.7 which expressed these large-scale data were meritorious for the quantitative analysis FA approach. Critically, the statistical significance value of the STS test for the FA approach demonstrated p = 0.000 (p < 0.05), satisfying the criteria for multivariate analysis within a 95% confidence level, as documented in Table 2.
The Kaiser-Meyer-Olkin measure of sampling adequacy.
Furthermore, the sixteen evaluated factors were computed in Table 3 by following the equations of the FA approach, AVE, and CV detailed in Appendices A-1 and A-2.
The communalities of entire evaluated criteria.

AIoT: artificial intelligence internet of things; SDG: sustainable development goal; MHP-AIoTS: medical and healthcare professionals AIoT skills; R-AioTG: responsible AIoT governance; OR-AIoTT: organizational responsibility-taking success with AIoT tool; T-AIoTDP: transparent AIoT decision-making processes; OIRAIoTDPP: organizations implementing robust AIoT data protection protocols; R-AIoTD: responsible AIoT deployment; E-AIoTP: ethical AIoT practice; OI-AIoTBM: organizational investment in the AIoT technological bias mitigation; PS-AIoTHA: public scrutiny of AIoT healthcare application; PHOM: public health outcome monitoring; SHIA-AIoTD: social health improvements from accountable AIoT deployment; SR-AIoTDNEOHTE: Socially responsible development creates the new treatment opportunities in medical and healthcare technologyT-AIoTS: transparent AIoT systems; SHIU-AIoT: social health initiatives using AIoT technology; HPDISB-AIoTA: healthcare professionals driving innovation in socially beneficial AIoT applications.
As a results, Table 3 distinctly lists a total of seventeen commonalities from the correlated measurements of the FA approach. The assessed factors were defined as the core evaluation criteria by verifying commonality values higher than 0.7, with AVE higher than 0.5 and CV higher than 0.6. The factors meeting these verified conditions were the MHP-AIoTS (0.867) with the values of the AVE (0.6836) and CV (0.8661); PHOM (0.862) with the values of the AVE (0.7623) and CV (0.9058); medical and healthcare prosperity and evolution from AIoT adoption (IP-AIoTA) (0.829) with the values of the AVE (0.6947) and CV (0.8722); PS-AIoTHA (0.819) with the values of the AVE (0.6724) and CV (0.8603); SR-AIoTDNEOHTE (0.813) with the values of the AVE (0.6593) and CV (0.8531); T-AIoTDP (0.804) with the values of the AVE (0.6698) and CV (0.8588); E-AIoTP (0.797) with the values of the AVE (0.628) and CV (0.835); R-AIoTG (0.792) with the values of the AVE (0.5574) and CV (0.7902); OR-AIoTT (0.785) with the values of the AVE (0.5625) and CV (0.7939); SHIA-AIoTD (0.769) with the values of the AVE (0.5531) and CV (0.7877) and HPDISB-AIoTA (0.757) with the values of the AVE (0.5971) and CV (0.8164). As a results, these ten core evaluation criteria within the six inter-influence correlations of the triadic reciprocal determinism of the SLT were highly correlated and appropriate for evaluating the research topic. Conversely, the other evaluated factors were excluded as core evaluation criteria due to not meeting the reliability and validity requirements of the quantitative FA approach.
TD measurements of qualitative analysis
Following the implementation of the FA approach, the complete communality values for each criterion were subsequently incorporated into equations (3) and (4) within the qualitative analytical framework. This process involved processing thirty validated expert-weighted survey instruments through entropy statistical computations, with preliminary calculations presented in Table 3 and final results documented in Table 4.
The TD evaluated criteria weighted measurement of six inter-influence correlations of the triadic reciprocal determinism.

TD: triple-dimensionality; SDG: sustainable development goal; R-AioTG: responsible AIoT governance; OR-AIoTT: organizational responsibility-taking success with AIoT tool; T-AIoTDP: transparent AIoT decision-making processes; SHIA-AIoTD: social health improvements from accountable AIoT deployment; SR-AIoTDNEOHTE: Socially responsible development creates the new treatment opportunities in medical and healthcare technology; HPDISB-AIoTA: healthcare professionals driving innovation in socially beneficial AIoT applications; SLT: social learning theory; PS-AIoTHA: public scrutiny of AIoT healthcare application.
In Table 4, the evaluated results show that the highest comprehensive weights of the MHP-AIoTS (0.0914) in the first inter-influence correlations of the individual medical no time-boundaries economic viability directly strengthening the medical and healthcare institutions treatment responsibilities and HPDISB-AIoTA (0.0927) in the six inter-influence correlations of the individual medical no time-boundaries economic viability reciprocally stimulating the social equality accountability of the third most important SDGs were located at the medical and healthcare prosperity and evolution from AIoT adoption (IP-AIoTA) in the six inter-influence correlations of individual medical no time-boundaries economic viability reciprocally stimulating the social equality accountability of the third most important SDGs.
Furthermore, the R-AIoTG (0.0926), T-AIoTDP (0.0915), E-AIoTP (0.0903) in the third inter-influence correlations of the medical and healthcare institutions treatment responsibilities effectively promoting the social equality accountability of the third most important SDGs and OR-AIoTT (0.0924) in the second inter-influence correlations of the medical and healthcare institutions treatment responsibilities conversely promote the individual medical no time-boundaries economic viability were located at the SHIA-AIoTD in the fifth inter-influence correlations of the social equality accountability of the third most important SDGs potentially triggering the individual medical no time-boundaries economic viability.
Critically, to establish the trustworthiness of findings derived from the qualitative TD method, this research employed multiple validation strategies for the thirty expert assessments of pairwise weights across the ten core evaluation criteria within the six reciprocal pathways of the SLT's framework. Firstly, triangulation: Expert responses were cross-verified through multiple data sources, including: (1) Comparison of expert-assigned weights with quantitative survey patterns from the 300-participant sample, (2) examination of consistency between expert assessments and existing literature on AIoT healthcare implementations, and (3) validation against documented healthcare outcome metrics from AIoT-enabled institutions. Secondly, member checking: Draft findings and interpretations were returned to a subset of participating experts for verification, allowing them to confirm accuracy of their weighted assessments and clarify any misinterpretations. Expert feedback resulted in refinement of thematic categorizations and strengthened the validity of criterion prioritizations. Thirdly, peer debriefing: Research procedures and preliminary findings were reviewed by independent healthcare technology researchers not involved in data collection, providing external perspective on analytical rigor and interpretation credibility. Finally, audit trail documentation: Comprehensive records of expert selection criteria, weighting procedures, analytical decision-making processes, and interpretation development were maintained to ensure dependability and enable external review of methodological transparency.
Through these qualitative validation procedures, the expert-weighted assessments demonstrated strong credibility, confirmability, dependability, and transferability—establishing that the measured results and evaluated conclusions are meaningful, trustworthy, and applicable to broader AIoT healthcare contexts.
Evaluated discussion
The empirical findings from Table 4 unveils a revolutionary transformation in healthcare delivery systems, where AIoT technologies catalyze fundamental restructuring of healthcare ecosystems through dynamic triadic interconnections. The evidence transcends conventional technological augmentation, revealing comprehensive reimagining of healthcare service paradigms that dissolve traditional demarcations between personal, institutional, and societal healthcare domains. In terms of the personal healthcare empowerment through chronological access liberation, this empirical research disclosed unprecedented bidirectional economic-institutional dynamics that challenge established healthcare economic frameworks. Patients achieving chronological adaptability and financial accessibility via AIoT platforms automatically catalyze institutional enhancement of care delivery mechanisms and treatment excellence benchmarks. This interaction functions reciprocally, where institutional advances in AIoT-supported treatment capacities concurrently diminish personal healthcare expenditures and temporal commitments while propelling increased individual financial access toward institutional technological advancement. Hence, this discovery constitutes a theoretical revolution in healthcare economics by establishing that AIoT platforms generate exceptional chronological adaptability in resource distribution and deployment. Healthcare consumers now engage with medical services unconstrained by conventional temporal limitations, fundamentally transforming healthcare utilization economics through decreased opportunity expenses, reduced transportation costs, and optimized intervention scheduling. The ramifications extend beyond personal convenience toward systemic economic effectiveness, indicating that chronological healthcare emancipation produces multiplicative economic advantages throughout the comprehensive healthcare network.
In sight of the institutional Evolution through accountability-focused healthcare models, the organizational analysis exposes fundamental institutional metamorphosis mechanisms where healthcare organizations transition from episodic intervention models toward comprehensive accountability-focused paradigms. Organizations amplifying treatment accountabilities through AIoT integration systematically enhance healthcare accessibility and excellence for marginalized populations, directly promoting sustainable development targets. This evolution functions bidirectionally, as social equity accountability mandates compel healthcare organizations to embrace more comprehensive AIoT frameworks and broaden treatment capacities to satisfy universal coverage mandates. Particularly, the importance centers on demonstrating that AIoT platforms compel healthcare organizations to broaden their institutional responsibilities beyond conventional care provision to include continuous health surveillance, predictive intervention, and proactive wellness administration. This constitutes essential progression toward sustainable healthcare networks that emphasize prevention over intervention, fundamentally restructuring institutional accountability and service provision models.
In view of the social justice enhancement through universal accessibility frameworks, the societal dimension exhibits powerful reciprocal stimulation mechanisms connecting equity advancement with personal empowerment. Systematic enhancements in healthcare justice establish conditions facilitating individual patients’ access to more economical, accessible, and chronologically flexible healthcare services. Concurrently, when individuals secure economic healthcare benefits through AIoT platforms, these advantages automatically advance broader social justice outcomes and sustainable development progression. Valuably, this discovery provides persuasive evidence for AIoT technology's function in promoting sustainable development through quantifiable social equality accountability mechanisms, establishing systematic channels for diminishing healthcare inequalities and improving universal access to quality services. The empirical documentation demonstrates that social justice improvements automatically produce individual economic advantages, indicating that investments in AIoT-supported social equality programs generate multiplicative returns through enhanced individual economic results.
In association with the strategic policy development and multi-context healthcare implementation, the triadic discoveries expose essential policy pathways for deploying AIoT healthcare solutions across varied healthcare environments, spanning resource-limited rural facilities to advanced urban medical institutions. In emerging healthcare networks, the individual-organizational reciprocal mechanism indicates that initial investments in fundamental AIoT infrastructure for chronological healthcare access can stimulate institutional capability enhancements without demanding extensive preliminary organizational transformation. For instance, remote healthcare AIoT platforms in isolated areas can simultaneously decrease patient travel expenses while enabling local healthcare facilities to access specialized knowledge, generating the bidirectional economic-organizational advantages identified in the investigation. Therefore, in sophisticated healthcare networks, the organizational-social justice correlation offers policy direction for utilizing existing institutional capabilities to address healthcare inequalities. The discoveries indicate that when well-equipped hospitals deploy responsible AIoT governance structures, they automatically advance broader social justice objectives while improving their own institutional effectiveness. This establishes opportunities for policy structures that encourage advanced healthcare institutions to function as AIoT innovation centers for underserved populations, producing multiplicative advantages across all three triadic dimensions. Ultimately, healthcare policy developers can employ these discoveries to construct integrated regulatory structures that acknowledge the reciprocal nature of AIoT healthcare advantages. Rather than developing separate policies for individual access, institutional capability, and social justice, the evidence supports comprehensive policy methods that utilize the reinforcing mechanisms between these dimensions. This encompasses developing compensation structures that reward healthcare institutions for AIoT implementations that simultaneously improve individual patient outcomes and social justice metrics, establishing systematic incentives for integrated sustainable development approaches.
In relation with the confronting AI ethics, information security, and regulatory complexities, the triadic reciprocal determinism structure demonstrates that ethical AIoT deployment constitutes not merely a compliance obligation but a fundamental enabler of the reciprocal advantages identified in this investigation. The organizational-social correlation establishes that responsible AIoT governance and transparent decision-making procedures are essential for achieving social justice accountability, indicating that ethical structures directly contribute to sustainable development outcomes rather than constraining them. Extensively, information security challenges emerge as critical enablers rather than obstacles within the triadic structure. The individual-organizational correlation demonstrates that patient confidence in AIoT systems, constructed through robust privacy safeguards, is essential for achieving the chronological healthcare adaptability that drives individual economic sustainability. When patients trust AIoT systems with their health information, they participate more comprehensively with continuous monitoring and predictive interventions, enabling healthcare institutions to develop more effective treatment capabilities. This establishes a privacy-confidence-effectiveness cycle that reinforces all three triadic dimensions.
Regulatory complexities require integrated approaches that recognize the reciprocal nature of AIoT healthcare advantages. Traditional regulatory structures that treat individual privacy, organizational compliance, and social justice as separate domains may inadvertently disrupt the reinforcing mechanisms identified in this investigation. The discoveries indicate that regulatory approaches should prioritize integrated structures that enable simultaneous advancement across all three dimensions. For example, regulatory innovation spaces that permit healthcare institutions to test innovative AIoT solutions while maintaining strict ethical oversight can facilitate the organizational transformation necessary for social justice advancement while protecting individual patient rights. The ethical implications extend to algorithmic bias reduction, which the investigation demonstrates as essential for the social-individual reciprocal stimulation mechanism. When AIoT systems exhibit bias against certain populations, they disrupt the social justice improvements that should trigger individual economic advantages, breaking the positive-sum transformation identified in the discoveries. This indicates that bias detection and reduction should be integrated into AIoT system design rather than treated as post-implementation corrections. Significantly, international regulatory harmonization emerges as critical for realizing the global sustainable development potential identified in the investigation. The triadic structure operates across healthcare systems, but regulatory fragmentation can prevent the cross-border knowledge sharing and technology transfer that maximize the reciprocal advantages. Policy structures should prioritize international cooperation in AIoT healthcare standards while respecting local healthcare contexts and cultural considerations. 76
Eventually, the measured results discoveries establish that triadic reciprocal determinism provides a robust structure for understanding AIoT healthcare transformation, exposing complex interdependencies that linear causation models cannot capture. The empirical documentation supports the theoretical proposition that sustainable healthcare development requires simultaneous advancement across individual, organizational, and social dimensions, with AIoT technology serving as the enabling mechanism for these integrated improvements while addressing ethical, privacy, and regulatory requirements as integral components rather than external constraints. From an implementation perspective, these discoveries indicate that healthcare policy and investment strategies should prioritize integrated AIoT implementations that simultaneously address individual empowerment, institutional transformation, and social justice advancement while embedding ethical governance, privacy protection, and regulatory compliance as core design principles. The evidence demonstrates that fragmented approaches focusing on single dimensions or treating ethical considerations as separate issues may miss the multiplicative advantages available through integrated AIoT deployment strategies that leverage the reciprocal reinforcement mechanisms identified in this investigation. The research advances both theoretical understanding of healthcare transformation dynamics and practical guidance for implementing AIoT solutions that maximize sustainable development outcomes through systematic integration of economic, organizational, and social improvement mechanisms while proactively addressing the ethical, privacy, and regulatory challenges that are essential for realizing the full potential of AIoT healthcare transformation across diverse global healthcare settings. 77
Conclusions and recommendations
After a series of quantitative and qualitative analyses and evaluations, the main research breakthrough is to prove that AIoT healthcare technology works like a positive feedback system. When any part improves, it automatically makes the other parts better too. We found six inter-influence correlations of this happens, showing that good healthcare technology creates win-win-win situations for patients, hospitals, and society. Critically, the biggest discovery is that healthcare technology doesn't force trade-offs between cost, quality, and fairness. Instead, AIoT makes all three better simultaneously. This completely changes how we should think about healthcare investment and policy. Rather than choosing between affordable care, high-quality treatment, or fair access, AIoT enables healthcare systems to achieve all three goals together. Because we used two different research methods and combined their results to get a complete picture. FA helped us measure the statistical relationships, while TD analysis helped us understand the deeper connections. Combining both methods gave us stronger evidence than either approach could provide alone.
On the other hand, according to our comprehensively measured results, the healthcare leaders should design policies that recognize these connected benefits instead of treating patient access, hospital performance, and health equity as separate issues. Investment decisions should prioritize technology solutions that improve multiple areas simultaneously rather than focusing on single problems. Hospital administrators should adopt comprehensive technology strategies that enhance patient care while building institutional capabilities and serving public medical needs. Noticeably, medical institutions should build ethics, privacy protection, and fairness directly into their medical operation, treatments, and activities from the beginning rather than adding these features later apply the AIoT technology. International organizations should create coordinated standards for healthcare AIoT technology that help not only countries work together while respecting local differences but also researchers to focus on interdisciplinary collaboration that connects AIoT technology innovation with healthcare policy and social justice work.
Furthermore, we identified three main categories where more research is urgently needed. First, methodological improvements should include long-term studies that track these relationships over several years, studies comparing different countries and healthcare systems, and advanced computer analysis that can handle even more complex data patterns. Second, ethical and privacy research must examine how unfair algorithms affect the positive cycles we discovered, how data protection rules influence patient trust and participation, and how different governance approaches impact healthcare outcomes. We particularly need studies on algorithm bias because unfair technology can break the positive feedback loops that make AIoT beneficial for everyone. Third, policy and cost research should focus on economic studies that prove whether AIoT investments actually save money and improve health outcomes, global health policy research that helps countries coordinate their technology strategies, and implementation studies that track what happens when healthcare systems actually adopt these integrated approaches.
Critically, this research provides strong evidence that AIoT technology can help achieve the United Nations SDG for “Good Health and Well-being” through integrated approaches that improve economic accessibility, institutional accountability, and social justice at the same time. The three-way interaction framework gives healthcare systems a practical guide for implementing technology solutions that create multiple benefits instead of requiring difficult choices between competing priorities. These findings apply immediately to both wealthy and resource-limited healthcare systems. In developing countries, strategic AIoT investments can address multiple healthcare challenges simultaneously with limited resources. In advanced healthcare systems, the framework shows how to use existing capabilities to solve persistent inequality problems while improving overall institutional performance and patient outcomes.
Our research has important limitations that future studies should address. Firstly, the measured results of FA approach depend on our specific dataset and may vary in different contexts. The qualitative analysis involves interpretive decisions that other researchers might make differently. Combining quantitative and qualitative methods requires subjective choices about how to weight different types of evidence. Successively, we addressed these limitations through multiple validation methods, transparent documentation of our procedures, testing our results under different assumptions, and seeking expert review of our methods and findings. Secondly, the surveyed data-collection were from the Taiwanese region that was a single-region and cross-sectional design research limitation. For the reason, future researchers should continue not only refining these approaches based on practical experience and new evidence but also collecting more surveyed collection-data from different regions, such as United States, Japan, China and etc.
Noticeably, the ethics, privacy, and regulation challenges of AIoT technology are still further worthy of great attention because our findings show that ethical AIoT implementation is not just about following rules; furthermore, it is essential for making the medical technologcal applications work effectively. Especially, when healthcare systems implement responsible governance and transparent decision-making, the ethics, privacy, and regulation of AIoT technology are don't just avoid problems; they actually achieve better health outcomes and social equity results. Critically, the comprehensive medical data privacy of AIoT technology works the same way. When patients trust healthcare AIoT technology with their information, the ethics, privacy, and regulation participate more fully in monitoring and prevention that helps healthcare institutions provide better care, which improves social health outcomes. Privacy protection creates a trust-effectiveness cycle of AIoT technology that benefits everyone involved because the best regulatory approaches will enable simultaneous progress across all three areas while protecting individual rights and maintaining ethical standards.
Contributively, this empirical research did establish AIoT technology as a transformative approach for sustainable healthcare development, demonstrating that digital health innovations can solve complex sustainability challenges through integrated solutions rather than simple technological upgrades. It is very apparent that this empirical research provides essential knowledge and practical guidance for realizing the full potential of digital health transformation in advancing global health equity and SDGs worldwide.
Footnotes
Acknowledgements
The authors would like to thank the anonymous reviews for their constructive comments to improve the manuscript.
Ethical statement
With reference to the current academic ethic regulation and policies of the global academic research institutions and the Taiwanese Ministry of Science and Technology and Ministry of Education, and Publication Ethics and Editorial Policies of your journal, this research belongs the free of paper and cargo examination in the social science researches. The reasons are (1) first of all, the entire interviewees agreed with the questionnaire's utilizing consent in this research; (2) the entire were over 18-year-old which is the legal age in Taiwan; (3) the entire interviewees were directly consent to be collected in person for this research; (4) no any personal information or concrete participants’ identification was disclosed in the research and questionnaires and (5) only questionnaire fill-out action was required and no invasive measures were used in the collection processes.
Consent publication
Not applicable. The survey process did not ask for or disclose the identity of the respondents. The dataset provided by the website administrators contained only anonymous data.
Contributorship
The motivation and concept: Wei-Hsi Chang and Mao-Hsien Chang. Methodology: Mao-Chang Chang, Yung-Kuan Chan, and Ming Y Hsieh. Resources: Wei-Hsi Chang and Mao-Hsien Chang. Wringing: Ming Yuan Hsieh. Project administration: Wei-Hsi Chang and Yung-Kuan Chan. Reviewing and editing: Mao-Chang Chang, Yung-Kuan Chan, and Ming Y. Hsieh. All authors have contributed to the finalization of the manuscript and are in agreement with the published version.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Taiwanese Ministry of Education (MOE-114-TPRBM-0039-017Y1), Taiwanese National Science and Technology Council (NSTC 113-2629-H-142-001-) and National Taichung Univesity of Eduaiton (NTCU114106).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.